



Group-Based Patterns of Life Satisfaction and Functional Independence over the 10 Years after Traumatic Brain Injury in Older Adults: A Model Systems Study


Abstract
1. Introduction
2. Method
2.1. Participants
2.2. Procedure
2.3. Measures
2.4. Statistical Analyses
3. Results
3.1. Cluster Analysis
3.2. ANOVAs and Chi-Square Analyses for Combined FIM and SWLS
4. Discussion
5. Limitations and Future Directions
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Rates of TBI-Related Emergency Department Visits, Hospitalizations, and Deaths—United States, 2001–2010. Available online: https://www.cdc.gov/traumaticbraininjury/data/rates.html (accessed on 12 April 2023).
- Centers for Disease Control and Prevention Get the Facts about TBI. Available online: https://www.cdc.gov/traumaticbraininjury/get_the_facts.html (accessed on 12 April 2023).
- Corrigan, J.D.; Hammond, F.M. Traumatic Brain Injury as a Chronic Health Condition. Arch. Phys. Med. Rehabil. 2013, 94, 1199–1201. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Moderate to Severe Traumatic Brain Injury Is a Lifelong Condition. Available online: https://www.cdc.gov/traumaticbraininjury/pdf/moderate_to_severe_tbi_lifelong-a.pdf (accessed on 11 October 2020).
- Cifu, D.X.; Kreutzer, J.S.; Marwitz, J.H.; Rosenthal, M.; Englander, J.; High, W. Functional Outcomes of Older Adults with Traumatic Brain Injury: A Prospective, Multicenter Analysis. Arch. Phys. Med. Rehabil. 1996, 77, 883–888. [Google Scholar] [CrossRef] [PubMed]
- Susman, M.; DiRusso, S.M.; Sullivan, T.; Risucci, D.; Nealon, P.; Cuff, S.; Haider, A.; Benzil, D. Traumatic Brain Injury in the Elderly: Increased Mortality and Worse Functional Outcome at Discharge Despite Lower Injury Severity. J. Trauma Inj. Infect. Crit. Care 2002, 53, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Mosenthal, A.C.; Livingston, D.H.; Lavery, R.F.; Knudson, M.M.; Lee, S.; Morabito, D.; Manley, G.T.; Nathens, A.; Jurkovich, G.; Hoyt, D.B.; et al. The Effect of Age on Functional Outcome in Mild Traumatic Brain Injury: 6-Month Report of a Prospective Multicenter Trial. J. Trauma Inj. Infect. Crit. Care 2004, 56, 1042–1048. [Google Scholar] [CrossRef] [PubMed]
- Dams-O’Connor, K.; Gibbons, L.E.; Bowen, J.D.; McCurry, S.M.; Larson, E.B.; Crane, P.K. Risk for Late-Life Re-Injury, Dementia and Death among Individuals with Traumatic Brain Injury: A Population-Based Study. J. Neurol. Neurosurg. Psychiatry 2013, 84, 177–182. [Google Scholar] [CrossRef]
- Gardner, R.C.; Dams-O’Connor, K.; Morrissey, M.R.; Manley, G.T. Geriatric Traumatic Brain Injury: Epidemiology, Outcomes, Knowledge Gaps, and Future Directions. J. Neurotrauma 2018, 35, 889–906. [Google Scholar] [CrossRef]
- Fu, T.S.; Jing, R.; McFaull, S.R.; Cusimano, M.D. Recent Trends in Hospitalization and In-Hospital Mortality Associated with Traumatic Brain Injury in Canada: A Nationwide, Population-Based Study. J. Trauma Acute Care Surg. 2015, 79, 449–455. [Google Scholar] [CrossRef]
- Harvey, L.A.; Close, J.C.T. Traumatic Brain Injury in Older Adults: Characteristics, Causes and Consequences. Injury 2012, 43, 1821–1826. [Google Scholar] [CrossRef]
- Haring, R.S.; Narang, K.; Canner, J.K.; Asemota, A.O.; George, B.P.; Selvarajah, S.; Haider, A.H.; Schneider, E.B. Traumatic Brain Injury in the Elderly: Morbidity and Mortality Trends and Risk Factors. J. Surg. Res. 2015, 195, 1–9. [Google Scholar] [CrossRef]
- Vollmer, D.G.; Torner, J.C.; Jane, J.A.; Sadovnic, B.; Charlebois, D.; Eisenberg, H.M.; Foulkes, M.A.; Marmarou, A.; Marshall, L.F. Age and Outcome Following Traumatic Coma: Why Do Older Patients Fare Worse? J. Neurosurg. 1991, 75, S37–S49. [Google Scholar] [CrossRef]
- Dams-O’Connor, K.; Gibbons, L.E.; Landau, A.; Larson, E.B.; Crane, P.K. Health Problems Precede Traumatic Brain Injury in Older Adults. J. Am. Geriatr. Soc. 2016, 64, 844–848. [Google Scholar] [CrossRef]
- Green, R.E.; Colella, B.; Christensen, B.; Johns, K.; Frasca, D.; Bayley, M.; Monette, G. Examining Moderators of Cognitive Recovery Trajectories after Moderate to Severe Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2008, 89, S16–S24. [Google Scholar] [CrossRef]
- Liu, H.; Yang, Y.; Xia, Y.; Zhu, W.; Leak, R.K.; Wei, Z.; Wang, J.; Hu, X. Aging of Cerebral White Matter. Ageing Res. Rev. 2017, 34, 64–76. [Google Scholar] [CrossRef] [PubMed]
- Rothweiler, B.; Temkin, N.R.; Dikmen, S.S. Aging Effect on Psychosocial Outcome in Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 1998, 79, 881–887. [Google Scholar] [CrossRef] [PubMed]
- Haller, C.S.; Delhumeau, C.; De Pretto, M.; Schumacher, R.; Pielmaier, L.; Rebetez, M.M.L.; Haller, G.; Walder, B. Trajectory of Disability and Quality-of-Life in Non-Geriatric and Geriatric Survivors after Severe Traumatic Brain Injury. Brain Inj. 2017, 31, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Jacobsson, L.J.; Westerberg, M.; Lexell, J. Health-Related Quality-of-Life and Life Satisfaction 6–15 Years after Traumatic Brain Injuries in Northern Sweden. Brain Inj. 2010, 24, 1075–1086. [Google Scholar] [CrossRef] [PubMed]
- Marquez de la Plata, C.D.; Hart, T.; Hammond, F.M.; Frol, A.B.; Hudak, A.; Harper, C.R.; O’Neil-Pirozzi, T.M.; Whyte, J.; Carlile, M.; Diaz-Arrastia, R. Impact of Age on Long-Term Recovery from Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2008, 89, 896–903. [Google Scholar] [CrossRef]
- Sveen, U.; Røe, C.; Sigurdardottir, S.; Skandsen, T.; Andelic, N.; Manskow, U.; Berntsen, S.A.; Soberg, H.L.; Anke, A. Rehabilitation Pathways and Functional Independence One Year after Severe Traumatic Brain Injury. Eur. J. Phys. Rehabil. Med. 2016, 52, 650–661. [Google Scholar]
- Sendroy-Terrill, M.; Whiteneck, G.G.; Brooks, C.A. Aging with Traumatic Brain Injury: Cross-Sectional Follow-Up of People Receiving Inpatient Rehabilitation Over More Than 3 Decades. Arch. Phys. Med. Rehabil. 2010, 91, 489–497. [Google Scholar] [CrossRef]
- Testa, J.A.; Malec, J.F.; Moessner, A.M.; Brown, A.W. Outcome after Traumatic Brain Injury: Effects of Aging on Recovery. Arch. Phys. Med. Rehabil. 2005, 86, 1815–1823. [Google Scholar] [CrossRef]
- Lin, Y.-N.; Hwang, H.-F.; Chen, Y.-J.; Cheng, C.-H.; Liang, W.-M.; Lin, M.-R. Suitability of the Quality of Life after Brain Injury Instrument for Older People with Traumatic Brain Injury. J. Neurotrauma 2016, 33, 1363–1370. [Google Scholar] [CrossRef]
- Corrigan, J.D.; Bogner, J.A.; Mysiw, W.J.; Clinchot, D.; Fugate, L. Life Satisfaction after Traumatic Brain Injury. J. Head Trauma Rehabil. 2001, 16, 543–555. [Google Scholar] [CrossRef] [PubMed]
- Resch, J.A.; Villarreal, V.; Johnson, C.L.; Elliott, T.R.; Kwok, O.-M.; Berry, J.W.; Underhill, A.T. Trajectories of Life Satisfaction in the First 5 Years Following Traumatic Brain Injury. Rehabil. Psychol. 2009, 54, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Stineman, M.G.; Shea, J.A.; Jette, A.; Tassoni, C.J.; Ottenbacher, K.J.; Fiedler, R.; Granger, C.V. The Functional Independence Measure: Tests of Scaling Assumptions, Structure, and Reliability across 20 Diverse Impairment Categories. Arch. Phys. Med. Rehabil. 1996, 77, 1101–1108. [Google Scholar] [CrossRef]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction with Life Scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Pavot, W.; Diener, E. Review of the Satisfaction with Life Scale. Psychol. Assess. 1993, 5, 164–172. [Google Scholar] [CrossRef]
- Teasdale, G.; Jennett, B. Assessment and Prognosis of Coma after Head Injury. Acta Neurochir. 1976, 34, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Reith, F.C.M.; Lingsma, H.F.; Gabbe, B.J.; Lecky, F.E.; Roberts, I.; Maas, A.I.R. Differential Effects of the Glasgow Coma Scale Score and Its Components: An Analysis of 54,069 Patients with Traumatic Brain Injury. Injury 2017, 48, 1932–1943. [Google Scholar] [CrossRef]
- Utomo, W.K.; Gabbe, B.J.; Simpson, P.M.; Cameron, P.A. Predictors of In-Hospital Mortality and 6-Month Functional Outcomes in Older Adults after Moderate to Severe Traumatic Brain Injury. Injury 2009, 40, 973–977. [Google Scholar] [CrossRef]
- Rapoport, M.J.; Herrmann, N.; Shammi, P.; Kiss, A.; Phillips, A.; Feinstein, A. Outcome after Traumatic Brain Injury Sustained in Older Adulthood: A One-Year Longitudinal Study. Am. J. Geriatr. Psychiatry 2006, 14, 456–465. [Google Scholar] [CrossRef]
- Corrigan, J.D.; Smith-Knapp, K.; Granger, C.V. Outcomes in the First 5 Years after Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 1998, 79, 298–305. [Google Scholar] [CrossRef]
- Webb, C.R.; Wrigley, M.; Yoels, W.; Fine, P.R. Explaining Quality of Life for Persons with Traumatic Brain Injuries 2 Years after Injury. Arch. Phys. Med. Rehabil. 1995, 76, 1113–1119. [Google Scholar] [CrossRef] [PubMed]
- Wood, R.Ll.; Rutterford, N.A. Demographic and Cognitive Predictors of Long-Term Psychosocial Outcome Following Traumatic Brain Injury. J. Int. Neuropsychol. Soc. 2006, 12, 350–358. [Google Scholar] [CrossRef]
- Juengst, S.B.; Adams, L.M.; Bogner, J.A.; Arenth, P.M.; O’Neil-Pirozzi, T.M.; Dreer, L.E.; Hart, T.; Bergquist, T.F.; Bombardier, C.H.; Dijkers, M.P.; et al. Trajectories of Life Satisfaction after Traumatic Brain Injury: Influence of Life Roles, Age, Cognitive Disability, and Depressive Symptoms. Rehabil. Psychol. 2015, 60, 353–364. [Google Scholar] [CrossRef]
- Nelson, L.D.; Kramer, M.D.; Joyner, K.J.; Patrick, C.J.; Stein, M.B.; Temkin, N.; Levin, H.S.; Whyte, J.; Markowitz, A.J.; Giacino, J.; et al. Relationship between Transdiagnostic Dimensions of Psychopathology and Traumatic Brain Injury (TBI): A TRACK-TBI Study. J. Abnorm. Psychol. 2021, 130, 423–434. [Google Scholar] [CrossRef] [PubMed]
- Arango-Lasprilla, J.C.; Rosenthal, M.; Deluca, J.; Komaroff, E.; Sherer, M.; Cifu, D.; Hanks, R. Traumatic Brain Injury and Functional Outcomes: Does Minority Status Matter? Brain Inj. 2007, 21, 701–708. [Google Scholar] [CrossRef]
- Gary, K.W.; Arango-Lasprilla, J.C.; Stevens, L.F. Do Racial/Ethnic Differences Exist in Post-Injury Outcomes after TBI? A Comprehensive Review of the Literature. Brain Inj. 2009, 23, 775–789. [Google Scholar] [CrossRef] [PubMed]
- Farace, E.; Alves, W.M. Do Women Fare Worse: A Metaanalysis of Gender Differences in Traumatic Brain Injury Outcome. J. Neurosurg. 2000, 93, 539–545. [Google Scholar] [CrossRef]
- Gretebeck, K.A.; Sabatini, L.M.; Black, D.R.; Gretebeck, R.J. Physical Activity, Functional Ability, and Obesity in Older Adults: A Gender Difference. J. Gerontol. Nurs. 2017, 43, 38–46. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | (N = 1841) |
|---|---|
| Age, M (SD) | 70.65 (8.17) |
| Sex, n (%) | |
| Male | 1148 (62.4) |
| Female | 693 (37.6) |
| Race/Ethnicity, n (%) | |
| White | 1478 (80.3) |
| Black | 210 (11.4) |
| Asian/Pacific Islander | 47 (2.6) |
| Native American | 5 (0.3) |
| Hispanic Origin | 87 (4.7) |
| Other | 14 (0.8) |
| Relationship Status n (%) | |
| Partnered | 1074 (58.3) |
| Unpartnered | 767 (41.6) |
| Education | 13.56 (3.43) |
| Employment at Injury, n (%) | |
| Competitively Employed | 668 (27.2) |
| Not Employed | 1620 (65.9) |
| Injury Severity (GCS), M (SD) | 13.55 (2.5) |
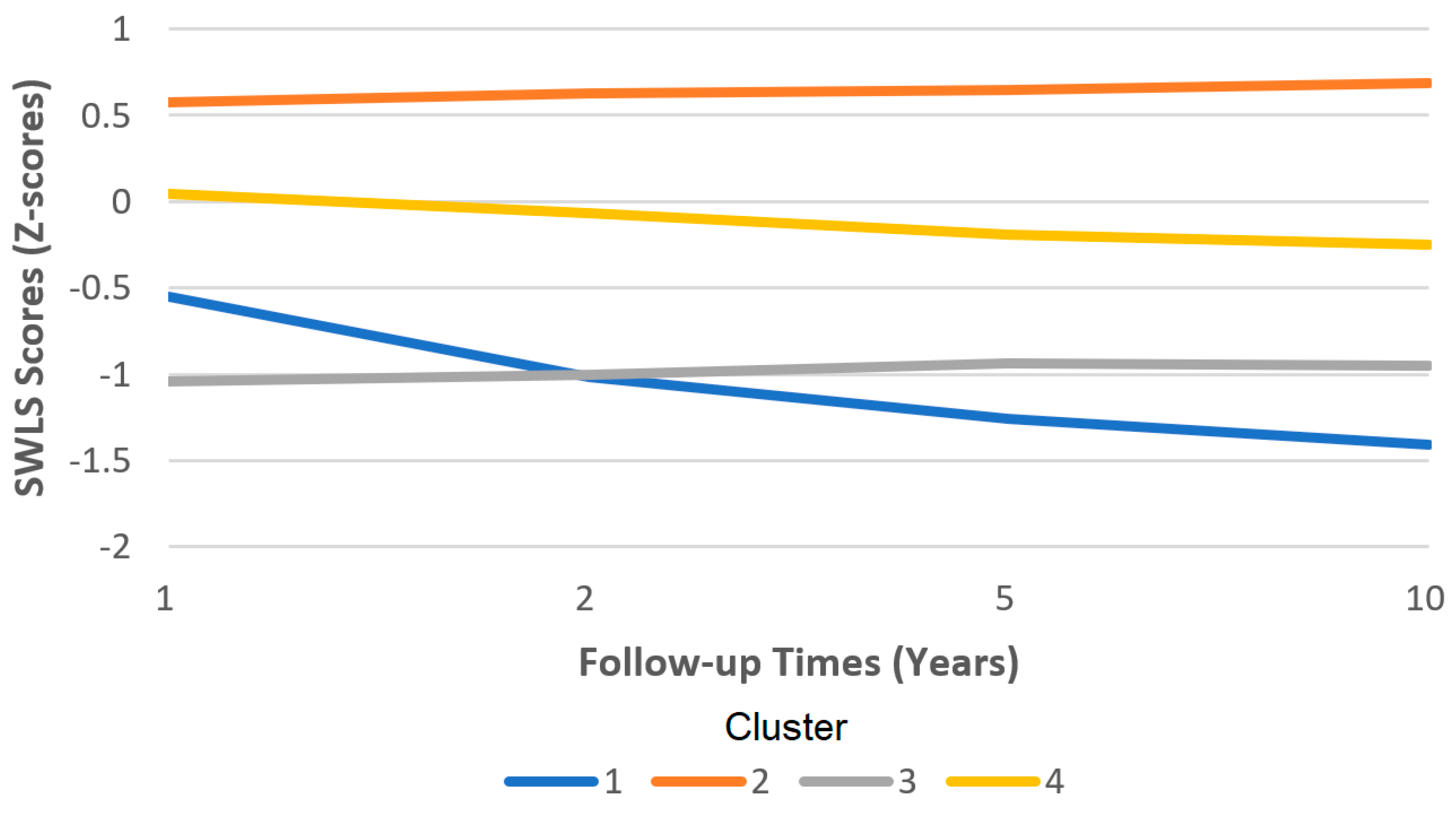
| Cluster 1 | Cluster 2 | Cluster 3 | Cluster 4 | |
|---|---|---|---|---|
| (Needs Much Help and Very Dissatisfied) | (Independent and Satisfied) | (Fairly Independent and Dissatisfied) | (Needs Some Help and Slightly Dissatisfied) | |
| Classifying Variable | (n = 91) | (n = 981) | (n = 505) | (n = 264) |
| Year 1 | ||||
| FIM | −2.40903 | 0.40953 | 0.14941 | −0.97718 |
| SWLS | −0.54831 | 0.57338 | −1.03979 | 0.04735 |
| Year 2 | ||||
| FIM | −3.02526 | 0.43514 | 0.19263 | −0.94262 |
| SWLS | −1.01471 | 0.62757 | −1.00188 | −0.06576 |
| Year 5 | ||||
| FIM | −3.09362 | 0.43031 | 0.21769 | −0.94905 |
| SWLS | −1.25781 | 0.64894 | −0.93576 | −0.18785 |
| Year 10 | ||||
| FIM | −2.74993 | 0.45825 | 0.10454 | −0.95487 |
| SWLS | −1.40552 | 0.68890 | −0.95328 | −0.25188 |
| Variable | Omnibus p-Value | Cluster 1: (Needs Much Help and Very Dissatisfied) | Cluster 2: (Independent and Satisfied) | Cluster 3: (Fairly Independent and Dissatisfied) | Cluster 4: (Needs Some Help and Slightly Dissatisfied) |
|---|---|---|---|---|---|
| Age at Injury, M (SD) | <0.001 | 73.04 (8.61) a,b | 70.46 (7.78) a,c,d | 68.64 (7.68) b,c,e | 74.37 (8.90) d,e |
| Sex (% male) | 0.022 | 49.5% | 64.3% | 62.8% | 58.7% |
| Race/Ethnicity (%) | <0.001 | ||||
| White | 69.2% | 82.1% | 81.0% | 76.1% | |
| Black | 14.3% | 9.5% | 13.1% | 14.4% | |
| Asian/Pacific Islander | 3.3% | 3.3% | 1.0% | 2.7% | |
| Na. American | 3.3% | 0.2% | 0.0% | 0.0% | |
| Hispanic | 9.9% | 4.2% | 4.2% | 6.1% | |
| Other | 0.0% | 0.8% | 0.8% | 0.8% | |
| Relationship (% partnered) | <0.001 | 52.7% | 64.7% | 47.5% | 57.2% |
| Education, M (SD) | 0.010 | 13.02 (3.51) | 13.79 (3.43) | 13.42 (3.16) | 13.10 (3.43) |
| Employed (weeks), M (SD) | 0.005 | 38 (22.02) | 46.69 (13.56) a | 42.55 (17.35) a | 43.7 (17.73) |
| (GCS) Injury Severity, M (SD) | 0.585 | 13.64 (2.58) | 13.57 (2.42) | 13.43 (2.73) | 13.69 (2.26) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tyler, C.M.; Dini, M.E.; Perrin, P.B. Group-Based Patterns of Life Satisfaction and Functional Independence over the 10 Years after Traumatic Brain Injury in Older Adults: A Model Systems Study. Int. J. Environ. Res. Public Health 2023, 20, 5643. https://doi.org/10.3390/ijerph20095643
Tyler CM, Dini ME, Perrin PB. Group-Based Patterns of Life Satisfaction and Functional Independence over the 10 Years after Traumatic Brain Injury in Older Adults: A Model Systems Study. International Journal of Environmental Research and Public Health. 2023; 20(9):5643. https://doi.org/10.3390/ijerph20095643
Chicago/Turabian StyleTyler, Carmen M., Mia E. Dini, and Paul B. Perrin. 2023. "Group-Based Patterns of Life Satisfaction and Functional Independence over the 10 Years after Traumatic Brain Injury in Older Adults: A Model Systems Study" International Journal of Environmental Research and Public Health 20, no. 9: 5643. https://doi.org/10.3390/ijerph20095643
APA StyleTyler, C. M., Dini, M. E., & Perrin, P. B. (2023). Group-Based Patterns of Life Satisfaction and Functional Independence over the 10 Years after Traumatic Brain Injury in Older Adults: A Model Systems Study. International Journal of Environmental Research and Public Health, 20(9), 5643. https://doi.org/10.3390/ijerph20095643