

Systematic Review of Brain-Eating Amoeba: A Decade Update

 , , and
, , and
Abstract
1. Introduction
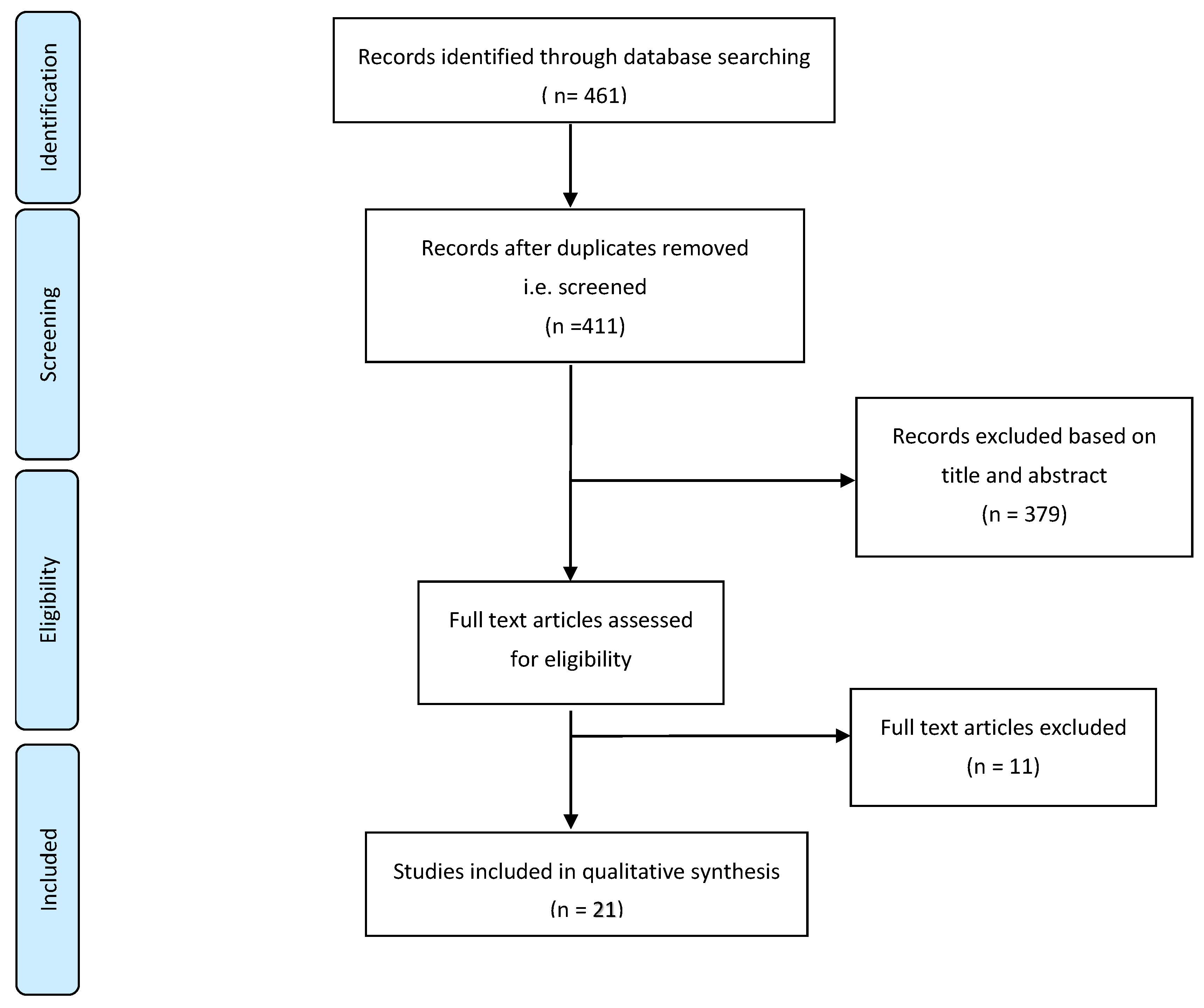
2. Methods
2.1. Selection Criteria
2.2. Operational Definition
2.3. Data Extraction Tool
2.4. Quality Assessment Tool
3. Results
Study Selection and Characteristics
4. Discussion
- Do not engage in water-based activities near warm, stagnant water, especially if the water is shallow, low, and has a weak flow rate;
- Pinch the nose or use a nose clip when taking part in water-related activities in potentially contaminated water;
- Keep the head above the water level when swimming in freshwater, hot springs, and other untreated thermal bodies of water;
- Avoid diving and jumping into stagnant freshwater;
- Do not to dig or stir up sediment from the bottom of bodies of water;
- Try to avoid water-related activities if there are any open cuts or wounds on the body.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pana, A.; Vini, V.; Arayamparambil, C.A. Amebic Meningoencephalitis; StatPearls Publishing: Tampa, FL, USA, 2022. [Google Scholar]
- Schuster, F.L.; Visvesvara, G.S. Free-living amoebae as opportunistic and non-opportunistic pathogens of humans and animals. Int. J. Parasitol. 2004, 34, 1001–1027. [Google Scholar] [CrossRef] [PubMed]
- Qvarnstrom, Y.; da Silva, A.J.; Schuster, F.L.; Gelman, B.B.; Visvesvara, G.S. Molecular confirmation of Sappinia pedata as a causative agent of amoebic encephalitis. J. Infect. Dis. 2009, 199, 1139–1142. [Google Scholar] [CrossRef] [PubMed]
- De Jonckheere, J.F. What do we know by now about the genus Naegleria? Exp. Parasitol. 2014, 145, S2–S9. [Google Scholar]
- Fowler, M.; Carter, R.F. Acute Pyogenic Meningitis Probably Due to Acanthamoeba sp.: A Preliminary Report. Br. Med. J. 1965, 2, 734–742. [Google Scholar] [CrossRef] [PubMed]
- Maclean, R.C.; Richardson, D.J.; LePardo, R.; Marciano-Cabral, F. The identification of Naegleria fowleri from water and soil samples by nested PCR. Parasitol. Res. 2004, 93, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Grace, E.; Asbill, S.; Virga, K. Naegleria fowleri: Pathogenesis, diagnosis, and treatment options. Antimicrob. Agents Chemother. 2015, 59, 6677–6681. [Google Scholar] [CrossRef]
- Visvesvara, G.S.; Moura, H.; Schuster, F.L. Pathogenic and opportunistic free-living amoebae: Acanthamoeba spp., Balamuthia mandrillaris, Naegleria fowleri, and Sappinia diploidea. FEMS Immunol. Med. Microbiol. 2007, 50, 1–26. [Google Scholar] [CrossRef]
- Cooper, A.M.; Aouthmany, S.; Shah, K.; Rega, P.P. Killer amoebas: Primary amoebic meningoencephalitis in a changing climate. JAAPA 2019, 32, 30–35. [Google Scholar] [CrossRef]
- Zahid, M.F.; Saad Shaukat, M.H.; Ahmed, B.; Beg, M.A.; Kadir, M.M.; Mahmood, S.F. Comparison of the clinical presentations of Naegleria fowleri primary amoebic meningoencephalitis with pneumococcal meningitis: A case-control study. Infection 2016, 44, 505–511. [Google Scholar] [CrossRef]
- Singh, P.; Kochhar, R.; Vashishta, R.K.; Khandelwal, N.; Prabhakar, S.; Mohindra, S.; Singhi, P. Amebic meningoencephalitis: Spectrum of imaging findings. AJNR. Am. J. Neuroradiol. 2006, 27, 1217–1221. [Google Scholar]
- Ong, T.Y.Y.; Khan, N.A.; Siddiqui, R. Brain-Eating Amoebae: Predilection Sites in the Brain and Disease Outcome. J. Clin. Microbiol. 2017, 55, 1989–1997. [Google Scholar] [CrossRef] [PubMed]
- Matanock, A.; Mehal, J.M.; Liu, L.; Blau, D.M.; Cope, J.R. Estimation of Undiagnosed Naegleria fowleri Primary Amebic Meningoencephalitis, United States. Emerg. Infect. Dis. 2018, 24, 162–164. [Google Scholar] [CrossRef] [PubMed]
- Saberi, R.; Seifi, Z.; Dodangeh, S.; Najafi, A.; Abdollah Hosseini, S.; Anvari, D.; Taghipour, A.; Norouzi, M.; Niyyati, M. A systematic literature review and meta-analysis on the global prevalence of Naegleria spp. in water sources. Transbound. Emerg. Dis. 2020, 67, 2389–2402. [Google Scholar] [CrossRef] [PubMed]
- Ithoi, I.; Ahmad, A.F.; Nissapatorn, V.; Lau, Y.L.; Mahmud, R.; Mak, J.W. Detection of Naegleria species in environmental samples from Peninsular Malaysia. PLoS ONE 2011, 6, e24327. [Google Scholar] [CrossRef]
- Richard, R.L.; Ithoi, I.; Abd Majid, M.A.; Wan Sulaiman, W.Y.; Tan, T.C.; Nissapatorn, V.; Lim, Y.A.L. Monitoring of Waterborne Parasites in Two Drinking Water Treatment Plants: A Study in Sarawak, Malaysia. Int. J. Environ. Res. Public Health 2016, 13, 641. [Google Scholar] [CrossRef]
- Gabriel, S.; Khan, N.A.; Siddiqui, R. Occurrence of free-living amoebae (Acanthamoeba, Balamuthia, Naegleria) in water samples in Peninsular Malaysia. J. Water Health 2018, 17, 160–171. [Google Scholar] [CrossRef]
- Gharpure, R.; Bliton, J.; Goodman, A.; Ali, I.K.M.; Yoder, J.; Cope, J.R. Epidemiology and Clinical Characteristics of Primary Amebic Meningoencephalitis Caused by Naegleria fowleri: A Global Review. Clin. Infect. Dis. 2021, 73, e19–e27. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar]
- Ma, L.-L.; Wang, Y.-Y.; Yang, Z.-H.; Huang, D.; Weng, H.; Zeng, X.-T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. Available online: https://pubmed.ncbi.nlm.nih.gov/23092060/ (accessed on 10 June 2020).
- Stowe, R.C.; Pehlivan, D.; Friederich, K.E.; Lopez, M.A.; DiCarlo, S.M.; Boerwinkle, V.L. Primary Amebic Meningoencephalitis in Children: A Report of Two Fatal Cases and Review of the Literature. Pediatr. Neurol. 2017, 70, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Cope, J.R.; Ratard, R.C.; Hill, V.R.; Sokol, T.; Causey, J.J.; Yoder, J.S.; Mirani, G.; Mull, B.; Mukerjee, K.A.; Narayanan, J.; et al. The first association of a primary amebic meningoencephalitis death with culturable Naegleria fowleri in tap water from a US treated public drinking water system. Clin. Infect. Dis. 2015, 60, e36–e42. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.O.; Cope, J.R.; Moskowitz, M.; Kahler, A.; Hill, V.; Behrendt, K.; Molina, L.; Fullerton, K.E.; Beach, M.J. Notes from the Field: Primary Amebic Meningoencephalitis Associated with Exposure to Swimming Pool Water Supplied by an Overland Pipe—Inyo County, California, 2015. MMWR. Morb. Mortal. Wkly. Rep. 2016, 65, 424. [Google Scholar] [CrossRef] [PubMed]
- Dunn, A.L.; Reed, T.; Stewart, C.; Levy, R.A. Naegleria fowleri that induces primary amoebic meningoencephalitis: Rapid diagnosis and rare case of survival in a 12-year-old Caucasian girl. Lab. Med. 2016, 47, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Heggie, T.W.; Küpper, T. Surviving Naegleria fowleri infections: A successful case report and novel therapeutic approach. Travel Med. Infect. Dis. 2017, 16, 49–51. [Google Scholar] [CrossRef]
- Cope, J.R.; Murphy, J.; Kahler, A.; Gorbett, D.G.; Ali, I.; Taylor, B.; Corbitt, L.; Roy, S.; Lee, N.; Roellig, D.; et al. Primary Amebic Meningoencephalitis Associated with Rafting on an Artificial Whitewater River: Case Report and Environmental Investigation. Clin. Infect. Dis. 2018, 66, 548–553. [Google Scholar] [CrossRef]
- Anjum, S.K.; Mangrola, K.; Fitzpatrick, G.; Stockdale, K.; Matthias, L.; Ali, I.K.M.; Cope, J.R.; O’Laughlin, K.; Collins, S.; Beal, S.G.; et al. A case report of primary amebic meningoencephalitis in North Florida. IDCases 2021, 25, e01208. [Google Scholar] [CrossRef]
- Yadav, D.; Aneja, S.; Dutta, R.; Maheshwari, A.; Seth, A. Youngest survivor of Naegleria meningitis. Indian J. Pediatr. 2013, 80, 253–254. [Google Scholar] [CrossRef]
- Sood, A.; Chauhan, S.; Chandel, L.; Jaryal, S.C. Prompt diagnosis and extraordinary survival from Naegleria fowleri meningitis: A rare case report. Indian J. Med. Microbiol. 2014, 32, 193–196. [Google Scholar] [CrossRef]
- Ravinder, K.; Uppal, B.; Aggarwal, P.; Mehra, B.; Hasan, F.; Mridul Daga, K. Co-infection of central nervous system by M. Tuberculosis, Cryptococcus and possibly Naegleria Fowleri. Trop. Biomed. 2016, 33, 387–392. [Google Scholar]
- Mittal, N.; Mahajan, L.; Hussain, Z.; Gupta, P.; Khurana, S. Primary amoebic meningoencephalitis in an infant. Indian J. Med. Microbiol. 2019, 37, 120–122. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Ruan, W.; Zhang, L.; Hu, B.; Yang, X. Primary amebic meningoencephalitis: A case report. Korean J. Parasitol. 2019, 57, 291–294. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Liang, X.; Han, Y.; Zhang, Y.; Li, X.; Yang, Z. A pediatric case of primary amoebic meningoencephalitis due to Naegleria fowleri diagnosed by next-generation sequencing of cerebrospinal fluid and blood samples. BMC Infect. Dis. 2021, 21, 1251. [Google Scholar] [CrossRef]
- McLaughlin, A.; O’Gorman, T. A local case of fulminant primary amoebic meningoencephalitis due to Naegleria fowleri. Rural Remote Health 2019, 19, 4313. [Google Scholar] [CrossRef]
- Sazzad, H.M.S.; Luby, S.P.; Sejvar, J.; Rahman, M.; Gurley, E.S.; Hill, V.; Murphy, J.L.; Roy, S.; Cope, J.R.; Ali, I.K.M. A case of primary amebic meningoencephalitis caused by Naegleria fowleri in Bangladesh. Parasitol. Res. 2020, 119, 339–344. [Google Scholar] [CrossRef]
- Baral, R.; Vaidya, B. Fatal case of amoebic encephalitis masquerading as herpes. Oxf. Med. Case Rep. 2018, 2018, omy010. [Google Scholar] [CrossRef]
- Stubhaug, T.T.; Reiakvam, O.M.; Stensvold, C.R.; Hermansen, N.O.; Holberg-Petersen, M.; Antal, E.A.; Gaustad, K.; Førde, I.S.; Heger, B. Fatal primary amoebic meningoencephalitis in a Norwegian tourist returning from Thailand. JMM Case Rep. 2016, 3, e005042. [Google Scholar] [CrossRef]
- Mushtaq, M.Z.; Mahmood, S.B.Z.; Aziz, A. A Fatal Case of Primary Amoebic Meningoencephalitis (PAM) Complicated with Diabetes Insipidus (DI): A Case Report and Review of the Literature. Case Rep. Infect. Dis. 2020, 2020, 4925819. [Google Scholar] [CrossRef]
- Su, M.Y.; Lee, M.S.; Shyu, L.Y.; Lin, W.C.; Hsiao, P.C.; Wang, C.P.; Der Ji, D.; Chen, K.M.; Lai, S.C. A fatal case of Naegleria fowleri meningoencephalitis in Taiwan. Korean J. Parasitol. 2013, 51, 203–206. [Google Scholar] [CrossRef]
- Celik, Y.; Arslankoylu, A.E. A Newborn with Brain-Eating Ameba Infection. J. Trop. Pediatr. 2021, 67, fmaa100. [Google Scholar] [CrossRef]
- Chomba, M.; Mucheleng’anga, L.A.; Fwoloshi, S.; Ngulube, J.; Mutengo, M.M. A case report: Primary amoebic meningoencephalitis in a young Zambian adult. BMC Infect. Dis. 2017, 17, 532. [Google Scholar] [CrossRef]
- Gharpure, R.; Gleason, M.; Salah, Z.; Blackstock, A.J.; Hess-Homeier, D.; Yoder, J.S.; Ali, I.K.M.; Collier, S.A.; Cope, J.R. Geographic Range of Recreational Water-Associated Primary Amebic Meningoencephalitis, United States, 1978–2018. Emerg. Infect. Dis. 2021, 27, 271–274. [Google Scholar] [CrossRef] [PubMed]
- Tabassum, S.; Naeem, A.; Gill, S.; Mumtaz, N.; Khan, M.Z.; Tabassum, S.; Naeem, R.; Mukherjee, D. Increasing cases of Naegleria fowleri during the time of COVID 19; an emerging concern of Pakistan. Int. J. Surg. 2022, 105, 106881. [Google Scholar] [CrossRef] [PubMed]
- Panda, A.; Mirdha, B.R.; Rastogi, N.; Kasuhik, S. Understanding the true burden of “Naegleria fowleri” (Vahlkampfiidae) in patients from Northern states of India: Source tracking and significance. Eur. J. Protistol. 2020, 76, 125726. [Google Scholar] [CrossRef] [PubMed]
- Yoder, J.S.; Eddy, B.A.; Visvesvara, G.S.; Capewell, L.; Beach, M.J.; Panda, A.; Mirdha, B.R.; Rastogi, N.; Kasuhik, S. The epidemiology of primary amoebic meningoencephalitis in the USA, 1962–2008. Epidemiol. Infect. 2020, 138, 968–975. [Google Scholar] [CrossRef]
- Heggie, T.W. Swimming with death: Naegleria fowleri infections in recreational waters. Travel Med. Infect. Dis. 2010, 8, 201–206. [Google Scholar] [CrossRef]
- da Rocha-Azevedo, B.; Tanowitz, H.B.; Marciano-Cabral, F. Diagnosis of infections caused by pathogenic free-living amoebae. Interdiscip. Perspect. Infect. Dis. 2009, 2009, 251406. [Google Scholar] [CrossRef]
- Madarová, L.; Trnková, K.; Feiková, S.; Klement, C.; Obernauerová, M. A real-time PCR diagnostic method for detection of Naegleria fowleri. Exp. Parasitol. 2010, 126, 37–41. [Google Scholar] [CrossRef]
- Siddiqui, R.; Ali, I.K.M.; Cope, J.R.; Khan, N.A. Biology and pathogenesis of Naegleria fowleri. Acta Trop. 2016, 164, 375–394. [Google Scholar] [CrossRef]
- Maciver, S.K.; Piñero, J.E.; Lorenzo-Morales, J. Is Naegleria fowleri an Emerging Parasite? Trends Parasitol. 2020, 36, 19–28. [Google Scholar] [CrossRef]
- Güémez, A.; García, E. Primary Amoebic Meningoencephalitis by Naegleria fowleri: Pathogenesis and Treatments. Biomolecules 2021, 11, 1320. [Google Scholar] [CrossRef]
- Jahangeer, M.; Mahmood, Z.; Munir, N.; Waraich, U.-E.-A.; Tahir, I.M.; Akram, M.; Ali Shah, S.M.; Zulfqar, A.; Zainab, R. Naegleria fowleri: Sources of infection, pathophysiology, diagnosis, and management; a review. Clin. Exp. Pharmacol. Physiol. 2020, 47, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Pugh, J.J.; Levy, R.A. Naegleria fowleri: Diagnosis, Pathophysiology of Brain Inflammation, and Antimicrobial Treatments. ACS Chem. Neurosci. 2016, 7, 1178–1179. [Google Scholar] [CrossRef] [PubMed]
- Sohn, H.-J.; Song, K.-J.; Kang, H.; Ham, A.-J.; Lee, J.-H.; Chwae, Y.-J.; Kim, K.; Park, S.; Kim, J.-H.; Shin, H.-J. Cellular characterization of actin gene concerned with contact-dependent mechanisms in Naegleria fowleri. Parasite Immunol. 2019, 41, e12631. [Google Scholar] [CrossRef] [PubMed]
- Cervantes-Sandoval, I.; de Jesús Serrano-Luna, J.; Meza-Cervantez, P.; Arroyo, R.; Tsutsumi, V.; Shibayama, M. Naegleria fowleri induces MUC5AC and pro-inflammatory cytokines in human epithelial cells via ROS production and EGFR activation. Microbiology 2009, 155 Pt 11, 3739–3747. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; Sohn, H.-J.; Yoo, J.-K.; Kang, H.; Seong, G.-S.; Chwae, Y.-J.; Kim, K.; Park, S.; Shin, H.-J. NLRP3 Inflammasome Activation in THP-1 Target Cells Triggered by Pathogenic Naegleria fowleri. Infect. Immun. 2016, 84, 2422–2428. [Google Scholar] [CrossRef]
- Engelborghs, S.; Niemantsverdriet, E.; Struyfs, H.; Blennow, K.; Brouns, R.; Comabella, M.; Dujmovic, I.; van der Flier, W.; Frölich, L.; Galimberti, D.; et al. Consensus guidelines for lumbar puncture in patients with neurological diseases. Alzheimer’s Dement. 2017, 8, 111–126. [Google Scholar] [CrossRef]
- Martinez, A.J.; Visvesvara, G.S. Free-living, amphizoic and opportunistic amebas. Brain Pathol. 1997, 7, 583–598. [Google Scholar] [CrossRef]
- Fotedar, R.; Stark, D.; Beebe, N.; Marriott, D.; Ellis, J.; Harkness, J. Laboratory diagnostic techniques for Entamoeba species. Clin. Microbiol. Rev. 2007, 20, 511–532. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Naegleria fowleri—Primary Amebic Meningoencephalitis (PAM)—Amebic Encephalitis [Internet]. 2022. Available online: https://www.cdc.gov/parasites/naegleria/diagnosis.html (accessed on 20 December 2022).


{kind=link}
| No | Citation | Country | Age (Year) | Sex | Exposure | Symptoms | Time to Onset | Full Blood Count | CSF Result | PCR Result | Survival |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Chen et al., 2019 [33] | China | 43 | Male | Waterpark activities; traveller | Fever; myalgia; fatigue; persistent occipital headache (for 2 days) | 5 days | Leucocytosis; CRP | Turbid; high pressure; glucose low; leucocyte high; protein high; Pandy’s test positive; trophozoites of N. fowleri with Wright–Giemsa stain | N. fowleri positive | Mortality |
| 2 | Celik and Arslankoylu 2021 [41] | Turkey | 11-day-old | Male | History of bathing with unchlorinated well water | Fever; inability to suck; irritability; convulsion (for 2 days) | 4 days | Leucocytosis; CRP | Leucocytosis; protein high; glucose low; negative for microbial growth, TORCH, acid-resistant bacilli, Ziehl–Neelsen staining | N. fowleri positive | Mortality |
| 3 | Ravinder et al., 2016 [31] | India | 15 | Male | Bathing in unclean village pond | Fever; vomiting; left-sided body weakness; convulsion; sudden loss of consciousness; jerky bilateral hand movement | No data | Leucocytosis | Direct microscopy—flagellated parasite and spherical budding yeast cells; latex agglutination test was positive for Cryptococcal antigen | Not performed | Survive at point of time |
| 4 | Chomba et al., 2017 [42] | Zambia | 24 | Male | Swimming in river; police recruit at training camp | Fever; convulsion | 2 days | No data | No bacterial or fungal pathogens were detected in CSF day 1 and day 3; numerous highly motile amoebic trophozoites and cysts day 8 | N. fowleri positive | Mortality |
| 5 | Stowe et al., 2017 * [22] | USA | 4 and 14 | Male | (1) Camping and swimming at lake | (1) Fever; convulsion; headache, vomiting; difficulty ambulating; altered mental status; (2) generalised muscle weakness; tactile fever; vomiting; confusion; convulsion | Both 8 days | No data | Grossly abnormal; (1) free-swimming amoebae | N. fowleri positive | Mortality |
| 6 | McLaughlin and O’Gorman 2019 [35] | Australia | 56 | Male | Swimming in stagnant water that was also accessed by cattle; irrigating nostrils | Headache; photophobia; nausea; vomiting; neck stiffness | No data | No data | Turbid; glucose low; protein high; leucocytosis; free-living amoebae | N. fowleri positive | Mortality |
| 7 | Cope et al., 2018 [27] | USA | 18 | Female | Freshwater swimming; water rafting activities | Fever; headache; lethargy | 14 days | No data | High pressure; leucocytosis; glucose low; protein high; wet mount of the CSF revealed possible motile trophozoites | N. fowleri positive, with concomitant detection of Balamuthia mandrillaris and Acanthamoeba spp. | Mortality |
| 8 | Sazzad et al., 2020 [36] | Bangladesh | 15 | Male | Bathing and contact with untreated ground water and river; irrigating nostrils | Fever; generalised headache; vomiting; weakness; neck stiffness; unconscious | No data | No data | Protein high; glucose low; leucocytosis; negative Ziehl–Neelsen stain and acid-fast bacilli | N. fowleri positive | Mortality |
| 9 | Stubhaug et al., 2016 [38] | Norway | 71 | Female | Travel to Thailand where hotel was supplied with untreated groundwater well; irrigating nostrils | Nausea; vomiting; fever; fatigue; | No data | Leucocytosis; CRP | Turbid; pressure high; glucose low; protein high; leucocytosis; negative nigrosin, acridine orange stain; equivocal cryptococcal latex antibody | N. fowleri positive | Mortality |
| 10 | Baral and Vaidya 2018 [37] | Nepal | 74 | Male | Nil | Fever; global headache; feature of anomic aphasia but no vomiting, seizure, or neurological deficit at presentation; altered sensorium and agitation; gradual weakness of bilateral lower limb and trunks | No data | No data | Leucocytosis; protein high; glucose low; negative for microbial growth, TB, AFB, HSV | Not performed | Mortality |
| 11 | Johnson et al., 2016 [24] | USA | 21 | Female | Swimming in private pool in a desert environment—not being chemically treated. Water supplied to the pool was from a mountain spring | Headache; nausea; vomiting; | 14 days | No data | Not mentioned | N. fowleri positive | Mortality |
| 12 | Huang et al., 2021 [34] | China | 8 | Male | Swimming in lake | Fever; headache; vomiting; altered consciousness; convulsion | 3 days | Leucocytosis; CRP | Leucocytosis; glucose low; protein high; pale, pink, thick necrotic fluid drawn out from the syringe | N. fowleri positive | Mortality |
| 13 | Mushtaq et al., 2020 [39] | Pakistan | 44 | Male | Not mentioned | Fever; worsening headache; generalised weakness | No data | Leucocytosis; | Leucocytosis; negative Gram stain, India ink, cryptococcal antigen; positive wet prep for Naegleria | N. fowleri positive | Mortality |
| 14 | Mittal et al., 2019 [32] | India | 8 months | Female | Nil | Fever; chills; rigors; abnormal body movement; vomiting; generalised tonic–clonic seizures; decreased oral intake; decrease urine output | No data | Microcytic hypochromic anaemia; raised CRP | High pressure; protein high; glucose low; leucocytosis; wet mount positive for moving trophozoites of amoeba; negative for India ink, Gram stain | N. fowleri positive | Survive at point of time (AOR) |
| 15 | Yadav et al., 2013 [29] | India | 25-day-old | Male | Untreated water well used for bathing | Fever; reduced feeding; multi-focal seizures (for 10 days) | No data | Leucocytosis; CRP | Leucocytosis; glucose low; protein high; CSF wet mount examination revealed presence of free-living motile amebae | Not performed | Survival |
| 16 | Dunn et al., 2016 [25] | USA | 12 | Female | Swimming at freshwater park | Fever; headache; lethargy; nausea; vomiting | 7 days | Leucocytosis | Milky colour; high turbidity; leucocytosis; Giemsa stain positive for Naegleria spp. | N. fowleri positive | Survival |
| 17 | Sood et al., 2014 [30] | India | 6 | Male | Collateral history—the boy played frequently with water stored in a cement tank used for varied purposes. The water was collected from a nearby diversion channel called “kuhl” | Fever; headache; altered sensorium | No data | Raised ESR | Clear colour; leucocytosis; negative Gram stain, India ink, Ziehl–Neelsen; positive wet mount revealed amoebic and flagellate trophozoites | Not performed | Survival |
| 18 | Cope et al., 2015 [23] | USA | 4 | Male | Water exposure: tap water that was used to supply water to a lawn water slide on which the child had played extensively | Diarrhoea; vomiting; poor oral intake; severe headache; fever; convulsion; lethargy | No data | Leucocytosis | Colourless; pressure high; protein high; leucocytosis; negative Gram stain | N. fowleri positive | Mortality |
| 19 | Anjum et al., 2021 [28] | USA | 13 | Male | Swimming at water park—untreated water supply | Headache; fever; intractable emesis; poor oral intake | 3 days | Leucocytosis; raised CRP | Pressure high; turbid; glucose low; protein high; leucocytosis; EVD protein high; Wright–Giemsa stain showed amoebic trophozoites | N. fowleri positive | Mortality |
| 20 | Su et al., 2013 [40] | Taiwan | 75 | Male | Thermal hot spring | Fever; headache; right arm myoclonic seizure; right-sided limb weakness | No data | Leucocytosis; raised CRP | Turbid; glucose low; protein high; leucocytosis; negative for India ink, Gram stain, AFB, fungi, viral; wet mount smear positive for trophozoites | N. fowleri positive | Mortality |
| 21 | Heggie and Küpper 2017 [26] | USA | 12 | Female | Swimming at lake-based water park (shallow depth and sandy bottom) | Fever; vomiting; headache; difficulty waking up from sleep; difficulty holding head up; unable to open eyes; hallucination | Less than 1 week | No data | N. fowleri | Not performed | Survival |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmad Zamzuri, M.‘A.I.; Abd Majid, F.N.; Mihat, M.; Ibrahim, S.S.; Ismail, M.; Abd Aziz, S.; Mohamed, Z.; Rejali, L.; Yahaya, H.; Abdullah, Z.; et al. Systematic Review of Brain-Eating Amoeba: A Decade Update. Int. J. Environ. Res. Public Health 2023, 20, 3021. https://doi.org/10.3390/ijerph20043021
Ahmad Zamzuri M‘AI, Abd Majid FN, Mihat M, Ibrahim SS, Ismail M, Abd Aziz S, Mohamed Z, Rejali L, Yahaya H, Abdullah Z, et al. Systematic Review of Brain-Eating Amoeba: A Decade Update. International Journal of Environmental Research and Public Health. 2023; 20(4):3021. https://doi.org/10.3390/ijerph20043021
Chicago/Turabian StyleAhmad Zamzuri, Mohd ‘Ammar Ihsan, Farah Nabila Abd Majid, Massitah Mihat, Siti Salwa Ibrahim, Muhammad Ismail, Suriyati Abd Aziz, Zuraida Mohamed, Lokman Rejali, Hazlina Yahaya, Zulhizzam Abdullah, and et al. 2023. "Systematic Review of Brain-Eating Amoeba: A Decade Update" International Journal of Environmental Research and Public Health 20, no. 4: 3021. https://doi.org/10.3390/ijerph20043021
APA StyleAhmad Zamzuri, M. ‘A. I., Abd Majid, F. N., Mihat, M., Ibrahim, S. S., Ismail, M., Abd Aziz, S., Mohamed, Z., Rejali, L., Yahaya, H., Abdullah, Z., Hassan, M. R., Dapari, R., & Mohd Isa, A. M. (2023). Systematic Review of Brain-Eating Amoeba: A Decade Update. International Journal of Environmental Research and Public Health, 20(4), 3021. https://doi.org/10.3390/ijerph20043021