

Effectiveness, Acceptability and Feasibility of Technology-Enabled Health Interventions for Adolescents Living with HIV in Low- and Middle-Income Countries: A Systematic Review





Abstract
1. Introduction
- What technology-enabled interventions have been implemented in LMIC to support and deliver healthcare to ALHIV (aged 10–19 years)?
- What is the effectiveness of various technology-enabled health interventions in general health and well-being and treatment outcomes of ALHIV in LMIC?
- What is the feasibility, acceptability, and fidelity of the various technology-enabled health interventions for ALHIV in LMICs?
2. Materials and Methods
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
- Types of participants: Adolescents living with HIV between the ages of 10 and 19 years as the primary study population. We considered variations in age ranges if the adolescents were the predominant focus of the intervention, as it was difficult to find disaggregated data specific to adolescents aged 10–19 years.
- Types of interventions: Studies that describe a technology-enabled intervention to deliver or support healthcare (defined as interventions that use electronic devices such as mobile phones or computers for health information communication).
- Types of studies: Quantitative (randomized controlled trials, non-randomized controlled trials, before- and after studies) and qualitative studies reporting on the feasibility and acceptability of technology-enabled interventions. Peer-reviewed studies were published in the English language, conducted in LMIC, and published between 2010 and 2022.
- Types of comparisons: Technology-enabled health intervention vs. no intervention, the standard of care, waitlist, or another intervention with no technology-enabled component. We also considered studies with no comparison.
- Types of outcomes: We considered studies reporting on any health-related individual outcomes as defined by the study authors. We report on qualitative data related to the feasibility, acceptability, and fidelity of the intervention.
- Review studies.
- Technology-enabled interventions that do not involve the adolescent directly as a recipient of the intervention, i.e., electronic health registers, monitoring and recording of service delivery.
2.3. Information and Search Strategy
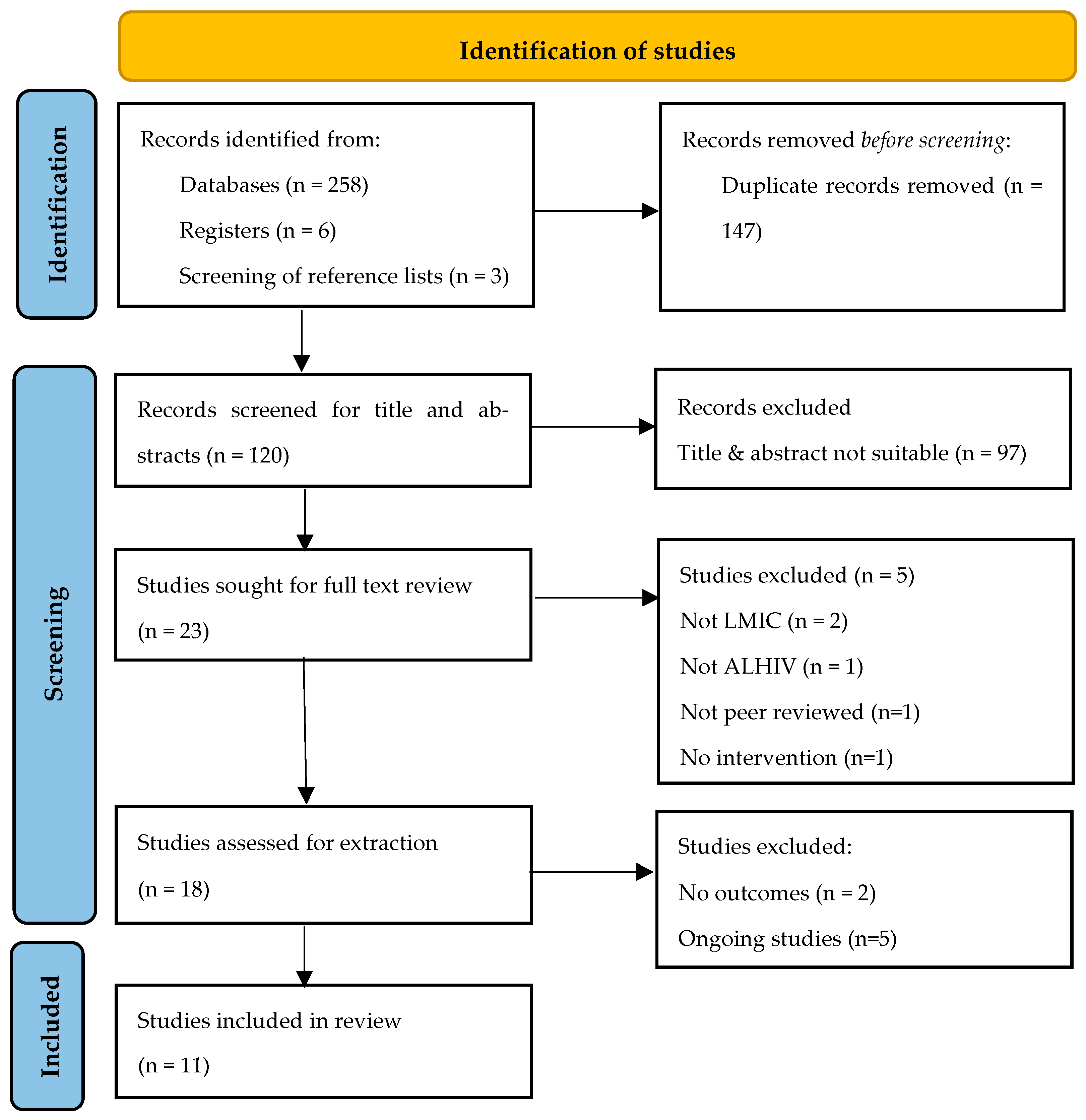
2.4. Study Selection
2.5. Data Extraction
2.6. Risk of Bias and Quality Assessment
2.7. Data Synthesis
2.8. Patient and Public Involvement
3. Results
3.1. Study Characteristics
3.2. Quality Assessment
3.3. Characteristics of Technology-Enabled Interventions
3.4. Assessment of the Effectiveness of Technology-Enabled Interventions: Primary Outcomes
3.5. Assessment of Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Authors | Country | Study Design | Title | Summary of Intervention | Trial No. |
|---|---|---|---|---|---|
| Pan African Clinical Trials Registry | |||||
| Alice Ketchaji | Cameroon | RCT | The HIV/AIDS mobile phone and home visit trial | The Short Message Service of Mobile Phones can be used as a reminder to improve adherence to ART. SMS messages sent to ALHIV on ART. Primary outcomes are adherence and retention rates. | PACTR201904582515723 |
| Joseph Ouko | Kenya | RCT | Assessing the effectiveness of a mobile phone short messaging to enhance youth peer navigation system (M-Care) for ART adherence and retention promotion among adolescents in Kenya. | To assess the feasibility and acceptability of implementing a peer-navigated mobile-based SMS tailored care platform (M-Care) into the rural healthcare system to promote ART adherence and retention among adolescents and young adults for a 9-month pilot period. To evaluate the feasibility and acceptability of implementing a peer-navigated mobile-based short messaging to promote adherence and retention among adolescents and young adults. To evaluate the effectiveness of the peer-navigated mobile-based short messaging intervention for adolescents and young adults’ ART adherence and retention. To collect information on intervention delivery approaches to inform future scale-up. | PACTR202209900806595 |
| Clinical Trials Registry | |||||
| Zanoni, B | South Africa | Pilot RCT | InTSHA: Interactive Transition Support for HIV-infected Adolescents Using Social Media (InTSHA) | The goal of this study is to develop and evaluate a social media behavioural intervention based on the Social-ecological Model of Adolescent and Young Adult Readiness to Transition (SMART) to improve transition care for adolescents living with HIV in South Africa. Primary outcomes are the acceptability and feasibility of the intervention. The secondary outcomes are peer support, connection to clinical staff, retention in care, and viral suppression. | NCT03624413 |
| Mulawa, M | South Africa | Pilot RCT | Piloting a Smartphone App (MASI) to Improve Treatment Adherence Among South African Adolescents Living With HIV | The overall goal of this pilot randomized-controlled trial (RCT) is to pilot an ART adherence-supporting smartphone app with 50 adolescents living with HIV to assess its feasibility and acceptability and to explore preliminary effects on ART adherence and social support. MASI is an adapted version of HealthMpowerment, a theory-based smartphone app. | NCT04661878 |
| Naggirinya A. B., Parkes-Ratanshi R. M., Meya D. B., Waiswa P., Rujumba J. | Uganda | RCT | Call for Life Youth ART Adherence Study (C4L-Youth) | To assess the effect of mHealth Call for life Uganda tool (CFLU) on ART adherence among youth measured by interactive voice response to daily adherence calls mapped in the database and proportion with viral suppression of copies below 1000 copies/mL. The intervention ‘Call for life Uganda’ (CFLU) uses interactive voice response (IVR) calls or text messages delivered via MOTECH™ based Connect for Life technology™. Primary outcomes are viral load, retention in care, and adherence. | NCT04718974 |
| Category of Study Designs | Methodological Quality Criteria | Studies | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chory et al., 2022 [41,42] | Dulli et al., 2018 [43] | Linnemayr et al. (2020) [48] | Henwood et al. (2016) [46] | Sanchez et al. (2021) [50] | McCarthy et al. (2020) [49] | Ivanova et al. (2019) [47] | Hacking et al. (2019) [45] | Dulli et al. (2020) [44] | Abiodun et al. (2020) [40] | Stankievich et al. (2018) [51] | ||
| Screening questions (for all types) | S1. Are there clear research questions? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| S2. Do the collected data allow to address the research questions? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | |
| 1. Qualitative | 1.1. Is the qualitative approach appropriate to answer the research question? | N/A | N/A | N/A | Y | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| 1.2. Are the qualitative data collection methods adequate to address the research question? | N/A | N/A | N/A | Y | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| 1.3. Are the findings adequately derived from the data? | N/A | N/A | N/A | Y | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| 1.4. Is the interpretation of results sufficiently substantiated by data? | N/A | N/A | N/A | Y | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| 1.5. Is there coherence between qualitative data sources, collection, analysis and interpretation? | N/A | N/A | N/A | Y | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| 2. Quantitative randomized controlled trials | 2.1. Is randomization appropriately performed? | N/A | N/A | Y | N/A | Y | Y | N/A | N/A | Y | Y | N/A |
| 2.2. Are the groups comparable at baseline? | N/A | N/A | N | N/A | N | N | N/A | N/A | N | Y | N/A | |
| 2.3. Are there complete outcome data? | N/A | N/A | Y | N/A | Y | Y | N/A | N/A | Y | Y | N/A | |
| 2.4. Are outcome assessors blinded to the intervention provided? | N/A | N/A | N | N/A | N | Y | N/A | N/A | N | Y | N/A | |
| 2.5 Did the participants adhere to the assigned intervention? | N/A | N/A | Y | N/A | Y | Y | N/A | N/A | Y | Y | N/A | |
| 3. Quantitative non- randomized | 3.1. Are the participants representative of the target population? | N/A | N | N/A | N/A | N/A | N/A | N | N/A | N/A | N/A | N |
| 3.2. Are measurements appropriate regarding both the outcome and intervention (or exposure)? | N/A | Y | N/A | N/A | N/A | N/A | Y | N/A | N/A | N/A | Y | |
| 3.3. Are there complete outcome data? | N/A | Y | N/A | N/A | N/A | N/A | Y | N/A | N/A | N/A | Y | |
| 3.4. Are the confounders accounted for in the design and analysis? | N/A | CT | N/A | N/A | N/A | N/A | CT | N/A | N/A | N/A | CT | |
| 3.5. During the study period, is the intervention administered (or exposure occurred) as intended? | N/A | Y | N/A | N/A | N/A | N/A | Y | N/A | N/A | N/A | Y | |
| 4. Quantitative descriptive | 4.1. Is the sampling strategy relevant to address the research question? | CT | N/A | N/A | N/A | N/A | N/A | N/A | Y | N/A | N/A | N/A |
| 4.2. Is the sample representative of the target population? | CT | N/A | N/A | N/A | N/A | N/A | N/A | Y | N/A | N/A | N/A | |
| 4.3. Are the measurements appropriate? | Y | N/A | N/A | N/A | N/A | N/A | N/A | Y | N/A | N/A | N/A | |
| 4.4. Is the risk of nonresponse bias low? | Y | N/A | N/A | N/A | N/A | N/A | N/A | CT | N/A | N/A | N/A | |
| 4.5. Is the statistical analysis appropriate to answer the research question? | Y | N/A | N/A | N/A | N/A | N/A | N/A | Y | N/A | N/A | N/A | |
| 5. Mixed methods | 5.1. Is there an adequate rationale for using a mixed methods design to address the research question? | N | N | N/A | N/A | N/A | N/A | N/A | Y | N | N/A | N/A |
| 5.2. Are the different components of the study effectively integrated to answer the research question? | Y | CT | N/A | N/A | N/A | N/A | N/A | Y | Y | N/A | N/A | |
| 5.3. Are the outputs of the integration of qualitative and quantitative components adequately interpreted? | Y | CT | N/A | N/A | N/A | N/A | N/A | Y | Y | N/A | N/A | |
| 5.4. Are divergences and inconsistencies between quantitative and qualitative results adequately addressed? | CT | CT | N/A | N/A | N/A | N/A | N/A | N | N | N/A | N/A | |
| 5.5. Do the different components of the study adhere to the quality criteria of each tradition of the methods involved? | Y | Y | N/A | N/A | N/A | N/A | N/A | Y | Y | N/A | N/A | |
| Score | 8/12 (0.66) | 6/12 (0.5) | 5/7 (0.71) | 7/7 (100) | 5/7 (0.71) | 6/7 (0.85) | 5/7 (0.71) | 10/12 (0.83) | 9/12 (0.75) | 12/12 (1) | 5/7 (0.71) | |
| Grade | Moderately strong | Weak | Moderately strong | Strong | Moderately strong | Strong | Moderately strong | Strong | Moderately strong | Strong | Moderately strong | |
References
- Laurenzi, C.A.; Skeen, S.; Gordon, S.; Akin-Olugbade, O.; Abrahams, N.; Bradshaw, M.; Brand, A.; Du Toit, S.; Melendez-Torres, G.J.; Tomlinson, M.; et al. Preventing mental health conditions in adolescents living with HIV: An urgent need for evidence. J. Int. AIDS Soc. 2020, 23, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Okumu, M.; Nyoni, T.; Byansi, W. Alleviating psychological distress and promoting mental wellbeing among adolescents living with HIV in sub-Saharan Africa, during and after COVID-19. Glob. Public Health 2021, 16, 964–973. [Google Scholar] [CrossRef] [PubMed]
- Mutumba, M.; Mugerwa, H.; Musiime, V.; Gautam, A.; Nakyambadde, H.; Matama, C.; Stephenson, R. Perceptions of Strategies and Intervention Approaches for HIV Self-Management among Ugandan Adolescents: A Qualitative Study. J. Int. Assoc. Provid. AIDS Care (JIAPAC) 2019, 18, 2325958218823246. [Google Scholar] [CrossRef] [PubMed]
- Enane, L.A.; Apondi, E.; Omollo, M.; Toromo, J.J.; Bakari, S.; Aluoch, J.; Morris, C.; Kantor, R.; Braitstein, P.; Fortenberry, J.D.; et al. “I just keep quiet about it and act as if everything is alright”—The cascade from trauma to disengagement among adolescents living with HIV in western Kenya. J. Int. AIDS Soc. 2021, 24, e25695. [Google Scholar] [CrossRef]
- Areri, H.A.; Marshall, A.; Harvey, G. Interventions to improve self-management of adults living with HIV on Antiretroviral Therapy: A systematic review. PLoS ONE 2020, 15, e0232709. [Google Scholar] [CrossRef]
- Modi, A.C.; Pai, A.L.; Hommel, K.A.; Hood, K.K.; Cortina, S.; Hilliard, M.E.; Guilfoyle, S.M.; Gray, W.N.; Drotar, D. Pediatric Self-management: A Framework for Research, Practice, and Policy. Pediatrics 2012, 129, e473–e485. [Google Scholar] [CrossRef]
- UNICEF. UNAIDS 2021 estimates [Internet]. 2021. Available online: https://data.unicef.org/topic/hiv-aids/ (accessed on 29 May 2022).
- Zanoni, B.C.; Sibaya, T.; Cairns, C.; Haberer, J.E. Barriers to Retention in Care are Overcome by Adolescent-Friendly Services for Adolescents Living with HIV in South Africa: A Qualitative Analysis. AIDS Behav. 2019, 23, 957–965. [Google Scholar] [CrossRef]
- Crowley, T.; Van der Merwe, A.; Kidd, M.; Skinner, D. Adolescent human immunodeficiency virus self-management: Associations with treatment adherence, viral suppression, sexual risk behaviours and health-related quality of life. S. Afr. J. HIV Med. 2020, 21, 592–606. [Google Scholar] [CrossRef]
- Navarra, A.-M.D.; Gwadz, M.V.; Whittemore, R.; Bakken, S.R.; Cleland, C.M.; Burleson, W.; Jacobs, S.K.; Melkus, G.D. Health Technology-Enabled Interventions for Adherence Support and Retention in Care Among US HIV-Infected Adolescents and Young Adults: An Integrative Review. AIDS Behav. 2017, 21, 3154–3171. [Google Scholar] [CrossRef]
- Park, E.; Kwon, M. Health-Related Internet Use by Children and Adolescents: Systematic Review. J. Med. Internet Res. 2018, 20, e120. [Google Scholar] [CrossRef]
- Hightow-Weidman, L.B.; Muessig, K.E.; Bauermeister, J.; Zhang, C.; LeGrand, S. Youth, Technology, and HIV: Recent Advances and Future Directions. Curr. HIV/AIDS Rep. 2015, 12, 500–515. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.; Powell, D.; Pichon, A.; Thai, J.; Bruce, J.; Kuhns, L.M.; Garofalo, R.; Schnall, R. A Mobile Health Intervention for HIV Prevention Among Racially and Ethnically Diverse Young Men: Usability Evaluation. JMIR mHealth uHealth 2018, 6, e11450. [Google Scholar] [CrossRef] [PubMed]
- Low, J.K.; Manias, E. Use of Technology-Based Tools to Support Adolescents and Young Adults with Chronic Disease: Systematic Review and Meta-Analysis. JMIR mHealth uHealth 2019, 7, e12042. [Google Scholar] [CrossRef]
- Celik, R.; Toruner, E.K. The Effect of Technology-Based Programmes on Changing Health Behaviours of Adolescents: Systematic Review. Compr. Child Adolesc. Nurs. 2020, 43, 92–110. [Google Scholar] [CrossRef] [PubMed]
- Radovic, A.; McCarty, C.A.; Katzman, K.; Richardson, L.P. Adolescents’ Perspectives on Using Technology for Health: Qualitative Study. JMIR Pediatr. Parent. 2018, 1, e2. [Google Scholar] [CrossRef]
- Kouvari, M.; Karipidou, M.; Tsiampalis, T.; Mamalaki, E.; Poulimeneas, D.; Bathrellou, E.; Panagiotakos, D.; Yannakoulia, M. Digital Health Interventions for Weight Management in Children and Adolescents: Systematic Review and Meta-analysis. J. Med. Internet Res. 2022, 24, e30675. [Google Scholar] [CrossRef]
- He, Z.; Wu, H.; Yu, F.; Fu, J.; Sun, S.; Huang, T.; Wang, R.; Chen, D.; Zhao, G.; Quan, M. Effects of Smartphone-Based Interventions on Physical Activity in Children and Adolescents: Systematic Review and Meta-analysis. JMIR mHealth uHealth 2021, 9, e22601. [Google Scholar] [CrossRef]
- Park, J.; Park, M.-J.; Seo, Y.-G. Effectiveness of Information and Communication Technology on Obesity in Childhood and Adolescence: Systematic Review and Meta-analysis. J. Med. Internet Res. 2021, 23, e29003. [Google Scholar] [CrossRef]
- do Amaral, E.; Melo, G.R.; de Carvalho Silva Vargas, F.; Dos Santos Chagas, C.M.; Toral, N. Nutritional interventions for adolescents using information and communication technologies (ICTs): A systematic review. PLoS ONE 2017, 12, e0184509. [Google Scholar] [CrossRef]
- Widman, L.; Nesi, J.; Kamke, K.; Choukas-Bradley, S.; Stewart, J. Technology-Based Interventions to Reduce Sexually Transmitted Infections and Unintended Pregnancy Among Youth. J. Adolesc. Health 2018, 62, 651–660. [Google Scholar] [CrossRef]
- Melia, R.; Francis, K.; Duggan, J.; Bogue, J.; O’Sullivan, M.; Chambers, D.; Young, K. Mobile Health Technology Interventions for Suicide Prevention: Protocol for a Systematic Review and Meta-Analysis. JMIR Res. Protoc. 2018, 7, e28. [Google Scholar] [CrossRef] [PubMed]
- Grist, R.; Croker, A.; Denne, M.; Stallard, P. Technology Delivered Interventions for Depression and Anxiety in Children and Adolescents: A Systematic Review and Meta-analysis. Clin. Child Fam. Psychol. Rev. 2018, 22, 147–171. [Google Scholar] [CrossRef] [PubMed]
- Lehtimaki, S.; Martic, J.; Wahl, B.; Foster, K.T.; Schwalbe, N. Evidence on Digital Mental Health Interventions for Adolescents and Young People: Systematic Overview. JMIR Ment. Health 2021, 8, e25847. [Google Scholar] [CrossRef] [PubMed]
- Bernardin, K.N.; Toews, D.N.; Restall, G.J.; Vuongphan, L. Self-management interventions for people living with human immunodeficiency virus: A scoping review. Can. J. Occup. Ther. 2013, 80, 314–327. [Google Scholar] [CrossRef] [PubMed]
- de Lima, I.C.V.; Galvão, M.T.G.; Alexandre, H.D.O.; Lima, F.E.T.; de Araújo, T.L. Information and communication technologies for adherence to antiretroviral treatment in adults with HIV/AIDS. Int. J. Med. Inform. 2016, 92, 54–61. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, X. Uses of information and communication technologies in HIV self-management: A systematic review of global literature. Int. J. Inf. Manag. 2017, 37, 75–83. [Google Scholar] [CrossRef]
- Daher, J.; Vijh, R.; Linthwaite, B.; Dave, S.; Kim, J.; Dheda, K.; Peter, T.; Pai, N.P. Do digital innovations for HIV and sexually transmitted infections work? Results from a systematic review (1996–2017). BMJ Open 2017, 7, e017604. [Google Scholar] [CrossRef]
- Manby, L.; Aicken, C.; Delgrange, M.; Bailey, J.V. Effectiveness of eHealth Interventions for HIV Prevention and Management in Sub-Saharan Africa: Systematic Review and Meta-analyses. AIDS Behav. 2022, 26, 457–469. [Google Scholar] [CrossRef]
- Casale, M.; Carlqvist, A.; Cluver, L. Recent Interventions to Improve Retention in HIV Care and Adherence to Antiretroviral Treatment Among Adolescents and Youth: A Systematic Review. AIDS Patient Care STDs 2019, 33, 237–252. [Google Scholar] [CrossRef]
- Crowley, T.; Rohwer, A. Self-management interventions for adolescents living with HIV: A systematic review. BMC Infect. Dis. 2021, 21, 1–29. [Google Scholar] [CrossRef]
- Goldstein, M.; Archary, M.; Adong, J.; Haberer, J.E.; Kuhns, L.M.; Kurth, A.; Ronen, K.; Lightfoot, M.; Inwani, I.; John-Stewart, G.; et al. Systematic Review of mHealth Interventions for Adolescent and Young Adult HIV Prevention and the Adolescent HIV Continuum of Care in Low to Middle Income Countries. AIDS Behav. 2022, 1–22, Advance online publication. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Altman, D. Systematic Reviews in Health Care: Meta-Analysis in Context; BMJ Books: Oxford, UK, 2001. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Covidence Systematic Review Software; Veritas Health Innovation: Melbourne, Australia; Available online: www.covidence.org (accessed on 6 June 2022).
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed]
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; et al. Improving the content validity of the mixed methods appraisal tool: A modified e-Delphi study. J. Clin. Epidemiol. 2019, 111, 49–59.e1. [Google Scholar] [CrossRef]
- Pluye, P.; Gagnon, M.-P.; Griffiths, F.; Johnson-Lafleur, J. A scoring system for appraising mixed methods research, and concomitantly appraising qualitative, quantitative and mixed methods primary studies in Mixed Studies Reviews. Int. J. Nurs. Stud. 2009, 46, 529–546. [Google Scholar] [CrossRef]
- Li, H.; Qian, D.; Griffiths, S.; Chung, R.Y.-N.; Wei, X. What are the similarities and differences in structure and function among the three main models of community health centers in China: A systematic review. BMC Health Serv. Res. 2015, 15, 504. [Google Scholar] [CrossRef]
- Abiodun, O.; Ladi-Akinyemi, B.; Olu-Abiodun, O.; Sotunsa, J.; Bamidele, F.; Adepoju, A.; David, N.; Adekunle, M.; Ogunnubi, A.; Imhonopi, G.; et al. A Single-Blind, Parallel Design RCT to Assess the Effectiveness of SMS Reminders in Improving ART Adherence Among Adolescents Living with HIV (STARTA Trial). J. Adolesc. Health 2021, 68, 728–738. [Google Scholar] [CrossRef]
- Chory, A.; Nyandiko, W.; Martin, R.; Aluoch, J.; Scanlon, M.; Ashimosi, C.; Njoroge, T.; McAteer, C.; Apondi, E.; Vreeman, R. HIV-Related Knowledge, Attitudes, Behaviors and Experiences of Kenyan Adolescents Living with HIV Revealed in WhatsApp Group Chats. J. Int. Assoc. Provid. AIDS Care 2021, 20, 2325958221999579. [Google Scholar] [CrossRef]
- Chory, A.; Callen, G.; Nyandiko, W.; Njoroge, T.; Ashimosi, C.; Aluoch, J.; Scanlon, M.; McAteer, C.; Apondi, E.; Vreeman, R. A Pilot Study of a Mobile Intervention to Support Mental Health and Adherence Among Adolescents Living with HIV in Western Kenya. AIDS Behav. 2022, 26, 232–242. [Google Scholar] [CrossRef]
- Dulli, L.; Ridgeway, K.; Packer, C.; Plourde, K.F.; Mumuni, T.; Idaboh, T.; Olumide, A.; Ojengbede, O.; McCarraher, D.R. An Online Support Group Intervention for Adolescents Living with HIV in Nigeria: A Pre-Post Test Study. JMIR Public Health Surveill. 2018, 4, e12397. [Google Scholar] [CrossRef]
- Dulli, L.; Ridgeway, K.; Packer, C.; Murray, K.R.; Mumuni, T.; Plourde, K.F.; Chen, M.; Olumide, A.; Ojengbede, O.; McCarraher, D.R. A Social Media–Based Support Group for Youth Living with HIV in Nigeria (SMART Connections): Randomized Controlled Trial. J. Med. Internet Res. 2020, 22, e18343. [Google Scholar] [CrossRef] [PubMed]
- Hacking, D.; Mgengwana-Mbakaza, Z.; Cassidy, T.; Runeyi, P.; Duran, L.T.; Mathys, R.H.; Boulle, A. Peer Mentorship via Mobile Phones for Newly Diagnosed HIV-Positive Youths in Clinic Care in Khayelitsha, South Africa: Mixed Methods Study. J. Med. Internet Res. 2019, 21, e14012. [Google Scholar] [CrossRef] [PubMed]
- Henwood, R.; Patten, G.; Barnett, W.; Hwang, B.; Metcalf, C.; Hacking, D.; Wilkinson, L. Acceptability and use of a virtual support group for HIV-positive youth in Khayelitsha, Cape Town using the MXit social networking platform. AIDS Care 2016, 28, 898–903. [Google Scholar] [CrossRef] [PubMed]
- Ivanova, O.; Wambua, S.; Mwaisaka, J.; Bossier, T.; Thiongo, M.; Michielsen, K.; Gichangi, P. Evaluation of the ELIMIKA Pilot Project: Improving ART Adherence among HIV Positive Youth Using an eHealth Intervention in Mombasa, Kenya. Afr. J. Reprod. Health 2019, 23, 100–110. [Google Scholar] [PubMed]
- Linnemayr, S.; Huang, H.; Luoto, J.; Kambugu, A.; Thirumurthy, H.; Haberer, J.E.; Wagner, G.; Mukasa, B. Text Messaging for Improving Antiretroviral Therapy Adherence: No Effects After 1 Year in a Randomized Controlled Trial Among Adolescents and Young Adults. Am. J. Public Health 2017, 107, 1944–1950. [Google Scholar] [CrossRef]
- MacCarthy, S.; Wagner, Z.; Mendoza-Graf, A.; Gutierrez, C.I.; Samba, C.; Birungi, J.; Okoboi, S.; Linnemayr, S. A randomized controlled trial study of the acceptability, feasibility, and preliminary impact of SITA (SMS as an Incentive to Adhere): A mobile technology-based intervention informed by behavioral economics to improve ART adherence among youth in Uganda. BMC Infect. Dis. 2020, 20, 173. [Google Scholar] [CrossRef]
- Sánchez, S.A.; Ramay, B.M.; Zook, J.; de Leon, O.; Peralta, R.; Juarez, J.; Cocohoba, J. Toward improved adherence: A text message intervention in an human immunodeficiency virus pediatric clinic in Guatemala City. Medicine 2021, 100, e24867. [Google Scholar] [CrossRef]
- Stankievich, E.; Malanca, A.; Foradori, I.; Ivalo, S.; Losso, M. Utility of Mobile Communication Devices as a Tool to Improve Adherence to Antiretroviral Treatment in HIV-infected Children and Young Adults in Argentina. Pediatr. Infect. Dis. J. 2018, 37, 345–348. [Google Scholar] [CrossRef]
- World Health Organisation. Youth-Centred Digital Health Interventions: A Framework for Planning, Developing and Implementing Solutions with and for Young People. World Health Organization: Geneva, Switzerland Licence: CC BY-NC-SA 3.0 IGO. Available online: https://www.who.int/publications/i/item/9789240011717 (accessed on 22 November 2022).
- Ahonkhai, A.A.; Pierce, L.J.; Mbugua, S.; Wasula, B.; Owino, S.; Nmoh, A.; Idigbe, I.; Ezechi, O.; Amaral, S.; David, A.; et al. PEERNaija: A Gamified mHealth Behavioral Intervention to Improve Adherence to Antiretroviral Treatment Among Adolescents and Young Adults in Nigeria. Front. Reprod. Health 2021, 3, 656507. [Google Scholar] [CrossRef]
- Tarantino, N.; Lartey, M.; Arnold, T.; Brown, L.; Kwara, A.; Guthrie, K. Preferences for a Game-Based SMS Adherence Intervention Among Young People Living with HIV in Ghana: A Qualitative Study. AIDS Behav. 2022, 26, 2169–2181. [Google Scholar] [CrossRef]
- Mulawa, M. Piloting a Smartphone App to Improve Treatment Adherence Among South African Adolescents Living With HIV. Clinical Trials Registry. Available online: https://clinicaltrials.gov/ct2/show/NCT04661878?term=Adolescents&cond=HIV&intr=%22Mhealth%22+OR+%22technology%22&draw=2&rank=38 (accessed on 15 November 2022).

| Component | Criteria |
|---|---|
| Patient/Population | Adolescents Living with HIV Aged 10–19 Years. |
| Intervention | Technology-enabled health interventions aimed at delivering or supporting health care directly to ALHIV |
| Comparisons | With or without comparison |
| Outcomes | Primary outcomes: health-related individual outcomes as specified by each study e.g., health/risk behaviours, self-management behaviours, self-efficacy, adherence, retention in care, viral suppression, quality of life, mental health or well-being. Secondary outcomes: process outcomes e.g., acceptability, feasibility, fidelity |
| Time | 2010–2022 |
| Other considerations | English language Low- and middle-income countries |
| Authors, Year | Country | Study Design | Type of Data | Study Population | Total Number of Participants |
|---|---|---|---|---|---|
| Abiodun et al., 2021 [40] | Nigeria | RCT | Quantitative | ALHIV aged 15–19 years. The mean age was 16.61 (+/− 1.38) years. The study had 101 (48.33%) female and 108 (51.67%) male participants. | N = 209 (intervention group = 105; control group = 104) |
| Chory et al., 2022 [41,42] | Kenya | Non-RCT pre-post | Quantitative & qualitative | ALHIV aged 10–19 years. The mean age was 15.4 years, and the majority (56.7%) were female. | N = 30 (each group had 15 study participants at baseline; one group was 9–14-year-olds and the other 15–19-year-olds) |
| Dulli et al., 2018 [43] | Nigeria | Non-RCT pre-post | Quantitative & qualitative | ALHIV aged between 15–19 years old, 22 females, 19 males, and a mean age of 17 years. | N = 41 (5 support groups of 8–10 individuals) |
| Dulli et al., 2020 [44] | Nigeria | RCT | Qualitative & qualitative | Most participants were female 87.7% (306/349) and the mean age was 21 years (SD 2.3). | N = 349 (intervention group = 177 (50.6%); control group = 172 (49.1%) |
| Hacking et al., 2019 [45] | South Africa | Non-RCT matched controls | Quantitative & qualitative | HIV-positive youths, 95% female virtual mentees with a median age of 20 years 5 months; 91% female matched controls cohort with a median age of 22 years 7 months. | Virtual mentees cohort (N = 40) Matched controls cohort (N = 70) |
| Henwood et al., 2016 [46] | South Africa | Qualitative | Qualitative | HIV-positive youths between the ages 14–28 (59% between 23 and 25 years, 63% female). | 60 club members completed the questionnaire, and 12 participated in the focus groups. |
| Ivanova et al., 2019 [47] | Kenya | Non-RCT pre-post | Quantitative | HIV-positive youths aged 15–24 years (36 were male and 45 were female). Mean age 18.4 years (SD = 2.8); range 15 to 25 years. | N = 90 |
| Linnemayr et al., 2017 [48] | Uganda | RCT | Quantitative | HIV-positive adolescents and young adults aged 15 to 22 years. The mean was age 18 years; 61% were female. | N = 110 (message-only group), N = 110 (message and response group) N = 112 (control group) |
| McCarthy et al., 2020 [49] | Uganda | RCT | Quantitative & qualitative | HIV-positive youths 15–24 years. | N = 40 (treatment 1) N = 56 (treatment 2) N = 59 (control) |
| Sanchez et al., 2021 [50] | Guatemala | RCT | Quantitative | Age range of 6 to 12 years old (49.1%), and 13 to 24 years old (50.9%). | N = 72 (intervention group) N = 71 (control group) |
| Stankievich et al., 2018 [51] | Argentina | Non-RCT sequential design (pre-post) | Quantitative | Children and young people living with HIV; mean age 7.2± 6.1 years (range: 6–25); 11(50%) < 18 years; 15 (68%) females. | N = 25 |
| Authors, Year | Study Design | Quality Assessment Score | Grading |
|---|---|---|---|
| Abiodun et al., 2021 [40] | RCT | 12/12 (1) | Strong |
| Chory et al., 2022 [41,42] | Non-RCT pre-post | 8/12 (0.66) | Moderately strong |
| Dulli et al., 2018 [43] | Non-RCT pre-post | 6/12 (0.5) | Weak |
| Dulli et al., 2020 [44] | RCT | 9/12 (0.75) | Moderately strong |
| Hacking et al., 2019 [45] | Non-RCT matched controls | 10/12 (0.83) | Strong |
| Henwood et al., 2016 [46] | Qualitative | 7/7 (1.00) | Strong |
| Ivanova et al., 2019 [47] | Non-RCT pre-post | 5/7 (0.71) | Moderately strong |
| Linnemayr et al., 2017 [48] | RCT | 5/7 (0.71) | Moderately strong |
| McCarthy et al., 2020 [49] | RCT | 6/7 (0.85) | Strong |
| Sanchez et al., 2021 [50] | RCT | 5/7 (0.71) | Moderately strong |
| Stankievich et al., 2018 [51] | Non-RCT pre-post (sequential design) | 5/7 (0.71) | Moderately strong |
| Authors, Year | Country | Name of the Intervention | Technology Design | Delivery Platform | Brief Description |
|---|---|---|---|---|---|
| Abiodun et al., 2021 [40] | Nigeria | STARTA Trial | Interactive individual | SMS | Duration 12 months Participants received daily ART adherence reminder SMS and were required to reply to their daily messages as soon as possible. |
| Chory et al., 2022 [41,42] | Kenya | A Mobile Intervention to Support Mental Health and Adherence Among Adolescents Living with HIV | Interactive groups | Duration: 6 months Weekly in-person meetings to discuss topics e.g., adherence, disclosure etc. Informal WhatsApp communication is encouraged. The counsellor sends direct messages every other week. | |
| Dulli et al., 2018 [43] | Nigeria | SMART (Social Media to promote Adherence and Retention in Treatment) Connections | Interactive groups | Duration: 6 months Secret Facebook groups with safe space, trained adult facilitator, social activities (riddles, puzzles), interactive polls and facilitated discussions, word of the week, and key messages. | |
| Dulli et al., 2020 [44] | Nigeria | SMART (Social Media to promote Adherence and Retention in Treatment) Connections | Interactive groups | Duration: 22 weeks Same as for Dulli et al., 2018 | |
| Hacking et al., 2019 [45] | South Africa | The Virtual Mentors Program | Interactive individual | SMS, call, or WhatsApp | Duration: 14 months The mentors chatted with the mentees who responded to the messages concerning their families, and social activities, and invited them to the youth adherence clubs. |
| Henwood et al., 2016 [46] | South Africa | A virtual support group for HIV-positive youth | Interactive groups | Mxit | Duration: 13 months An adherence counsellor moderated the chat room for one hour on weekday afternoons and sent out a short message service to all registered chat room users to alert them when the counsellor joined the chat room. The counsellor-initiated conversations and promote interaction among users. |
| Ivanova et al., 2019 [47] | Kenya | ELIMIKA—digital peer support for improving ART adherence | Interactive groups | Web-based | Duration: 12 months Participants took part in blog post discussions with each other, project coordinators, and health care providers. |
| Linnemayr et al., 2017 [48] | Uganda | Text Messaging for Improving Antiretroviral Therapy Adherence | Interactive and non-interactive, individual (one-way vs. two-way vs. control) | SMS | Duration: 48 weeks Every Sunday at 9 AM, the program manager dispatched text messages to both intervention groups. Participants in the in the second group could respond to the messages. |
| McCarthy et al., 2020 [49] | Uganda | SITA (SMS as an Incentive To Adhere) | Non-interactive individual | SMS | Duration: 18 months Weekly messages were sent informing participants about their adherence level. |
| Sanchez et al., 2021 [50] | Guatemala | A text message intervention in an HIV paediatric clinic | Non-interactive individual | SMS | Duration: 6 months Frontline SMS was used to send SMS messages to the entire intervention group at the same time of the day. Messages were designed to improve each of the areas measured in the adherence questionnaire. |
| Stankievich et al., 2018 [51] | Argentina | Mobile Communication Devices as a Tool to Improve Adherence to Antiretroviral Treatment in HIV-Infected Children and Young Adults in Argentina | Interactive individual | Text messages sent via phone or Facebook | Duration: 32 weeks. A text message was sent through the application selected by the participant. A generic mobile message is sent twice a month. Patients agreed to answer the message to verify that the contact had been received. |
| Author, Year | Linkage to Care | Adherence | Viral Load | Retention in Care | HIV Knowledge | Social Support | Self-Efficacy for Adherence | Mental Health | Stigma | Behavioural Health |
|---|---|---|---|---|---|---|---|---|---|---|
| Abiodun et al., 2021 [40] | - | No | No | - | - | - | - | - | - | - |
| Chory et al., 2022 [41,42] | - | No | - | - | - | - | - | No | No | No |
| Dulli 2020 [44] | - | No | - | No | Yes | No | - | No | No | - |
| Hacking 2019 [45] | Yes | - | No | No | - | - | - | - | - | - |
| Ivanova et al., 2019 [47] | - | No | - | - | No | - | No | - | - | - |
| Linnemayr 2017 [48] | - | No | - | - | - | - | - | - | - | - |
| McCarthy 2020 [49] | - | No | - | - | - | - | - | - | - | - |
| Sanchez 2021 [50] | - | Yes | - | - | - | - | - | - | - | - |
| Steinkievich et al., 2018 [51] | - | Yes | Yes | - | - | - | - | - | - | - |
| Study ID | Acceptability | Feasibility | Fidelity |
|---|---|---|---|
| Abiodun et al., 2021 [40] | High | High | Not reported |
| Chory et al., 2022 [41,42] | High | High | Not reported |
| Dulli et al., 2018 [43] | High | High | High |
| Dulli et al., 2020 [44] | High | High | High |
| Hacking et al., 2019 [45] | High | High | Not reported |
| Henwood et al., 2016 [46] | High | High | Low |
| Ivanova et al., 2019 [47] | High | High | Not reported |
| McCarthy et al., 2020 [49] | High | High | High |
| Sanchez et al., 2021 [50] | High | Not reported | Not reported |
| Steinkievich et al., 2018 [51] | High | High | Not reported |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crowley, T.; Petinger, C.; Nchendia, A.I.; van Wyk, B. Effectiveness, Acceptability and Feasibility of Technology-Enabled Health Interventions for Adolescents Living with HIV in Low- and Middle-Income Countries: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 2464. https://doi.org/10.3390/ijerph20032464
Crowley T, Petinger C, Nchendia AI, van Wyk B. Effectiveness, Acceptability and Feasibility of Technology-Enabled Health Interventions for Adolescents Living with HIV in Low- and Middle-Income Countries: A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(3):2464. https://doi.org/10.3390/ijerph20032464
Chicago/Turabian StyleCrowley, Talitha, Charné Petinger, Azia Ivo Nchendia, and Brian van Wyk. 2023. "Effectiveness, Acceptability and Feasibility of Technology-Enabled Health Interventions for Adolescents Living with HIV in Low- and Middle-Income Countries: A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 3: 2464. https://doi.org/10.3390/ijerph20032464
APA StyleCrowley, T., Petinger, C., Nchendia, A. I., & van Wyk, B. (2023). Effectiveness, Acceptability and Feasibility of Technology-Enabled Health Interventions for Adolescents Living with HIV in Low- and Middle-Income Countries: A Systematic Review. International Journal of Environmental Research and Public Health, 20(3), 2464. https://doi.org/10.3390/ijerph20032464