
Policy Analysis of the Integration of Sports and Medicine against the Backdrop of “Healthy China”: A Qualitative Study Using NVivo


Abstract
1. Introduction
2. Study Design
2.1. Data Sources and Selection
2.2. Research Tools and Methods
2.3. Theoretical Basis and Analytical Framework
3. Research Results
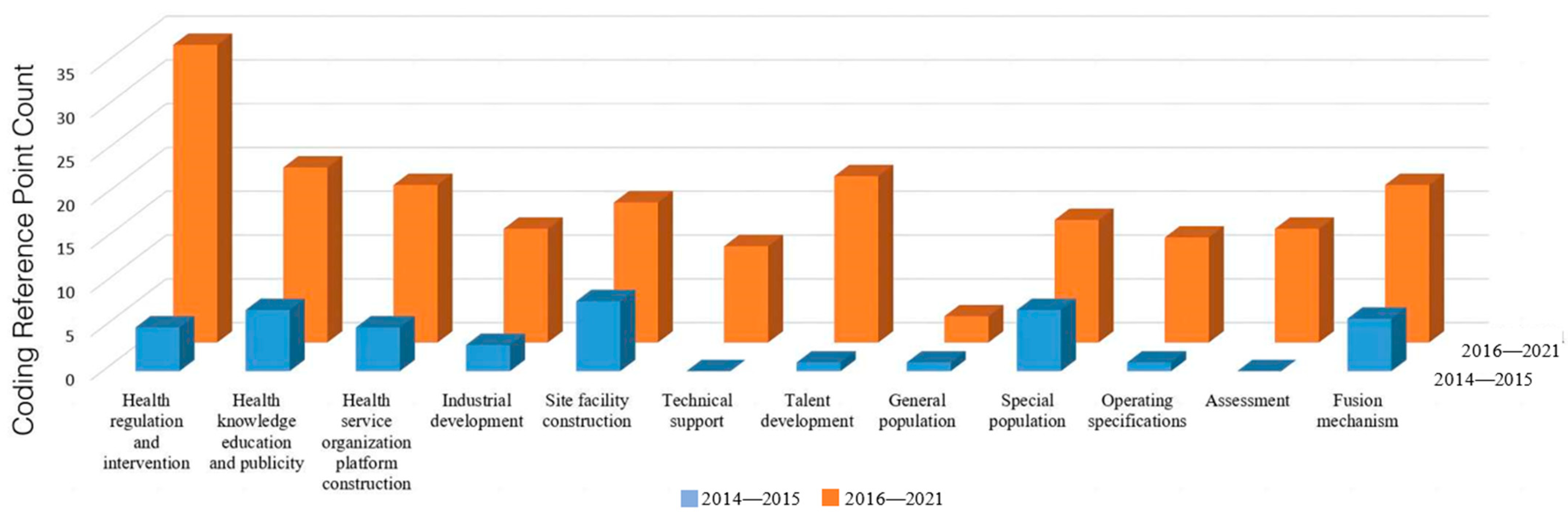
3.1. Policy Practice Distribution
3.2. Analysis of the Main Points of the Policy of Integration of Sports and Medicine
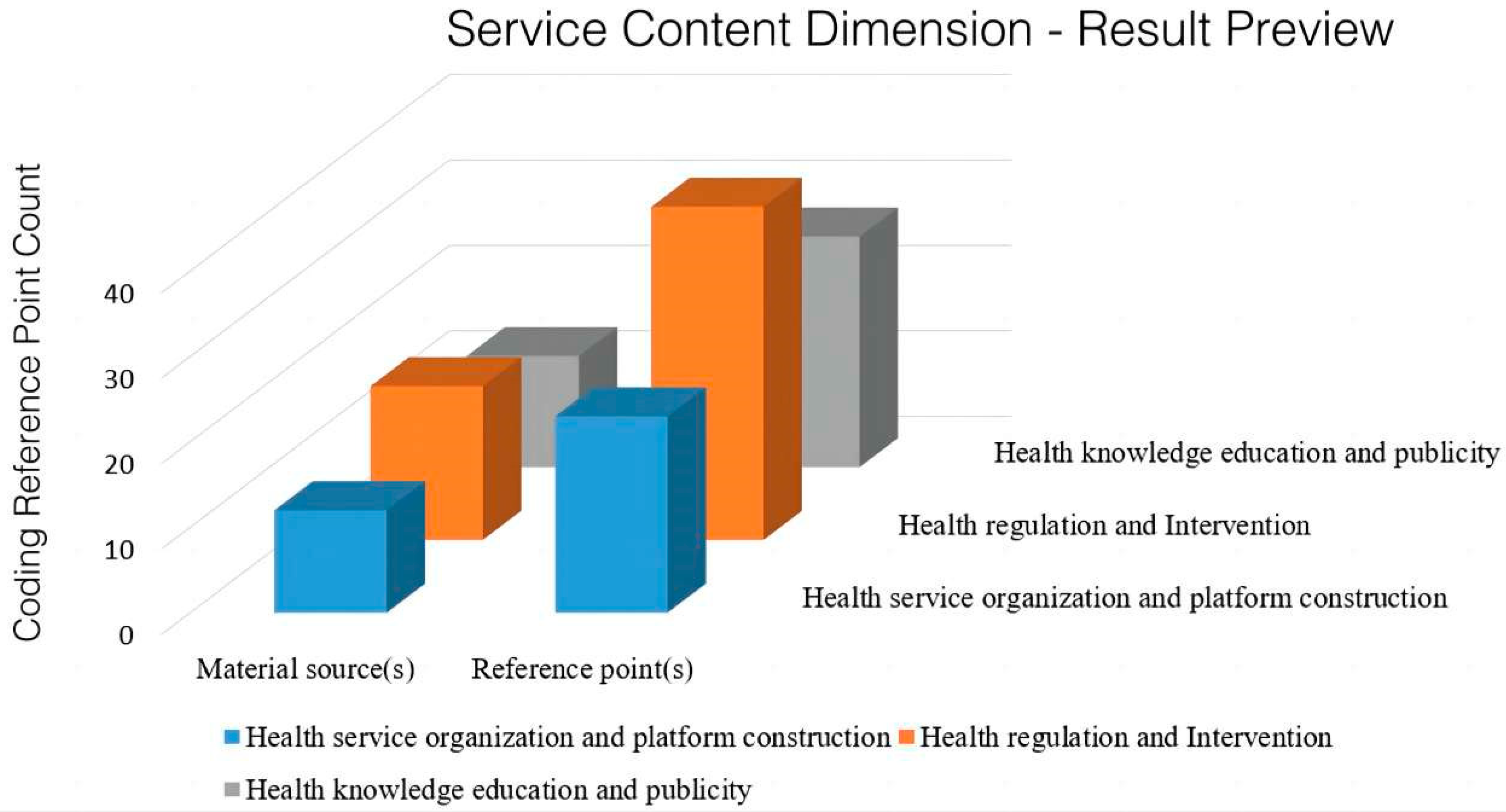
3.2.1. Analysis of the Main Points of the Policy Service Content with respect to the Integration of Sports and Medicine
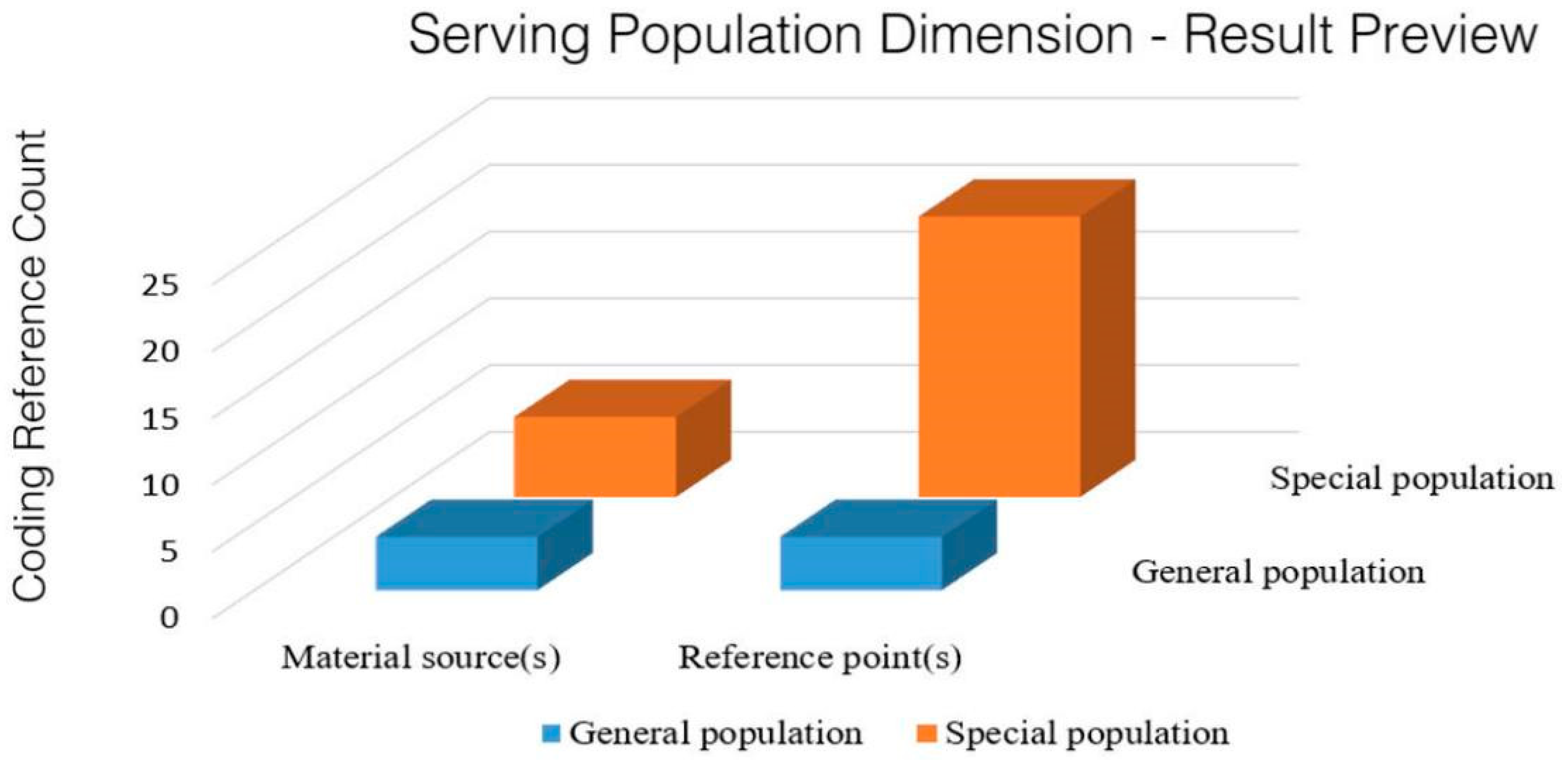
3.2.2. Analysis of the Main Points of the Population Served by the Policy of Integration of Sports and Medicine
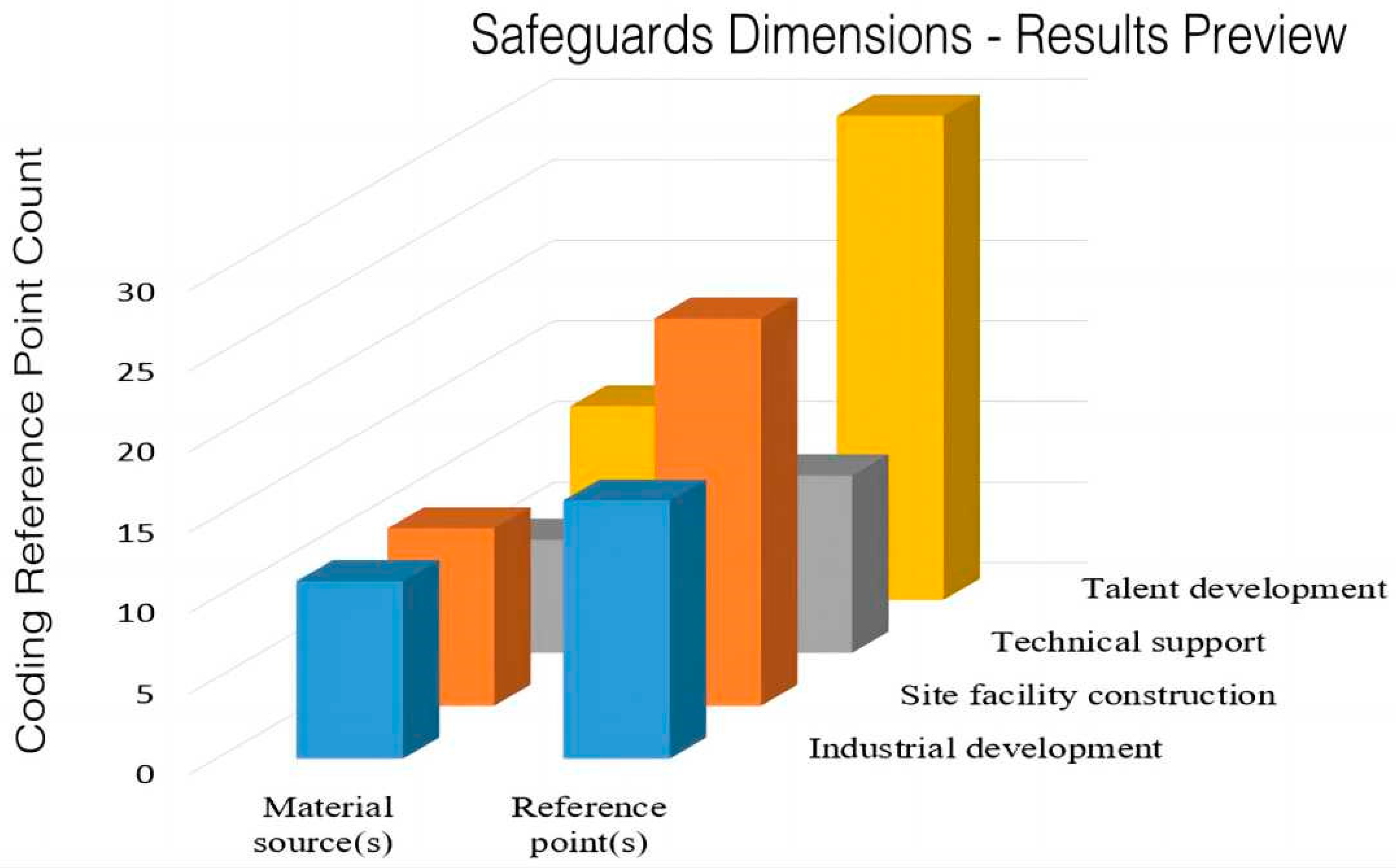
3.2.3. Analysis of the Main Points of the Policy Safeguards for the Integration of Sports and Medicine
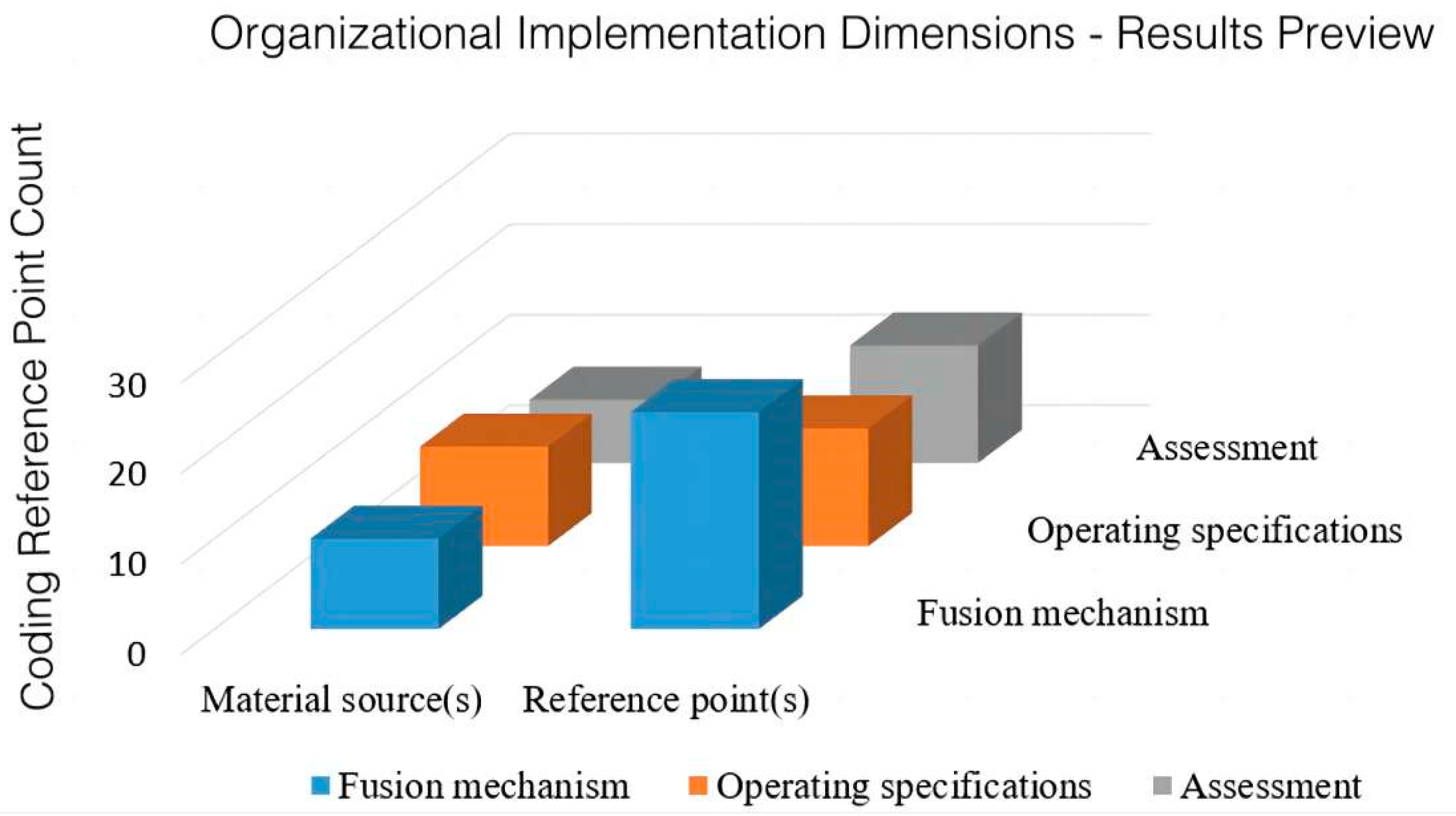
3.2.4. Analysis of the Main Points of the Organization and Implementation of the Policy of Integration of Sports and Medicine
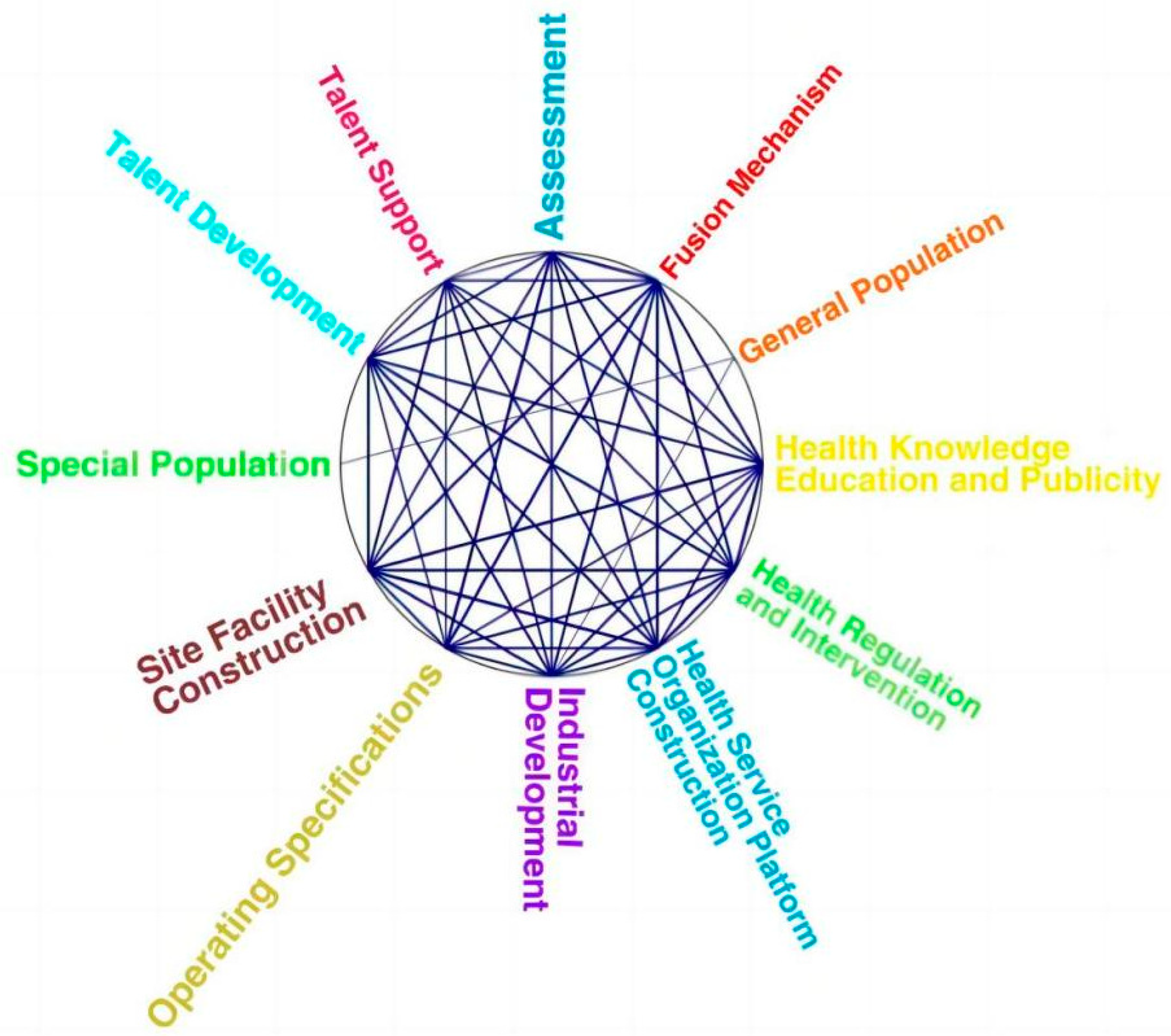
4. Coding Cluster Analysis of Integration of Sports and Medicine Policy Text
4.1. Insufficient Attention to Specific Service Populations
4.2. Lack of Attention to Sports Risk Assessment Issues
5. Policy Evolution and Use of Practical Tools
5.1. Policy Evolution
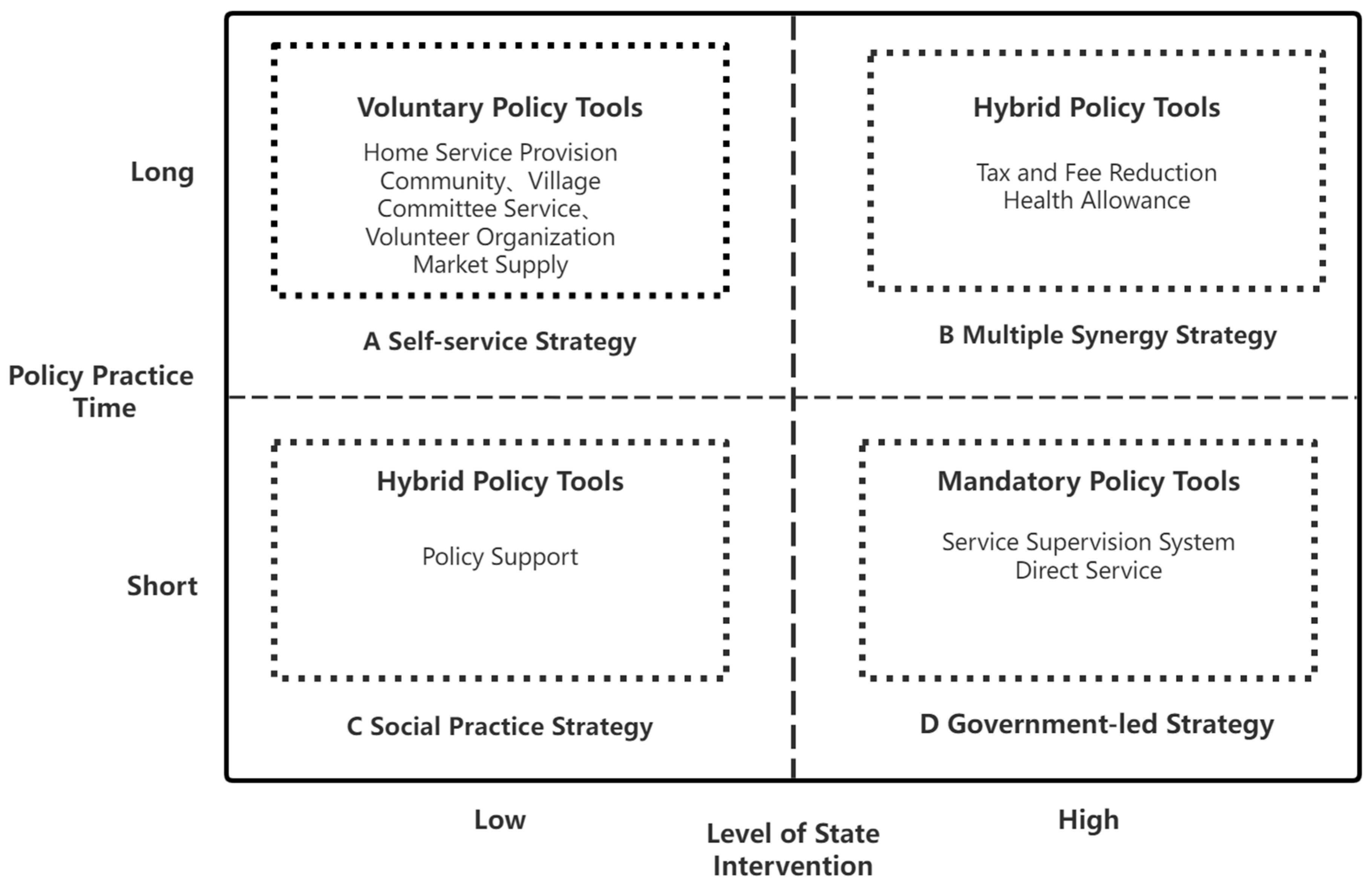
5.2. Practice Tool Usage
6. Conclusions
6.1. Research Limitations
6.2. Future Prospects of Policies of the Integration of Sports and Medicine in China
Active Attention to the Division of Specific Service Populations and Service Supply Issues
6.3. Valuing the Social Needs of Sport Risk Assessment
6.4. Focus on Balancing the Proportion of Policy Tools Used
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The CPC Central Committee, The State Council. The “Healthy China 2030” Plan Outline. 2016. Available online: www.gov.cn/zhengce/2016-10/25/content_5124174.htm (accessed on 15 October 2022).
- Dong, H. Analysis of Hotspots and Evolution Trends about Chinese Integration of Physical Education and Medicine Based on CiteSpace. J. Nanjing Inst. Phys. Educ. 2021, 20, 19–29. [Google Scholar]
- Fang, X.-L.; Fan, M. Research on Relevant Policies of “Sports Medical Integration” in the Context of Healthy China. In Proceedings of the Compilation of Abstracts from the 7th China Sports Doctor Forum [China Conference], Xinxiang, China, 28–30 June 2018; pp. 141–142. [Google Scholar]
- Chai, W.-J.; Liu, L.-F. Integration measurement and spatiotemporal evolution of China’ s sports industry and medical and health industry. J. Shandong Inst. Phys. Educ. 2021, 37, 20–31. [Google Scholar]
- Yu, H.-J.; Feng, X.-L.; Chou, J. A Review of the Research on the “Integration of Sports and Medicine” from the Perspective of “Healthy China”. J. Cap. Univ. Phys. Educ. 2020, 32, 484–491. [Google Scholar]
- Wang, L.; Gao, P. Rooted Theory and Its Application in Management Research. Foreign Econ. Manag. 2010, 32, 10–18. [Google Scholar]
- Jia, Z.-M. Application of Rooted Theory in Public Administration Research: Methods and Practice. J. Adm. China 2015, 03, 90–95. [Google Scholar]
- Jiang, X.; Wang, D.-Z. Stakeholder Perspective—Qualitative Text Analysis Based on Nvivo 12. Intell. Theory Pract. 2022, 45, 92–102. [Google Scholar]
- Zhao, H.-B.; Peng, Q. An Exploratory Study on Practical Competence Based on Prounded Theory. J. Chengdu Inst. Phys. Educ. 2022, 48, 74–79. [Google Scholar]
- Yang, J.-X.; Chen, J.-Q.; Gao, K.-T. Origin and Measures of Policies on Intergrated Development of Sports and Medicine: An Understanding of General Secretary Xi Jinping’s Important Discussions on Integrated Development. J. Wuhan Sport. Univ. 2022, 56, 45–53. [Google Scholar]
- Wang, Z.; Xu, C. Analysis of the population aging policies in the health planning outlines of 23 provinces: A qual-itative research from the perspective of healthy aging by Nvivo 12. Health Policy Res. China 2021, 14, 8–15. [Google Scholar]
- Shen, X. An overview of Current Situation and Trend of Theoretical Application of Sports Policy Analysis. J. Wuhan Inst. Phys. Educ. 2020, 54, 16–25+63. [Google Scholar]
- Fang, Y.-H.; Liu, J.-M. Mining and quantitative evaluation of the elderly care service policy of the State Council based on PMC index model. J. Yunnan Adm. Coll. 2020, 22, 167–176. [Google Scholar]
- Hou, B. Research on the Level of Demand and Its Satisfaction Strategies for Urban Elderly; East China Normal University: Shanghai, China, 2018. [Google Scholar]
- Li, J.-Y.; Liang, C.; Gao, C. Research on the Connotation and Path of Sports and Medicine Convergence—A Case Study of Exercise Prescription Clinic. China Sport. Sci. 2019, 39, 23–32. [Google Scholar]
- Chen, X.-H.; Guo, J.-J. Construction of Service Framework of Integration of Sports and Medicine in China Under the Background of Proactive Health. J. Cap. Univ. Phys. Educ. 2021, 33, 474–480. [Google Scholar]
- Guo, Y.-X.; Liu, S.-M.; Wang, W.-G. Analysis of Qualitative Research Data: NVivo8’s Living Treasure; Higher Education and Cultural Undertakings Co., Ltd.: Taipei, Taiwan, 2009. [Google Scholar]
- Roya, S.; Lawrence, S.C.; Robert, C.C. Sports Medicine: Concussions in Sports. Am. J. Lifestyle Med. 2012, 6, 133–140. [Google Scholar]
- Blair, S.N. Physical activity, clinical medicine, and public health. Curr. Sport. Med. Rep. 2007, 6, 71–72. [Google Scholar]
- Heath, G.W. Physical Activity Transitions and Chronic Disease. Am. J. Lifestyle Med. 2009, 3, 27S–31S. [Google Scholar] [CrossRef]
- Xue, X.; Xu, F.-Z.; Guo, J.-J. Research on the Current Situation and Policy Issues Confirmation of Sports and Medicine Integration in China. J. Sport. Res. 2021, 35, 20–28. [Google Scholar]
- Wang, S.-Q.; Lv, W.-G. Exploration on the service mode of physical and medical integration for the prevention and treatment of chronic diseases in the context of “Healthy China”. Chin. J. Prev. Control Chronic Dis. 2020, 28, 792–797. [Google Scholar]
- Xu, H.-D. The new development and enlightenment of chinese residents’ health literacy. Popul. Health 2021, 10, 25–29. [Google Scholar]
- Li, J.; Zhang, L. Research on the Experiences, Realistic Challenges, Countermeasure of Chronic Disease Prevention and Treatment of Integration of Sports and Medicine in Construction of Healthy China. China Sport Sci. 2020, 40, 73–82. [Google Scholar]
- McCrory, P. The reformation of sports medicine. Br. J. Sport. Med. 2007, 41, 281–282. [Google Scholar]
- Han, C.-Y. Development Dilemma and Promotion Path of the Integration of Sports and Medicine Under Healthy China Strategy. Sport. Cult. Guide 2021, 61–66. [Google Scholar]
- Zhang, Y.; Wang, Z.-H.; Zhang, M. Service Demand, Constraints and Development Ideas of Integration of Sports and Medical Care in the Context of Healthy China: A Case Study of Hefei City. J. Shenyang Sport Univ. 2020, 30, 61–67+87. [Google Scholar]
- Lu, W.-Y.; Wang, Z.-H.; Chen, P.-J. Consideration of Deepening the Research on Physical-Medical Integrationin the Context of Establishing Healthy China and Sports Power. J. Shanghai Univ. Sport 2021, 45, 40–50. [Google Scholar]
- Wang, X.-Y.; Wang, J.-Y. Policy Features and Development Strategies of the Integration of Sports and Medicine in China. Sport. Cult. Guide 2021, 59–65. [Google Scholar]
- Yang, X.-L. Investigation on the status quo of health education demand of physical examination population in different age groups. J. Qilu Nurs. 2017, 23, 46–47. [Google Scholar]
- Luo, Y.; Zhang, E.-L. Research on risk prevention of sports injury in primary and secondary schools in China. In Proceedings of the The First Shaanxi Provincial Sports Science Paper Report Excellent Paper Collection. [China Conference], Xi’an, China, 16 May 2021; pp. 819–827. [Google Scholar]
- Ji, L.-Y. Research on the Policy of Lower Body Medical Integrationfrom the Perspective of Policy Tools; Wuhan Institute of Physical Education: Wuhan, China, 2021. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Date of Promulgation | Document Name | Policy Sources |
|---|---|---|
| 20 October 2014 | Some Opinions on Accelerating the Development of Sports Industry and Promoting Sports Consumption | General Office of the State Council |
| 22 November 2015 | Guiding Opinions on Accelerating the Development of Life Service Industry and Promoting the Upgrade of Consumption Structure | General Office of the State Council |
| 25 October 2016 | Outline of “Healthy China 2030” Plan | The CPC Central Committee and the State Council |
| 28 October 2016 | Guiding Opinions on Accelerating the Development of Fitness and Leisure Industry | General Office of the State Council |
| 16 November 2016 | Guiding Opinions on Strengthening Health Promotion and Education | Ministry of Education, etc. |
| 22 January 2017 | Notice on Printing and Distributing China’s Medium and Long term Plan for the Prevention and Control of Chronic Diseases (2017–2025) | General Office of the State Council |
| 27 April 2017 | Notice on Issuing the Action Plan for Healthy Lifestyle for All (2017–2025) | National Health Commission, etc. |
| 16 May 2017 | Opinions on Supporting Social Forces to Provide Multilevel and Diversified Medical Services | General Office of the State Council |
| 30 June 2017 | Notice on Issuing the National Nutrition Plan (2017–2030) | General Office of the State Council |
| 15 July 2019 | Opinions on Implementing the Action of Healthy China | General Office of the State Council |
| 2 September 2019 | Notice on Printing and Distributing the Outline of Building a Sports Powerful Country | General Office of the State Council |
| 18 September 2019 | Opinions on Promoting National Fitness and Sports Consumption to Promote the High Quality Development of Sports Industry | General Office of the State Council |
| 30 September 2019 | Notice on the Action Plan for Promoting the High Quality Development of Health Industry (2019–2022) | National Development and Reform Commission, Ministry of Education, etc. |
| 6 December 2019 | Opinions on Promoting the Development of “Internet Social Services” | National Development and Reform Commission, Ministry of Education, etc. |
| 13 October 2021 | Circular of The State Council of The People’s Republic of China on Several Opinions on Promoting The Living Service Industry to Improve The People’s Quality of Life | National Development and Reform Commission |
| High-Frequency Node | Number of Occurrences | High-Frequency Node | Number of Occurrences | High-Frequency Node | Number of Occurrences |
|---|---|---|---|---|---|
| health | 708 | mechanism | 98 | combination | 60 |
| service | 242 | chronic disease | 96 | data | 59 |
| sports | 224 | activity | 93 | knowledge | 58 |
| fitness | 197 | constitution | 92 | technology | 57 |
| national | 128 | guidance | 89 | information | 56 |
| work | 123 | get some action | 84 | disease | 54 |
| society | 123 | science | 80 | department | 54 |
| hygiene | 121 | the masses | 79 | community | 53 |
| sports | 118 | standard | 78 | organization | 53 |
| nutrition | 116 | system | 76 | propaganda | 51 |
| education | 110 | mode | 71 | psychology | 50 |
| country | 107 | crowd | 69 | recovery | 49 |
| medical | 105 | environment | 65 | major | 48 |
| life | 105 | physical exercise | 62 | mechanism | 48 |
| monitor | 101 | prevention and treatment | 62 | family | 44 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, B.; Lin, Q.; Wang, Y.; Tang, S. Policy Analysis of the Integration of Sports and Medicine against the Backdrop of “Healthy China”: A Qualitative Study Using NVivo. Int. J. Environ. Res. Public Health 2023, 20, 2079. https://doi.org/10.3390/ijerph20032079
Wang B, Lin Q, Wang Y, Tang S. Policy Analysis of the Integration of Sports and Medicine against the Backdrop of “Healthy China”: A Qualitative Study Using NVivo. International Journal of Environmental Research and Public Health. 2023; 20(3):2079. https://doi.org/10.3390/ijerph20032079
Chicago/Turabian StyleWang, Baihui, Qinqin Lin, Yawei Wang, and Shaokai Tang. 2023. "Policy Analysis of the Integration of Sports and Medicine against the Backdrop of “Healthy China”: A Qualitative Study Using NVivo" International Journal of Environmental Research and Public Health 20, no. 3: 2079. https://doi.org/10.3390/ijerph20032079
APA StyleWang, B., Lin, Q., Wang, Y., & Tang, S. (2023). Policy Analysis of the Integration of Sports and Medicine against the Backdrop of “Healthy China”: A Qualitative Study Using NVivo. International Journal of Environmental Research and Public Health, 20(3), 2079. https://doi.org/10.3390/ijerph20032079