
Experiences of Non-Pharmaceutical Primary Care Interventions for Common Mental Health Disorders in Socioeconomically Disadvantaged Groups: A Systematic Review of Qualitative Studies

 , , , , , , , and
, , , , , , , and
Abstract
1. Introduction
2. Methods
2.1. Search Strategy and Data Sources
2.2. Screening and Selection
2.3. Data Extraction and Quality Appraisal
2.4. Thematic Synthesis
3. Results
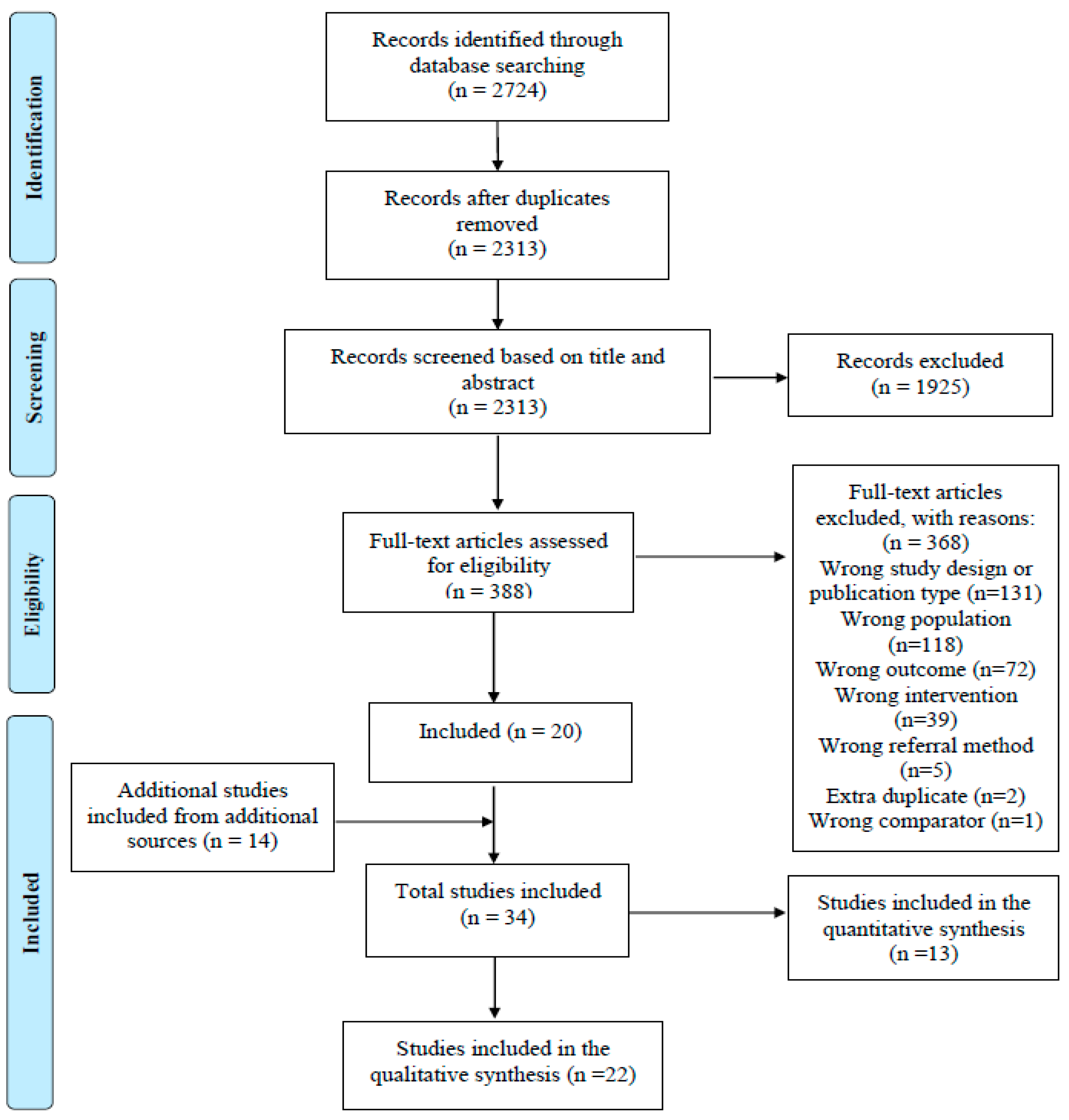
3.1. Findings from Systematic Searches
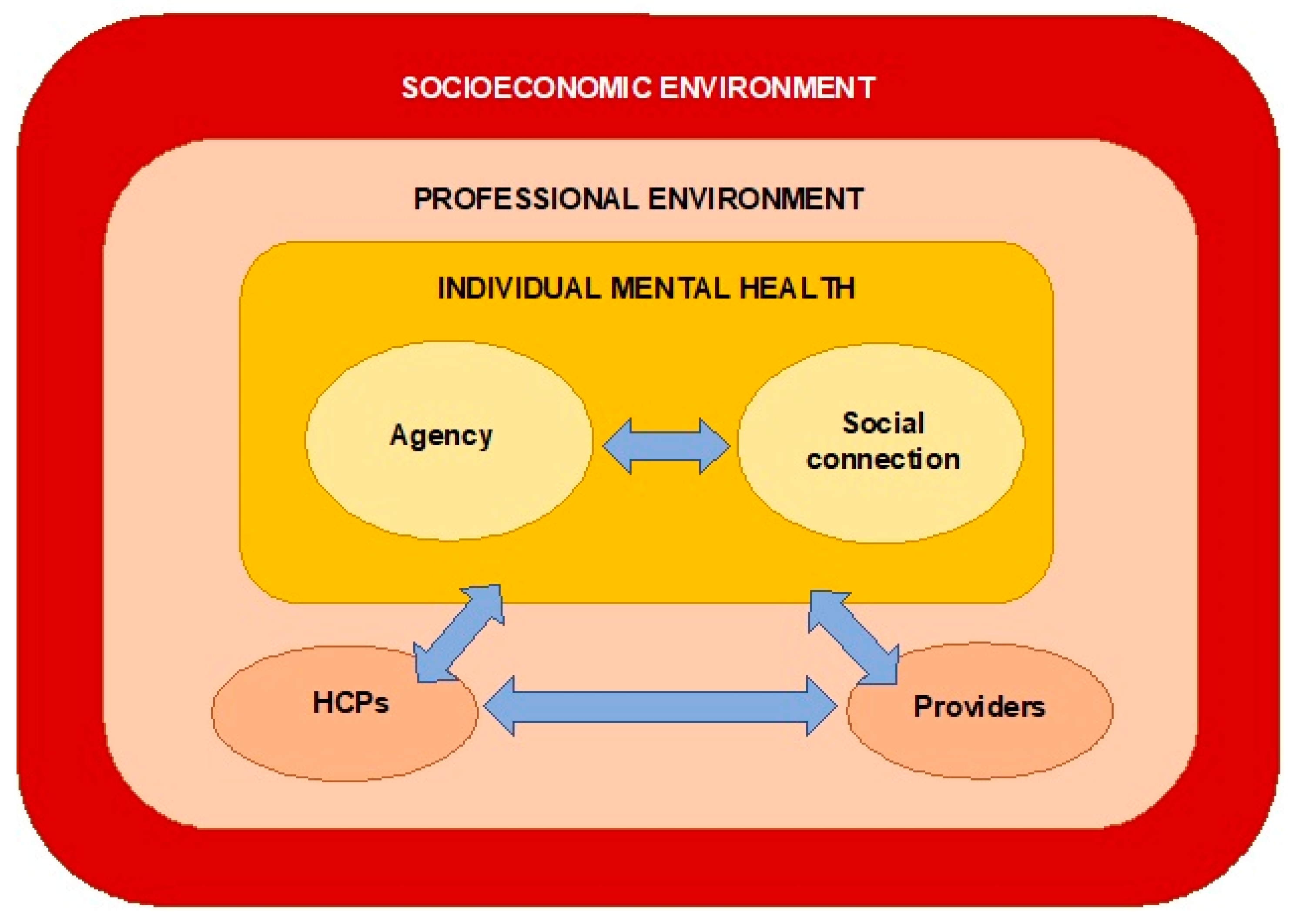
3.2. Findings from Thematic Analysis
- Agency
- Social connections
- Socioeconomic environment
3.2.1. Theme 1: Agency
Sense of Control and Choice
“You can come in here [community hub—LifeRooms] for say 10 minutes, 20 minutes, half an hour… you are in charge of what you’re doing. I think it’s really really important and just that little bit of control can make you feel on top of the world”.[45]
“Being able to take an active role in decision making was contrasted with interactions with HCPs that often felt more prescriptive and less collaborative”.
Confidence, Motivation and Purpose
Understanding of Health and Self-Management
Functioning and Achieving Goals
Health Conditions
“You get the days where you are feeling dead down and you can’t be bothered…There are things I want to do, but over these last few months I just haven’t had the energy.”.[58]
Lack of Awareness
3.2.2. Theme 2: Social Connections
Information Sharing
“I think it’s a good idea that they should know that you’ve got a bit of depression because when I go in there and she says your blood sugar, I said well, I’ve been a bad boy, I’ve eaten this, that and the other, she shouldn’t start saying, oh, what are you doing that for?”.[47]
Positive Relationships
“Another thing that I find for which I’m very grateful and surprised is how understanding people here are. It’s about one of the very few places that I feel welcome and respected as I am”.[39]
“It’s very much more acceptable for our patients to see someone regarding mood at the practice as opposed to going externally to see a counsellor… more acceptable when it’s seen to be the nurse… People like to hang hooks on names, patients don’t generally go round talking about their depression, but you do hear them going around all the time talking about their diabetes or angina or whatever”.[56]
Difficulties in Relationships with Providers
“My first worker left, I used to see her a lot. I was put onto another one… Now she’s left and they’ve put me onto somebody else who I’ve never seen…I just feel as though I’ve been let down… pushed to one side”.[58]
3.2.3. Theme 3: Socioeconomic Environment
Help with Social Needs
“Whatever money I owed like electricity and TV licence was in my mind always eating me from inside. I sorted out that and it just changed so many things … It changed my attitude, it changed my behaviour and it changed my mood … I am not depressed like before”.[49]
“My consultation had to move away from this sort of biomedical model of depression…and see the patient a bit more in the wider family and community… Talk about appetite or sleep leads quite smoothly to antidepressants and sleeping tablets but doesn’t move to social prescribing… So I had to change my consultation style … I find it easier now”.[42]
Socioeconomic Deprivation
“Now there is a big drive to get people off benefits—rightly or wrongly—so they are reluctant to go anywhere where it says Job Centre Plus. I think they (patients) saw a little bit of similarity between social prescribing and Discover Opportunities and that put the brakes on”.[42]
Social Needs beyond HCP Capacity
Feeling Failed by the System
“There’s nobody for the likes o’ me. You’re just left tae, I don’t know, vegetate… No, the system’s totally wrong… As I say, they told me… “You’ll never work again.” So, where do you get the hope fae? Where dae you get the faith fae?”.[44]
Sustainability and Funding
“I’m seeing more and more of the time, the resources demand, the stretch on organisations in terms of the amount of people that seem to be getting referred to these organisations now. And I think potentially the quality of service of these organisations could suffer”.[55]
3.2.4. Interactions between Themes
4. Discussion
4.1. Strengths and Limitations
4.2. Implications
- If existing inequalities are to be seriously addressed, the experiences of those living with socioeconomic disadvantage must become a central part of decision-making processes.
- For interventions to be effective, the community sector organisations they rely upon need to be adequately and sustainably funded., This is likely to require pressure on policy makers to provide sustained funding for community organisations that provide non-pharmaceutical primary care interventions for CMDs.
- Raising awareness of non-pharmaceutical interventions among both healthcare professionals and service users is likely to be beneficial for engagement and implementation.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mind. Mental Health in Primary Care: A Briefing for Clinical Commissioning Groups; Mind: London, UK, 2016. [Google Scholar]
- Kendrick, T.; Burns, T.; Garland, C.; Greenwood, N.; Smith, P. Are specialist mental health services being targeted on the most needy patients? The effects of setting up special services in general practice. Br. J. Gen. Pract. 2000, 50, 121–126. [Google Scholar] [PubMed]
- Reilly, S.; Planner, C.; Hann, M.; Reeves, D.; Nazareth, I.; Lester, H. The role of primary care in service provision for people with severe mental illness in the United Kingdom. PLoS ONE 2012, 7, e36468. [Google Scholar] [CrossRef] [PubMed]
- Sundquist, J.; Ohlsson, H.; Sundquist, K.; Kendler, K.S. Common adult psychiatric disorders in Swedish primary care where most mental health patients are treated. BMC Psychiatry 2017, 17, 235. [Google Scholar] [CrossRef] [PubMed]
- WHO. Social Determinants of Mental Health; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Jenkins, R.; Bhugra, D.; Bebbington, P.; Brugha, T.; Farrell, M.; Coid, J.; Fryers, T.; Weich, S.; Singleton, N.; Meltzer, H. Debt, income and mental disorder in the general population. Psychol. Med. 2008, 38, 1485–1493. [Google Scholar] [CrossRef]
- Fryers, T.; Melzer, D.; Jenkins, R.; Brugha, T. The distribution of the common mental disorders: Social inequalities in Europe. Clin. Pract. Epidemiol. Ment. Health 2005, 1, 14. [Google Scholar] [CrossRef]
- McManus, S.; Bebbington, P.; Jenkins, R.; Brugha, T. Mental Health and Wellbeing in England: Adult Psychiatric Morbidity Survey 2014; NHS Digital: Leeds, UK, 2014. [Google Scholar]
- Allen, J.; Balfour, R.; Bell, R.; Marmot, M. Social determinants of mental health. Int. Rev. Psychiatry 2014, 26, 392–407. [Google Scholar] [CrossRef]
- Hodgson, K.; Stafford, M.; Fisher, R.; Docherty, M.; Deeny, S. Inequalities in Health Care for People with Depression and/or Anxiety; The Health Foundation UK: London, UK, 2020. [Google Scholar]
- Shaw, I.; Woodward, L. The medicalisation of unhappiness? The management of mental distress in primary care. In Constructions of Health and Illness; Routledge: London, UK, 2017; pp. 124–136. [Google Scholar]
- Mills, C. Decolonizing Global Mental Health: The Psychiatrization of the Majority World; Routledge: New York, NY, USA, 2014. [Google Scholar]
- Spence, R.; Roberts, A.; Ariti, C.; Bardsley, M. Focus On: Antidepressant Prescribing; The Health Foundation & Nuffield Trust: London, UK, 2014. [Google Scholar]
- Bogowicz, P.; Curtis, H.J.; Walker, A.J.; Cowen, P.; Geddes, J.; Goldacre, B. Trends and variation in antidepressant prescribing in English primary care. BJGP Open 2021, 5. [Google Scholar] [CrossRef]
- Mills, C. The Psychiatrization of Poverty: Rethinking the Mental Health-Poverty Nexus. Soc. Personal. Psychol. Compass 2015, 9, 213–222. [Google Scholar] [CrossRef]
- Walters, P.; Ashworth, M.; Tylee, A. Ethnic density, physical illness, social deprivation and antidepressant prescribing in primary care: Ecological study. Br. J. Psychiatry 2008, 193, 235–239. [Google Scholar] [CrossRef][Green Version]
- Gopfert, A.; Deeny, S.R.; Fisher, R.; Stafford, M. Primary care consultation length by deprivation and multimorbidity in England: An observational study using electronic patient records. Br. J. Gen. Pract. 2021, 71, e185–e192. [Google Scholar] [CrossRef]
- Hodgson, K. Inequalities in English NHS Talking Therapy Services: What Can the Data Tell Us?: Examining NHS Digital Annual Reports to Look at Deprivation; The Health Foundation: London, UK, 2019. [Google Scholar]
- Wakefield, S.; Kellett, S.; Simmonds-Buckley, M.; Stockton, D.; Bradbury, A.; Delgadillo, J. Improving Access to Psychological Therapies (IAPT) in the United Kingdom: A systematic review and meta-analysis of 10-years of practice-based evidence. Br. J. Clin. Psychol. 2021, 60, 1–37. [Google Scholar] [CrossRef] [PubMed]
- Jonker, L.; Thwaites, R.; Fisher, S. Patient referral from primary care to psychological therapy services: A cohort study. Fam. Pract. 2020, 37, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Drinkwater, C.; Wildman, J.; Moffatt, S. Social prescribing. BMJ 2019, 364, l1285. [Google Scholar] [CrossRef] [PubMed]
- Husk, K.; Blockley, K.; Lovell, R.; Bethel, A.; Lang, I.; Byng, R.; Garside, R. What approaches to social prescribing work, for whom, and in what circumstances? A realist review. Health Soc. Care Community 2020, 28, 309–324. [Google Scholar] [CrossRef]
- Brown, R.C.H.; Mahtani, K.; Turk, A.; Tierney, S. Social Prescribing in National Health Service Primary Care: What Are the Ethical Considerations? Milbank Q. 2021, 99, 610–628. [Google Scholar] [CrossRef]
- Heywood-Everett, S.; Schlosser, A.; Lavis, P.; Howell, S.; Ibison, J. Clinical Psychology in Primary Care—How Can We Afford to Be without It?: A Briefing for Clinical Commissioners and Integrated Care Systems; British Psychological Society: London, UK, 2022. [Google Scholar]
- Naylor, C.; Taggart, H.; Charles, A. Mental Health and New Models of Care: Lessons from the Vanguards; King’s Fund: London, UK, 2017. [Google Scholar]
- NHS. NHS Long Term Plan. Available online: https://www.longtermplan.nhs.uk (accessed on 16 June 2022).
- Stevens, S.; Pritchard, A. Third Phase of NHS Response to COVID-19. Available online: https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/07/20200731-Phase-3-letter-final-1.pdf (accessed on 22 November 2021).
- Tanner, L.M.; Wildman, J.M.; Stoniute, A.; Still, M.; Bernard, K.; Green, R.; Eastaugh, C.H.; Thomson, K.H.; Sowden, S. Non-pharmaceutical primary care interventions to improve mental health in deprived populations: A systematic review. Br. J. Gen. Pract. 2023, bjgp.2022.0343. [Google Scholar] [CrossRef]
- Tanner, L.; Sowden, S.; Still, M.; Thomson, K.; Bambra, C.; Wildman, J. Which Non-Pharmaceutical Primary Care Interventions Reduce Inequalities in Common Mental Health Disorders? A Protocol for a Systematic Review of Quantitative and Qualitative Studies. Int. J. Environ. Res. Public Health 2021, 18, 12978. [Google Scholar] [CrossRef]
- NIHR. Which Non-Pharmaceutical Primary Care Interventions Reduce Inequalities in Common Mental Health Disorders? A Protocol for a Systematic Review of Quantitative and Qualitative Studies (PROSPERO 2021 CRD42021281166) 2021. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=281166 (accessed on 29 November 2021).
- Tong, A.; Flemming, K.; McInnes, E.; Oliver, S. Enhancing transparency in reporting the synthesis of qualitative research: ENTRE. Q. BMC Med. Res. Methodology 2012, 12, 181. [Google Scholar] [CrossRef]
- The Social Prescribing Network. Resources. Available online: https://www.socialprescribingnetwork.com/resources (accessed on 10 September 2021).
- SIREN (Social Interventions Research and Evaluation Network). Make Health Whole. Integrating Care. Improving Lives. Available online: https://makehealthwhole.org/resource/siren-social-interventions-research-evaluation-network/ (accessed on 10 September 2021).
- Long, H.A.; French, D.P.; Brooks, J.M. Optimising the value of the critical appraisal skills programme (CASP) tool for quality appraisal in qualitative evidence synthesis. Res. Methods Med. Health Sci. 2020, 1, 31–42. [Google Scholar] [CrossRef]
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 2008, 8, 45. [Google Scholar] [CrossRef]
- QSR International. Best Qualitative Data Analysis Software for Researchers|NVivo. Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 10 June 2022).
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Altman, D.G.; Booth, A.; et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Bertotti, M.; Frostick, C.; Hutt, P.; Sohanpal, R.; Carnes, D. A realist evaluation of social prescribing: An exploration into the context and mechanisms underpinning a pathway linking primary care with the voluntary sector. Prim. Health Care Res. Dev. 2018, 19, 232–245. [Google Scholar] [CrossRef] [PubMed]
- Bhatti, S.; Rayner, J.; Pinto, A.D.; Mulligan, K.; Cole, D.C. Using self-determination theory to understand the social prescribing process: A qualitative study. BJGP Open 2021, 5. [Google Scholar] [CrossRef]
- Carnes, D.; Sohanpal, R.; Matthur, R.; Homer, K.; Hull, S.; Bertotti, M.; Frostick, C.; Netuveli, G.; Tong, J.-J.; Findlay, G.; et al. City and Hackney Social Prescribing Service: Evaluation Report; QMUL: London, UK, 2015. [Google Scholar]
- Chng, N.R.; Hawkins, K.; Fitzpatrick, B.; O’Donnell, C.; Mackenzie, M.; Wyke, S.; Mercer, S.W. Implementing social prescribing in primary care in areas of high socioeconomic deprivation: Process evaluation of the ‘Deep End’ community links worker programme. Br. J. Gen. Pract. 2021, 71, e912–e920. [Google Scholar] [CrossRef] [PubMed]
- Friedli, L.; Themessl-Huber, M.; Butchart, M. Evaluation of Dundee Equally Well Sources of Support: Social Prescribing in Maryfield; Evaluation Report Four; Dundee Partnership Prescribing: Dundee, Scotland, 2012. [Google Scholar]
- Galvin, K.; Sharples, A.; Jackson, D. Citizens Advice Bureaux in general practice: An illuminative evaluation. Health Soc. Care Community 2000, 8, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Hanlon, P.; Gray, C.M.; Chng, N.R.; Mercer, S.W. Does Self-Determination Theory help explain the impact of social prescribing? A qualitative analysis of patients’ experiences of the Glasgow ‘Deep-End’ Community Links Worker Intervention. Chronic Illn. 2021, 17, 173–188. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S.M.; Giebel, C.; Morasae, E.K.; Rotheram, C.; Mathieson, V.; Ward, D.; Reynolds, V.; Price, A.; Bristow, K.; Kullu, C. Social prescribing for people with mental health needs living in disadvantaged communities: The Life Rooms model. BMC Health Serv. Res. 2020, 20, 19. [Google Scholar] [CrossRef]
- Kiely, B.; Connolly, D.; Clyne, B.; Boland, F.; O’Donnell, P.; Shea, E.O.; Smith, S.M. Primary care-based link workers providing social prescribing to improve health and social care outcomes for people with multimorbidity in socially deprived areas (the LinkMM trial): Pilot study for a pragmatic randomised controlled trial. J. Multimorb. Comorbidity 2021, 11, 1–9. [Google Scholar] [CrossRef]
- Knowles, S.E.; Chew-Graham, C.; Adeyemi, I.; Coupe, N.; Coventry, P.A. Managing depression in people with multimorbidity: A qualitative evaluation of an integrated collaborative care model. BMC Fam. Pract. 2015, 16, 32. [Google Scholar] [CrossRef]
- Makin, S.; Gask, L. ‘Getting back to normal’: The added value of an art-based programme in promoting ‘recovery’ for common but chronic mental health problems. Chronic Illn. 2012, 8, 64–75. [Google Scholar] [CrossRef]
- Moffatt, S.; Steer, M.; Lawson, S.; Penn, L.; O’Brien, N. Link Worker social prescribing to improve health and well-being for people with long-term conditions: Qualitative study of service user perceptions. BMJ Open 2017, 7, e015203. [Google Scholar] [CrossRef]
- Mulligan, K.; Hsiung, S.; Bhatti, S.; Rehel, J.; Rayner, J. Social Prescribing in Ontario: Final Report; AHC: Toronto, ON, Canada, 2020. [Google Scholar]
- Payne, K.; Walton, E.; Burton, C. Steps to benefit from social prescription: A qualitative interview study. Br. J. Gen. Pract. 2020, 70, e36–e44. [Google Scholar] [CrossRef] [PubMed]
- Pescheny, J.; Randhawa, G.; Pappas, Y. Patient uptake and adherence to social prescribing: A qualitative study. BJGP Open 2018, 2. [Google Scholar] [CrossRef] [PubMed]
- Siantz, E.; Henwood, B.; Gilmer, T. Patient Experience With a Large-Scale Integrated Behavioral Health and Primary Care Initiative: A Qualitative Study. Fam. Syst. Health 2020, 38, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, J. The Deep End Advice Worker Project: Embedding an Advice Worker in General Practice Settings; GCPH: Glasgow, UK, 2017. [Google Scholar]
- Skivington, K.; Smith, M.; Chng, N.R.; Mackenzie, M.; Wyke, S.; Mercer, S.W. Delivering a primary care-based social prescribing initiative: A qualitative study of the benefits and challenges. Br. J. Gen. Pract. 2018, 68, e487–e494. [Google Scholar] [CrossRef] [PubMed]
- Webster, L.A.D.; Ekers, D.; Chew-Graham, C.A. Feasibility of training practice nurses to deliver a psychosocial intervention within a collaborative care framework for people with depression and long-term conditions. BMC Nurs. 2016, 15, 71. [Google Scholar] [CrossRef]
- White, J.M.; Cornish, F.; Kerr, S. Front-line perspectives on ‘joined-up’ working relationships: A qualitative study of social prescribing in the west of Scotland. Health Soc. Care Community 2017, 25, 194–203. [Google Scholar] [CrossRef]
- Wildman, J.M.; Moffatt, S.; Steer, M.; Laing, K.; Penn, L.; O’Brien, N. Service-users’ perspectives of link worker social prescribing: A qualitative follow-up study. BMC Public Health 2019, 19, 98. [Google Scholar] [CrossRef]
- Wildman, J.M.; Moffatt, S.; Penn, L.; O’Brien, N.; Steer, M.; Hill, C. Link workers’ perspectives on factors enabling and preventing client engagement with social prescribing. Health Soc. Care Community 2019, 27, 991–998. [Google Scholar] [CrossRef]
- Stuckler, D.; Reeves, A.; Loopstra, R.; Karanikolos, M.; McKee, M. Austerity and health: The impact in the UK and Europe. Eur. J. Public Health 2017, 27, 18–21. [Google Scholar] [CrossRef]
- Pescheny, J.; Pappas, Y.; Randhawa, G. Facilitators and barriers of implementing and delivering social prescribing services: A systematic review. BMC Health Serv. Res. 2018, 18, 86. [Google Scholar] [CrossRef]
- Pescheny, J.; Randhawa, G.; Pappas, Y. The impact of social prescribing services on service users: A systematic review of the evidence. Eur. J. Public Health 2020, 30, 664–673. [Google Scholar] [CrossRef] [PubMed]
- Tierney, S.; Wong, G.; Roberts, N.; Boylan, A.-M.; Park, S.; Abrams, R.; Reeve, J.; Williams, V.; Mahtani, K.R. Supporting social prescribing in primary care by linking people to local assets: A realist review. BMC Med. 2020, 18, 49. [Google Scholar] [CrossRef] [PubMed]
- Vidovic, D.; Reinhardt, G.Y.; Hammerton, C. Can Social Prescribing Foster Individual and Community Well-Being? A Systematic Review of the Evidence. Int. J. Environ. Res. Public Health 2021, 18, 5276. [Google Scholar] [CrossRef] [PubMed]
- Cottam, H. Radical Help: How We Can Remake the Relationships between Us and Revolutionise the Welfare State; Virago: London, UK, 2018. [Google Scholar]
- Skivington, K.; Matthews, L.; Simpson, S.A.; Craig, P.; Baird, J.; Blazeby, J.M.; Boyd, K.A.; Craig, N.; French, D.P.; McIntosh, E.; et al. A new framework for developing and evaluating complex interventions: Update of Medical Research Council guidance. BMJ 2021, 374, n2061. [Google Scholar] [CrossRef]
- Somers, J.M.; Goldner, E.M.; Waraich, P.; Hsu, L. Prevalence and Incidence Studies of Anxiety Disorders: A Systematic Review of the Literature. Can. J. Psychiatry 2006, 51, 100–113. [Google Scholar] [CrossRef]
- Sentell, T.; Shumway, M.; Snowden, L. Access to mental health treatment by English language proficiency and race/ethnicity. J. Gen. Intern. Med. 2007, 22, 289–293. [Google Scholar] [CrossRef]
- McLean, C.; Campbell, C.; Cornish, F. African-Caribbean interactions with mental health services in the UK: Experiences and expectations of exclusion as (re)productive of health inequalities. Soc. Sci. Med. 2003, 56, 657–669. [Google Scholar] [CrossRef]
- Grey, T.; Sewell, H.; Shapiro, G.; Ashraf, F. Mental health inequalities facing U.K. minority ethnic populations: Causal factors and solutions. J. Pyschol. Issues Organ. Cult. 2013, 3, 146–157. [Google Scholar] [CrossRef]
- Emerson, E.; Hatton, C. Contribution of socioeconomic position to health inequalities of British children and adolescents with intellectual disabilities Am. J. Ment. Retard. 2007, 112, 140–150. [Google Scholar] [CrossRef]
- Semlyen, J.; King, M.; Varney, J.; Hagger-Johnson, G. Sexual orientation and symptoms of common mental disorder or low wellbeing: Combined meta-analysis of 12 UK population health surveys. BMC Psychiatry 2016, 16, 67. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Author, Year and Setting | Aim | Methods | Participants | Health Conditions Targeted | SES Characteristics | Intervention Description | Quality Appraisal |
|---|---|---|---|---|---|---|---|
| Bertotti et al., 2018 [38] City and Hackney, London, England | To explore what worked in the social prescribing pilot in City and Hackney, for whom and under what circumstances. | Mixed methods: Quantitative online surveys, qualitative interviews, FGDs *, observations of sessions with social prescribing coordinators | Service users (n = 17), community organisations (n = 3), social prescribing coordinators (n = 3), commissioners (n = 2), GPs (n = 2) | Social problems or mild to moderate mental health problems, including anxiety and depression | Area of socioeconomic deprivation | Social prescribing: link workers 23 GP practices; patients referred to social prescribing coordinators who referred to community organisations. | Medium |
| Bhatti et al., 2021 [39] Ontario, Canada | To explore how social prescribing as a process facilitates positive outcomes for patients. | Qualitative: FGDs and semi-structured interviews | Service users (n = 96) | ‘Unmet social needs’, including individuals with anxiety and depression | Majority of participants described as low income | Social prescribing: link workers 11 community health centres; referred to activities by health provider directly or via link worker. Supported to attend prescribed with opportunity to become involved as ‘health champion’. | High |
| Carnes et al., 2015 [40] City and Hackney, London, England | To assess the social prescribing project with respect to effects on individuals, primary care team awareness of community resources, and costs. | Mixed methods (evaluation): interviews, FGDs, field visits, quantitative survey, electronic patient record data | Coordinators (n = 4), GPs (n = 2), commissioners (n = 2), service users (n = 5), 4 field visits to service providers | Social isolation, including individuals with anxiety and depression | Area of socioeconomic deprivation | Social prescribing: link workers 22 GP practices; patients referred to social prescribing coordinator, discussed action plans for achieving goals in up to 6 sessions. | Low |
| Chng et al., 2021 [41] Glasgow, Scotland | To explore the implementation process of the link worker approach to social prescribing in practice. | Qualitative: FGDs, email surveys, in-depth interviews | GPs, link workers, practice managers and community organisation workers (n = 31 FGDs, 19 surveys, 33 in-depth interviews, staff distribution unclear) | Social problems and multimorbidity, including individuals with anxiety and depression | Areas of socioeconomic deprivation | Social prescribing: link workers ‘Deep End Link Worker Programme’ in seven GP practices in deprived areas of Glasgow. Link workers embedding social prescribing approaches within practices, establishing referral pathways, and building networks with local community organisations. | High |
| Friedli et al., 2012 [42] Dundee, Scotland | To evaluate a pilot social prescribing scheme. | Mixed methods (evaluation): Pre- and post-intervention questionnaires, link worker notes and reflections, qualitative interviews, semi-structured interviews | Service users (n = 16), GPs (n = 2), link workers (n = 3) | Social problems and long-term conditions including mild to moderate anxiety and depression | Area of socioeconomic deprivation | Social prescribing: link workers One GP surgery (‘test site’); patients referred to link worker, had up to four consultations for assess needs and identify community-based information, support or activities. | Low |
| Galvin et al., 2000 [43] Southern county of England | To explore the impact of a Citizens Advice Bureaux service in primary care. | Mixed methods: quantitative questionnaire; qualitative interviews; FGDs | Service users (n = 10), CAB advisers (n = 2), GPs (n = 6) | ‘Complex needs’ including depression | Service mainly accessed by people needing help with financial problems, accessing benefits or having employment issues. | Social prescribing Citizens Advice Bureau advisers located in GP practices to offer advice e.g., on finance, housing and employment. | High |
| Hanlon et al., 2021 [44] Glasgow, Scotland | To investigate if Self Determination Theory can be used to understand the change, or lack of change, resulting from patients’ involvement in the Links Worker Programme. | Qualitative: Semi-structured interviews (conducted as part of quasi experimental cluster RCT) | Service users (n = 12) | ‘Complex needs’ including anxiety and depression | Areas of socioeconomic deprivation | Social prescribing: link workers 11 GP practices; one community link practitioner attached to each surgery. Patients referred to community link practitioners to signpost and support engagement with community organisations. Involved GP surgeries had a practice development fund and access to shared learning events for practice staff. | High |
| Hassan et al., 2020 [45] Northwest of England | To explore a community hub project as a social prescribing model and identify key elements that contribute toward enhancing its effectiveness. | Qualitative: FGDs | Service users (n = 18) | ‘Mental health’ | Areas of socioeconomic deprivation | Social prescribing “Life Rooms” programme: physical space for learning opportunities and social support from specialist staff, and peer tutors. Provides safe environment including cafe and computer facilities. | High |
| Kiely et al., 2021 [46] Ireland | To report the results of a pilot study, conducted in preparation for an RCT that aims to test the effectiveness of primary care-based link workers. | Qualitative: Structured interviews | Service users (n = 6), link worker (n = 1), GPs (n = 2) | ‘Individuals with multimorbidity’; including those with anxiety and depression | Area of socioeconomic deprivation | Social prescribing: link workers One pilot GP practice; patients invited to meet with link workers at the practice link workers supported them over six week period to access recommended community resources. | Medium |
| Knowles et al., 2015 [47] Northwest of England | To report the results of a nested qualitative study within a trial which aimed to examine how a collaborative care model was implemented, and how providers experienced the integration of physical and mental healthcare. | Qualitative: semi-structured interviews (conducted as part of wider trial) | Service users (n = 31), practice nurses (n = 12), psychological wellbeing practitioners (n = 11), GPs (n = 7). | Depression and long-term conditions | Areas of socioeconomic deprivation | New method of clinical practice 17 GP practices; collaborative care integrating depression care within the management of long-term conditions. Eight sessions of low intensity psychological therapy delivered by psychological wellbeing practitioners who acted as case managers, including joint meetings with practice nurses and discussion of physical-mental comorbidities. | High |
| Makin and Gask, 2012 [48] Salford, England | “To explore the added value of participation in an Arts on Prescription programme to aid the process of recovery in people with common but chronic mental health problems that have already undergone a psychological ‘talking’-based therapy”.” | Qualitative: in-depth interviews | Service users (n = 15) | Mild to moderate anxiety and depression | Area of socioeconomic deprivation | Social prescribing ‘Arts on prescription’: referrals from health/social care providers, initial assessment by mental health worker, two arts sessions weekly for six months | High |
| Moffat et al., 2017 [49] Newcastle-upon-Tyne, England | To describe the experiences of patients with long-term conditions in a Link Worker social prescribing programme and identify the programme’s impact on health and wellbeing. | Qualitative: semi-structured interviews | Service users (n = 30) | Long-term conditions, including individuals with co-morbid anxiety and depression | Area of socioeconomic deprivation | Social prescribing: link workers ‘Ways to Wellness’ programme: referrals from primary care practitioner, link workers trained in behaviour change meet with them to identify goals and connect to community groups and resources. | High |
| Mulligan et al., 2020 [50] Ontario, Canada | To examine how a social prescribing programme was implemented, perceptions of the programme, and its impact on healthcare systems. | Mixed methods (evaluation): FGDs, aggregate-level data reporting | Service users, community champions, providers (numbers in FGDs unclear) | ‘Unmet social needs’, including individuals with anxiety and depression | Majority of participants described as low income | Social prescribing: link workers This is an early report which provides a descriptive summary of main outcomes. It precedes the journal article Bhatti 2021 and reports on the same project (see above). | Low |
| Payne et al., 2020 [51] Sheffield, England | “To explore the ways by which social prescribing may be beneficial to individuals undertaking socially prescribed activity.” | Qualitative: semi-structured interviews | Service users (n = 17) | Range of psychosocial issues, including depression | Areas of socioeconomic deprivation | Social prescribing: link workers Social prescribing organisation: referrals from local healthcare professionals, initial consultation then signposted to community groups or within the organisation to advocacy, social cafes and health trainers. | High |
| Pescheny et al., 2018 [52] Luton, England | “To explore the experiences and views of service users, involved GPs, and navigators on factors influencing uptake and adherence to social prescribing”. | Qualitative: semi-structured interviews | Service users (n = 10), GPs (n = 3), navigators (n = 2) | Range of psychosocial issues, including anxiety and depression | Area of socioeconomic deprivation | Social prescribing HCP refers to navigator. Navigators can refer service users onwards to a maximum of 12 sessions e.g., meditation, physical activity, arts, job centre support, housing advice | High |
| Siantz et al., 2020 [53] Southern California, USA | To explore patient experience and provider perceptions within an initiative to deliver integrated care to people with complex needs as part of a system redesign. | Qualitative: FGDs, qualitative interviews | Service users (n = 54), providers (n = 32) | ‘Complex needs’, including depression | Individuals using Medicaid services (health coverage for people on low income) | New model of care Behavioral Health Integration and Complex Care Initiative (BHICCI): a large-scale system redesign to deliver integrated care to people with complex needs. Delivery across multiple participating health care clinics. Participating clinics created multidisciplinary teams to oversee care management of patients with >1 chronic care condition and one mental health condition. | High |
| Sinclair, 2017 [54] Glasgow, Scotland | To explore the impact of an advice worker project in GP practices both on people delivering and accessing the project, and to better understand the supporting processes. | Mixed methods (evaluation): semi-structured interviews, written notes during meetings and conversations, referral and financial data | GPs (n = 3), advice worker (n = 1), practice managers (n = 2) | Self-reported long-term illness, mobility impairments and ‘mental health issues’ | Areas of socioeconomic deprivation | Social prescribing Advice workers delivering service in two GP practices, offering appointments on issues such as housing, social security and financial management. If appropriate, they referred people onto additional forms of specialist community support, such as carers’ support, mental health and homelessness organisations. | Medium |
| Skivington et al., 2018 [55] Glasgow, Scotland | “To investigate issues relevant to implementing a social prescribing programme to improve inter-sectoral working to achieve public health goals.” | Qualitative: semi-structured interviews | Community link practitioners (n = 6), community organisation representatives (n = 30) | Community organisations designed for range of problems including ‘mental health’ | Areas of socioeconomic deprivation | Social prescribing: link workers ‘Links Worker Programme’: primary care professionals refer to community links practitioners, who support patients to access community organisations. It is also designed to improve inter-sectoral working by strengthening links between GP practices and community organisations. | High |
| Webster et al., 2016 [56] North of England | “To examine the acceptability of a Brief Behavioural Activation intervention within a collaborative care framework.” | Qualitative: semi-structured interviews (nested qualitative evaluation within a service development pilot) | GPs (n = 5), practice nurse (n = 3), healthcare assistant (n = 1), mental health gateway worker (n = 1), service users (n = 4) | Depression and long-term conditions | Area of socioeconomic deprivation | New method of clinical practice A ‘collaborative care framework’ to address both depression and long-term conditions. Practice nurses acted as case managers and delivered Behavioural Activation (intervention for depression), with support from GPs and a mental health specialist. | High |
| White et al., 2017 [57] West Central Scotland | To “examine factors that may promote or compromise the implementation of social prescribing, as a collaboration between statutory and third sectors in Scotland”. | Qualitative: semi-structured interviews | Health visitors (n = 7), district nurses (n = 8), GPs (n = 3), community organisation representatives (n = 15) | ‘Mental health’ | Areas of socioeconomic deprivation | Social prescribing Three community organisations: a healthy lifestyle project, a carers’ centre and a project to address mental health issues including substance misuse. Service users were referred to these programmes by health visitors, district nurses and GPs. | High |
| Wildman et al., 2019 [58] Newcastle-upon-Tyne, England | “To explore experiences of social prescribing among people with long-term conditions one to two years after their initial engagement with a social prescribing service”. | Qualitative: semi-structured interviews Follow up study of participants from Moffatt 2017. | Service users (n = 24) | ‘Mental health and social isolation issues’, including anxiety and depression | Area of socioeconomic deprivation | Social prescribing: link workers ‘Ways to Wellness’ programme: referrals from primary care practitioner, link workers trained in behaviour change meet with them to identify goals and connect to community groups and resources. | High |
| Wildman et al., 2019 [59] Newcastle-upon-Tyne, England | To explore how link workers understand their role in social prescribing, as well as its challenges and threats to client engagement. | Qualitative: FGDs, semi-structured interviews | Link workers (n = 26) | Long-term conditions, including individuals with co-morbid anxiety and depression | Area of socioeconomic deprivation | Social prescribing: link workers ‘Ways to Wellness’ programme: referrals from primary care practitioner, link workers trained in behaviour change meet with them to identify goals and connect to community groups and resources. | High |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernard, K.; Wildman, J.M.; Tanner, L.M.; Stoniute, A.; Still, M.; Green, R.; Eastaugh, C.; Sowden, S.; Thomson, K.H. Experiences of Non-Pharmaceutical Primary Care Interventions for Common Mental Health Disorders in Socioeconomically Disadvantaged Groups: A Systematic Review of Qualitative Studies. Int. J. Environ. Res. Public Health 2023, 20, 5237. https://doi.org/10.3390/ijerph20075237
Bernard K, Wildman JM, Tanner LM, Stoniute A, Still M, Green R, Eastaugh C, Sowden S, Thomson KH. Experiences of Non-Pharmaceutical Primary Care Interventions for Common Mental Health Disorders in Socioeconomically Disadvantaged Groups: A Systematic Review of Qualitative Studies. International Journal of Environmental Research and Public Health. 2023; 20(7):5237. https://doi.org/10.3390/ijerph20075237
Chicago/Turabian StyleBernard, Kate, Josephine M. Wildman, Louise M. Tanner, Akvile Stoniute, Madeleine Still, Rhiannon Green, Claire Eastaugh, Sarah Sowden, and Katie H. Thomson. 2023. "Experiences of Non-Pharmaceutical Primary Care Interventions for Common Mental Health Disorders in Socioeconomically Disadvantaged Groups: A Systematic Review of Qualitative Studies" International Journal of Environmental Research and Public Health 20, no. 7: 5237. https://doi.org/10.3390/ijerph20075237
APA StyleBernard, K., Wildman, J. M., Tanner, L. M., Stoniute, A., Still, M., Green, R., Eastaugh, C., Sowden, S., & Thomson, K. H. (2023). Experiences of Non-Pharmaceutical Primary Care Interventions for Common Mental Health Disorders in Socioeconomically Disadvantaged Groups: A Systematic Review of Qualitative Studies. International Journal of Environmental Research and Public Health, 20(7), 5237. https://doi.org/10.3390/ijerph20075237