
Dismantling the Component-Specific Effects of Yogic Breathing: Feasibility of a Fully Remote Three-Arm RCT with Virtual Laboratory Visits and Wearable Physiology

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
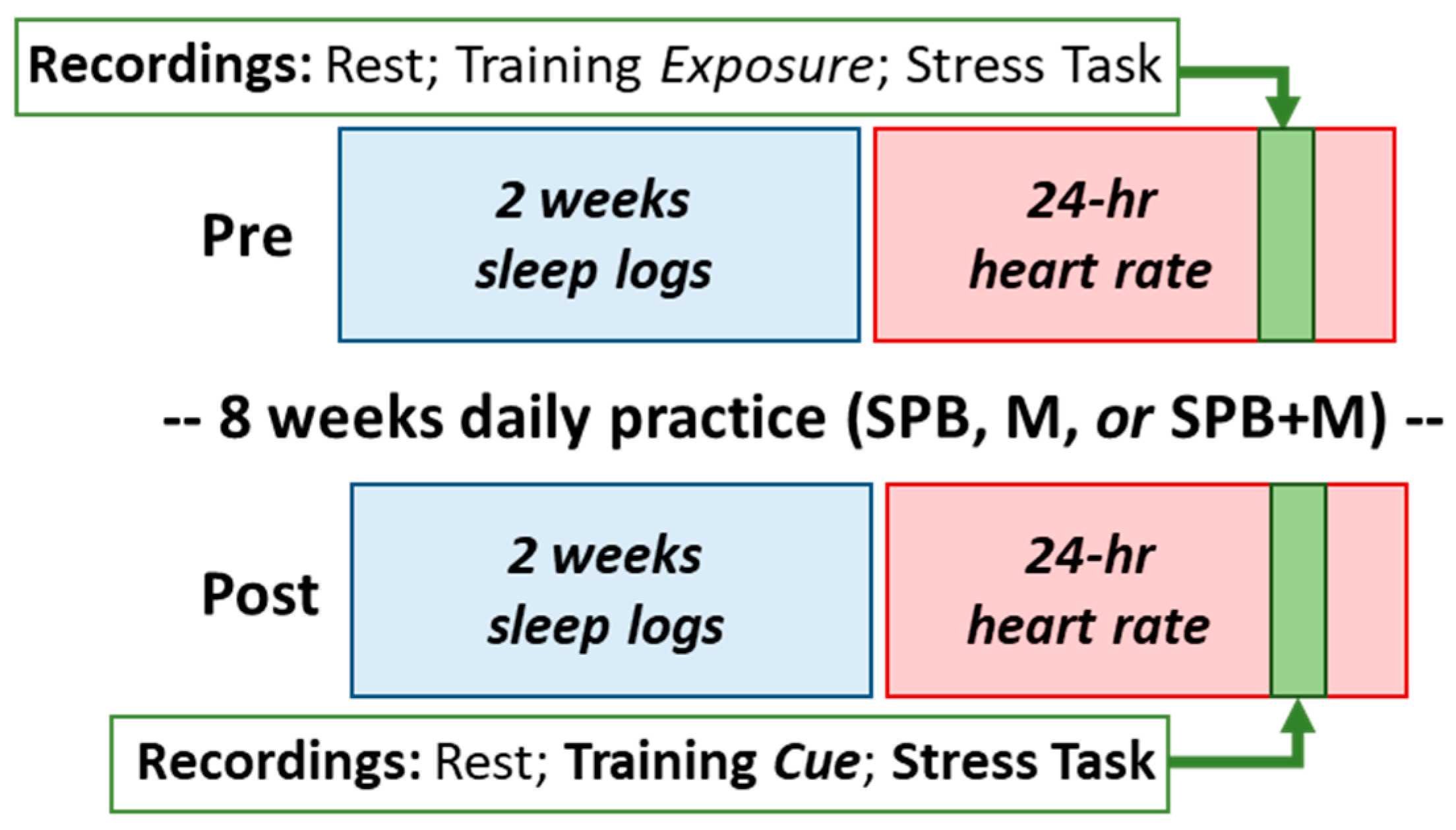
2.1. Eligibility Criteria and Randomized Trial Design
2.2. Recruitment and Consent
2.3. Randomization and Interventions
2.4. Virtual Lab Visits
2.5. Baseline Questionnaire-Based Measures
2.6. Daily Logs
2.7. Ambulatory Heart Rate and Heart Rate Variability
2.8. Outcome Measurements
2.9. Statistical Analyses
3. Results
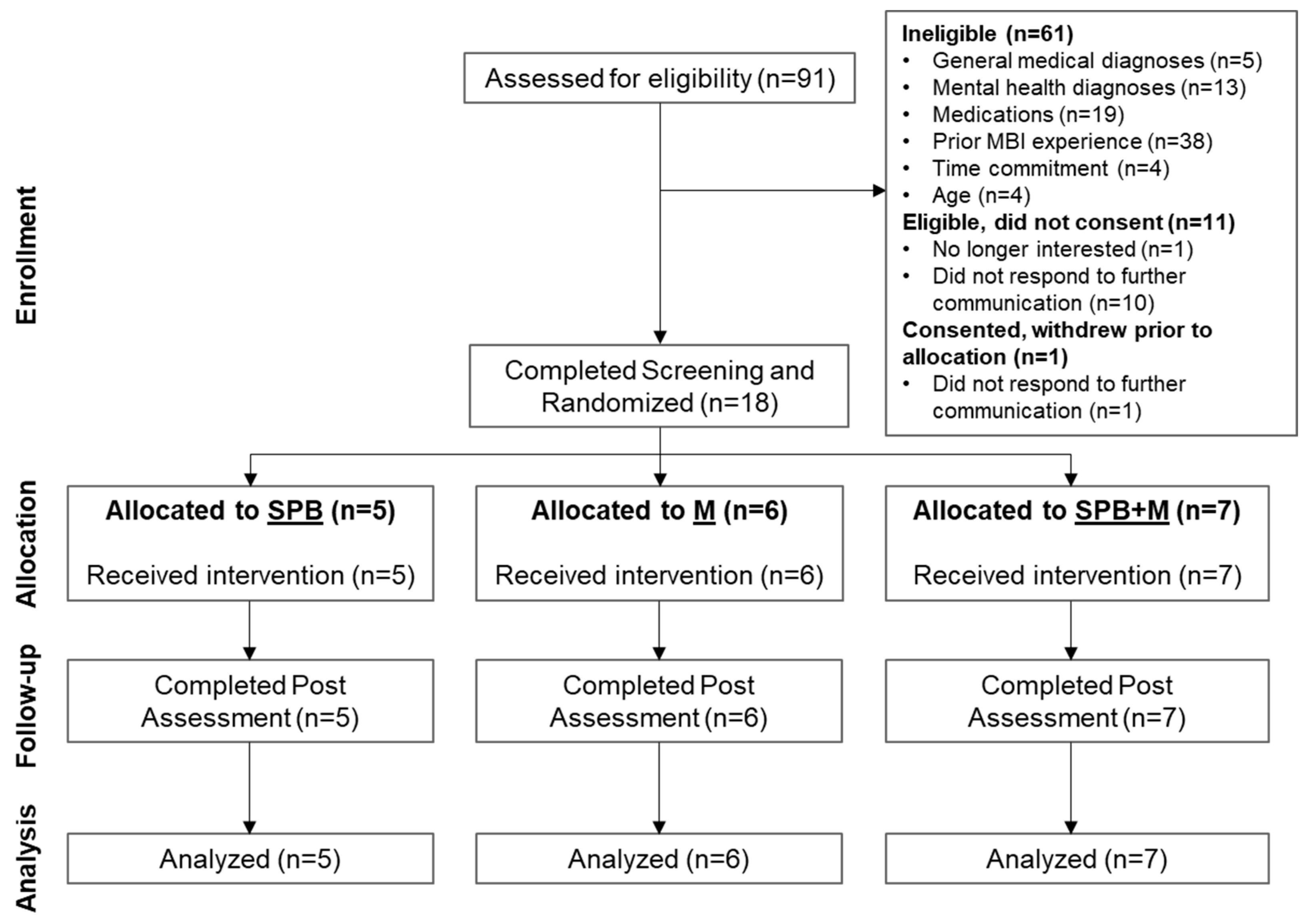
3.1. Feasibility of the Remote RCT
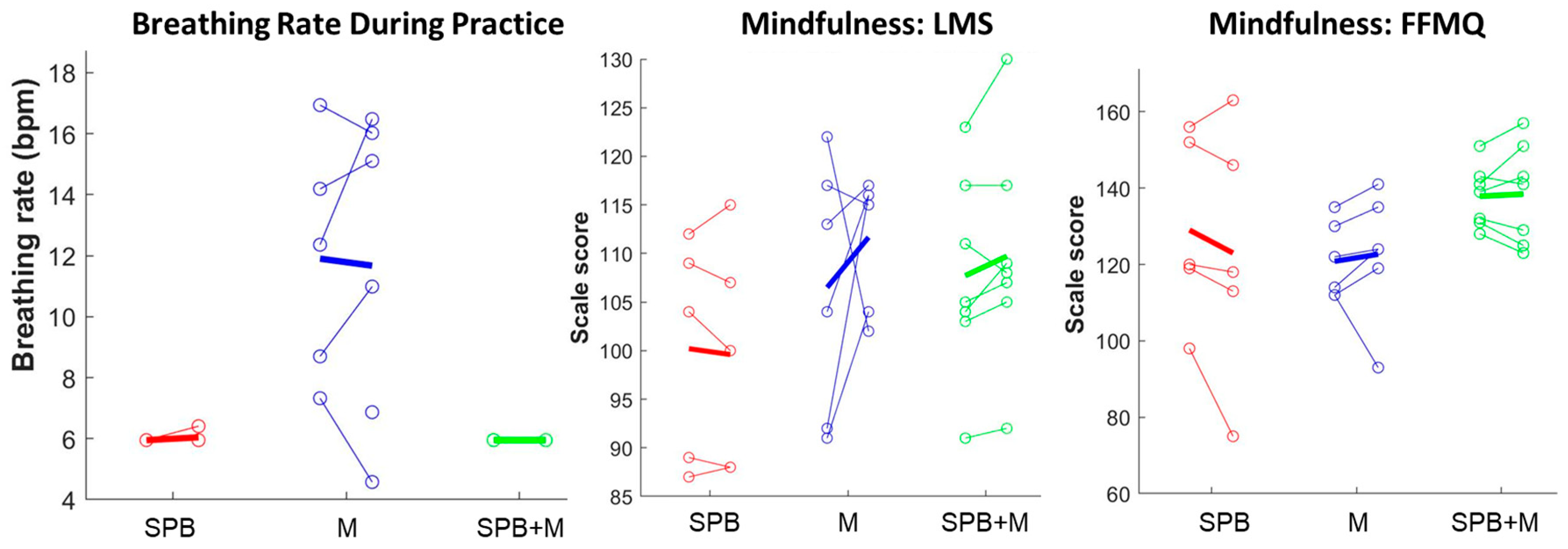
3.2. Feasibility of Wearable Devices to Detect Intervention-Specific Breathing Patterns
3.3. Mindfulness
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tran, B.X.; Harijanto, C.; Vu, G.T.; Ho, R.C.M. Global mapping of interventions to improve quality of life using mind-body therapies during 1990-2018. Complement. Ther. Med. 2020, 49, 102350. [Google Scholar] [CrossRef] [PubMed]
- Younge, J.O.; Gotink, R.A.; Baena, C.P.; Roos-Hesselink, J.W.; Hunink, M.G. Mind-body practices for patients with cardiac disease: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2015, 22, 1385–1398. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Singh, S.; Sibinga, E.M.; Gould, N.F.; Rowland-Seymour, A.; Sharma, R.; Berger, Z.; Sleicher, D.; Maron, D.D.; Shihab, H.M.; et al. Meditation programs for psychological stress and well-being: A systematic review and meta-analysis. JAMA Intern. Med. 2014, 174, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Pascoe, M.C.; Thompson, D.R.; Jenkins, Z.M.; Ski, C.F. Mindfulness mediates the physiological markers of stress: Systematic review and meta-analysis. J. Psychiatr. Res. 2017, 95, 156–178. [Google Scholar] [CrossRef] [PubMed]
- Khoury, B.; Sharma, M.; Rush, S.E.; Fournier, C. Mindfulness-based stress reduction for healthy individuals: A meta-analysis. J. Psychosom. Res. 2015, 78, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Cocchiara, R.A.; Peruzzo, M.; Mannocci, A.; Ottolenghi, L.; Villari, P.; Polimeni, A.; Guerra, F.; La Torre, G. The Use of Yoga to Manage Stress and Burnout in Healthcare Workers: A Systematic Review. J. Clin. Med. 2019, 8, 284. [Google Scholar] [CrossRef]
- Pascoe, M.C.; Thompson, D.R.; Ski, C.F. Yoga, mindfulness-based stress reduction and stress-related physiological measures: A meta-analysis. Psychoneuroendocrinology 2017, 86, 152–168. [Google Scholar] [CrossRef]
- Rusch, H.L.; Rosario, M.; Levison, L.M.; Olivera, A.; Livingston, W.S.; Wu, T.; Gill, J.M. The effect of mindfulness meditation on sleep quality: A systematic review and meta-analysis of randomized controlled trials. Ann. New York Acad. Sci. 2019, 1445, 5–16. [Google Scholar] [CrossRef]
- Li, H.; Chen, J.; Xu, G.; Duan, Y.; Huang, D.; Tang, C.; Liu, J. The Effect of Tai Chi for Improving Sleep Quality: A Systematic Review and Meta-analysis. J. Affect. Disord. 2020, 274, 1102–1112. [Google Scholar] [CrossRef]
- Wang, W.L.; Chen, K.H.; Pan, Y.C.; Yang, S.N.; Chan, Y.Y. The effect of yoga on sleep quality and insomnia in women with sleep problems: A systematic review and meta-analysis. BMC Psychiatry 2020, 20, 195. [Google Scholar] [CrossRef]
- Zou, L.; Yeung, A.; Quan, X.; Boyden, S.D.; Wang, H. A Systematic Review and Meta-Analysis of Mindfulness-Based (Baduanjin) Exercise for Alleviating Musculoskeletal Pain and Improving Sleep Quality in People with Chronic Diseases. Int. J. Environ. Res. Public Health 2018, 15, 206. [Google Scholar] [CrossRef] [PubMed]
- Raman, G.; Zhang, Y.; Minichiello, V.J.; D’Ambrosio, C.M.; Wang, C. Tai Chi Improves Sleep Quality in Healthy Adults and Patients with Chronic Conditions: A Systematic Review and Meta-analysis. J. Sleep Disord. Ther. 2013, 2, 141. [Google Scholar] [CrossRef]
- Nivethitha, L.; Mooventhan, A.; Manjunath, N.K. Effects of Various Prāṇāyāma on Cardiovascular and Autonomic Variables. Anc. Sci. Life 2016, 36, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Akella, K.; Kanuri, S.H.; Murtaza, G.; Della Rocca, D.G.; Kodwani, N.; Turagam, M.K.; Shenthar, J.; Padmanabhan, D.; Ray, I.B.; Natale, A.; et al. Impact of Yoga on Cardiac Autonomic Function and Arrhythmias. J. Atr. Fibrillation 2020, 13, 2408. [Google Scholar] [CrossRef] [PubMed]
- Russo, M.A.; Santarelli, D.M.; O’Rourke, D. The physiological effects of slow breathing in the healthy human. Breathe (Sheff. Engl.) 2017, 13, 298–309. [Google Scholar] [CrossRef]
- Zaccaro, A.; Piarulli, A.; Laurino, M.; Garbella, E.; Menicucci, D.; Neri, B.; Gemignani, A. How Breath-Control Can Change Your Life: A Systematic Review on Psycho-Physiological Correlates of Slow Breathing. Front. Hum. Neurosci. 2018, 12, 353. [Google Scholar] [CrossRef]
- Lindsay, E.K.; Creswell, J.D. Mechanisms of mindfulness training: Monitor and Acceptance Theory (MAT). Clin. Psychol. Rev. 2017, 51, 48–59. [Google Scholar] [CrossRef]
- Tang, Y.Y.; Tang, R.; Gross, J.J. Promoting Psychological Well-Being Through an Evidence-Based Mindfulness Training Program. Front. Hum. Neurosci. 2019, 13, 237. [Google Scholar] [CrossRef]
- Harrison, S.L.; Lee, A.; Goldstein, R.S.; Brooks, D. Perspectives of healthcare professionals and patients on the application of mindfulness in individuals with chronic obstructive pulmonary disease. Patient Educ. Couns. 2017, 100, 337–342. [Google Scholar] [CrossRef]
- Taylor, A.G.; Goehler, L.E.; Galper, D.I.; Innes, K.E.; Bourguignon, C. Top-down and bottom-up mechanisms in mind-body medicine: Development of an integrative framework for psychophysiological research. Explore 2010, 6, 29–41. [Google Scholar] [CrossRef]
- Goldin, P.R.; Moodie, C.A.; Gross, J.J. Acceptance versus reappraisal: Behavioral, autonomic, and neural effects. Cogn. Affect. Behav. Neurosci. 2019, 19, 927–944. [Google Scholar] [CrossRef] [PubMed]
- Kabat-Zinn, J. Wherever You Go, There You Are: Mindfulness Meditation in Everyday Life, 10th ed.; Hyperion: New York, NY, USA, 2005. [Google Scholar]
- Ma, Y.; Kraemer, K.M.; Lyu, J.; Yeh, G.Y. Randomized controlled trials of mindfulness and Acceptance-Based interventions over the past two decades: A bibliometric analysis. J. Altern. Complement. Med. 2021, 27, 930–939. [Google Scholar] [CrossRef]
- Tymofiyeva, O.; Hu, M.Y.; Sipes, B.S.; Jakary, A.; Glidden, D.V.; Jariwala, N.; Bhandari, S.; Parks, K.C.; Nguyen, C.; Henje, E.; et al. A Feasibility Study of a Remotely-Delivered Mindfulness-Based Training for Adolescents During the COVID-19 Pandemic. Front. Psychiatry 2022, 13, 645. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Darbari, I.; Tolaymat, M.; Quezada, S.; Allen, J.; Cross, R.K. Randomized controlled pilot study of feasibility and effectiveness of peer led remote Mindfulness-Based Art Workshops on stress, anxiety, and depression in medical students. Psychol. Sch. 2022. [Google Scholar] [CrossRef]
- Farewell, C.V.; Walls, J.; Powers, J.; Whalen, J.; Shefferman, M.; Leiferman, J. Feasibility of a Perinatal Mindfulness-Based Intervention Delivered Remotely Due to COVID-19. OBM Integr. Complement. Med. 2021, 6, 17. [Google Scholar] [CrossRef]
- Moulton-Perkins, A.; Moulton, D.; Cavanagh, K.; Jozavi, A.; Strauss, C. Systematic review of mindfulness-based cognitive therapy and mindfulness-based stress reduction via group videoconferencing: Feasibility, acceptability, safety, and efficacy. J. Psychother. Integr. 2022, 32, 110–130. [Google Scholar] [CrossRef]
- Mirabito, G.; Verhaeghen, P. Remote delivery of a Koru Mindfulness intervention for college students during the COVID-19 pandemic. J. Am. Coll. Health 2022, 1–8. [Google Scholar] [CrossRef]
- Hanson, P.; Villarreal, M.; Khan, M.; Dale, J.; Sankar, S. Effect of an Online Mindfulness Course for Hospital Doctors During COVID-19 Pandemic on Resilience and Coping. J. Prim. Care Community Health 2022, 13, 21501319221138425. [Google Scholar] [CrossRef]
- Boettcher, J.; Åström, V.; Påhlsson, D.; Schenström, O.; Andersson, G.; Carlbring, P. Internet-Based Mindfulness Treatment for Anxiety Disorders: A Randomized Controlled Trial. Behav. Ther. 2014, 45, 241–253. [Google Scholar] [CrossRef]
- Cole, A.R.; Wijarnpreecha, K.; Chattipakorn, S.C.; Chattipakorn, N. Effects of Tai Chi exercise on heart rate variability. Complement. Ther. Clin. Pract. 2016, 23, 59–63. [Google Scholar] [CrossRef]
- Laborde, S.; Allen, M.S.; Borges, U.; Dosseville, F.; Hosang, T.J.; Iskra, M.; Mosley, E.; Salvotti, C.; Spolverato, L.; Zammit, N.; et al. Effects of voluntary slow breathing on heart rate and heart rate variability: A systematic review and a meta-analysis. Neurosci. Biobehav. Rev. 2022, 138, 104711. [Google Scholar] [CrossRef] [PubMed]
- Rådmark, L.; Sidorchuk, A.; Osika, W.; Niemi, M. A Systematic Review and Meta-Analysis of the Impact of Mindfulness Based Interventions on Heart Rate Variability and Inflammatory Markers. J. Clin. Med. 2019, 8, 1638. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Sasaki, J.E.; Wei, G.X.; Huang, T.; Yeung, A.S.; Neto, O.B.; Chen, K.W.; Hui, S.S. Effects of Mind-Body Exercises (Tai Chi/Yoga) on Heart Rate Variability Parameters and Perceived Stress: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2018, 7, 404. [Google Scholar] [CrossRef]
- National Center For Complementary and Alternative Medicine—Pilot Studies: Common Uses and Misuses. Available online: https://www.nccih.nih.gov/grants/pilot-studies-common-uses-and-misuses (accessed on 5 February 2023).
- Orsmond, G.I.; Cohn, E.S. The Distinctive Features of a Feasibility Study: Objectives and Guiding Questions. OTJR Occup. Particip. Health 2015, 35, 169–177. [Google Scholar] [CrossRef]
- Berghoff, C.R.; Wheeless, L.E.; Ritzert, T.R.; Wooley, C.M.; Forsyth, J.P. Mindfulness Meditation Adherence in a College Sample: Comparison of a 10-Min Versus 20-Min 2-Week Daily Practice. Mindfulness 2017, 8, 1513–1521. [Google Scholar] [CrossRef]
- Chin, M.S.; Kales, S.N. Understanding mind-body disciplines: A pilot study of paced breathing and dynamic muscle contraction on autonomic nervous system reactivity. Stress Health J. Int. Soc. Investig. Stress 2019, 35, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Chin, M.S.; Kales, S.N. Is There an Optimal Autonomic State for Enhanced Flow and Executive Task Performance? Front. Psychol. 2019, 10, 1716. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Lee, E.-H. Review of the Psychometric Evidence of the Perceived Stress Scale. Asian Nurs. Res. 2012, 6, 121–127. [Google Scholar] [CrossRef]
- Mollayeva, T.; Thurairajah, P.; Burton, K.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 25, 52–73. [Google Scholar] [CrossRef]
- Grandner, M.A.; Kripke, D.F.; Yoon, I.-Y.; Youngstedt, S.D. Criterion validity of the Pittsburgh Sleep Quality Index: Investigation in a non-clinical sample. Sleep Biol. Rhythm. 2006, 4, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Manzar, M.D.; BaHammam, A.S.; Hameed, U.A.; Spence, D.W.; Pandi-Perumal, S.R.; Moscovitch, A.; Streiner, D.L. Dimensionality of the Pittsburgh Sleep Quality Index: A systematic review. Health Qual. Life Outcomes 2018, 16, 89. [Google Scholar] [CrossRef] [PubMed]
- Backhaus, J.; Junghanns, K.; Broocks, A.; Riemann, D.; Hohagen, F. Test–retest reliability and validity of the Pittsburgh Sleep Quality Index in primary insomnia. J. Psychosom. Res. 2002, 53, 737–740. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds III, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.; Clark, L.A.; Weber, K.; Assenheimer, J.S.; Strauss, M.E.; McCormick, R.A. Testing a tripartite model: II. Exploring the symptom structure of anxiety and depression in student, adult, and patient samples. J. Abnorm. Psychol. 1995, 104, 15–25. [Google Scholar] [CrossRef]
- Watson, D.; Weber, K.; Assenheimer, J.S.; Clark, L.A.; Strauss, M.E.; McCormick, R.A. Testing a tripartite model: I. Evaluating the convergent and discriminant validity of anxiety and depression symptom scales. J. Abnorm. Psychol. 1995, 104, 3–14. [Google Scholar] [CrossRef]
- Buckby, J.A.; Yung, A.R.; Cosgrave, E.M.; Killackey, E.J. Clinical utility of the Mood and Anxiety Symptom Questionnaire (MASQ) in a sample of young help-seekers. BMC Psychiatry 2007, 7, 50. [Google Scholar] [CrossRef]
- John, O.P.; Donahue, E.; Kentle, R. Big Five Inventory (BFI). APA PsycTests. 1991. Available online: https://www.ebsco.com/products/research-databases/apa-psyctests (accessed on 5 February 2023).
- Yang, H.; Haack, M.; Dang, R.; Gautam, S.; Simpson, N.S.; Mullington, J.M. Heart rate variability rebound following exposure to persistent and repetitive sleep restriction. Sleep 2019, 42, zsy226. [Google Scholar] [CrossRef]
- Blons, E.; Arsac, L.M.; Gilfriche, P.; McLeod, H.; Lespinet-Najib, V.; Grivel, E.; Deschodt-Arsac, V. Alterations in heart-brain interactions under mild stress during a cognitive task are reflected in entropy of heart rate dynamics. Sci. Rep. 2019, 9, 18190. [Google Scholar] [CrossRef]
- Martin, L.R.; Williams, S.L.; Haskard, K.B.; Dimatteo, M.R. The challenge of patient adherence. Ther. Clin. Risk Manag. 2005, 1, 189–199. [Google Scholar]
- Vettese, L.C.; Toneatto, T.; Stea, J.N.; Nguyen, L.; Wang, J.J. Do Mindfulness Meditation Participants Do Their Homework? And Does It Make a Difference? A Review of the Empirical Evidence. J. Cogn. Psychother 2009, 23, 198–225. [Google Scholar] [CrossRef]
- Thurman, S.M.; Wasylyshyn, N.; Roy, H.; Lieberman, G.; Garcia, J.O.; Asturias, A.; Okafor, G.N.; Elliott, J.C.; Giesbrecht, B.; Grafton, S.T.; et al. Individual differences in compliance and agreement for sleep logs and wrist actigraphy: A longitudinal study of naturalistic sleep in healthy adults. PLoS ONE 2018, 13, e0191883. [Google Scholar] [CrossRef] [PubMed]
- Chung, A.H.; Gevirtz, R.N.; Gharbo, R.S.; Thiam, M.A.; Ginsberg, J.P. Pilot Study on Reducing Symptoms of Anxiety with a Heart Rate Variability Biofeedback Wearable and Remote Stress Management Coach. Appl. Psychophysiol. Biofeedback 2021, 46, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Leon, A.C.; Davis, L.L.; Kraemer, H.C. The role and interpretation of pilot studies in clinical research. J. Psychiatr. Res. 2011, 45, 626–629. [Google Scholar] [CrossRef]
- Davidson, R.J.; Kabat-Zinn, J.; Schumacher, J.; Rosenkranz, M.; Muller, D.; Santorelli, S.F.; Urbanowski, F.; Harrington, A.; Bonus, K.; Sheridan, J.F. Alterations in brain and immune function produced by mindfulness meditation. Psychosom. Med. 2003, 65, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Mantzios, M.; Giannou, K. A Real-World Application of Short Mindfulness-Based Practices: A Review and Reflection of the Literature and a Practical Proposition for an Effortless Mindful Lifestyle. Am. J. Lifestyle Med. 2019, 13, 520–525. [Google Scholar] [CrossRef]
- Carmody, J.; Baer, R.A. Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. J. Behav. Med. 2008, 31, 23–33. [Google Scholar] [CrossRef]
- Chaddha, A.; Modaff, D.; Hooper-Lane, C.; Feldstein, D.A. Device and non-device-guided slow breathing to reduce blood pressure: A systematic review and meta-analysis. Complement. Ther. Med. 2019, 45, 179–184. [Google Scholar] [CrossRef]
- Kubo, A.; Aghaee, S.; Kurtovich, E.M.; Nkemere, L.; Quesenberry, C.P.; McGinnis, M.K.; Avalos, L.A. mHealth Mindfulness Intervention for Women with Moderate-to-Moderately-Severe Antenatal Depressive Symptoms: A Pilot Study Within an Integrated Health Care System. Mindfulness 2021, 12, 1387–1397. [Google Scholar] [CrossRef]
- Malboeuf-Hurtubise, C.; Léger-Goodes, T.; Mageau, G.A.; Joussemet, M.; Herba, C.; Chadi, N.; Lefrançois, D.; Camden, C.; Bussières, È.-L.; Taylor, G.; et al. Philosophy for children and mindfulness during COVID-19: Results from a randomized cluster trial and impact on mental health in elementary school students. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 107, 110260. [Google Scholar] [CrossRef]
- Kubo, A.; Kurtovich, E.; McGinnis, M.; Aghaee, S.; Altschuler, A.; Quesenberry, C., Jr.; Kolevska, T.; Liu, R.; Greyz-Yusupov, N.; Avins, A. Pilot pragmatic randomized trial of mHealth mindfulness-based intervention for advanced cancer patients and their informal caregivers. Psychooncology 2020. [Google Scholar] [CrossRef] [PubMed]
- Mhende, J.; Bell, S.A.; Cottrell-Daniels, C.; Luong, J.; Streiff, M.; Dannenfelser, M.; Hayat, M.J.; Spears, C.A. Mobile Delivery of Mindfulness-Based Smoking Cessation Treatment Among Low-Income Adults During the COVID-19 Pandemic: Pilot Randomized Controlled Trial. JMIR Res 2021, 5, e25926. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | SPB | M | SPB + M | |
|---|---|---|---|---|
| Gender (F/M) | 12/6 | 4/1 | 4/2 | 4/3 |
| Age (M yrs, SD) | 24.2 (2.9) | 24.6 (2.1) | 23.7 (3.7) | 24.3 (3.1) |
| Ethnicity | ||||
| Hispanic | 2 | 1 | 1 | 0 |
| Non-Hispanic | 16 | 4 | 5 | 7 |
| Race | ||||
| Black or African American | 0 | 0 | 0 | 0 |
| Asian American | 5 | 1 | 1 | 3 |
| American Indian or Alaska Native | 0 | 0 | 0 | 0 |
| White | 11 | 3 | 4 | 4 |
| Other specified | 1 | 1 | 0 | 0 |
| Multi-racial | 1 | 0 | 1 | 0 |
| Baseline questionnaires | ||||
| Perceived Stress Scale (PSS-14) | 14.9 (5.1) | 18.6 (5.1) | 14.7 (5.5) | 12.4 (3.7) |
| Pittsburgh Sleep Quality Index (PSQI) | 4.2 (2.2) | 4 (3.6) | 4.2 (0.8) | 4.4 (2.2) |
| Mood and Anxiety Symptom Questionnaire (MASQ) | ||||
| General Distress | 16.2 (7.2) | 23.6 (8.6) | 14.8 (4.5) | 12 (3.6) |
| Anxious Arousal | 13.6 (5.2) | 18.8 (7.6) | 12 (2.3) | 11.3 (1.6) |
| Anhedonic Depression | 19.9 (5.4) | 22.4 (7.9) | 18.7 (4.8) | 19.1 (3.8) |
| Total mood disturbance | 49.7 (15.3) | 64.8 (21.5) | 45.5 (8.5) | 42.4 (4.6) |
| Big Five Inventory of personality (BFI) | ||||
| Extraversion | 27.3 (5.7) | 28.4 (3.6) | 26.5 (6.2) | 27.1 (7.1) |
| Agreeableness | 35.7 (4.5) | 36.2 (3.6) | 33 (4.4) | 37.6 (4.6) |
| Conscientiousness | 35.1 (5.7) | 35 (6.4) | 33.2 (6.1) | 36.9 (5.1) |
| Neuroticism | 20.7 (5.2) | 21.8 (5.4) | 22.7 (3.7) | 18.3 (5.7) |
| Openness | 32.3 (4.9) | 33.4 (5.2) | 32.2 (5.4) | 31.6 (5) |
| All | SPB | M | SPB + M | |
|---|---|---|---|---|
| Daily sleep logs (%) | ||||
| Pre | 96.4 (8.9) | 92.9 (16) | 96.4 (6) | 99 (2.7) |
| Post | 91.7 (17.4) | 100 (0) | 83.3 (28.1) | 92.9 (8.2) |
| Daily practice logs (%) | ||||
| Weeks 1–2 | 80.6 (24.5) | 85.7 (16.8) | 76.2 (27.4) | 80.6 (29.1) |
| Weeks 3–4 | 73.4 (23.1) | 75.7 (21.8) | 64.3 (32.3) | 79.6 (13.9) |
| Weeks 5–6 | 67.5 (26.4) | 68.6 (35.2) | 57.1 (28.9) | 75.5 (16.4) |
| Weeks 7–8 | 64.7 (31.6) | 72.9 (29.2) | 57.1 (41.4) | 65.3 (26.9) |
| Total | 72.8 (22.7) | 77.1 (24.5) | 64.9 (30.9) | 76.5 (13.3) |
| SPB | M | SPB + M | ||||
|---|---|---|---|---|---|---|
| pre | post | pre | post | pre | post | |
| Average breathing rate during practice | 6.0 (0) | 6.0 (0.2) | 11.9 (3.9) | 11.7 (5.1) | 6.0 (0) | 6.0 (0) |
| Langer Mindfulness Scale (LMS) | ||||||
| Total | 100.2 (11.5) | 99.6 (11.8) | 106.5 (13) | 111.7 (6.8) | 107.7 (10.4) | 109.7 (11.6) |
| Flexibility | 19.2 (1.6) | 18.8 (2.5) | 21 (3.7) | 23.2 (2.2) | 19.4 (3) | 19.6 (2) |
| Novelty seeking | 28.6 (8.7) | 29.6 (6.3) | 34.8 (5.5) | 34 (3.7) | 35.1 (2.7) | 34.7 (3.6) |
| Novelty producing | 26.6 (2.2) | 26 (2.5) | 25.3 (5.1) | 27.3 (4.5) | 26.3 (6.4) | 28.4 (6.3) |
| Engagement | 25.8 (3.8) | 25.2 (4.9) | 25.3 (4.8) | 27.2 (2.9) | 26.9 (2.7) | 27 (2.7) |
| Five Facet Mindfulness Questionnaire (FFMQ) | ||||||
| Total | 129 (24.5) | 123 (33.8) | 120.8 (9.9) | 122.7 (16.6) | 137.9 (8.1) | 138.4 (13.2) |
| Observe | 25 (6.2) | 24 (6.5) | 19.8 (3.1) | 22.8 (3.6) | 25.9 (2.7) | 26.9 (2.9) |
| Describe | 29.6 (7.4) | 27.2 (10.4) | 26.7 (5.3) | 26.7 (6.3) | 29.6 (3.9) | 29.7 (5) |
| Act with awareness | 26.6 (7.1) | 24.8 (9.6) | 26.3 (3.2) | 25.3 (4.2) | 28.7 (4.8) | 29.4 (5.3) |
| Non-judging of inner experience | 24.8 (9.1) | 23.4 (10.5) | 27.3 (8.8) | 25.3 (10.7) | 29.7 (6.6) | 29.7 (7.5) |
| Non-reactivity to inner experience | 23 (4.9) | 23.6 (6.1) | 20.7 (1.5) | 22.5 (2.9) | 24 (3.1) | 22.7 (4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, Y.; Yang, H.; Vazquez, M.; Buraks, O.; Haack, M.; Mullington, J.M.; Goldstein, M.R. Dismantling the Component-Specific Effects of Yogic Breathing: Feasibility of a Fully Remote Three-Arm RCT with Virtual Laboratory Visits and Wearable Physiology. Int. J. Environ. Res. Public Health 2023, 20, 3180. https://doi.org/10.3390/ijerph20043180
Ma Y, Yang H, Vazquez M, Buraks O, Haack M, Mullington JM, Goldstein MR. Dismantling the Component-Specific Effects of Yogic Breathing: Feasibility of a Fully Remote Three-Arm RCT with Virtual Laboratory Visits and Wearable Physiology. International Journal of Environmental Research and Public Health. 2023; 20(4):3180. https://doi.org/10.3390/ijerph20043180
Chicago/Turabian StyleMa, Yan, Huan Yang, Michael Vazquez, Olivia Buraks, Monika Haack, Janet M. Mullington, and Michael R. Goldstein. 2023. "Dismantling the Component-Specific Effects of Yogic Breathing: Feasibility of a Fully Remote Three-Arm RCT with Virtual Laboratory Visits and Wearable Physiology" International Journal of Environmental Research and Public Health 20, no. 4: 3180. https://doi.org/10.3390/ijerph20043180
APA StyleMa, Y., Yang, H., Vazquez, M., Buraks, O., Haack, M., Mullington, J. M., & Goldstein, M. R. (2023). Dismantling the Component-Specific Effects of Yogic Breathing: Feasibility of a Fully Remote Three-Arm RCT with Virtual Laboratory Visits and Wearable Physiology. International Journal of Environmental Research and Public Health, 20(4), 3180. https://doi.org/10.3390/ijerph20043180