
Decreased Respiratory-Related Absenteeism among Preschool Students after Installation of Upper Room Germicidal Ultraviolet Light: Analysis of Newly Discovered Historical Data


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. The Source Document and Data
- Several documents that are likely internal company documents generated by GUV manufacturers or vendors, in particular Westinghouse (makers of a GUV lamp called “Sterilamp”) and Sanitron, a predecessor of Atlantic Ultraviolet. These corporate documents are identifiable either by the Westinghouse Lamp Division letterhead, or the appearance of a small “ASC-nnn” notation, where “nnn” is a number. This appears to be a notation used by Westinghouse Electric Corporation on some of its internal documents, as seen, for example, in the reference lists in a 1966 article about GUV by Minkin [22], and in a 1971 US Government Printing Office publication authored by Dubin–Mindell–Bloome Associates [23].
- Photocopies of short New York Times articles, labelled May 24 and 28, 1950, about GUV deployments and trials.
- A photocopy of an article presented at the 140th annual meeting of the Medical Society of the State of New York, section on pediatrics, on 2 May 1946, and published in the New York State Journal of Medicine [24].
2.2. Statistical Analysis
2.3. Reviews and Approvals
3. Results
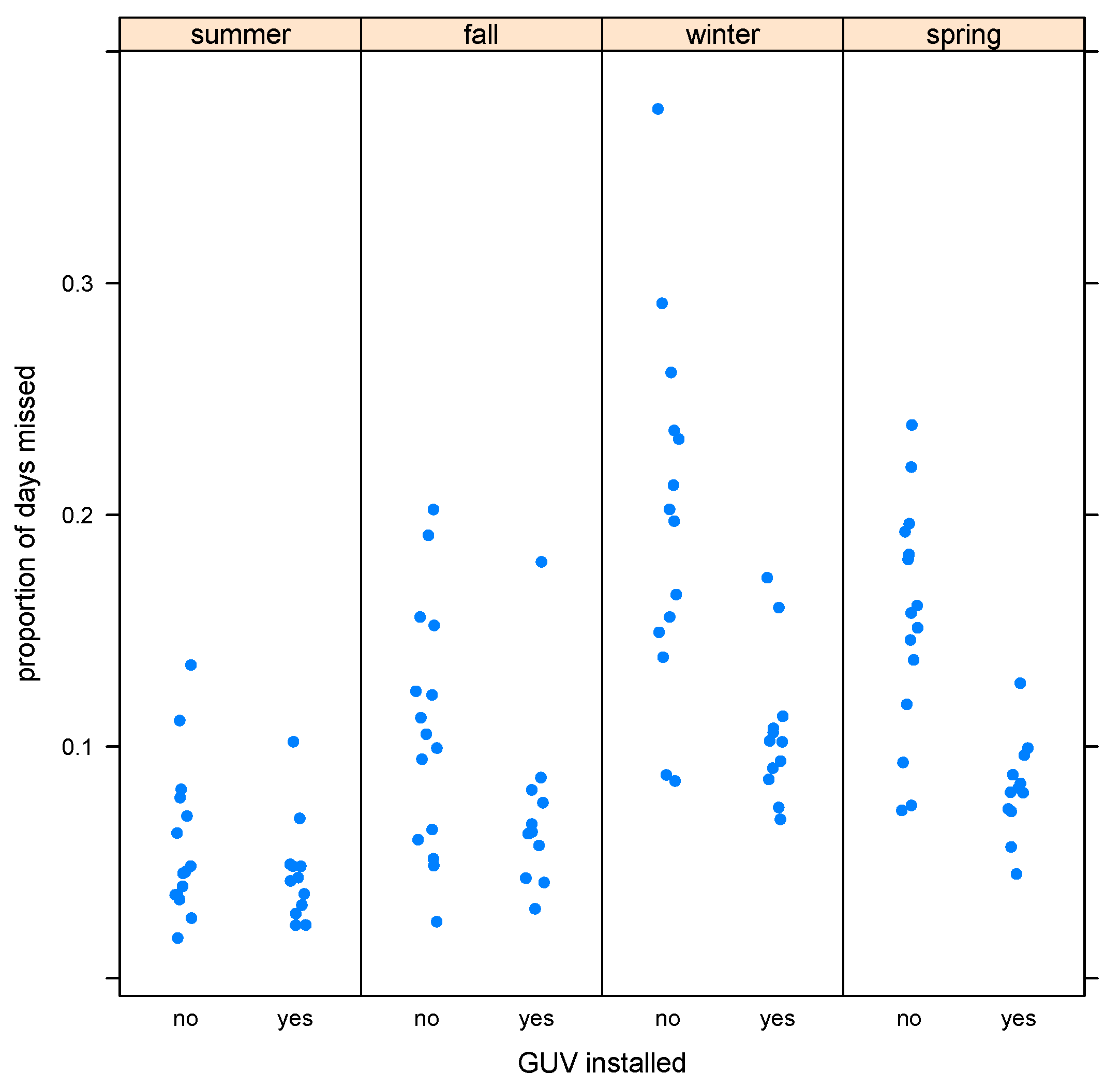
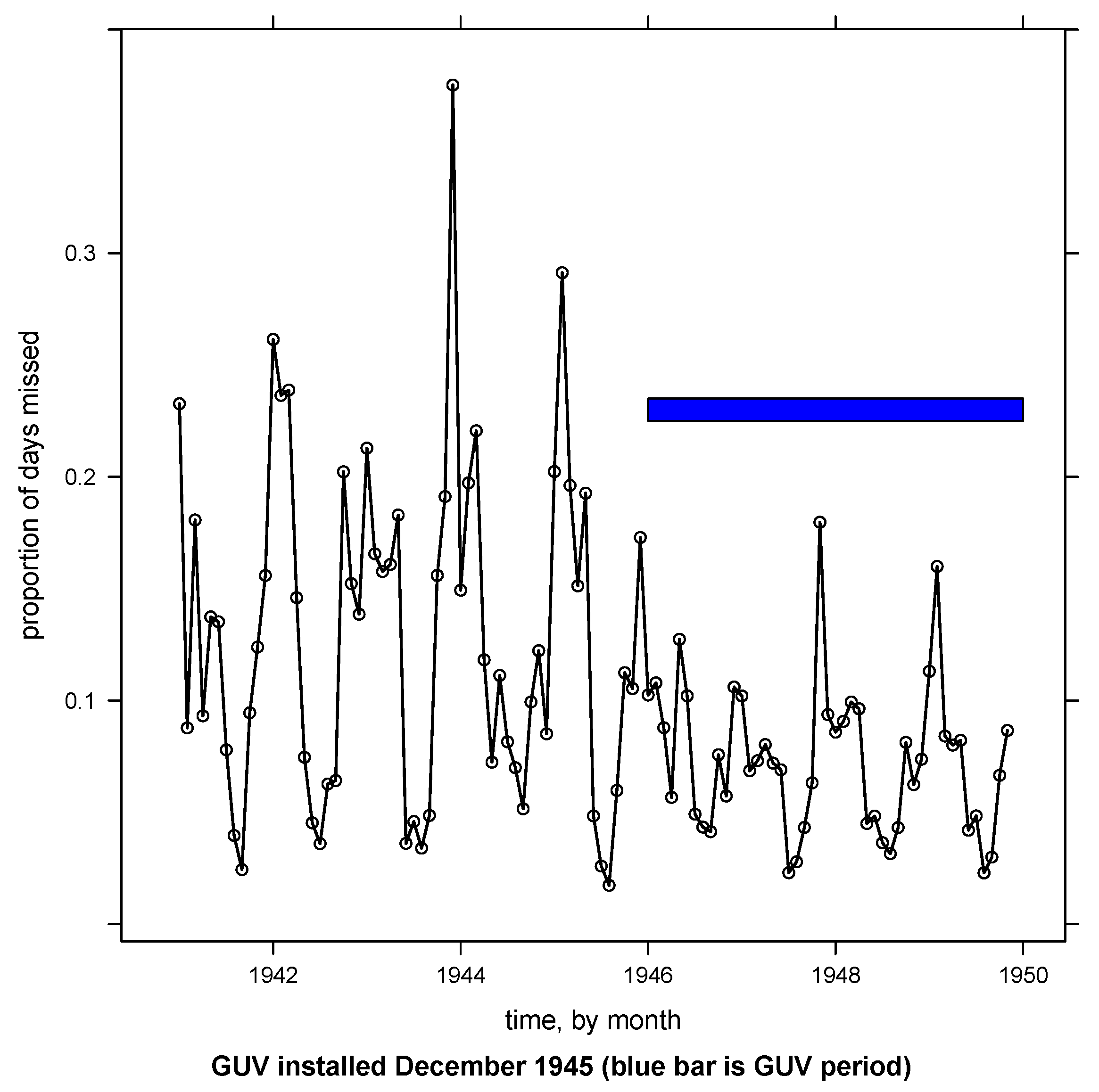
3.1. Data Exploration
3.2. Modeling
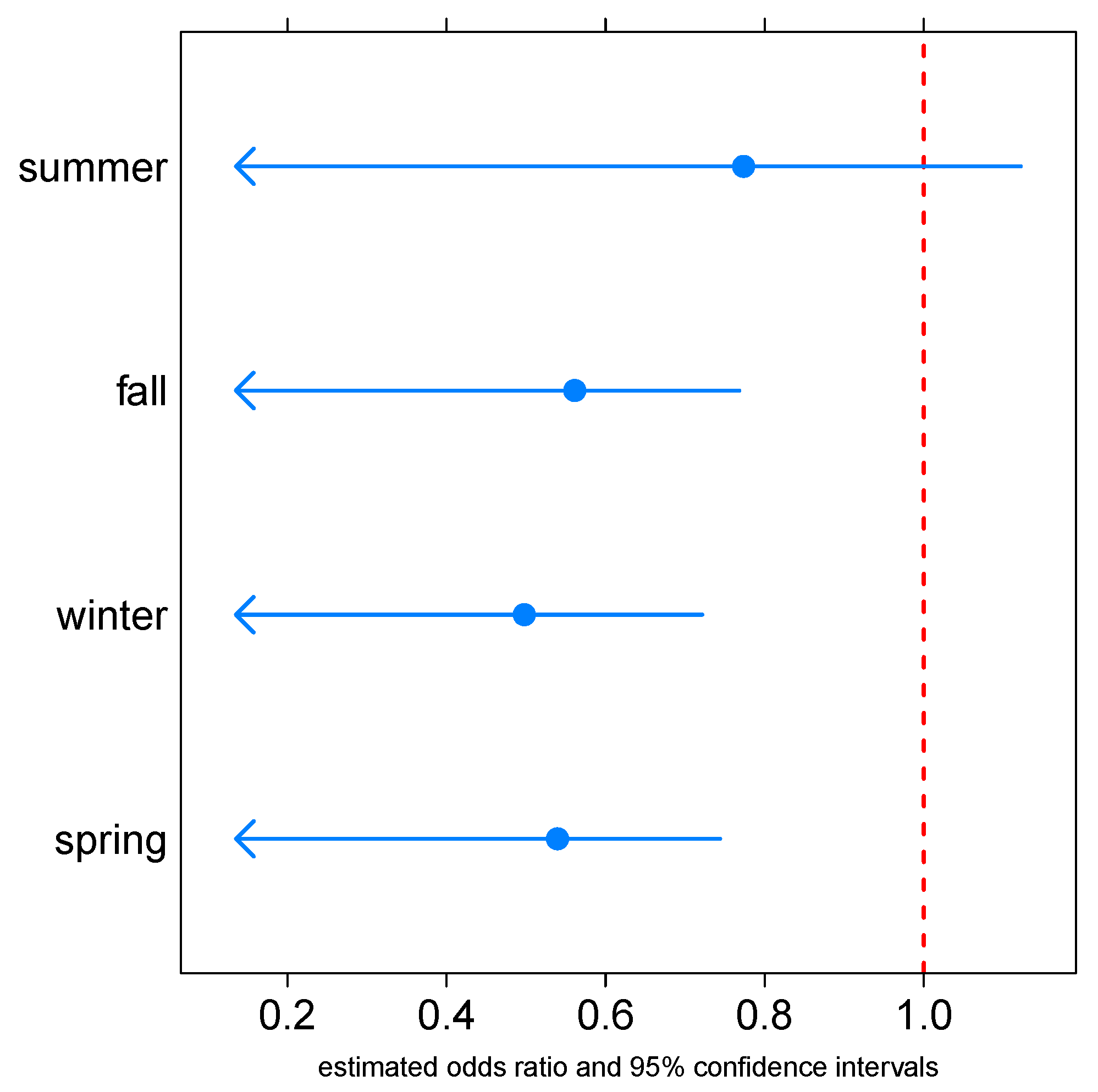
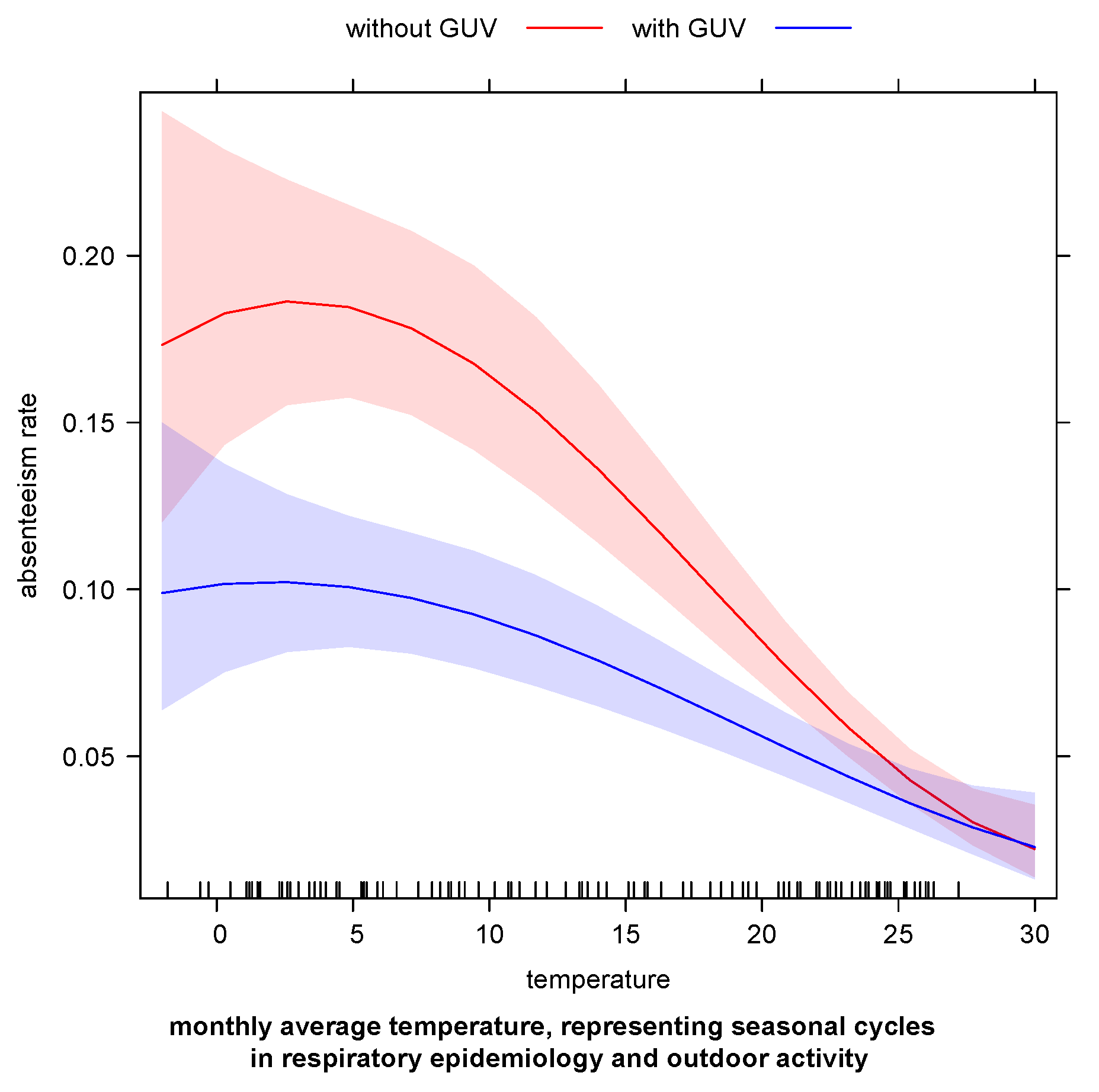
3.3. Interpretation of the Working Model
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| GUV | upper room germicidal ultraviolet light |
References
- Walker, C.M.; Ko, G. Effect of ultraviolet germicidal irradiation on viral aerosols. Environ. Sci. Technol. 2007, 41, 5460–5465. [Google Scholar] [CrossRef]
- Kim, D.K.; Kang, D.H. UVC LED Irradiation Effectively Inactivates Aerosolized Viruses, Bacteria, and Fungi in a Chamber-Type Air Disinfection System. Appl. Environ. Microbiol. 2018, 84, 1–11. [Google Scholar] [CrossRef] [PubMed]
- First, M.; Rudnick, S.N.; Banahan, K.F.; Vincent, R.L.; Brickner, P.W. Fundamental factors affecting upper-room ultraviolet germicidal irradiation—Part I. Experimental. J. Occup. Environ. Hyg. 2007, 4, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Su, C.; Lau, J.; Yu, F. A Case Study of Upper-Room UVGI in Densely-Occupied Elementary Classrooms by Real-Time Fluorescent Bioaerosol Measurements. Int. J. Environ. Res. Public Health 2017, 14, 51. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.L.; Hernandez, M.; Fennelly, K.; Martyny, J.; Marcher, J. Efficacy of Ultraviolet Irradiation in Controlling the Spread of Tuberculosis; Resreport; University of Colorado Boulder: Boulder, CO, USA, 2002. [Google Scholar]
- Nardell, E.A.; Bucher, S.J.; Brickner, P.W.; Wang, C.; Vincent, R.L.; Becan-McBride, K.; James, M.A.; Michael, M.; Wright, J.D. Safety of upper-room ultraviolet germicidal air disinfection for room occupants: Results from the Tuberculosis Ultraviolet Shelter Study. Public Health Rep. 2008, 123, 52–60. [Google Scholar] [CrossRef] [PubMed]
- First, M.W.; Weker, R.A.; Yasui, S.; Nardell, E.A. Monitoring human exposures to upper-room germicidal ultraviolet irradiation. J. Occup. Environ. Hyg. 2005, 2, 285–292. [Google Scholar] [CrossRef] [PubMed]
- International Commission on Illumination. UV-C Photocarcinogenesis Risks from Germicidal Lamps; Technical Report CIE 187:2010; International Commission on Illumination: Vienna, Austria, 2010. [Google Scholar]
- UNESCO. Education: From Disruption to Recovery. Available online: https://en.unesco.org/covid19/educationresponse#schoolclosures (accessed on 8 January 2023).
- Viner, R.; Russell, S.; Saulle, R.; Croker, H.; Stansfield, C.; Packer, J.; Nicholls, D.; Goddings, A.L.; Bonell, C.; Hudson, L.; et al. School Closures during Social Lockdown and Mental Health, Health Behaviors, and Well-being Among Children and Adolescents during the First COVID-19 Wave: A Systematic Review. JAMA Pediatr. 2022, 176, 400–409. [Google Scholar] [CrossRef]
- Lordan, R.; Prior, S.; Hennessy, E.; Naik, A.; Ghosh, S.; Paschos, G.K.; Skarke, C.; Barekat, K.; Hollingsworth, T.; Juska, S.; et al. Considerations for the Safe Operation of Schools During the Coronavirus Pandemic. Front. Public Health 2021, 9, 751451. [Google Scholar] [CrossRef]
- Viner, R.M.; Russell, S.J.; Croker, H.; Packer, J.; Ward, J.; Stansfield, C.; Mytton, O.; Bonell, C.; Booy, R. School closure and management practices during coronavirus outbreaks including COVID-19: A rapid systematic review. Lancet. Child Adolesc. Health 2020, 4, 397–404. [Google Scholar] [CrossRef]
- Keogh-Brown, M.R.; Smith, R.D.; Edmunds, J.W.; Beutels, P. The macroeconomic impact of pandemic influenza: Estimates from models of the United Kingdom, France, Belgium and The Netherlands. Eur. J. Health Econ. 2010, 11, 543–554. [Google Scholar] [CrossRef]
- Bayham, J.; Fenichel, E.P. Impact of school closures for COVID-19 on the US health-care workforce and net mortality: A modelling study. Lancet Public Health 2020, 5, e271–e278. [Google Scholar] [CrossRef] [PubMed]
- Frieden, T.R. A framework for public health action: The health impact pyramid. Am. J. Public Health 2010, 100, 590–595. [Google Scholar] [CrossRef]
- Wells, W.F.; Wells, M.W.; Wilder, T.S. The Environmental Control of Epidemic Contagion. I. An Epidemiologic Study of Radiant Disinfection of Air in Day Schools. Am. J. Hyg. 1942, 35, 97–121. [Google Scholar]
- Perkins, J.E.; Bahlke, A.M.; Silverman, H.F. Effect of ultra-violet irradiation of classrooms on spread of measles in large rural central schools. Am. J. Public Health Nation’s Health 1947, 37, 529–537. [Google Scholar] [CrossRef]
- Bahlke, A.M.; Silverman, H.F.; Ingraham, H.S. Effect of ultra-violet irradiation of classrooms on spread of mumps and chickenpox in large rural central schools. Am. J. Public Health Nation’s Health 1949, 39, 1321–1330. [Google Scholar] [CrossRef] [PubMed]
- Gelperin, A.; Granoff, M.A.; Linde, J.I. The effect of ultraviolet light upon absenteeism from upper respiratory infections in New Haven schools. Am. J. Public Health Nation’s Health 1951, 41, 796–805. [Google Scholar] [CrossRef]
- Su, C.; Lau, J.; Gibbs, S. Student absenteeism and the comparisons of two sampling procedures for culturable bioaerosol measurement in classrooms with and without upper room ultraviolet germicidal irradiation devices. Indoor Built Environ. 2016, 25, 551–562. [Google Scholar] [CrossRef]
- Reed, N.G. The history of ultraviolet germicidal irradiation for air disinfection. Public Health Rep. 2010, 125, 15–27. [Google Scholar] [CrossRef]
- Minkin, J.L.; Kellerman, A.S. A bacteriological method of estimating effectiveness of UV germicidal lamps. Public Health Rep. 1966, 81, 875–884. [Google Scholar] [CrossRef]
- Associates, D.M.B. A Study of Design Criteria and Systems for Air Conditioning Existing V.A. Hospitals: For Research Staff, Office of Construction, Veterans Administration; U.S. Government Printing Office: Washington, DC, USA, 1971. [Google Scholar]
- Higgons, R.; Hyde, G. Effect of ultraviolet air sterilization upon incidence of respiratory infections in a children’s institution; a 6-year study. N. Y. State J. Med. 1947, 47, 707–710. [Google Scholar]
- Hommel, G. A stagewise rejective multiple test procedure based on a modified Bonferroni test. Biometrika 1988, 75, 383–386. [Google Scholar] [CrossRef]
- Salk, J.; Surianao, P. Importance of antigenic composition of influenza virus vaccine in protecting against the natural disease; observations during the winter of 1947–1948. Am. J. Public Health Nation’s Health 1949, 39, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Kilbourne, E.; Loge, J. Influenza A prime: A clinical study of an epidemic caused by a new strain of virus. Ann. Intern. Med. 1950, 33, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Kilbourne, E.D.; Smith, C.; Brett, I.; Pokorny, B.A.; Johansson, B.; Cox, N. The total influenza vaccine failure of 1947 revisited: Major intrasubtypic antigenic change can explain failure of vaccine in a post-World War II epidemic. Proc. Natl. Acad. Sci. USA 2002, 99, 10748–10752. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryan, C.W. Decreased Respiratory-Related Absenteeism among Preschool Students after Installation of Upper Room Germicidal Ultraviolet Light: Analysis of Newly Discovered Historical Data. Int. J. Environ. Res. Public Health 2023, 20, 2536. https://doi.org/10.3390/ijerph20032536
Ryan CW. Decreased Respiratory-Related Absenteeism among Preschool Students after Installation of Upper Room Germicidal Ultraviolet Light: Analysis of Newly Discovered Historical Data. International Journal of Environmental Research and Public Health. 2023; 20(3):2536. https://doi.org/10.3390/ijerph20032536
Chicago/Turabian StyleRyan, Christopher W. 2023. "Decreased Respiratory-Related Absenteeism among Preschool Students after Installation of Upper Room Germicidal Ultraviolet Light: Analysis of Newly Discovered Historical Data" International Journal of Environmental Research and Public Health 20, no. 3: 2536. https://doi.org/10.3390/ijerph20032536
APA StyleRyan, C. W. (2023). Decreased Respiratory-Related Absenteeism among Preschool Students after Installation of Upper Room Germicidal Ultraviolet Light: Analysis of Newly Discovered Historical Data. International Journal of Environmental Research and Public Health, 20(3), 2536. https://doi.org/10.3390/ijerph20032536