
Efficacy of an Online Workplace Mental Health Accommodations Psychoeducational Course: A Randomized Controlled Trial

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Method
2.1. Research Design and Ethics
2.2. Participants
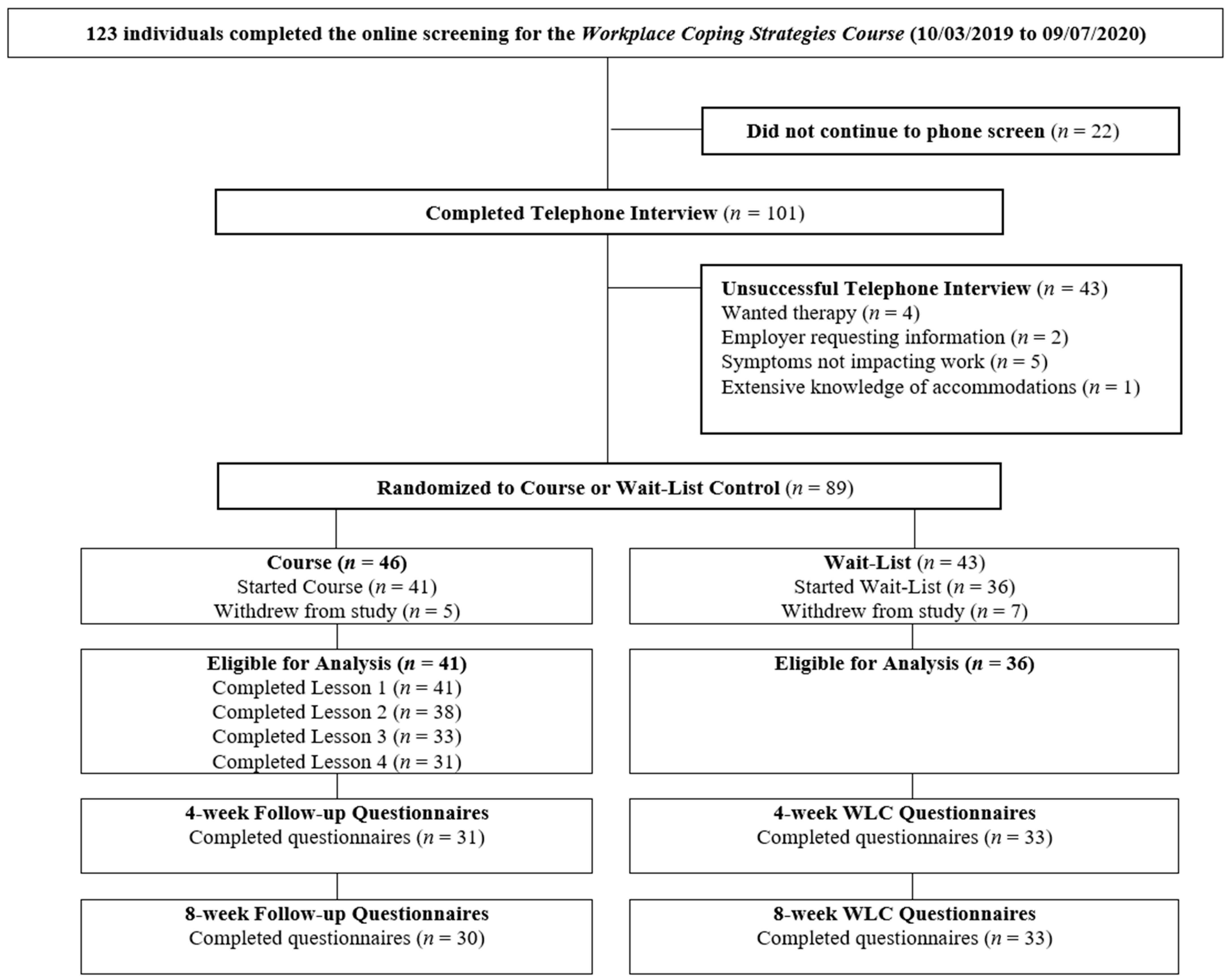
2.2.1. Recruitment
2.2.2. Eligibility
2.2.3. Randomization
2.2.4. Sample Size
2.2.5. Power
2.3. Intervention
Procedure
2.4. Measures
2.4.1. Demographics
2.4.2. Accommodation Questions
2.4.3. Self-Stigma of Mental Illness Scale Short Form (SSMIS-SF; [41])
2.4.4. Worker Relations Scale (WRS; [42])
2.4.5. Work Performance
2.4.6. New General Self-Efficacy Scale (NGSE; [45])
2.4.7. Supervisor Servant Leadership Scale (SSLS; [47])
2.4.8. Climate for Inclusion Scale (CIS; [48])
2.4.9. Disclosure
2.4.10. PHQ-9
2.4.11. GAD-7
2.4.12. SIAS-6 and SPS-6
2.5. Analyses
3. Results
3.1. Participant Characteristics
3.2. Primary Outcome Measures
Psychological Distress/Symptomology
3.3. Role of Supervisory Leadership and Organizational Inclusiveness
4. Discussion
5. Study Limitations
6. Future Directions
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kensbock, J.M.; Boehm, S.A.; Bourovoi, K. Is there a downside of job accommodations? An employee perspective on individual change processes. Front. Psychol. 2017, 8, 1536. [Google Scholar] [CrossRef]
- Follmer, K.B.; Jones, K.S. Mental illness in the workplace: An interdisciplinary review and organizational research agenda. J. Manag. 2018, 44, 325–351. [Google Scholar] [CrossRef]
- McDowell, C.; Fossey, E. Workplace accommodations for people with mental illness: A scoping review. J. Occup. Rehabil. 2015, 25, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Fabian, E.S.; Waterworth, A.; Ripke, B. Reasonable accommodations for workers with serious mental illness: Type, frequency, and associated outcomes. Psychosoc. Rehabil. J. 1993, 17, 163–172. [Google Scholar] [CrossRef]
- Chow, C.M.; Cichocki, B. Predictors of job accommodations for individuals with psychiatric disabilities. Rehabil. Couns. Bull. 2016, 59, 172–184. [Google Scholar] [CrossRef]
- O’Donnell, S.; Vanderloo, S.; McRae, L.; Onysko, J.; Patten, S.B.; Pelletier, L. Comparison of the estimated prevalence of mood and/or anxiety disorders in Canada between self-report and administrative data. Epidemiol. Psychiatr. Sci. 2016, 25, 360–369. [Google Scholar] [CrossRef] [PubMed]
- Fan, L.B.; Blumenthal, J.A.; Watkins, L.L.; Sherwood, A. Work and home stress: Associations with anxiety and depression symptoms. Occup. Med. 2015, 65, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Milner, A.; Witt, K.; LaMontagne, A.D.; Niedhammer, I. Psychosocial job stressors and suicidality: A meta-analysis and systematic review. Occup. Environ. Med. 2018, 75, 245. [Google Scholar] [CrossRef]
- Hennekam, S.; Richard, S.; Grima, F. Coping with mental health conditions at work and its impact on self-perceived job performance. Empl. Relat. Int. J. 2020, 42, 626–645. [Google Scholar] [CrossRef]
- Kelloway, E.K.; Dimoff, J.K.; Gilbert, S. Mental health in the workplace. Annu. Rev. Organ. Psychol. Organ. Behav. 2023, 10, 363–387. [Google Scholar] [CrossRef]
- Wilmer, M.T.; Anderson, K.; Reynolds, M. Correlates of Quality of Life in Anxiety Disorders: Review of Recent Research. Curr. Psychiatry Rep. 2021, 23, 77. [Google Scholar] [CrossRef] [PubMed]
- Miraglia, M.; Johns, G. Going to work ill: A meta-analysis of the correlates of presenteeism and a dual-path model. J. Occup. Health Psychol. 2016, 21, 261–283. [Google Scholar] [CrossRef] [PubMed]
- Johnston, D.A.; Harvey, S.B.; Glozier, N.; Calvo, R.A.; Christensen, H.; Deady, M. The relationship between depression symptoms, absenteeism and presenteeism. J. Affect. Disord. 2019, 256, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Bolo, C.; Sareen, J.; Patten, S.; Schmitz, N.; Currie, S.; Wang, J. Receiving workplace mental health accommodations and the outcome of mental disorders in employees with a depressive and/or anxiety disorder. J. Occup. Environ. Med. 2013, 55, 1293–1299. [Google Scholar] [CrossRef]
- Villotti, P.; Corbière, M.; Fossey, E.; Fraccaroli, F.; Lecomte, T.; Harvey, C. Work accommodations and natural supports for employees with severe mental illness in social businesses: An international comparison. Community Ment. Health J. 2017, 53, 864–870. [Google Scholar] [CrossRef]
- Bastien, M.-F.; Corbière, M. Return-to-work following depression: What work accommodations do employers and human resources directors put in place? J. Occup. Rehabil. 2018, 29, 423–432. [Google Scholar] [CrossRef] [PubMed]
- Chow, C.M.; Cichocki, B.; Croft, B. The impact of job accommodations on employment outcomes among individuals with psychiatric disabilities. Psychiatr. Serv. 2014, 65, 1126–1132. [Google Scholar] [CrossRef] [PubMed]
- Gewurtz, R.E.; Langan, S.; Shand, D. Hiring people with disabilities: A scoping review. Work 2016, 54, 135–148. [Google Scholar] [CrossRef]
- Schartz, H.A.; Hendricks, D.J.; Blanck, P. Workplace accommodations: Evidence-based outcomes. Work 2006, 27, 345–354. [Google Scholar]
- Schur, L.; Nishii, L.; Adya, M.; Kruse, D.; Bruyère, S.; Blanck, P. Accommodating employees with and without disabilities. Hum. Resour. Manag. 2014, 53, 593–621. [Google Scholar] [CrossRef]
- Wang, J.; Patten, S.; Currie, S.; Sareen, J.; Schmitz, N. Perceived needs for and use of workplace accommodations by individuals with a depressive and/or anxiety disorder. J. Occup. Environ. Med. 2011, 53, 1268–1272. [Google Scholar] [CrossRef] [PubMed]
- Mellifont, D.; Smith-Merry, J.; Scanlan, J.N. Disabling Accommodation Obstacles: A Study Exploring Accommodations That Can Assist Government Employees with Anxiety Disorders; Centre for Disability Research and Policy, The University of Sydney: Camperdown, Australia, 2016. [Google Scholar]
- Pischel, S.; Felfe, J. “Should I tell my leader or not?”—Health-oriented leadership and stigma as antecedents of employees’ mental health information disclosure intentions at work. J. Occup. Environ. Med. 2023, 65, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Nevala, N.; Pehkonen, I.; Koskela, I.; Ruusuvuori, J.; Anttila, H. Workplace accommodation among persons with disabilities: A systematic review of its effectiveness and barriers or facilitators. J. Occup. Rehabil. 2015, 25, 432–448. [Google Scholar] [CrossRef]
- Dewa, C.S.; van Weeghel, J.; Joosen, M.C.W.; Brouwers, E. What could influence workers’ decisions to disclose a mental illness at work? Int. J. Occup. Environ. Med. 2020, 11, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Brohan, E.; Henderson, C.; Wheat, K.; Malcolm, E.; Clement, S.; Barley, E.; Slade, M.; Thornicroft, G. Systematic review of beliefs, behaviours and influencing factors associated with disclosure of a mental health problem in the workplace. BMC Psychiatry 2012, 12, 11. [Google Scholar] [CrossRef]
- MacDonald-Wilson, K.L.; Russinova, Z.; Rogers, E.S.; Lin, C.H.; Ferguson, T.; Dong, S.; Kash-MacDonald, M. Disclosure of mental health disabilities in the workplace. In Work Accommodation and Retention in Mental Health, 1st ed.; Schultz, I.Z., Rogers, E.S., Eds.; Springer: New York, NY, USA, 2011; pp. 191–218. [Google Scholar]
- Minister of Labour. Canada Labour Code; Minister of Labour: Ottawa, ON, Canada, 1985.
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Osman, A.; Bagge, C.L.; Gutierrez, P.M.; Konick, L.C.; Kopper, B.A.; Barrios, F.X. The suicidal behaviors questionnaire-revised (SBQ-R):Validation with clinical and nonclinical samples. Assessment 2001, 8, 443–454. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 672–677. [Google Scholar] [CrossRef]
- Donohue, M. Longpower: Power and Sample Size Calculations for Linear Mixed Models. 2021. Available online: https://cran.r-project.org/web/packages/longpower/longpower.pdf (accessed on 12 January 2023).
- Diggle, P.J.; Heagerty, P.J.; Liang, K.Y.; Zeger, S.L. Analysis of Longtudinal Data, 2nd ed.; Oxford Statistical Science Series; Oxford University Press: Oxford, UK, 2002. [Google Scholar]
- Liu, G.; Liang, K.Y. Sample size calculations for studies with correlated observations. Biometrics 1997, 53, 937–947. [Google Scholar] [CrossRef]
- Lu, K.; Luo, X.; Chen, P. Sample size estimation for repeated measures analysis in randomized clinical trial with missing data. Int. J. Biostat. 2008, 4, 937–947. [Google Scholar] [CrossRef]
- Joyce, S.; Modini, M.; Christensen, H.; Mykletun, A.; Bryant, R.; Mitchell, P.B.; Harvey, S.B. Workplace interventions for common mental disorders: A systematic meta-review. Psychol. Med. 2016, 46, 683–697. [Google Scholar] [CrossRef]
- Sundram, B.M.; Dahlui, M.; Chinna, K. Effectiveness of progressive muscle relaxation therapy as a worksite health promotion program in the automobile assembly line. Ind. Health 2016, 54, 204–214. [Google Scholar] [CrossRef] [PubMed]
- Krajewski, J.; Wieland, R.; Sauerland, M. Regulating strain states by using the recovery potential of lunch breaks. J. Occup. Health Psychol. 2010, 15, 131. [Google Scholar] [CrossRef] [PubMed]
- Dimoff, J.K.; Kelloway, E.K.; Burnstein, M.D. Mental Health Awareness Training (MHAT): The development and evaluation of an intervention for workplace leaders. Int. J. Stress Manag. 2016, 23, 167–189. [Google Scholar] [CrossRef]
- Corrigan, P.W.; Michaels, P.J.; Vega, E.; Gause, M.; Watson, A.C.; Rüsch, N. Self-stigma of mental illness scale—Short form: Reliability and validity. Psychiatry Res. 2012, 199, 65–69. [Google Scholar] [CrossRef]
- Biggs, D.M.; Swailes, S.; Baker, S. The measurement of worker relations: The development of a three-component scale. Leadersh. Organ. Dev. J. 2016, 37, 2–12. [Google Scholar] [CrossRef]
- Kessler, R.C.; Barber, D.C.; Beck, B.A.; Berglund, B.P.; Cleary, B.P.; McKenas, B.D.; Pronk, B.N.; Simon, B.G.; Stang, B.P.; Ustun, B.T.; et al. The World Health Organization health and work performance questionnaire (HPQ). J. Occup. Environ. Med. 2003, 45, 156–174. [Google Scholar] [CrossRef]
- Kessler, R.C. News Notes: The Clinical Trials Version of the HPQ; Department of Health Care Policy, Harvard Medical School: Boston, MA, USA, 2002; p. 2. [Google Scholar]
- Chen, G.; Gully, S.M.; Eden, D. Validation of a new general self-efficacy scale. Organ. Res. Methods 2001, 4, 62–83. [Google Scholar] [CrossRef]
- Scherbaum, C.A.; Cohen-Charash, Y.; Kern, M.J. Measuring general self-efficacy: A comparison of three measures using item response theory. Educ. Psychol. Meas. 2006, 66, 1047–1063. [Google Scholar] [CrossRef]
- Tucker, S.; Johnson, A. Employability Study; University of Regina: Regina, SK, Canada, 2019. [Google Scholar]
- Nishii, L. The benefits of climate of inclusion for gender-diverse groups. Acad. Manag. J. 2013, 56, 1754–1774. [Google Scholar] [CrossRef]
- Rüsch, N.; Brohan, E.; Gabbidon, J.; Thornicroft, G.; Clement, S. Stigma and disclosing one’s mental illness to family and friends. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 1157. [Google Scholar] [CrossRef] [PubMed]
- Munir, F.; Leka, S.; Griffiths, A. Dealing with self-management of chronic illness at work: Predictors for self-disclosure. Soc. Sci. Med. 2005, 60, 1397–1407. [Google Scholar] [CrossRef]
- Levis, B.; Benedetti, A.; Thombs, B.D. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: Individual participant data meta-analysis. BMJ 2019, 365, l1476. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.M.D.; Spitzer, R.L.M.D.; Williams, J.B.W.D.S.W.; Löwe, B.M.D.P.D. The patient health questionnaire somatic, anxiety, and depressive symptom scales: A systematic review. Gen. Hosp. Psychiatry 2010, 32, 345–359. [Google Scholar] [CrossRef] [PubMed]
- Decker, J.T.; Aarestad, D.; Elliott, W.; Lowe, C. Chemical sensitivity in the workplace. J. Soc. Work Disabil. Rehabil. 2002, 1, 45–61. [Google Scholar] [CrossRef]
- Peters, L.; Rapee, R.M.; Sunderland, M.; Andrews, G.; Mattick, R.P. Development of a short form social interaction anxiety (SIAS) and social phobia scale (SPS) using nonparametric item response theory: The SIAS-6 and the SPS-6. Psychol. Assess. 2012, 24, 66–76. [Google Scholar] [CrossRef]
- Liang, K.-Y.; Zeger, S.L. Longitudinal data analysis using generalized linear models. Biometrika 1986, 73, 13–22. [Google Scholar] [CrossRef]
- Karin, E.; Dear, B.F.; Heller, G.Z.; Gandy, M.; Titov, N. Measurement of symptom change following web-based psychotherapy: Statistical characteristics and analytical methods for measuring and interpreting change. JMIR Ment. Health 2018, 5, e10200. [Google Scholar] [CrossRef]
- Gupta, S.K. Intention-to-treat concept: A review. Perspect. Clin. Res. 2011, 2, 109–112. [Google Scholar] [CrossRef]
- Peng, A.C.; Schaubroeck, J.M.; Xie, J.L. When confidence comes and goes: How variation in self-efficacy moderates stressor–strain relationships. J. Occup. Health Psychol. 2015, 20, 359. [Google Scholar] [CrossRef] [PubMed]
- Deady, M.; Collins, D.; Johnston, D.; Glozier, N.; Calvo, R.; Christensen, H.; Harvey, S. The impact of depression, anxiety and comorbidity on occupational outcomes. Occup. Med. 2022, 72, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Pohling, R.; Buruck, G.; Jungbauer, K.-L.; Leiter, M.P. Work-related factors of presenteeism: The mediating role of mental and physical health. J. Occup. Health Psychol. 2016, 21, 220. [Google Scholar] [CrossRef]
- Dimoff, J.K.; Kelloway, E.K. Resource utilization model: Organizational leaders as resource facilitators. In The Role of Leadership in Occupational Stress (Research in Occupational Stress and Well-Being); Gentry, W.A., Clerkin, C., Perrewe, P.L., Halbesleben, J.R.B., Rosen, C.C., Eds.; Emerald Group Publishing Limited: Bingley, UK, 2016; Volume 14, pp. 141–160. [Google Scholar]
- Kim, J.; De Dear, R. Workspace satisfaction: The privacy-communication trade-off in open-plan offices. J. Environ. Psychol. 2013, 36, 18–26. [Google Scholar] [CrossRef]
- Samani, S.A. The impact of personal control over office workspace on environmental satisfaction and performance. J. Soc. Sci. Humanit. 2015, 1, 163–175. [Google Scholar]
- Tavares, A.I. Telework and health effects review. Int. J. Healthc. 2017, 3, 30–36. [Google Scholar] [CrossRef]
- Tulk, C.; Mantler, J.; Dupré, K.E. The impact of job accommodations on stereotyping and emotional responses to coworkers with anxiety or depression. Can. J. Behav. Sci. 2021, 53, 138–151. [Google Scholar] [CrossRef]
- McCall, H.C.; Hadjistavropoulos, H.D.; Sundström, C.R.F. Exploring the role of persuasive design in unguided Internet-delivered cognitive behavioral therapy for depression and anxiety among adults: Systematic review, meta-analysis, and meta-regression. J. Med. Internet Res. 2021, 23, e26939. [Google Scholar] [CrossRef]
- Hadjistavropoulos, H.D.; Faller, Y.N.; Klatt, A.; Nugent, M.N.; Dear, B.F.; Titov, N. Patient perspectives on strengths and challenges of therapist-assisted internet-delivered cognitive behaviour therapy: Using the patient voice to improve care. Community Ment. Health J. 2018, 54, 944–950. [Google Scholar] [CrossRef] [PubMed]
- Memish, K.B.; Martin, A.P.; Bartlett, L.B.; Dawkins, S.P.; Sanderson, K.P. Workplace mental health: An international review of guidelines. Prev. Med. 2017, 101, 213–222. [Google Scholar] [CrossRef]
- Dewa, C.S.; Trojanowski, L.; Joosen, M.C.W.; Bonato, S. Employer Best Practice Guidelines for the Return to Work of Workers on Mental Disorder-Related Disability Leave: A Systematic Review. Can. J. Psychiatry 2016, 61, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Mental Health Commission of Canada [MHCC]. Making the Case for Investing in Mental Health in Canada; Mental Health Commission of Canada [MHCC]: Ottawa, ON, Canada, 2013. [Google Scholar]


{kind=link}
| Variable | All Participants (n = 77) | Course (n = 41) | Wait-List Control (n = 36) | Statistical Significance | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Participant pre-treatment characteristics | |||||||
| Age | |||||||
| Mean (SD) | 43.84 (10.64) | - | 44.62 (9.66) | - | 43.0 (11.68) | - | t(75) = 0.66, p = 0.52 |
| Range | 20–63 | - | 26–60 | - | 20–63 | - | |
| Gender | |||||||
| Female | 60 | 77.9 | 31 | 75.6 | 29 | 80.6 | χ2 (2) = 0.11, p = 0.61 |
| Male | 16 | 20.8 | 9 | 22.0 | 7 | 19.4 | |
| Two-Spirit | 1 | 1.3 | 1 | 2.4 | 0 | 0 | |
| Ethnicity | |||||||
| European | 59 | 76.6 | 30 | 73.2 | 29 | 80.6 | χ2 (1) = 0.24 p = 0.62 |
| Indigenous, Métis, Caribbean, East Asian, Latin American, Not Listed | 18 | 23.4 | 11 | 26.8 | 7 | 19.4 | |
| Employment characteristics | |||||||
| Employment status | |||||||
| Employed full/part time | 51 | 76.3 | 29 | 72.5 | 29 | 80.6 | χ2 (1) = 0.31; p = 0.58 |
| Disability Leave | 18 | 23.7 | 11 | 27.5 | 7 | 19.4 | |
| Position | |||||||
| Executive/senior manager | 19 | 24.7 | 13 | 31.7 | 6 | 16.7 | χ2 (3) = 5.72; p = 0.13 |
| Professional (engineer, analyst) | 20 | 26.0 | 8 | 19.6 | 12 | 33.3 | |
| Technical/administrative support | 22 | 28.5 | 14 | 34.1 | 8 | 22.2 | |
| Sales, service, labourer | 16 | 20.8 | 6 | 14.6 | 10 | 27.8 | |
| Company Size | |||||||
| 1–99 employees | 46 | 59.7 | 25 | 61.0 | 21 | 59.7 | χ2 (2) = 0.09; p = 0.96 |
| 100–499 employees | 16 | 20.8 | 8 | 19.5 | 8 | 20.8 | |
| Over 500 employees | 15 | 19.5 | 8 | 19.5 | 7 | 19.5 | |
| Work functioning (last 28 days) | |||||||
| Full day absent mean (SD) | 5.61 (9.92) | 6.95 (11.26) | 4.08 (8.01) | t(75) = 1.29; p = 0.19 | |||
| Partial days absent mean (SD) | 3.52 (8.27) | 4.68 (9.47) | 2.19 (6.53) | t(75) = 1.36; p = 0.18 | |||
| Performance mean (SD) | 56.49 (24.64) | 53.90 (23.65) | 59.44 (25.74) | t(75) = 0.98; p = 0.33 | |||
| Mental health characteristics | |||||||
| Duration of depression concerns | |||||||
| 0–6 months | 19 | 24.7 | 12 | 29.3 | 7 | 19.4 | χ2 (2) = 1.11; p = 0.58 |
| 7–12 months | 11 | 14.3 | 6 | 14.6 | 5 | 13.9 | |
| >1 year | 47 | 61.0 | 23 | 56.12 | 24 | 66.7 | |
| Duration of anxiety concerns | |||||||
| 0–6 months | 14 | 18.2 | 9 | 22.0 | 5 | 18.2 | χ2 (2) = 1.02; p = 0.60 |
| 7–12 months | 5 | 6.5 | 3 | 7.3 | 2 | 5.5 | |
| >1 year | 58 | 75.3 | 29 | 70.7 | 29 | 75.3 | |
| Pre-treatment symptom scores | |||||||
| PHQ-9 mean (SD) | 12.77 (5.53) | 12.71 (5.67) | 12.83 (5.50) | t(75) = 0.09; p = 0.92 | |||
| GAD-7 mean (SD) | 10.86 (4.54) | 10.51 (4.70) | 11.25 (4.38) | t(75) = 0.71; p = 0.48 | |||
| SPS-6 mean (SD) | 5.64 (5.21) | 5.44 (5.39) | 5.86 (5.07) | t(75) = 0.35; p = 0.72 | |||
| SIAS-6 mean (SD) | 8.47 (5.64) | 8.19 (5.99) | 8.78 (5.29) | t(75) = 0.45; p = 0.65 | |||
| Estimated Marginal Means | Percentage Reductions from Pre-Treatment | ||||
|---|---|---|---|---|---|
| Pre-Treatment | 4-Week Follow-up | 8-Week Follow-up | to 4-Week Follow-up | to 8-Week Follow-up | |
| AccoKnow a | |||||
| Course | 4.63 (3.29) | 6.53 (2.38) | 6.92 (2.12) | −40 [−57, −22] | −47 [−62, −32] |
| Wait-list Control | 3.47 (2.81) | 3.66 (2.42) | 3.83 (2.51) | −6 [−29, 17] | −11 [−34, 13] |
| SSMIS (Aware) b | |||||
| Course | 17.68 (9.85) | 15.81 (9.15) | 20.45 (11.98) | 11 [−7, 29] | −16 [−39, 8] |
| Wait-list Control | 23.83 (10.32) | 25.08 (10.49) | 26.28 (11.08) | −5 [−20, 9] | −10 [−26, 5] |
| SSMIS (Agree) b | |||||
| Course | 12.12 (6.64) | 11.89 (6.95) | 12.29 (8.01) | 2 [−18, 22] | −1 [−24, 21] |
| Wait-list Control | 15.47 (8.72) | 12.96 (6.69) | 15.01 (7.57) | 16 [2, 30] | 3 [−13, 19] |
| SSMIS (Apply) b | |||||
| Course | 13.02 (6.04) | 12.43 (6.92) | 12.08 (6.46) | 5 [−12, 22] | 7 [−9, 23] |
| Wait-list Control | 15.78 (8.51) | 14.63 (7.14) | 14.95 (6.36) | 7 [−7, 22] | 5 [−8, 19] |
| SSMIS (Hurts) b | |||||
| Course | 14.12 (7.82) | 11.45 (7.20) | 12.04 (8.75) | 19 [3, 35] | 15 [−5, 34] |
| Wait-list Control | 16.78 (9.03) | 14.49 (8.58) | 14.39 (7.77) | 14 [−3, 30] | 14 [−1, 30] |
| WRS b | |||||
| Course | 40.10 (12.66) | 39.86 (11.40) | 38.82 (10.82) | 1 [−9, 10] | 3 [−5, 11] |
| Wait-list Control | 39.75 (11.11) | 39.63 (9.99) | 40.19 (9.88) | 0 [−8, 8] | −1 [−9, 7] |
| WHOHPQ (PD) b | |||||
| Course | 3.80 (7.02) | 3.51 (6.96) | 2.98 (7.18) | 8 [−55, 71] | 22 [−44, 87] |
| Wait-list Control | 2.19 (6.53) | 4.49 (9.57) | 2.71 (8.13) | −104 [−249, 40] | −23 [−148, 101] |
| WHOHPQ (Pre) a | |||||
| Course | 53.90 (23.65) | 55.20 (26.37) | 62.24 (20.46) | −2 [−18, 13] | −15 [−29, −2] |
| Wait-list Control | 59.44 (25.74) | 56.20 (26.79) | 55.08 (27.28) | 5 [−9, 20] | 7 [−7, 22] |
| NGSE a | |||||
| Course | 3.29 (0.74) | 3.51 (0.70) | 3.73 (0.66) | −8 [−15, −1] | −13 [−20, −6] |
| Wait-list Control | 3.43 (0.73) | 3.49 (0.69) | 3.49 (0.68) | −2 [−8, 4] | −2 [−8, 5] |
| DISC (Comfort Full) a | |||||
| Course | 2.59 (0.89) | 2.71 (0.75) | 2.80 (0.79) | −5 [−14, 4] | −8 [−18, 2] |
| Wait-list Control | 2.36 (0.87) | 2.54 (0.79) | 2.43 (0.91) | −7 [−18, 4] | −3 [−15, 10] |
| DISC (Comfort Partial) a | |||||
| Course | 2.29 (0.75) | 2.54 (072) | 2.53 (0.78) | −11 [−22, 0] | −10 [−21, 1] |
| Wait-list Control | 2.42 (0.87) | 2.57 (0.71) | 2.66 (0.85) | −6 [−16, 3] | −10 [−22, 1] |
| DISC (Rate) a | |||||
| Course | 2.05 (0.71) | 2.16 (0.66) | 2.35 (0.54) | −5 [−16, 5] | −15 [−24, −6] |
| Wait-list Control | 2.11 (0.57) | 2.10 (0.67) | 2.17 (0.64) | 0 [−10, 11] | −3 [−13, 7] |
| PHQ-9 b | |||||
| Course | 12.71 (5.67) | 9.31 (5.98) | 9.08 (7.26) | 27 [12, 42] | 29 [11, 46] |
| Wait-list Control | 12.83 (5.46) | 9.44 (4.86) | 9.70 (5.03) | 26 [14, 39] | 24 [12, 37] |
| GAD-7 b | |||||
| Course | 10.51 (4.70) | 7.58 (4.29) | 7.54 (5.97) | 28 [14, 41] | 28 [10, 47] |
| Wait-list Control | 11.25 (4.38) | 8.40 (5.12) | 9.40 (5.00) | 25 [10, 40] | 16 [2, 31] |
| SPS-6 b | |||||
| Course | 5.44 (5.39) | 4.83 (6.05) | 4.92 (6.01) | 11 [−22, 45] | 10 [−24, 43] |
| Wait-list Control | 5.86 (5.07) | 6.11 (5.91) | 5.94 (5.20) | −4 [−37, 29] | −1 [−32, 29] |
| SIAS-6 b | |||||
| Course | 8.20 (5.99) | 6.96 (5.97) | 7.23 (6.28) | 15 [−7, 37] | 11 [−12, 35] |
| Wait-list Control | 8.78 (5.29) | 8.36 (5.96) | 8.55 (5.67) | 5 [−18, 27] | 3 [−18, 24] |
| Within-Group Effect Sizes from Pre-Treatment | Between-Group Effect Size | |||
|---|---|---|---|---|
| to 4-Week Follow-up | to 8-Week Follow-up | at 4-Week Follow-up | at 8-Week Follow-up | |
| AccoKnow | ||||
| Course | −0.65 [−1.09, −0.20] | −0.81 [−1.26, −0.36] | 1.17 [0.69, 1.66] | 1.31 [0.82, 1.80] |
| Wait-list Control | −0.07 [−0.53, 0.39] | −0.13 [−0.60, 0.33] | ||
| SSMIS (Aware) | ||||
| Course | 0.19 [−0.24, 0.63] | −0.25 [−0.68, 0.19] | −0.93 [−1.40, −0.46] | −0.49 [−0.95, −0.04] |
| Wait-list Control | −0.12 [−0.58, 0.35] | −0.22 [−0.69, 0.24] | ||
| SSMIS (Agree) | ||||
| Course | 0.03 [−0.40, 0.47] | −0.02 [−0.46, 0.41] | −0.15 [−0.60, 0.29] | −0.34 [−0.79, 0.11] |
| Wait-list Control | 0.32 [−0.15, 0.78] | 0.06 [−0.41, 0.52] | ||
| SSMIS (Apply) | ||||
| Course | 0.09 [−0.34, 0.52] | 0.15 [−0.28, 0.58] | −0.31 [−0.76, 0.14] | −0.44 [−0.89, 0.01] |
| Wait-list Control | 0.14 [−0.32, 0.61] | 0.11 [−0.35, 0.57] | ||
| SSMIS (Hurts) | ||||
| Course | 0.35 [−0.09, 0.78] | 0.25 [−0.19, 0.68] | −0.38 [−0.83, 0.07] | −0.28 [−0.73, 0.17] |
| Wait-list Control | 0.25 [−0.21, 0.72] | 0.28 [−0.19, 0.74] | ||
| WRS | ||||
| Course | 0.02 [−0.41, 0.45] | 0.11 [−0.33, 0.54] | 0.02 [−0.43, 0.47] | −0.13 [−0.58, 0.32] |
| Wait-list Control | 0.01 [−0.45, 0.47] | −0.04 [−0.50, 0.42] | ||
| WHOHPQ (PD) | ||||
| Course | 0.04 [−0.39, 0.47] | 0.11 [−0.32, 0.55] | −0.12 [−0.56, 0.33] | 0.04 [−0.41, 0.48] |
| Wait-list Control | −0.27 [−0.74, 0.19] | −0.07 [−0.53, 0.39] | ||
| WHOHPQ (Pre) | ||||
| Course | −0.05 [−0.48, 0.38] | −0.37 [−0.81, 0.07] | −0.04 [−0.48, 0.41] | 0.29 [−0.16, 0.74] |
| Wait-list Control | 0.12 [−0.34, 0.58] | 0.16 [−0.30, 0.62] | ||
| NGSE | ||||
| Course | −0.29 [−0.73, 0.14] | −0.62 [−1.06, −0.17] | 0.02 [−0.42, 0.47] | 0.35 [−0.10, 0.80] |
| Wait-list Control | −0.08 [−0.54, 0.38] | −0.09 [−0.55, 0.37] | ||
| DISC (Comfort Full) | ||||
| Course | −0.15 [−0.59, 0.28] | −0.25 [−0.68, 0.19] | 0.23 [−0.22, 0.68] | 0.43 [−0.02, 0.88] |
| Wait-list Control | −0.21 [−0.67, 0.26] | −0.07 [−0.54, 0.39] | ||
| DISC (Comfort Partial) | ||||
| Course | −0.33 [−0.77, 0.11] | −0.30 [−0.74, 0.13] | −0.04 [−0.49, 0.40] | −0.16 [−0.61, 0.29] |
| Wait-list Control | −0.19 [0.66, 0.27] | −0.28 [−0.75, 0.18] | ||
| DISC (Rate) | ||||
| Course | −0.16 [−0.59, 0.28] | −0.47 [−0.91, −0.04] | 0.08 [−0.37, 0.53] | 0.30 [−0.15, 0.75] |
| Wait-list Control | 0.01 [−0.45, 0.47] | −0.10 [−0.56, 0.36] | ||
| PHQ-9 | ||||
| Course | 0.57 [0.13, 1.01] | 0.55 [0.11, 0.99] | −0.02 [−0.47, 0.42] | −0.10 [−0.54, 0.35] |
| Wait-list Control | 0.64 [0.17, 1.12] | 0.58 [0.11, 1.06] | ||
| GAD-7 | ||||
| Course | 0.64 [0.20, 1.08] | 0.54 [0.10, 0.98] | −0.17 [−0.62, 0.28] | −0.33 [−0.78, 0.12] |
| Wait-list Control | 0.59 [0.11, 1.06] | 0.38 [−0.08, 0.85] | ||
| SPS-6 | ||||
| Course | 0.10 [−0.33, 0.54] | 0.09 [−0.34, 0.52] | −0.21 [−0.66, 0.24] | −0.18 [−0.63, 0.27] |
| Wait-list Control | −0.04 [−0.51, 0.42] | −0.01 [−0.48, 0.45] | ||
| SIAS-6 | ||||
| Course | 0.20 [−0.23, 0.64] | 0.15 [−0.28, 0.58] | −0.23 [−0.68, 0.22] | −0.21 [−0.66, 0.24] |
| Wait-list Control | 0.07 [−0.39, 0.53] | 0.04 [−0.42, 0.50] | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faller, Y.N.; Peynenburg, V.; Tessier, E.; Thiessen, D.; Hadjistavropoulos, H.D. Efficacy of an Online Workplace Mental Health Accommodations Psychoeducational Course: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2023, 20, 5317. https://doi.org/10.3390/ijerph20075317
Faller YN, Peynenburg V, Tessier E, Thiessen D, Hadjistavropoulos HD. Efficacy of an Online Workplace Mental Health Accommodations Psychoeducational Course: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2023; 20(7):5317. https://doi.org/10.3390/ijerph20075317
Chicago/Turabian StyleFaller, Yvonne Nichole, Vanessa Peynenburg, Eric Tessier, David Thiessen, and Heather D. Hadjistavropoulos. 2023. "Efficacy of an Online Workplace Mental Health Accommodations Psychoeducational Course: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 20, no. 7: 5317. https://doi.org/10.3390/ijerph20075317
APA StyleFaller, Y. N., Peynenburg, V., Tessier, E., Thiessen, D., & Hadjistavropoulos, H. D. (2023). Efficacy of an Online Workplace Mental Health Accommodations Psychoeducational Course: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 20(7), 5317. https://doi.org/10.3390/ijerph20075317