
Occupational Burnout in Healthcare Workers, Stress and Other Symptoms of Work Overload during the COVID-19 Pandemic in Poland
 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Assessment of Burnout
2.3. Assessment of Stress
2.4. Other Variables
2.5. Statistical Analyses
3. Results
3.1. Sample Characteristics
3.2. Occupational Burnout
3.3. Determinants of Occupational Burnout
3.4. Using Professional Help (Psychological, Psychiatric and Support Group)
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khamisa, N.; Oldenburg, B.; Peltzer, K.; Ilic, D. Work related stress, burnout, job satisfaction and general health of nurses. Int. J. Environ. Res. Public Health 2015, 12, 652–666. [Google Scholar] [CrossRef] [PubMed]
- Marsollier, R.G. An analysis on burnout-engagement model in public employees. Psicogente 2018, 22, 272–289. [Google Scholar] [CrossRef]
- Tremblay, M.A.; Messervey, D. The Job Demands-Resources model: Further evidence for the buffering effect of personal resources. SAJIP 2011, 37, 10. [Google Scholar] [CrossRef]
- Freudenberger, H. Staff burnout. J. Soc. Issues 1974, 30, 159–165. [Google Scholar] [CrossRef]
- Kim, M.H.; Mazenga, A.C.; Simon, K.; Yu, X.; Ahmed, S.; Nyasulu, P.; Kazembe, P.N.; Ngoma, S.; Abrams, E.J. Burnout and self-reported suboptimal patient care amongst health care workers providing HIV care in Malawi. PLoS ONE 2018, 13, e0192983. [Google Scholar] [CrossRef]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems (ICD-11), 11th ed.; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Maslach, C.; Jackson, S. The measurement of experienced Burnout. J. Organ. Behav. 1981, 2, 99–113. [Google Scholar] [CrossRef]
- Carlotto, M.S.; Palazzo, L.O.S. Factors associated with burnout’s syndrome: An epidemiological study of teachers. Cad. Saude Publica 2006, 22, 1017–1026. [Google Scholar] [CrossRef]
- Gómez-Urquiza, J.L.; Albendín-García, L.; Velando-Soriano, A.; Ortega-Campos, E.; Ramírez-Baena, L.; Membrive-Jiménez, M.J.; Suleiman-Martos, N. Burnout in Palliative Care Nurses, Prevalence and Risk Factors: A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 7672. [Google Scholar] [CrossRef]
- Maslach, C.; Leiter, M. The Truth About Burnout: How Organizations Cause Personal Stress and What to Do About It; Jossey-Bass: San Francisco, CA, USA, 2000. [Google Scholar]
- Sęk, H. Wypalenie Zawodowe. Przyczyny i Zapobieganie (Occupational Burnout. Causes and Prevention); PWN: Warsaw, Poland, 2011; pp. 13–31. [Google Scholar]
- Łaguna, M. Satysfakcja z życia i satysfakcja z pracy a motywacja do podejmowania szkoleń: Doniesienie z badań (Satisfaction with life and job satisfaction and motivation to undertake training: Research report). Psychol. Qual. Life 2006, 11, 163–172. [Google Scholar] [CrossRef]
- Dębska, G.; Pasek, M.; Wilczek-Rużyczka, E. Obciążenia psychiczne i wypalenie zawodowe u pielęgniarek pracujących w różnych specjalnościach zawodowych (Psychological burdens and burnout in nurses working in various professional specialties). Hygeia Public Health 2014, 49, 113–119. [Google Scholar]
- Dugani, S.; Afari, H.; Hirschhorn, L.R.; Ratcliffe, H.; Veillard, J.; Martin, G.; Lagomarsino, G.; Basu, L.; Bitton, A. Prevalence and factors associated with burnout among frontline primary health care providers in low- and middle-income countries: A systematic review. Gates Open Res. 2018, 2, 4. [Google Scholar] [CrossRef] [PubMed]
- Adriaenssens, J.; De Gucht, V.; Maes, S. Determinants and prevalence of burnout in emergency nurses: A systematic review of 25 years of research. Int. J. Nurs. Stud. 2015, 52, 649–661. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.; Hall, L.H.; Berzins, K.; Baker, J.; Melling, K.; Thompson, C. Mental healthcare staff well-being and burnout: A narrative review of trends, causes, implications, and recommendations for future interventions. Int. J. Ment. Health Nurs. 2018, 27, 20–32. [Google Scholar] [CrossRef]
- Drummond, D. Physician Burnout: Its Origin, Symptoms, and Five Main Causes. Fam. Pract. Manag. 2015, 22, 42–47. [Google Scholar]
- Shanafelt, T.D.; Balch, C.M.; Bechamps, G.J.; Russell, T.; Dyrbye, L.; Satele, D.; Collicott, P.; Novotny, P.J.; Sloan, J.; Freischlag, J.A. Burnout and career satisfaction among American surgeons. Ann. Surg. 2009, 250, 463–471. [Google Scholar] [CrossRef]
- Profit, J.; Sharek, P.J.; Amspoker, A.B.; Kowalkowski, M.A.; Nisbet, C.C.; Thomas, E.J.; Chadwick, W.A.; Sexton, J.B. Burnout in the NICU setting and its relation to safety culture. BMJ Qual. Saf. 2014, 23, 806–813. [Google Scholar] [CrossRef] [PubMed]
- Lacy, B.E.; Chan, J.L. Physician Burnout: The Hidden Health Care Crisis. Clin. Gastroenterol. Hepatol. 2018, 16, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Moss, M.; Good, V.S.; Gozal, D.; Kleinpell, R.; Sessler, C.N. An Official Critical Care Societies Collaborative Statement-Burnout Syndrome in Critical Care Health-care Professionals: A Call for Action. Chest 2016, 150, 17–26. [Google Scholar] [CrossRef]
- Labrague, L.J.; McEnroe-Petitte, D.M.; Leocadio, M.C.; Van Bogaert, P.; Cummings, G.G. Stress and ways of coping among nurse managers: An integrative review. J. Clin. Nurs. 2018, 27, 1346–1359. [Google Scholar] [CrossRef]
- Morsiani, G.; Bagnasco, A.; Sasso, L. How staff nurses perceive the impact of nurse managers’ leadership style in terms of job satisfaction: A mixed method study. J. Nurs. Manag. 2017, 25, 119–128. [Google Scholar] [CrossRef]
- Rothenberger, D.A. Physician Burnout and Well-Being: A Systematic Review and Framework for Action. Dis. Colon Rectum 2017, 60, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Eyoun, K. Do mindfulness and perceived organizational support work? Fear of COVID-19 on restaurant frontline employees’ job insecurity and emotional exhaustion. Int. J. Hosp. Manag. 2021, 94, 102850. [Google Scholar] [CrossRef] [PubMed]
- Aguiar-Quintana, T.; Nguyen, T.H.H.; Araujo-Cabrera, Y.; Sanabria-Díaz, J.M. Do job insecurity, anxiety and depression caused by the COVID-19 pandemic influence hotel employees’ self-rated task performance? The moderating role of employee resilience. Int. J. Hosp. Manag. 2021, 94, 102868. [Google Scholar] [CrossRef] [PubMed]
- Białorudzki, M.; Izdebski, Z. Changes in the body mass of adult residents of rural and urban areas in the initial months of the COVID-19 pandemic vs. their mental, physical and sexual health. Ann. Agric. Environ. Med. 2021, 28, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; McManus, S.; et al. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef]
- Denning, M.; Goh, E.T.; Tan, B.; Kanneganti, A.; Almonte, M.; Scott, A.; Martin, G.; Clarke, J.; Sounderajah, V.; Markar, S.; et al. Determinants of burnout and other aspects of psychological well-being in healthcare workers during the COVID-19 pandemic: A multinational cross-sectional study. PLoS ONE 2021, 16, e0238666. [Google Scholar] [CrossRef]
- Elghazally, S.A.; Alkarn, A.F.; Elkhayat, H.; Ibrahim, A.K.; Elkhayat, M.R. Burnout Impact of COVID-19 Pandemic on Health-Care Professionals at Assiut University Hospitals. Int. J. Environ. Res. Public Health 2021, 18, 5368. [Google Scholar] [CrossRef]
- Schaufeli, W.; de Witte, H.; Desart, S. Burnout Assessment Tool 1 English Translation of the Dutch Manual Content; Burnout Assessment Tool: Leuven, Belgium, 2019; pp. 1–111. Available online: http://burnoutassessmenttool.be/wpcontent/uploads/2019/04/Handleiding-BAT-engels-versie-1.2.pdf (accessed on 2 December 2022).
- Bayes, A.; Tavella, G.; Parker, G. The biology of burnout: Causes and consequences. World J. Biol. Psychiatry 2021, 22, 686–698. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. JHSB 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Lee, E.H. Review of the psychometric evidence of the perceived stress scale. Asian Nurs. Res. (Korean Soc. Nurs. Sci.) 2012, 6, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Warttig, S.L.; Forshaw, M.J.; South, J.; White, A.K. New, normative, English-sample data for the Short Form Perceived Stress Scale (PSS-4). J. Health Psychol. 2013, 18, 1617–1628. [Google Scholar] [CrossRef] [PubMed]
- Izdebski, Z. Zdrowie i Życie Seksualne Polek i Polaków w Wieku 50–74 lat w 2017 Roku. Perspektywa Starzejącego Się Społeczeństwa; University of Warsaw Press: Warsaw, Poland, 2021. [Google Scholar] [CrossRef]
- Izdebski, Z. Zdrowie i Życie Seksualne Polek i Polaków w Wieku 18-49 lat w 2017 Roku. Studium Badawcze na tle Przemian od 1997 Roku; University of Warsaw Press: Warsaw, Poland, 2020. [Google Scholar] [CrossRef]
- Cain, M.K.; Zhang, Z.; Yuan, K.-H. Univariate and multivariate skewness and kurtosis for measuring nonnormality: Prevalence, influence and estimation. Behav. Res. Methods 2017, 49, 1716–1735. [Google Scholar] [CrossRef] [PubMed]
- Claponea, R.M.; Pop, L.M.; Iorga, M.; Iurcov, R. Symptoms of Burnout Syndrome among Physicians during the Outbreak of COVID-19 Pandemic—A Systematic Literature Review. Healthcare 2022, 10, 979. [Google Scholar] [CrossRef]
- Bhardwaj, A. COVID-19 Pandemic and Physician Burnout: Ramifications for Healthcare Workforce in the United States. J. Healthc. Leadersh. 2022, 14, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, R.; Sichuan, N.; Green, H.; Halcomb, E.J.; Middleton, R.; Alananzeh, I.; Alanzeh, I.; Trakis, S.; Moxham, L. Anxiety and depression among healthcare workers during the COVID-19 pandemic: A systematic umbrella review of the global evidence. BMJ Open 2021, 11, e054528. [Google Scholar] [CrossRef]
- Ilic, I.M.; Arandjelovic, M.Z.; Jovanovic, J.M.; Nesic, M.M. Relationships of work-related psychosocial risks, stress, individual factors and burnout—Questionnaire survey among emergency physicians and nurses. Med. Pr. 2017, 68, 167–178. [Google Scholar]
- Bridgeman, P.J.; Bridgeman, M.B.; Barone, J. Burnout syndrome among healthcare professionals. Am. J. Health-Syst. Pharm. 2018, 75, 147–152. [Google Scholar] [CrossRef]
- Friganović, A.; Selič, P.; Ilić, B.; Sedić, B. Stress and burnout syndrome and their associations with coping and job satisfaction in critical care nurses: A literature review. Psychiatr. Danub. 2019, 31, 21–31. [Google Scholar]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health careworkers exposed to coronavirus disease 2019. JAMA Network Open 2020, 3, e203976. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.Z.; Han, M.F.; Luo, T.D.; Ren, A.K.; Zhou, X.P. Mental health survey of 230 medical staff in a tertiary infectious disease hospital for COVID-19. Chin. J. Ind. Hyg. Occup. Dis. 2020, 38, E001. [Google Scholar]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Lv, Y.; Zhang, Z.; Zeng, W.; Li, J.; Wang, X.; Luo, G.Q. Anxiety and Depression Survey of Chinese Medical Staff before and during COVID-19 Defense (3/7/2020). Available online: https://ssrn.com/abstract=3551350 (accessed on 8 December 2022).
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2022, 291, 113190. [Google Scholar] [CrossRef]
- Kang, L.; Ma, S.; Chen, M.; Yang, J.; Wang, Y.; Li, R.; Yao, L.; Bai, H.; Cai, Z.; Yang, B.X.; et al. Impact on mental health and perceptions of psychological care among medical and nursing staff in Wuhan during the 2019 novel coronavirus disease outbreak: A cross-sectional study. Brain Behav. Immun. 2020, 87, 11–17. [Google Scholar] [CrossRef]
- Olaya, B.; Pérez-Moreno, M.; Bueno-Notivol, J.; Gracia-García, P.; Lasheras, I.; Santabárbara, J. Prevalence of Depression among Healthcare Workers during the COVID-19 Outbreak: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 3406. [Google Scholar] [CrossRef]
- Florin, D.; Basham, S. Evaluation of health promotion in clinical settings. In Evaluating Health Promotion. Practice and Methods; Thorogood, M., Coombes, Y., Eds.; Oxford University Press: Oxford, UK, 2000; pp. 140–150. [Google Scholar]
- Endacott, R.; Jones, C.; Bloomer, M.J.; Boulanger, C.; Ben Nun, M.; Lliopoulou, K.K. The state of critical care nursing education in Europe: An international survey. Intensive Care Med. 2015, 41, 2237–2240. [Google Scholar] [CrossRef]
- Zhang, Q.; Li, S.; Liu, J.; Chen, J. Global Trends in Nursing-Related Research on COVID-19: A Bibliometric Analysis. Front. Public Health 2022, 10, 933555. [Google Scholar] [CrossRef]
- Ching, S.M.; Ng, K.Y.; Lee, K.W.; Yee, A.; Lim, P.Y.; Ranita, H.; Devaraj, N.K.; Ooi, P.B.; Cheong, A.T. Psychological distress among healthcare providers during COVID-19 in Asia: Systematic review and meta-analysis. PLoS ONE 2021, 16, e0257983. [Google Scholar] [CrossRef]
- Garcia, C.D.L.; Abreu, L.C.D.; Ramos, J.L.S.; Castro, C.F.D.D.; Smiderle, F.R.N.; Santos, J.A.D.; Bezerra, I.M.P. Influence of Burnout on Patient Safety: Systematic Review and Meta-Analysis. Medicina 2019, 55, 553. [Google Scholar] [CrossRef]
- Rotenstein, L.S.; Torre, M.; Ramos, M.A.; Rosales, R.C.; Guille, C.; Sen, S.; Mata, D.A. Prevalence of Burnout Among Physicians: A Systematic Review. JAMA 2018, 320, 1131–1150. [Google Scholar] [CrossRef] [PubMed]
- Dyrbye, L.N.; Varkey, P.; Boone, S.L.; Satele, D.V.; Sloan, J.A.; Shanafelt, T.D. Physician satisfaction and burnout at different career stages. Mayo Clin. Proc. 2013, 88, 1358–1367. [Google Scholar] [CrossRef]
- Gómez-Urquiza, J.L.; Albendín-García, L.; Vargas-Pecino, C.; De La Fuente-Solana, E.I.; Ortega-Campos, E.M.; La Fuente, G.A.C.D. Prevalence of Burnout Syndrome in Emergency Nurses: A Meta-Analysis. Crit. Care Nurse 2017, 37, e1–e9. [Google Scholar] [CrossRef]
- Imo, U.O. Burnout and psychiatric morbidity among doctors in the UK: A systematic literature review of prevalence and associated factors. BJPsych Bull. 2017, 41, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Vijendren, A.; Yung, M.; Shiralkar, U. Are ENT surgeons in the UK at risk of stress, psychological morbidities and burnout? A national questionnaire survey. Ssurgeon 2018, 16, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Dewey, C.; Hingle, S.; Goelz, E.; Linzer, M. Supporting clinicians during the COVID-19 pandemic. Ann. Intern. Med. 2020, 2020, 752–753. [Google Scholar] [CrossRef]
- Dyrbye, L.N.; Shanafelt, T.D.; Balch, C.M.; Satele, D.; Sloan, J.; Freischlag, J. Relationship between work-home conflicts and burnout among American surgeons: A comparison by sex. Arch. Surg. 2011, 146, 211–217. [Google Scholar] [CrossRef]
- Oreskovich, M.R.; Kaups, K.L.; Balch, C.M.; Hanks, J.B.; Satele, D.; Sloan, J.; Meredith, C.; Buhl, A.; Dyrbye, L.N.; Shanafelt, T.D. Prevalence of alcohol use disorders among American surgeons. Arch. Surg. 2012, 147, 168–174. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Balch, C.M.; Bechamps, G.; Russell, T.; Dyrbye, L.; Satele, D.; Collicott, P.; Novotny, P.J.; Sloan, J.; Freischlag, J. Burnout and medical errors among American surgeons. Ann. Surg. 2010, 251, 995–1000. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Balch, C.M.; Dyrbye, L.; Bechamps, G.; Russell, T.; Satele, D.; Rummans, T.; Swartz, K.; Novotny, P.J.; Sloan, J.; et al. Special report: Suicidal ideation among American surgeons. Arch. Surg. 2011, 146, 54–62. [Google Scholar] [CrossRef]
- Dimou, F.M.; Eckelbarger, D.; Riall, T.S. Surgeon burnout: A systematic review. J. Am. Coll. Surg. 2016, 222, 1230–1239. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C. Finding solutions to the problem of burnout. Consult. Psychol. J. Pract. Res. 2017, 69, 143–152. [Google Scholar] [CrossRef]
- Balasubramanian, A.; Paleri, V.; Bennett, R.; Paleri, V. Impact of COVID-19 on the mental health of surgeons and coping strategies. Head Neck 2020, 42, 1638–1644. [Google Scholar] [CrossRef] [PubMed]
- Krasner, M.S.; Epstein, R.M.; Beckman, H.; Suchman, A.L.; Chapman, B.; Mooney, C.J.; Quill, T.E. Association of an educational program in mindful communication with burnout, empathy, and attitudes among primary care physicians. JAMA 2009, 302, 1284–1293. [Google Scholar] [CrossRef] [PubMed]
- Lebares, C.C.; Guvva, E.V.; Ascher, N.L.; O’Sullivan, P.S.; Harris, H.W.; Epel, E.S. Burnout and Stress among US Surgery Residents: Psychological Distress and Resilience. J. Am. Coll. Surg. 2018, 226, 80–90. [Google Scholar] [CrossRef]
- Liu, K.; Chen, Y.; Wu, D.; Lin, R.; Wang, Z.; Pan, L. Effects of progressive muscle relaxation on anxiety and sleep quality in patients with COVID-19. Complement Ther. Clin. Pract. 2020, 6, 101132. [Google Scholar] [CrossRef]
- Yeo, C.J.; Barbieri, A.; Roman, G.; Wiesman, J.; Powell, S. Using smartphone mindfulness apps to increase trainee resilience and reduce burnout. Neurology 2019, 92 (Suppl. 15), P2.9-005. [Google Scholar]
- American Psychiatric Association. App Evaluation Model. 2017. Available online: https://www.psychiatry.org/psychiatrists/practice/mentalhealth-apps/app-evaluation-model (accessed on 2 December 2022).
- Pospos, S.; Young, I.T.; Downs, N.; Iglewicz, A.; Depp, C.; Chen, J.Y.; Newton, I.; Lee, K.; Light, G.A.; Zisook, S. Web-based tools and mobile applications to mitigate burnout, depression, and suicidality among healthcare students and professionals: A systematic review. Acad. Psychiatry 2018, 42, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.S.; Chee, C.Y.; Ho, R.C. Mental health strategies to combat the psychological impact of COVID-19 beyond paranoia and panic. Ann. Acad. Med. Singap. 2020, 49, 155–160. [Google Scholar] [CrossRef]
- Real-Ramirez, J.; Alberto Garcia-Bello, L.; Robles-Garcia, R.; Martinez, M.; Adame-Rivas, K.; Balderas-Pliego, M.; Garcia-Alfaro, C.; Perez-Cabanas, E.; Sierra-Medina, S.; Romero-Gonzalez, M.; et al. Well-being status and post-traumatic stress symptoms in health workers attending mindfulness sessions during the early stage of the COVID-19 epidemic in Mexico. Salud Ment. 2020, 43, 303–310. [Google Scholar] [CrossRef]
- Gaiaschi, C. Same job, different rewards: The gender pay gap among physicians in Italy. Gend. Work Organ. 2019, 26, 1562–1588. [Google Scholar] [CrossRef]
- Iorga, M.; Socolov, V.; Muraru, D.; Dirtu, C.; Soponaru, C.; Ilea, C.; Socolov, D.-G. Factors Influencing Burnout Syndrome in Obstetrics and Gynecology Physicians. BioMed Res. Int. 2017, 2017, 9318534. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, A.; Sampogna, G.; Giallonardo, V.; Del Vecchio, V.; Luciano, M.; Albert, U.; Carmassi, C.; Carrà, G.; Cirulli, F.; Dell’Osso, B.; et al. Effects of the lockdown on the mental health of the general population during the COVID-19 pandemic in Italy: Results from the COMET collaborative network. Eur. Psychiatry 2020, 63, e87. [Google Scholar] [CrossRef] [PubMed]
- Khosravi, M. Burnout among Iranian medical students: Prevalence and its relationship to personality dimensions and physical activity. Eur. J. Transl. Myol. 2021, 31, 9411. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Wang, W.; Hong, J.; Luan, B.; Zhu, Y.; Wang, J. Subjective well-being and job burnout of clinical nurses: The role of empathy. Chin. Nurs. Manag. 2015, 15, 280–284. [Google Scholar] [CrossRef]
- Yu, J.; Chae, S. The mediating effect of resilience on the relationship between the academic burnout and psychological well-being of medical students. Korean J. Med. Educ. 2020, 32, 256. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Categories | Total N = 2196 | Percentage |
|---|---|---|---|
| Gender | Male Female | 413 1783 | 18.8% 81.2% |
| Duration of employment | Less than one year | 56 | 2.6% |
| 1–2 years | 137 | 6.2% | |
| 3–5 years | 196 | 8.9% | |
| 6–10 years | 215 | 9.8% | |
| More than 10 years | 1592 | 72.0% | |
| Profession | Physicians | 486 | 22.1% |
| Nurses | 1157 | 52.7% | |
| Paramedics | 160 | 7.3% | |
| Non-medical profession | 173 | 7.9% | |
| Other medical profession | 220 | 10.1% | |
| Workload during the COVID-19 pandemic | The same amount of time as before (before the pandemic) | 1293 | 58.9% |
| Less than before the pandemic | 142 | 6.5% | |
| More than before the pandemic | 761 | 34.7% | |
| Workplace mobbing experienced in the COVID-19 pandemic | Never | 1379 | 62.8% |
| Almost never | 279 | 12.7% | |
| Sometimes | 300 | 13.6% | |
| Quite often | 77 | 3.5% | |
| Very often | 37 | 1.7% | |
| Refused to answer | 124 | 5.6% | |
| Workplace trauma | Yes, I did. | 725 | 33.0% |
| No. | 1091 | 49.7% | |
| I do not know. | 241 | 11.0% | |
| Refused to answer | 139 | 6.3% | |
| Financial situation | Rather bad | 155 | 7.1% |
| Fair | 1123 | 51.1% | |
| Good | 632 | 28.8% | |
| Refused to answer | 286 | 13.0 % | |
| Stress level | Increased and high | 1209 | 55.1% |
| Low | 987 | 44.9% |
| Profession | N | M (SD) | Levels of Occupational Burnout (%) | p | ||
|---|---|---|---|---|---|---|
| Lack of Burnout | At Risk for Burnout | At a Significant Risk for Burnout | ||||
| Physicians | 486 | 2.26 (0.66) | 66.9 | 17.3 | 15.8 | Chi-sq. = 17.719 d.f. = 8 p = 0.023 |
| Nurses | 1157 | 2.30 (0.69) | 63.5 | 18.1 | 18.4 | |
| Paramedic | 160 | 2.19 (0.69) | 70.6 | 15.0 | 14.4 | |
| Non-medical profession | 173 | 2.19 (0.74) | 72.3 | 11.0 | 16.8 | |
| Other medical profession | 220 | 2.15 (0.69) | 75.0 | 11.8 | 13.2 | |
| Increased and High Stress Level | Mobbing | Traumatic Event | |
|---|---|---|---|
| % (N) | % (N) | % (N) | |
| Physicians | 50.4 (245) | 14.2 (69) | 33.5 (163) |
| Nurses | 58.6 (678) | 20.3 (235) | 36.2 (419) |
| Paramedics | 56.9 (91) | 24.4 (39) | 41.3 (66) |
| Non-medical professions | 51.4 (89) | 17.9 (31) | 19.1 (33) |
| Other medical profession | 55.1 (106) | 18.2 (40) | 20.0 (44) |
| Chi-square test | 15.436 | 15.496 | 42.374 |
| DF 1 | 4 | 8 | 4 |
| p 2 | 0.004 | 0.050 | <0.001 |
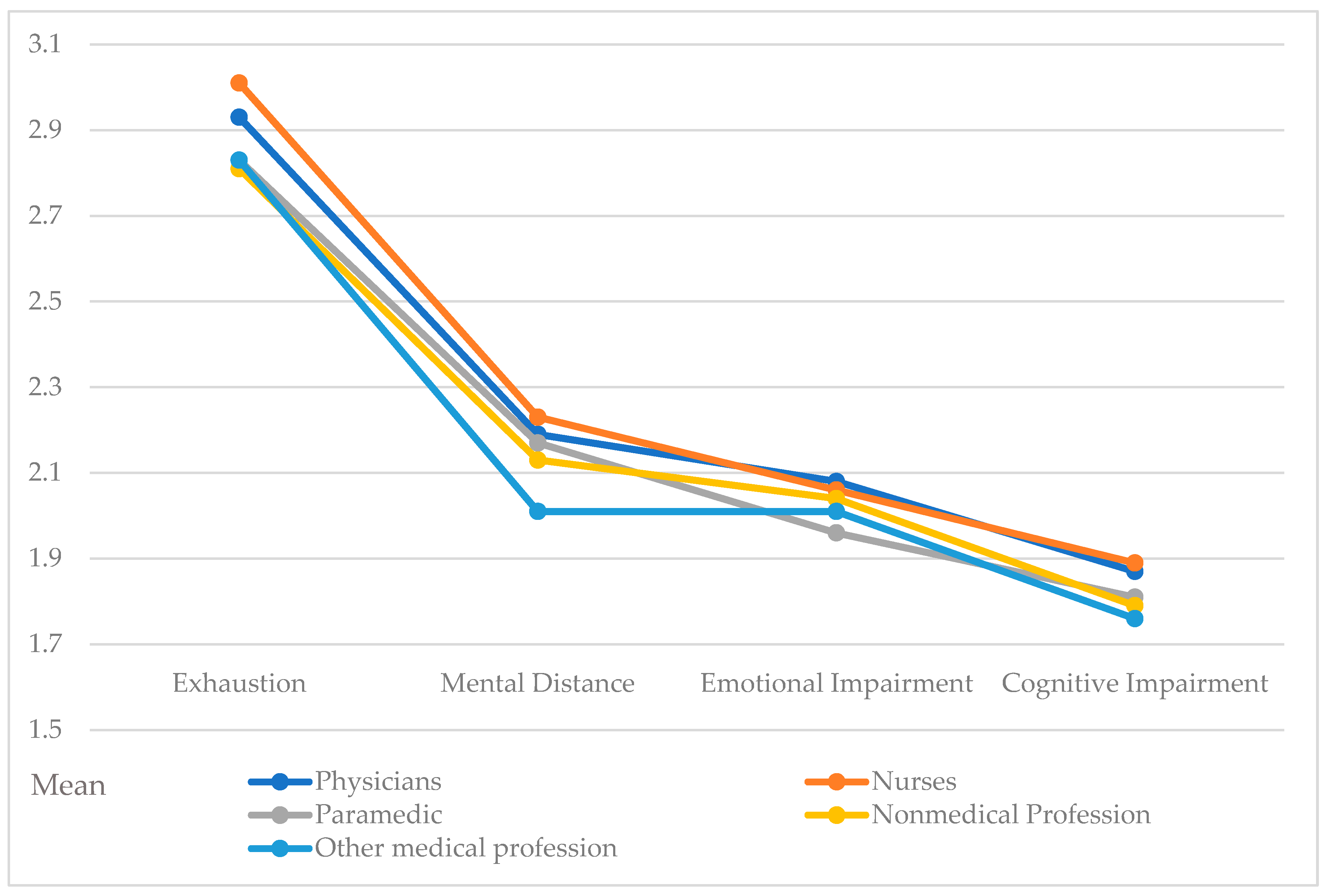
| Exhaustion | Mental Distance | Emotional Impairment | Cognitive Impairment | |
|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | M (SD) | |
| Physicians | 2.93 (0.85) | 2.19 (0.85) | 2.08 (0.77) | 1.87 (0.75) |
| Nurses | 3.01 (0.91) | 2.23 (0.84) | 2.06 (0.77) | 1.89 (0.78) |
| Paramedics | 2.83 (0.94) | 2.17 (0.87) | 1.96 (0.77) | 1.81 (0.77) |
| Non-medical Professions | 2.81 (1.01) | 2.13 (0.93) | 2.04 (0.76) | 1.79 (0.83) |
| Other medical profession | 2.83 (0.89) | 2.01 (0.82) | 2.01 (0.77) | 1,76 (0.78) |
| DF 1 | 3 | 3 | 3 | 3 |
| H-KW 2 | 17.855 | 16.175 | 4.580 | 11.474 |
| p3 | <0.001 | 0.003 | 0.333 | 0.022 |
| 95% Confidence Interval | ||||
|---|---|---|---|---|
| % Burnout | OR 1 | Lower | Upper | |
| Duration of employment | ||||
| Less than one year | 21.4% | 1 | ||
| 1–2 years | 30.7% | 1.736 | 0.8296 | 3.632 |
| 3–5 years | 27.6% | 1.484 | 0.7262 | 3.033 |
| 6–10 years | 41.4% | 2.619 * | 1.3033 | 5.263 |
| More than 10 years | 33.7% | 1.681 | 0.8747 | 3.231 |
| Workload | ||||
| The same as before the pandemic | 29.3% | 1 | ||
| Less than before the pandemic | 30.3% | 1.081 | 0.739 | 1.580 |
| More than before the pandemic | 40.9% | 1.661 * | 1.372 | 2.011 |
| Mobbing | ||||
| No | 27.7% | 1 | ||
| Yes | 55.3% | 3.253 * | 2.601 | 4.068 |
| Refused to answer | 35.5% | 1.424 | 0.969 | 2.093 |
| Traumatic event | ||||
| No | 24.3% | 1 | ||
| Yes | 45.9% | 2.599 * | 2.120 | 3.185 |
| Don’t know or refused to answer | 35.5% | 1.720 * | 1.336 | 2.214 |
| Financial situation | ||||
| Good | 26.6% | 1 | ||
| Poor | 51.0% | 3.379 * | 2.314 | 4.933 |
| Fair | 37.0% | 1.692 * | 1.353 | 2.117 |
| Refused to answer | 24.8% | 0.955 | 0.689 | 1.323 |
| Stress level | ||||
| Low | 16.2% | 1 | ||
| Increased and high | 47.6% | 4.770 * | 3.8845 | 5.858 |
| 95% Confidence Interval | ||||
|---|---|---|---|---|
| Predictor | p | Odds Ratio | Lower | Upper |
| Age | 0.037 | 0.987 | 0.976 | 0.999 |
| Gender | ||||
| Male—ref. | 1 | |||
| Female | 0.446 | 1.130 | 0.825 | 1.549 |
| Duration of employment | ||||
| Less than one year—ref. | 1 | |||
| 1–2 years | 0.089 | 1.584 | 0.932 | 2.692 |
| 3–5 years | 0.316 | 1.286 | 0.787 | 2.101 |
| 6–10 years | 0.004 | 2.095 | 1.262 | 3.447 |
| More than 10 years | 0.007 | 1.953 | 1.204 | 3.167 |
| Profession | ||||
| Other medical profession—ref. | 1 | |||
| Physicians | 0.005 | 1.822 | 1.194 | 2.782 |
| Nurses | 0.068 | 1.420 | 0.974 | 2.071 |
| Paramedics | 0.655 | 0.885 | 0.518 | 1.513 |
| Non-medical profession | 0.548 | 1.116 | 0.706 | 1.925 |
| Workload | ||||
| The same as before the pandemic | 1 | |||
| Less than before the pandemic | 0.737 | 1.074 | 0.708 | 1.630 |
| More than before the pandemic | 0.002 | 1.414 | 1.140 | 1.754 |
| Mobbing | ||||
| No experience—ref. | 1 | |||
| Experienced | <0.001 | 2.337 | 1.828 | 2.988 |
| Refused to answer | 0.563 | 1.134 | 0.741 | 1.735 |
| Traumatic event | ||||
| No experience—ref. | 1 | |||
| Yes | <0.001 | 1.910 | 1.522 | 2.397 |
| Don’t know/Refused to answer | 0.016 | 1.416 | 1.068 | 1.878 |
| Financial situation | ||||
| Good—ref. | 1 | |||
| Rather poor | <0.001 | 2.040 | 1.347 | 3.091 |
| Fair | 0.008 | 1.396 | 1.091 | 1.788 |
| Refused to answer | 0.239 | 0.826 | 0.577 | 1.184 |
| Stress level | ||||
| Low—ref. | 1 | |||
| Increased or high | <0.001 | 3.878 | 3.126 | 4.810 |
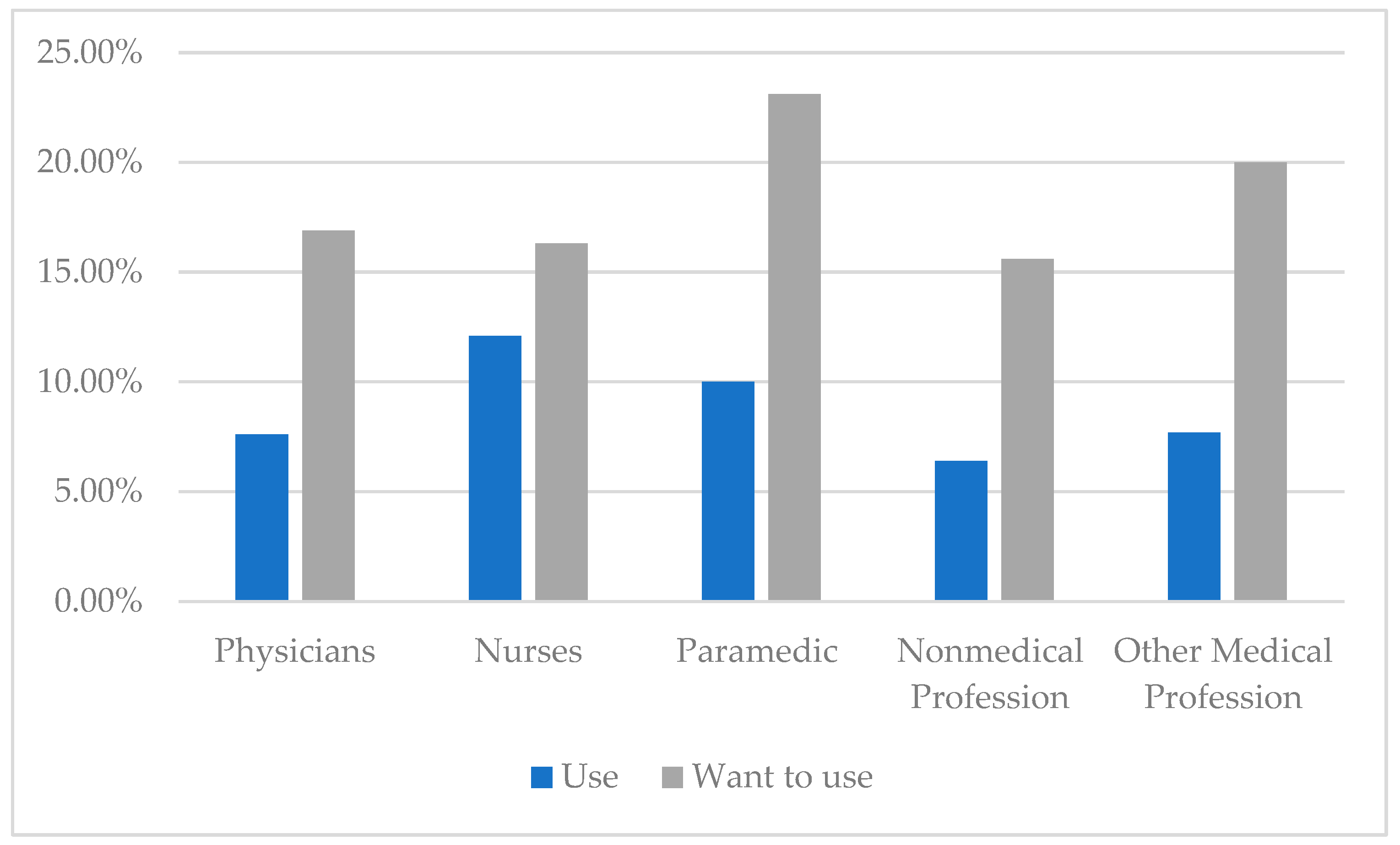
| Lack of Burnout (N = 1463) | At Risk for Burnout (N = 362) | Burned Out (N = 371) | ||||
|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |
| Receiving help | 58 | 4.0% | 36 | 10.0% | 83 | 22.3% |
| Willing to use help | 122 | 8.3% | 73 | 20.1% | 185 | 49.9% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Izdebski, Z.; Kozakiewicz, A.; Białorudzki, M.; Dec-Pietrowska, J.; Mazur, J. Occupational Burnout in Healthcare Workers, Stress and Other Symptoms of Work Overload during the COVID-19 Pandemic in Poland. Int. J. Environ. Res. Public Health 2023, 20, 2428. https://doi.org/10.3390/ijerph20032428
Izdebski Z, Kozakiewicz A, Białorudzki M, Dec-Pietrowska J, Mazur J. Occupational Burnout in Healthcare Workers, Stress and Other Symptoms of Work Overload during the COVID-19 Pandemic in Poland. International Journal of Environmental Research and Public Health. 2023; 20(3):2428. https://doi.org/10.3390/ijerph20032428
Chicago/Turabian StyleIzdebski, Zbigniew, Alicja Kozakiewicz, Maciej Białorudzki, Joanna Dec-Pietrowska, and Joanna Mazur. 2023. "Occupational Burnout in Healthcare Workers, Stress and Other Symptoms of Work Overload during the COVID-19 Pandemic in Poland" International Journal of Environmental Research and Public Health 20, no. 3: 2428. https://doi.org/10.3390/ijerph20032428
APA StyleIzdebski, Z., Kozakiewicz, A., Białorudzki, M., Dec-Pietrowska, J., & Mazur, J. (2023). Occupational Burnout in Healthcare Workers, Stress and Other Symptoms of Work Overload during the COVID-19 Pandemic in Poland. International Journal of Environmental Research and Public Health, 20(3), 2428. https://doi.org/10.3390/ijerph20032428