
Psychometric Properties of the Japanese Version of the Parental Acceptance and Action Questionnaire in Parents with Infants and Toddlers



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Method of Analysis
3. Results
3.1. Demographic Data
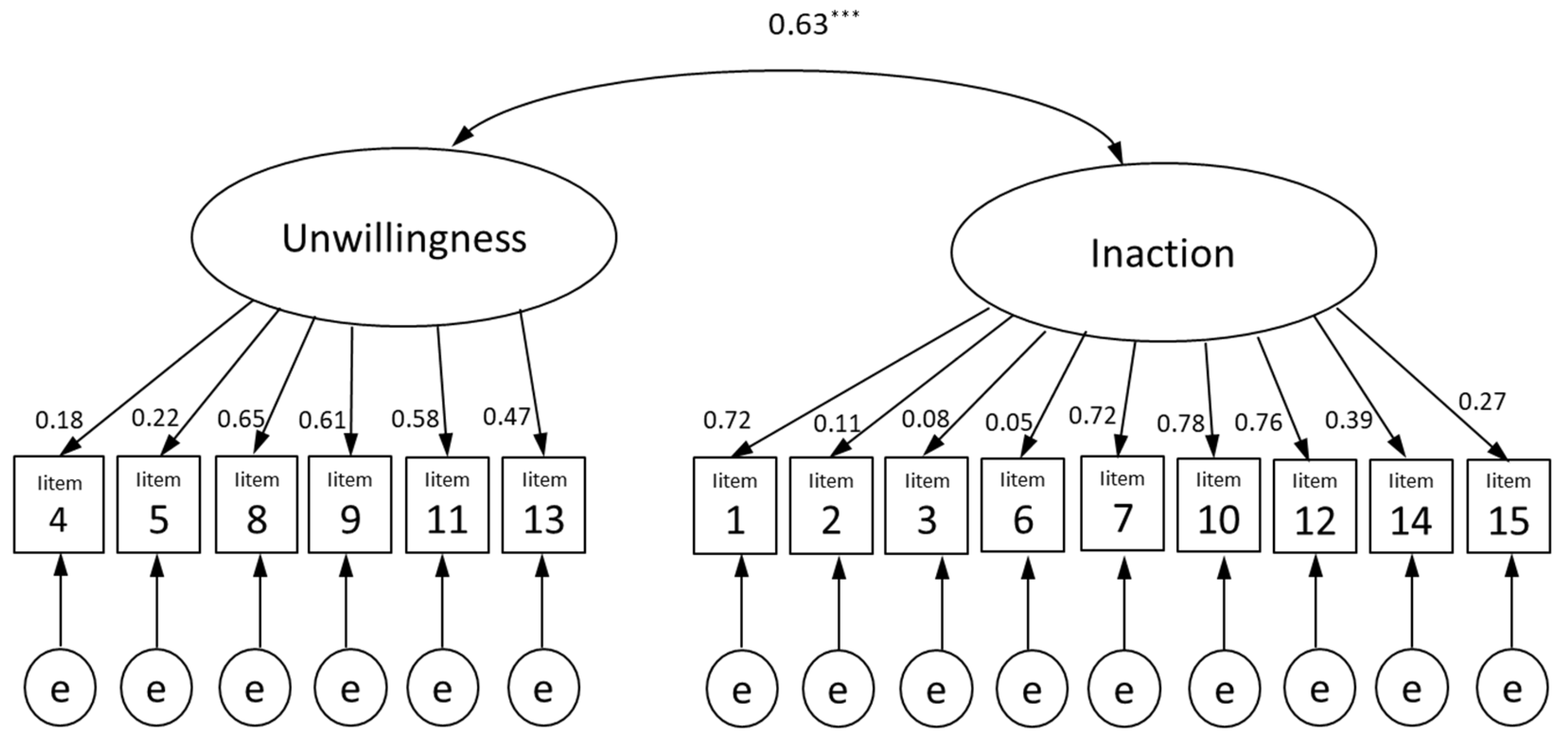
3.2. Structural Validity
3.3. Reliability
3.4. Criterion and Construct Validity
4. Discussion
4.1. Structural Validity
4.2. Reliability
4.3. Criterion and Construct Validity
4.4. Limitation and Future Research Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ministry of Health, Labour and Welfare. Number of Consultations on Child Abuse in 2021. Available online: https://www.mhlw.go.jp/content/001040752.pdf (accessed on 18 February 2023).
- Kusakabe, N.; Sakano, Y. Examination on structure of stressor related to nursing. Waseda Hum. Sci. Res. 1999, 8, 27–39. [Google Scholar]
- Maeda, K.; Nakakita, Y. Literature review on factors of parenting stress in mothers with infants. J. Mie Prefectual Coll. Nurs. 2017, 21, 97–108. [Google Scholar]
- Rutherford, H.J.V.; Wallace, N.S.; Laurent, H.K.; Mayes, L.C. Emotion regulation in parenthood. Dev. Rev. 2015, 36, 1–14. [Google Scholar] [CrossRef]
- Byrne, G.; Ghrada, A.N.; O’Mahony, T.; Brennan, E. A systematic review of the use of acceptance and commitment therapy in supporting parents. Psychol. Psychother. 2021, 94, 378–407. [Google Scholar] [CrossRef]
- Blackledge, J.T.; Ciarrochi, J.; Deane, F. Acceptance and Commitment Therapy: Contemporary Theory, Research, and Practice; Australian Academic Press: Bowen Hills, Australia, 2009. [Google Scholar]
- Bond, F.W.; Hayes, S.C.; Barnes-Holmes, D. Psychological flexibility, ACT, and organizational behavior. J. Organ. Behav. Manag. 2006, 26, 25–54. [Google Scholar] [CrossRef]
- Luoma, J.B.; Hayes, S.C.; Walser, R.D. Learning ACT: An Acceptance and Commitment Therapy Skills-Training Manual for Therapists; New Harbinger Publications: Oakland, CA, USA, 2007. [Google Scholar]
- Coyne, L.W.; McHugh, L.; Martinez, E.R. Acceptance and commitment therapy (ACT): Advances and applications with children, adolescents, and families. Child Adolesc. Psychiatr. Clin. N. Am. 2011, 20, 379–399. [Google Scholar] [CrossRef]
- Bond, F.W.; Hayes, S.C.; Baer, R.A.; Carpenter, K.M.; Guenole, N.; Orcutt, H.K.; Walts, T.; Zettle, R.D. Preliminary psychometric properties of the Acceptance and Action Questionnaire-II: A revised measure of psychological inflexibility and experiential avoidance. Behav. Ther. 2011, 42, 676–688. [Google Scholar] [CrossRef]
- Blackledge, J.T.; Hayes, S.C. Using acceptance and commitment training in the support of parents of children diagnosed with autism. Child Fam. Behav. Ther. 2006, 28, 1–18. [Google Scholar] [CrossRef]
- Brown, F.L.; Whittingham, K.; Boyd, R.N.; McKinlay, L.; Sofronoff, K. Improving child and parenting outcomes following paediatric acquired brain injury: A randomised controlled trial of Stepping Stones Triple P plus acceptance and commitment therapy. J. Child Psychol. Psychiatry 2014, 55, 1172–1183. [Google Scholar] [CrossRef]
- Whittingham, K.; Sanders, M.; McKinlay, L.; Boyd, R.N. Interventions to reduce behavioral problems in children with cerebral palsy: An RCT. Pediatrics 2014, 133, e1249–e1257. [Google Scholar] [CrossRef]
- Kanstrup, M.; Wicksell, R.K.; Kemani, M.; Wiwe, L.C.; Lekander, M.; Holmström, L. A clinical pilot study of individual and group treatment for adolescents with chronic pain and their parents: Effects of acceptance and commitment therapy on functioning. Children 2016, 3, 30. [Google Scholar] [CrossRef]
- Kemani, M.K.; Kanstrup, M.; Jordan, A.; Caes, L.; Gauntlett-Gilbert, J. Evaluation of an intensive interdisciplinary pain treatment based on acceptance and commitment therapy for adolescents with chronic pain and their parents: A nonrandomized clinical trial. J. Pediatr. Psychol. 2018, 43, 981–994. [Google Scholar] [CrossRef]
- Greene, R.L.; Field, C.E.; Fargo, J.D.; Twohig, M.P. Development and validation of the parental acceptance questionnaire (6-PAQ). J. Context. Behav. Sci. 2015, 4, 170–175. [Google Scholar] [CrossRef]
- Burke, K.; Moore, S. Development of the parental psychological flexibility questionnaire. Child Psychiatry Hum. Dev. 2015, 46, 548–557. [Google Scholar] [CrossRef]
- Coyne, L.W.; Wilson, K.G. The Role of Cognitive Fusion in Impaired Parenting: An RFT Analysis. Int. J. Psychol. Psychol. Ther. 2004, 4, 469–486. [Google Scholar]
- Brassell, A.A.; Rosenberg, E.; Parent, J.; Rough, J.N.; Fondacaro, K.; Seehuus, M. Parent’s psychological flexibility: Associations with parenting and child psychosocial well-being. J. Context. Behav. Sci. 2016, 5, 111–120. [Google Scholar] [CrossRef]
- Fonseca, A.; Moreira, H.; Canavarro, M.S. Uncovering the links between parenting stress and parenting styles: The role of psychological flexibility within parenting and global psychological flexibility. J. Context. Behav. Sci. 2020, 18, 59–67. [Google Scholar] [CrossRef]
- Cheron, D.M.; Ehrenreich, J.T.; Pincus, D.B. Assessment of parental experiential avoidance in a clinical sample of children with anxiety disorders. Child Psychiatry Hum. Dev. 2009, 40, 383–403. [Google Scholar] [CrossRef]
- Hayes, S.C.; Strosahl, K.; Wilson, K.G.; Bissett, R.T.; Pistorello, J.; Toarmino, D.; Polusny, M.A.; Dykstra, T.A.; Batten, S.V.; Bergan, J.; et al. Measuring experiential avoidance: A preliminary test of a working model. Psychol. Rec. 2004, 54, 553–578. [Google Scholar] [CrossRef]
- Mizusaki, Y.; Sato, H. Development of the Japanese version of the parental acceptance and action questionnaire: A preliminary study. Humanit. Rev. Bull. Kwansei Gakuin Univ. Pepository 2018, 67, 45–56. [Google Scholar]
- Shima, T.; Yanagihara, M.; Kawai, T.; Kumano, H. Validation of the Japanese Version of the Acceptance and Action Questionnaire-II. In Proceedings of the 77th Annual Convention of the Japanese Psychological Association, Sapporo, Japan, 19 September 2013; Volume 77, p. 271. (In Japanese). [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Hatta, H.; Higashi, A.; Yashiro, H.; Ozasa, K.; Hayashi, K.; Kiyota, K.; Inokuchi, H.; Ikeda, J.; Fujita, K.; Watanabe, Y.; et al. A validation of the hospital anxiety and depression scale. Jpn. J. Psychosom. Med. 1998, 38, 309–315, (In Japanese with English abstract). [Google Scholar] [CrossRef]
- Terwee, C.B.; Mokkink, L.B.; Knol, D.L.; Ostelo, R.W.J.G.; Bouter, L.M.; de Vet, H.C. Rating the methodological quality in systematic reviews of studies on measurement properties: A scoring system for the COSMIN checklist. Qual. Life Res. 2012, 21, 651–657. [Google Scholar] [CrossRef]
- de Vet, H.C.W.; Terwee, C.B.; Mokkink, L.B.; Knol, D.L. Measurement in Medicine: A Practical Guide; Cambridge University Press: Cambridge, MA, USA, 2011. [Google Scholar]
- Coyne, L.W.; Murrell, A.R. The Joy of Parenting. An Acceptance and Commitment Therapy Guide to Effective Parenting in the Early Years; New Harbinger Publications: Oakland, CA, USA, 2009. [Google Scholar]
- Twohig, M.M.P.; Levin, M.E. Acceptance and commitment therapy as a treatment for anxiety and depression: A review. Psychiatr. Clin. N. Am. 2017, 40, 751–770. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| n = 2000 | ||
|---|---|---|
| Mean | % or SD | |
| Parent Age | 33.58 | 4.70 |
| Employment status | ||
| Full-time (over 4 days) | 559 | 28.0% |
| Part-time (under 3 days) | 162 | 8.1% |
| Childcare leave | 438 | 21.4% |
| Unemployed | 829 | 41.4% |
| Number of births | 2.66 | 0.80 |
| Child birth order | 1.51 | 0.74 |
| Child Age | 1.50 | 1.12 |
| Current Illness | ||
| Psychiatric disorders | 50 | 2.5% |
| PMS | 254 | 12.7% |
| PMDD | 54 | 2.7% |
| Measures: | ||
| Inaction-B | 15.93 | 4.47 |
| Inaction-C | 13.62 | 4.45 |
| Unwillingness | 13.62 | 4.40 |
| PAAQ-total | 43.18 | 7.42 |
| AAQ-II-total | 20.12 | 8.35 |
| HADS-D | 8.48 | 3.65 |
| HADS-A | 6.01 | 3.79 |
| Factor | No. | Item | Factor Loadings | ||
|---|---|---|---|---|---|
| I | II | III | |||
| Inaction-B | 10 * | Despite my doubts, I feel as though I can set a plan for managing my child’s feelings. | 0.08 | −0.11 | 0.78 |
| 12 * | If I get frustrated with my child, then I can still help him or her. | 0.77 | −0.07 | 0.07 | |
| 7 * | I’m not afraid of my child’s feelings. | 0.76 | 0.02 | −0.07 | |
| 1 * | I am able to take action about my child’s fears, worries, and feelings even if I am uncertain what the right thing is to do. | 0.74 | 0.05 | −0.06 | |
| Inaction-C | 15 | When I compare myself to other parents, it seems that most of them are handling their lives better than I do. | 0.04 | 0.72 | −0.04 |
| 14 | I often catch myself daydreaming about things I’ve done with my child and what I would do differently next time. | 0.19 | 0.71 | −0.07 | |
| 2 | When I feel depressed or anxious, I am unable to help my child manage their fears, worries, or feelings. | −0.15 | 0.62 | −0.06 | |
| 3 | I try to suppress thoughts and feelings about my child that I don’t like by just not thinking about them. | −0.18 | 0.46 | 0.15 | |
| Unwillingness | 9 | It is bad if my child feels anxious. | −0.09 | −0.05 | 0.85 |
| 11 | If I could magically remove all the painful experiences my child has had in his or her life, I would do so. | 0.12 | 0.03 | 0.48 | |
| 13 | Worries can get in the way of my child’s success. | 0.01 | 0.13 | 0.42 | |
| 8 | I try hard to avoid having my child feel depressed or anxious. | 0.30 | 0.12 | 0.38 | |
| Inter-Factor Correlation | I | II | III | ||
| I | ― | −0.18 | −0.04 | ||
| II | ― | 0.41 | |||
| III | ― | ||||
| HADS | ||||
|---|---|---|---|---|
| α | AAQ-II | Depression | Anxiety | |
| Total | 0.80 | 0.57 ** | 0.32 ** | 0.33 ** |
| Inaction | 0.74 | 0.48 ** | 0.36 ** | 0.34 ** |
| Inaction-B | 0.84 | 0.01 | 0.30 ** | 0.30 ** |
| Inaction-C | 0.72 | 0.59 ** | 0.19 ** | 0.27 ** |
| Unwillingness | 0.68 | 0.35 ** | 0.02 | 0.09 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okajima, J.; Okajima, I. Psychometric Properties of the Japanese Version of the Parental Acceptance and Action Questionnaire in Parents with Infants and Toddlers. Int. J. Environ. Res. Public Health 2023, 20, 5674. https://doi.org/10.3390/ijerph20095674
Okajima J, Okajima I. Psychometric Properties of the Japanese Version of the Parental Acceptance and Action Questionnaire in Parents with Infants and Toddlers. International Journal of Environmental Research and Public Health. 2023; 20(9):5674. https://doi.org/10.3390/ijerph20095674
Chicago/Turabian StyleOkajima, Junko, and Isa Okajima. 2023. "Psychometric Properties of the Japanese Version of the Parental Acceptance and Action Questionnaire in Parents with Infants and Toddlers" International Journal of Environmental Research and Public Health 20, no. 9: 5674. https://doi.org/10.3390/ijerph20095674
APA StyleOkajima, J., & Okajima, I. (2023). Psychometric Properties of the Japanese Version of the Parental Acceptance and Action Questionnaire in Parents with Infants and Toddlers. International Journal of Environmental Research and Public Health, 20(9), 5674. https://doi.org/10.3390/ijerph20095674