1. Introduction
Suicide is a critical global public health issue; rates of suicide vary by sex, age, geographic region, cultural background, sexual preference and means. Prevention efforts have been increasing over time, in addition governmental prioritisation of suicide prevention on the national agenda [
1,
2] via universal or targeted means to address the factors associated with increased risk. The risk factors for suicide death are numerous and can have complex interactions; the stigma of suicide can further impact these risks by perpetuating suicidal thoughts or behaviours [
3] and increasing the potential for social exclusion, coercive treatment and contact with the justice system [
4]. The stigmatisation of suicide is also deemed to be a central barrier to seeking help and disclosing suicidality (incorporating suicidal ideation and behaviours) [
5] for oneself or for others in need of help [
1,
6]. As a broader effect of suicide stigma inhibiting help-seeking, people may suffer additional preventable physical and mental distress, relationship breakdown, personal stigma and loss of life satisfaction and opportunities [
7].
Suicide stigma is defined as the social disapproval or criticism of suicidal thoughts and behaviour and is an additional stressor among persons who experience or have experienced suicidality. This stigma is also experienced by people bereaved by suicide; some describe feeling blame towards themselves as they were unable to assist the person who died [
8,
9]. Suicide stigma towards oneself is defined as the internalisation of the negative stereotypes and can exacerbate shame and feelings of hopelessness, potentially blocking prevention efforts [
3]. Suicidal ideation has been shown to be more prevalent among individuals with high self-stigma [
10].
Most of the research investigating perceptions of suicide such as stigma or its converse—glorification—have been conducted in discrete community or clinical populations [
11,
12,
13,
14]. However, examining correlates of suicide stigma across different population groups using a representative cross-section of individuals could aid in the further understanding of where similarities or differences lie to better inform prevention activities.
Additional attitudes about suicide that may influence support for individuals experiencing suicidal distress include the glorification or normalisation of suicide. Glorifying suicide has been associated with lower suicide stigma; however, this conversely has a disturbing impact on suicide rates. Hom and colleagues quantified this in a large sample of career firefighters, finding that those who reported a previous suicide attempt during their career were more likely to normalise or glorify it, and this glorification was positively correlated with greater self-reported likelihood of future suicide attempts [
15].
There are many gaps in our understanding of the impact of culture on suicide stigma, despite broad evidence indicating higher stigma among non-Anglo cultures [
16]. Peel et al. [
17] identified cultural variations in conceptualisations of suicide with significant differences in willingness to acknowledge it as a concern in some cultures. For example, studies conducted in North America have identified a higher suicide stigma in their Indigenous people compared to their non-Indigenous counterparts [
18]. Despite significantly higher suicide rates among Indigenous Australians compared with their non-Indigenous counterparts [
19], there is negligible research considering the influence of cultural differences on suicide in Australia, although the impact of colonisation on Indigenous people has been proposed to contribute significantly [
20,
21].
Suicidality is well documented to differ substantially by sex, with higher rates of suicidal ideation among females and higher suicide death rates among males [
22]. Sexual identity and preference appears to exert an additional effect, where people identifying as lesbian, gay or bisexual are at an increased risk of lifetime suicide attempts compared to their heterosexual counterparts [
23], with some reports suggesting up to a six-fold increased risk [
24]. Suicide prevention efforts among sexual minorities that experience discrimination may be further hampered in the presence of suicide stigma [
25], and there is a need to better understand the measure of this disparity.
Despite its importance for suicide prevention, there have been few interventions to reduce suicide stigma in the general population and to support affected persons in dealing with suicide stigma [
26]. Further investigation of stigmatising attitudes in communities is needed and in the context of rigorous prevention efforts to understand and document what works. Across New South Wales (NSW), Australia, a population-scale, multi-level intervention called ‘LifeSpan’ [
27] has been trialled by the Black Dog Institute, providing this opportunity.
The LifeSpan trial expressed numerous aims, including to:
Increase awareness of suicide-related knowledge and decrease stigma towards suicide at the community-level and among relevant health professionals;
Promote help-seeking behaviours among those at risk;
Improve suicide literacy and stigma, particularly among people in gatekeeper roles (e.g., emergency services, teachers).
The aim of this study, therefore, was to investigate the association between the key socio-demographic factors that may increase a person’s expression of suicide stigma and to understand if self-reported levels of suicide stigma differed between people who have attempted suicide and general community members prior to the LifeSpan suicide prevention intervention.
2. Materials and Methods
This study comprised baseline cross-sectional survey data collected as part of the LifeSpan suicide prevention trial, which was previously described in detail [
27]. In brief, the LifeSpan intervention is an integrated suicide prevention framework consisting of nine evidence-based strategies, comprising universal, selective, and indicated interventions, which was implemented as a research trial across four distinct geographic regions in NSW, Australia, during a study period from April 2017–March 2020. To establish a baseline representation of the various sectors of the community and health service, surveys were conducted within selected groups of trial region populations and in various settings. The surveys were set up to capture whether there were changes in the attitudes, awareness and experiences of community and emergency department (ED) attendees over time due to potential exposure to the LifeSpan intervention.
2.1. Survey Populations and Recruitment
Survey participants represented members of the general community (“community survey”) and individuals who had attended EDs for suicidal crisis (“RESTORE”). The community survey was initiated to obtain demographic information, measures of suicidal ideation and behaviours and help-seeking from a sample across all trial sites. Prior to the implementation of any LifeSpan intervention within these regions, baseline data were obtained to assess beliefs, attitudes and knowledge around suicide. Subsequent community surveys were taken at various time points during and post the trial implementation; however, the data used in the current study represented only the baseline timepoint. Eligible community survey study participants were self-identified general community members, recruited predominantly online through paid Facebook advertisements. The survey was commenced following the provision of a study information sheet (online), whereby all persons gave their informed consent prior to their inclusion in the study; respondents were not reimbursed for their participation.
The RESTORE survey used a mixed-methods prospective cohort design with data collected from LifeSpan trial sites and control sites, which was detailed in the published study protocol [
28]. Eligible participants were individuals who had presented to an ED following a suicidal crisis in the prior 18 and 12 months for cohort one and two, respectively, and were recruited online through paid Facebook advertisements or via ED staff in participating trial sites who handed out study information flyers to eligible participants. The key data collected across both the community and RESTORE surveys formed the basis for the correlates of stigma included in the current study.
2.2. Survey Instruments and Variables
Consenting participants responded to a series of demographic questions including age, sex (male, female, non-binary), Indigenous status (Aboriginal, Torres Strait Islander, both, neither), marital status (married, de facto, single, divorced, separated, widowed) employment status (full-time, part-time, unemployed), residence (metropolitan, inner regional, outer regional/remote), sexual orientation (heterosexual, homosexual, bisexual, other), self-reported history of mental illness (Yes/No) or suicide attempt (Yes/No) and whether they had sought help in the past year for suicidality (Yes/No). The ‘Stigma of Suicide Scale’ (SOSS) [
29] was included in both surveys to assess attitudes towards people who die by suicide. The SOSS shows a three-factor structure, which has been replicated in multiple samples internationally [
29,
30,
31]. The sixteen-item short form of the SOSS was used in the present study, which included eight items assessing suicide stigma, four items assessing glorification/normalisation of suicide and four items attributing suicide to depression or isolation. Each item consisted of a one- or two-word descriptor of a person who dies by suicide, rated on a five-point Likert scale from (1) strongly disagree to (5) strongly agree. The subscales of the SOSS were calculated by obtaining the mean response to all items on the subscale, ranging from 1 to 5. The SOSS subscales have previously demonstrated robust internal consistency [
31]. The SOSS stigma subscale was used as the outcome measure for this study as a continuous numeric variable. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement [
32] was used to report the study management and findings appropriately.
2.3. Data Management and Assumptions
Data from the two surveys were appended after first cleaning and ensuring all variables were coded alike. Very few respondents categorised themselves as non-binary and were therefore also removed from the final dataset. Missingness was examined, and the median was imputed if missing at random for ≤5% for continuous variables (excluding any of the three SOSS subscales). Participants from the original survey populations who did not respond to any of the SOSS questions were excluded from the analysis. As the SOSS stigma subscale was used as the outcome of interest, respondents with less than 7 of the 8 subscale responses were excluded.
2.4. Statistical Analysis
All survey responses were entered into purpose-built Qualtrics survey databases and then downloaded into Microsoft Excel (Microsoft Corporation, Washington). Analysis for this study was conducted using STATAv16 [
33] and in RStudio [
34], with the figures being produced using the package ggplot2 [
35]. Variable reporting followed internationally standardised formats; parametric data were described using mean and standard deviations.
p-values of association were significant at <0.05. Predictors were assessed for multicollinearity using the ‘cor’ command. An ordinary least-squares regression model was fitted using the mean of the stigma subscale of the SOSS as the response variable [
29] and other variables of interest or significance as the predictors. Analysis was commenced by fitting a model with the mean of the SOSS score as the response and other variables of interest or significance as the predictors. The first full model comprised all predictors, and the second included the interaction terms of significance based on the initial exploratory data analysis in addition to all interactions with the sex variable. Model selection was conducted using the ‘step’ function in the R base package [
36], which was reduced by comparing all possible models sequentially by evaluation of Akaike’s information criterion (AIC). Variables removed throughout this stepwise process included marital status, interactions between sex and help-seeking, as well as mental illness diagnoses and employment status. The most parsimonious model was selected as that with the lowest AIC. Examination of the residuals was undertaken by creating a residual plot, plotting the least-squares residuals against ŷ. We assessed for the presence of heteroskedasticity for conducting the Breusch–Pagan test. The lmtest package [
37] and bptest function were used to evaluate our fitted model.
3. Results
Eligible respondents totalled 5426 individuals across the two combined surveys; 4283 (78.9%) from the community survey and 1143 (21.1%) from the RESTORE survey. The total respondents were predominantly female (71.4%) with a mean (SD) age of 41.7 (14.8) years, and 3.9% were identified as Indigenous. Around one third of the participants reported a previous suicide attempt (n = 1690, 31.5%), and almost two-thirds of the study population (n = 3545, 65.3%) had sought help for suicidality in the past year.
Table 1 describes the characteristics of the study population, presented by survey group and total.
ED attendees for suicidality from the RESTORE study were more likely to describe themselves as homosexual (8.3%) or bisexual (21.3%) than individuals from the community survey (4.5% and 6.8%, respectively). ED attendees were also more likely to report being single (60.6%) and unemployed (42.5%) than the community survey participants (20.8% and 26%, respectively).
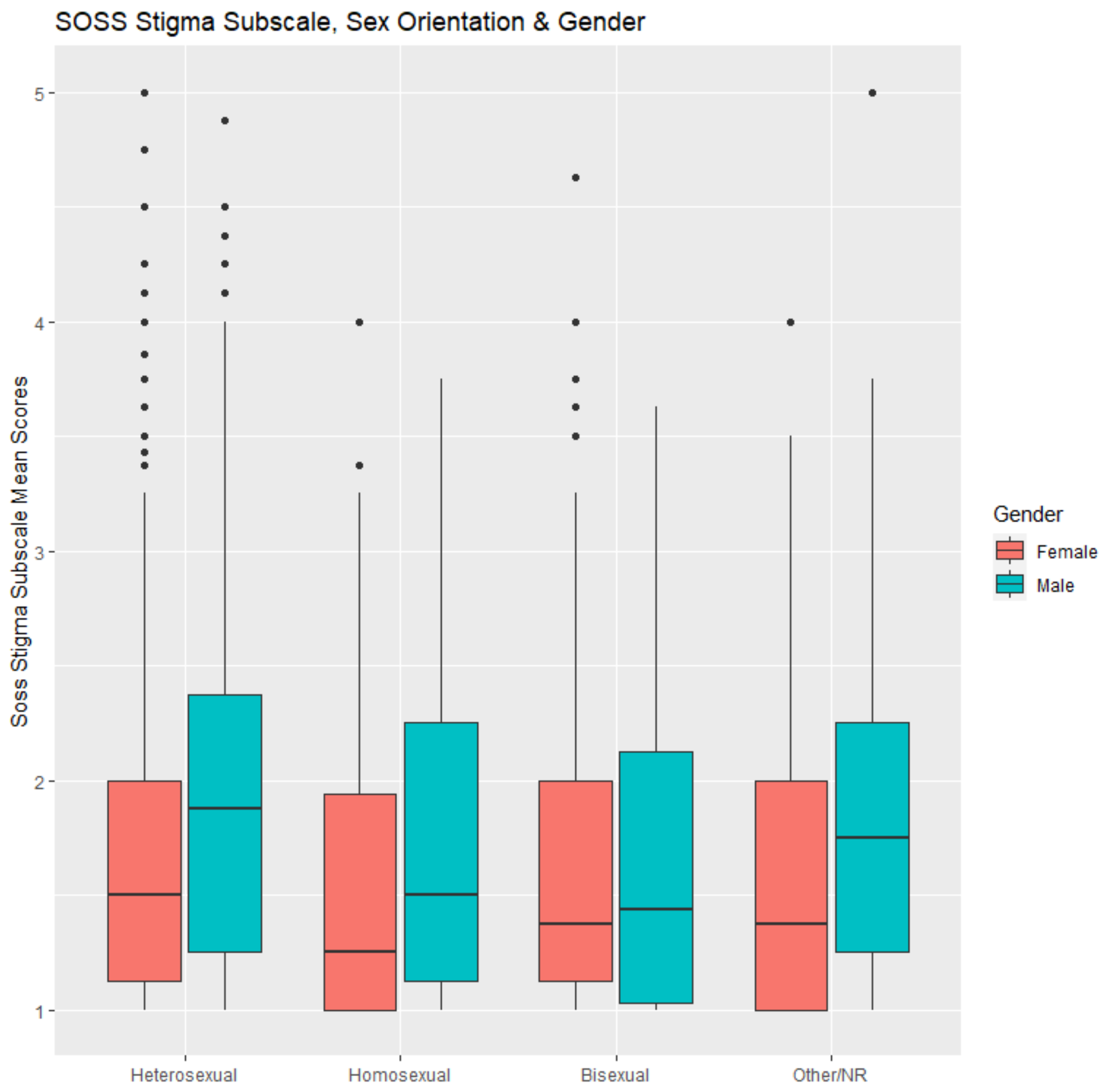
Further investigation of the summary values (mean [SD]) of the SOSS subscales showed distinctly higher stigma values among males, Indigenous persons and heterosexual participants (
Table 2). Glorification scores were highest among homosexual people, and scores for attribution to isolation were highest among bisexual people and Indigenous people.
Figure 1 shows a boxplot which depicts the differences in the distributions of the SOSS stigma subscale mean scores for males compared with females and across each category of sexual orientation, expanding on that shown in
Table 2.
After assessing for multicollinearity and finding −0.05 to be the highest value, we determined there was no evidence of multicollinearity. All the covariates retained in the most parsimonious model (selected as that with the lowest AIC) and their effect estimates are shown in
Table 3. Male sex was associated with the greatest magnitude of effect increasing the suicide stigma mean scores (compared to female sex) (β 0.527, 95%CI 0.375 to 0.626); however, higher glorification of suicide scores (SOSS subscale) were a substantial effect modifier for this (i.e., glorification had a larger negative impact on stigma for males than females), which was retained in the most parsimonious model as an interaction (β −0.075, 95%CI −0.119 to −0.030). To establish the veracity of this linear regression model, we performed a residuals analysis using the plot function. This showed a linear pattern, with the residuals in the qq-plot appearing normally distributed. The residual standard error was 0.639 on 5404 degrees of freedom. The Breusch–Pagen test for heteroskedasticity (LM-BP Test) result was 14.21. Therefore, the null hypothesis was rejected at the 5% level (χ2 0.05 ≈ 3.87,
p = 0.0001).
Indigenous status (compared to non-Indigenous status) was associated with a higher suicide stigma (β 0.123, 95%CI 0.074 to 0.172). Area of residence was also found to influence the suicide stigma scores, where higher scores were associated with outer regional or remote areas of residence compared with metropolitan areas (β 0.079, 95%CI 0.015 to 0.143). Finally, and to a lesser degree, the isolation subscale scores were associated with higher stigma of suicide scores (β 0.040, 95%CI 0.017 to 0.063).
Younger ages (continuous variable) demonstrated lower stigma scores (β −0.002, 95%CI −0.004 to −0.001), and sexual preference was also significantly associated with a lower stigma of suicide. Lower stigma scores were associated with homosexual and bisexual respondents compared to heterosexual respondents (β −0.127, 95%CI −0.182 to −0.021 and β −0.056, 95%CI −0.135 to −0.032 respectively). Male bisexuality was again associated with lower stigma scores (β −0.201, 95%CI −0.350 to −0.052).
Differences in the reported stigma of suicide were clear between the survey populations and were retained as significant in the final model, whereby participants attending an ED for suicidal crisis (RESTORE survey) had significantly higher stigma scores than participants in the community survey (β 0.08, 95%CI 0.036 to 0.132). The adjusted R2 in the final model was 0.17.
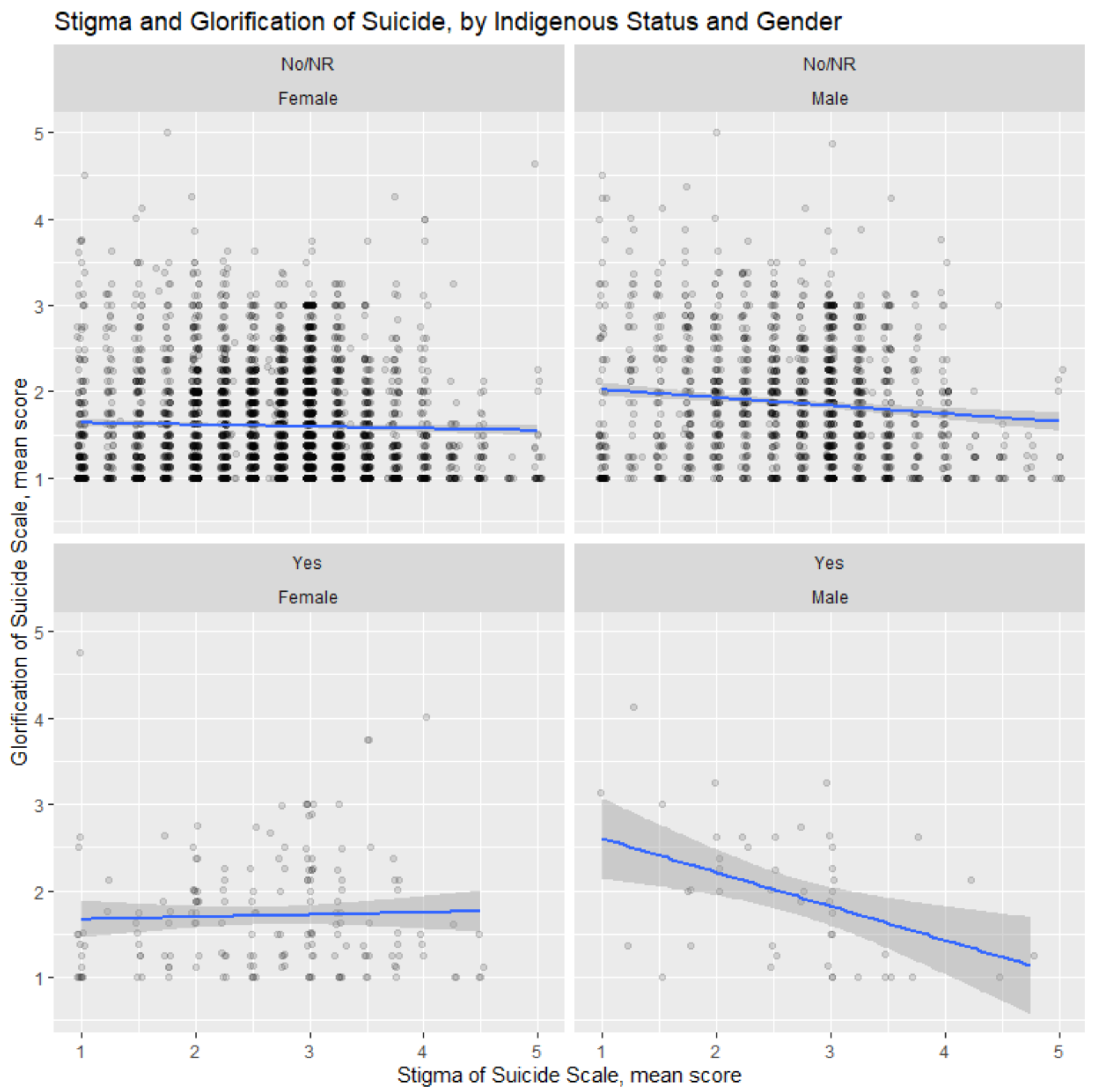
The mean scores for the SOSS subscales of suicide stigma and glorification differed by sex and Indigenous status. The stigma scores among Indigenous males contrasted significantly to Indigenous females, as demonstrated clearly in
Figure 2, whose plot was produced using the ggplot2 package in R. Indigenous male participants had greater reductions in stigma with a higher glorification compared to non-Indigenous males, where there were no differences in the relationship between Indigenous and non-Indigenous females.
4. Discussion
This study involved a large sample of two populations, where self-reported stigma of suicide was identified to be highest among Indigenous people, males, heterosexual persons and those living in outer regional or remote areas of NSW during the study period, 2017–2020. These findings contribute to and should be considered in the context of the developing evidence bases regarding Indigenous suicide research internationally, which focusses on holistic, culturally safe and strength-based approaches that promote social and emotional wellbeing.
Suicide rates among Indigenous Australians are twice that of the non-Indigenous population [
22]. The factors identified with heightened suicide among Indigenous Australians include challenges surrounding acculturation and minority group status, discrimination, socioeconomic deprivation, poverty, unemployment, and inequalities of access to healthcare and service provision [
38]. A greater understanding of the role of suicide stigma in pathways to Indigenous suicide can be used to encourage and foster resilience, as discussed by Dudgeon et al. [
20,
21].
No representative Australian data are available to reliably determine the rates of suicide and suicide attempts amongst the LGBTQI+ community, although the international literature indicates that minority sexual orientation is associated with an increased prevalence of suicidal behaviour [
39].
This study found that groups of people typically characterised as having a high suicide risk (Indigenous people and men) also had high suicide stigma scores, whereas stigma scores were comparatively low among homosexual and bisexual people, despite their documented levels of suicidality compared with heterosexual people [
23,
24]. The high suicide stigma in Indigenous populations may have developed alongside the historical mistrust of Western systems, including healthcare systems, which have largely ignored the importance of practicing, acknowledging and reclaiming culture as vital to Indigenous good health and wellbeing [
19,
40,
41]. The Australian Government created the National Aboriginal and Torres Strait Islander Suicide Prevention Strategy in 2013 [
42]; however, this did not specifically address stigma, and as such more needs to be done at the government and community levels to explore and address the links between the historical trauma associated with colonisation and the stigma of suicide among Indigenous Australians [
43]. A recently published scoping review, which thematically examined 72 articles about Indigenous suicide prevention, identified that culturally grounded suicide education and awareness initiatives reduced stigma towards suicide and increased willingness to seek help [
44]. Our study did not evaluate any past experiences with suicide prevention interventions.
The strengths of this study included the incorporation of novel factors associated with stigma, its large, diverse sample of general community and clinical populations, and a validated measure of suicide stigma.
This study had several limitations. While all the surveyed populations were asked a core set of questions that were compiled in one dataset for the purpose of this study, the groups within this study were comprised from two discrete studies and represented somewhat heterogenous and non-representative populations. Some measures were therefore notably higher in one group over the other. For example, individuals in the RESTORE study reported a higher prevalence of mental illness and/or suicide attempt than the other study group. The inclusion of the survey indicator as a factor in the model, however, attempted to account for this as much as possible. To the authors’ knowledge, the stigma of suicide scale (SOSS) has not been evaluated for its cultural appropriateness in Indigenous populations. This further work is needed, as the results may otherwise differ. Finally, as the baseline study was cross-sectional, the direction of effects could not be established.
The implications from the findings in this study include recommendations for a focus on education programs or campaigns [
45,
46,
47,
48], which have been previously researched and shown as effective. Other potentially effective approaches might include:
(1) Changes to health system policies and service pathways to better support individuals experiencing suicidal distress;
(2) Contact interventions to challenge stereotypes and promote messages related to recovery [
46];
(3) De-stigmatisation through media representation of suicide [
49];
(4) Peer services to destigmatise the treatment of suicidal distress;
(5) The development of alternatives to ED that are more person-centred, less stigmatising and with less potential for coercive control.
5. Conclusions
The results of this study suggested that suicide stigma was diverse across the population, varying by sociodemographic factors. Higher levels of suicide stigma were found among people identifying as Indigenous, male, and heterosexual after controlling for other relevant variables. This provided new information as to the higher-risk subgroups, within which there was also higher stigma. These identified subgroups of the population could benefit from targeted educational programs to address what is likely a higher risk of stigmatisation toward their peers. Campaign messages should focus on suicidality as a complex phenomenon with multiple interactive causes, many of which can be treated, supported, and addressed through multisystem and culturally sensitive approaches to suicide prevention.
Author Contributions
Study conceptualization, L.N.S., M.T. and F.S.; methodology, L.N.S.; formal analysis, L.N.S., A.L.C. and P.J.B.; investigation, M.T. and F.S.; data curation, S.Z.; writing—original draft preparation, L.N.S.; writing—review and editing, AC, P.J.B., M.T., L.M., D.R. and T.E.; Indigenous cultural guidance, T.E.; project administration, F.S.; funding acquisition, F.S. and M.T. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by an AUD 14.76 million grant from the Paul Ramsay Foundation for the period of 1 January 2016 until 31 December 2021. The design, management, analysis and reporting of the study were entirely independent of the Paul Ramsay Foundation.
Institutional Review Board Statement
The LifeSpan study was conducted in accordance with the Declaration of Helsinki and approved by the Hunter New England Human Research Ethics Committee (HREC) (approval number: 16/09/21/4.05). Ethics approval was also provided by the Aboriginal Health and Medical Research Council (approval number: 1232.16). Survey-specific approvals were obtained for the community survey from the Hunter New England HREC (HREC/16/HNE/399), and the RESTORE Emergency Department Study from the Hunter New England HREC (HREC/17/HNE/144). All studies were therefore performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data obtained from these surveys may be made available following request to the authors and only after human research ethics approval.
Acknowledgments
We acknowledge the valuable inputs of all study participants, without whom such insights would not be possible.
Conflicts of Interest
All authors declare that they do not have a financial relationship with the organization that sponsored the research, and all authors declare that they have no conflict of interest.
References
- Calear, A.L.; Batterham, P.J.; Christensen, H. Predictors of help-seeking for suicidal ideation in the community: Risks and opportunities for public suicide prevention campaigns. Psychiat. Res. 2014, 219, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.T.E.; Nicholas, J.; Shand, F.; Green, R.; Christensen, H. A comparison of multi-component systems approaches to suicide prevention. Australas. Psychiat. 2018, 26, 128–131. [Google Scholar] [CrossRef] [PubMed]
- Carpiniello, B.; Pinna, F. The Reciprocal Relationship between Suicidality and Stigma. Front. Psychiat. 2017, 8, 35. [Google Scholar] [CrossRef] [PubMed]
- Corrigan, P.; Kleinlein, P. The Impact of Mental Illness Stigma. In On the Stigma of Mental Illness: Practical Strategies for Research and Social Change; Corrigan, P.W., Ed.; American Psychological Association: Washington, DC, USA, 2005; pp. 11–44. [Google Scholar] [CrossRef]
- Calear, A.L.; Batterham, P.J. Suicidal ideation disclosure: Patterns, correlates and outcome. Psychiat. Res. 2019, 278, 1–6. [Google Scholar] [CrossRef]
- Naghavi, M. Global, regional, and national burden of suicide mortality 1990 to 2016: Systematic analysis for the Global Burden of Disease Study 2016. BMJ 2019, 364, l94. [Google Scholar] [CrossRef]
- Ludwig, J.; Dreier, M.; Liebherz, S.; Härter, M.; von dem Knesebeck, O. Suicide literacy and suicide stigma–results of a population survey from Germany. J. Ment. Health 2021, 31, 517–523. [Google Scholar] [CrossRef]
- Cvinar, J.G. Do Suicide Survivors Suffer Social Stigma: A Review of the Literature. Perspect. Psychiat. Care 2005, 41, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Pitman, A.L.; Stevenson, F.; Osborn, D.P.; King, M.B. The stigma associated with bereavement by suicide and other sudden deaths: A qualitative interview study. Soc. Sci. Med. 2018, 198, 121–129. [Google Scholar] [CrossRef]
- Oexle, N.; Rüsch, N.; Viering, S.; Wyss, C.; Seifritz, E.; Xu, Z.; Kawohl, W. Self-stigma and suicidality: A longitudinal study. Eur. Arch. Psychiat. Clin. Neurosci. 2017, 267, 359–361. [Google Scholar] [CrossRef]
- Kennedy, A.J.; Brumby, S.A.; Versace, V.L.; Brumby-Rendell, T. The ripple effect: A digital intervention to reduce suicide stigma among farming men. BMC Public Health 2020, 20, 813. [Google Scholar] [CrossRef]
- Al-Shannaq, Y.; Aldalaykeh, M. Suicide literacy, suicide stigma, and psychological help seeking attitudes among Arab youth. Curr. Psychol. 2021, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Batterham, P.J.; Calear, A.L.; Christensen, H. Correlates of suicide stigma and suicide literacy in the community. Suicide Life-Threat. Behav. 2013, 43, 406–417. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Segarra, E.; Rosario-Hernández, E.; Carminelli-Corretjer, P.; Tollinchi-Natali, N.; Polanco-Frontera, N. Suicide stigma among medical students in Puerto Rico. Int. J. Environ. Res. Public Health 2018, 15, 1366. [Google Scholar] [CrossRef] [PubMed]
- Hom, M.A.; Stanley, I.H.; Duffy, M.E.; Davis, L.; Joiner, T.E. Examining the relationship between attitudes toward suicide and suicide attempt history. Crisis 2018, 40, 4. [Google Scholar] [CrossRef]
- Money, T.T.; Batterham, P.J. Sociocultural factors associated with attitudes toward suicide in Australia. Death Stud. 2021, 45, 219–225. [Google Scholar] [CrossRef]
- Peel, R.; Buckby, B.; McBain, K. Comparing the effect of stigma on the recognition of suicide risk in others between Australia and Brazil. GSTF J. Psychol. 2017, 3, 2. [Google Scholar] [CrossRef]
- Wexler, L.M.; Gone, J.P. Culturally responsive suicide prevention in indigenous communities: Unexamined assumptions and new possibilities. Am. J. Public Health 2012, 102, 800–806. [Google Scholar] [CrossRef]
- Brown, K.; Toombs, M.; Nasir, B.; Kisely, S.; Ranmuthugala, G.; Brennan-Olsen, S.L.; Nicholson, G.C.; Gill, N.S.; Hayman, N.S.; Kondalsamy-Chennakesavan, S. How can mobile applications support suicide prevention gatekeepers in Australian Indigenous communities? Soc. Sci. Med. 2020, 258, 113015. [Google Scholar] [CrossRef]
- Dudgeon, P.; Bray, A.; Walker, R. Self-determination and strengths-based Aboriginal and Torres Strait Islander suicide prevention: An emerging evidence-based approach. In Alternatives to Suicide: Beyond Risk and toward a Life Worth Living; Page, A., Stritzke, W., Eds.; Academic Press: Cambridge, MA, USA, 2020; pp. 237–256. [Google Scholar] [CrossRef]
- Dudgeon, P.; Bray, A.; Ring, I.; McPhee, R. Beyond Evidence-Deficit Narratives in Indigenous Suicide Prevention; Indigenous Mental Health and Suicide Prevention Clearinghouse: Canberra, Australia, 2021; Cat. no. IMH 6. [Google Scholar]
- Australian Bureau of Statistics. Causes of Death in Australia. 2020. Available online: https://www.abs.gov.au/statistics/health/causes-death/causes-death-australia/latest-release#key-statistics (accessed on 1 November 2022).
- LGBTIQ + Health Australia. Snapshot of Mental Health and Suicide Prevention Statistics for LGBTIQ + People. 2021. Available online: https://www.lgbtiqhealth.org.au/statistics (accessed on 1 November 2022).
- Haas, A.P.; Lane, A.; Working Group for Postmortem Identification of SO/GI. Collecting sexual orientation and gender identity data in suicide and other violent deaths: A step towards identifying and addressing LGBT mortality disparities. LGBT Health 2015, 2, 84–87. [Google Scholar] [CrossRef]
- Saewyc, E.M.; Li, G.; Gower, A.L.; Watson, R.J.; Erickson, D.; Corliss, H.L.; Eisenberg, M.E. The link between LGBTQ-supportive communities, progressive political climate, and suicidality among sexual minority adolescents in Canada. Prev. Med. 2020, 139, 106191. [Google Scholar] [CrossRef]
- Niederkrotenthaler, T.; Reidenberg, D.J.; Till, B.; Gould, M.S. Increasing Help-Seeking and Referrals for Individuals at Risk for Suicide by Decreasing Stigma: The Role of Mass Media. Am. J. Prev. Med. 2014, 47, S235–S243. [Google Scholar] [CrossRef]
- Shand, F.; Torok, M.; Cockayne, N.; Batterham, P.J.; Calear, A.L.; Mackinnon, A.; Martin, D.; Zbukvic, I.; Mok, K.; Chen, N.; et al. Protocol for a stepped-wedge, cluster randomized controlled trial of the LifeSpan suicide prevention trial in four communities in New South Wales, Australia. Trials 2020, 21, 332. [Google Scholar] [CrossRef] [PubMed]
- Rosebrock, H.; Chen, N.; Tye, M.; Mackinnon, A.; Calear, A.L.; Batterham, P.J.; Maple, M.; Rasmussen, V.-M.; Schroeder, L.; Cutler, H.; et al. Study protocol for a mixed methods prospective cohort study to explore experiences of care following a suicidal crisis in the Australian healthcare system. BMJ Open 2020, 10, e033814. [Google Scholar] [CrossRef] [PubMed]
- Batterham, P.J.; Calear, A.L.; Christensen, H. The Stigma of Suicide Scale. Psychometric properties and correlates of the stigma of suicide. Crisis 2013, 34, 13–21. [Google Scholar] [CrossRef]
- Williams, S.M.; Frey, L.M.; Stage, D.L.; Cerel, J. Exploring lived experience in gender and sexual minority suicide attempt survivors. Am. J. Orthopsychiat. 2018, 88, 691–700. [Google Scholar] [CrossRef]
- Ludwig, J.; Liebherz, S.; Dreier, M.; Härter, M.; von dem Knesebeck, O. The Stigma of Suicide Scale: Psychometric Validation of the German Short Version (SOSS-SF-D). Psychiat. Prax. 2020, 47, 433–439. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Stata Statistical Software, Version 15.1; Stata Corp: College Station, TX, USA, 2017.
- RS Team. RStudio: Integrated Development for R. RStudio; PBC: Boston, MA, USA, 2020. [Google Scholar]
- Wickham, R. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; ISBN 978-3-319-24277-4. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.R-project.org/ (accessed on 1 November 2022).
- Zeileis, A.; Hothorn, T. Diagnostic Checking in Regression Relationships. R News 2002, 2, 7–10. [Google Scholar]
- Dickson, J.M.; Cruise, K.; McCall, C.A.; Taylor, P.J. A Systematic Review of the Antecedents and Prevalence of Suicide, Self-Harm and Suicide Ideation in Australian Aboriginal and Torres Strait Islander Youth. Int. J. Env. Res. Public Health 2019, 16, 3154. [Google Scholar] [CrossRef]
- Plöderl, M.; Wagenmakers, E.-J.; Tremblay, P.; Ramsay, R.; Kralovec, K.; Fartacek, C.; Fartacek, R. Suicide Risk and Sexual Orientation: A Critical Review. Arch. Sex. Behav. 2013, 42, 715–727. [Google Scholar] [CrossRef]
- Backholer, K.; Baum, F.; Finlay, S.M.; Friel, S.; Giles-Corti, B.; Jones, A.; Patrick, R.; Shill, J.; Townsend, B.; Armstrong, F.; et al. Australia in 2030: What is our path to health for all? Med. J. Aust. 2021, 214, S5–S40. [Google Scholar] [CrossRef] [PubMed]
- Gupta, H.; Tari-Keresztes, N.; Stephens, D.; Smith, J.A.; Sultan, E.; Lloyd, S. A scoping review about social and emotional wellbeing programs and services targeting Aboriginal and Torres Strait Islander young people in Australia: Understanding the principles guiding promising practice. BMC Public Health 2020, 20, 1625. [Google Scholar] [CrossRef] [PubMed]
- Department of Health and Ageing. National Aboriginal and Torres Strait Islander Suicide Prevention Strategy; Department of Health and Ageing: Canberra, Australia, 2013.
- Smallwood, R.; Woods, C.; Power, T.; Usher, K. Understanding the Impact of Historical Trauma Due to Colonization on the Health and Well-Being of Indigenous Young Peoples: A Systematic Scoping Review. J. Transcult. Nurs. 2021, 32, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Sjoblom, E.; Ghidei, W.; Leslie, M.; James, A.; Bartel, R.; Campbell, S.; Montesanti, S. Centering Indigenous knowledge in suicide prevention: A critical scoping review. BMC Public Health 2022, 22, 2377. [Google Scholar] [CrossRef]
- Corrigan, P. On the Stigma of Mental Illness: Practical Strategies for Research and Social Change; American Psychological Association: Washington, DC, USA, 2005. [Google Scholar]
- Mehta, N.; Clement, S.; Marcus, E.; Stona, A.C.; Bezborodovs, N.; Evans-Lacko, S.; Palacios, J.; Docherty, M.; Barley, E.; Rose, D.; et al. Evidence for effective interventions to reduce mental health-related stigma and discrimination in the medium and long term: Systematic review. Br. J. Psychiat. 2015, 207, 377–384. [Google Scholar] [CrossRef]
- Dalky, H.F. Mental Illness Stigma Reduction Interventions: Review of Intervention Trials. West. J. Nurs. Res. 2011, 34, 520–547. [Google Scholar] [CrossRef]
- Morgan, A.J.; Reavley, N.J.; Ross, A.; Too, L.S.; Jorm, A.F. Interventions to reduce stigma towards people with severe mental illness: Systematic review and meta-analysis. J. Psychiat. Res. 2018, 103, 120–133. [Google Scholar] [CrossRef]
- Niederkrotenthaler, T.; Voracek, M.; Herberth, A.; Till, B.; Strauss, M.; Etzersdorfer, E.; Eisenwort, B.; Sonneck, G. Papageno vs. Werther effect. BMJ 2010, 341, c5841. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



 ,
, 



{kind=link}
{kind=link}