
The Effects of Outdoor versus Indoor Exercise on Psychological Health, Physical Health, and Physical Activity Behaviour: A Systematic Review of Longitudinal Trials

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Review Protocol
2.2. Search Strategy and Screening
2.3. Eligibility Criteria
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Data Synthesis
3. Results
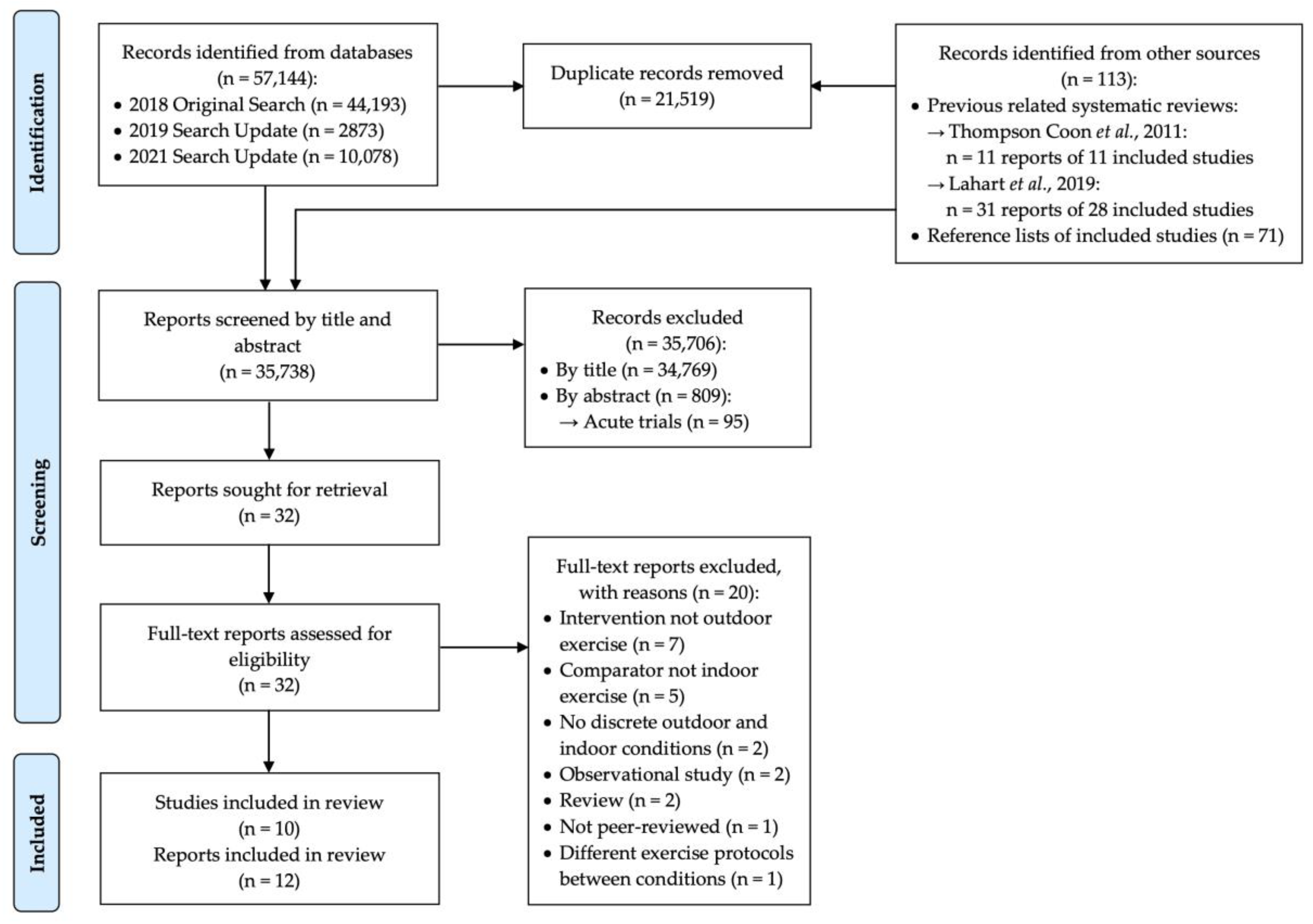
3.1. Search Results
3.2. Study Characteristics
3.2.1. Trial Design Characteristics
3.2.2. Participant Characteristics
3.2.3. Exercise Environment: Physical Setting and Conditions
3.2.4. Exercise Protocols
Time Spent Exercising
Exercise Type and Modality
Exercise Intensity
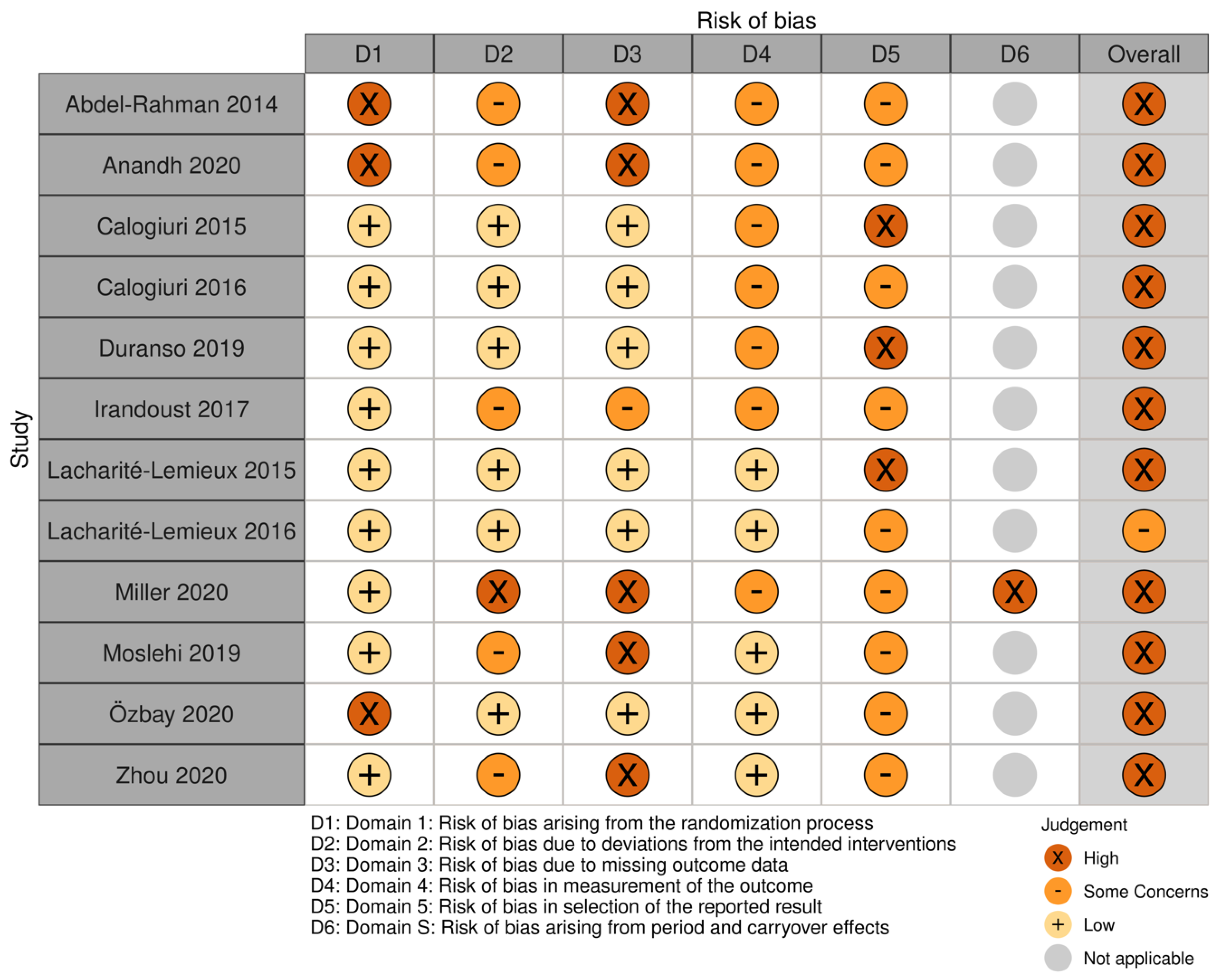
3.3. Risk of Bias
3.4. Study Outcomes
3.5. Results of Included Studies
3.5.1. Psychological Health Outcomes
3.5.2. Physical Health Outcomes
3.5.3. Physical Activity Behaviour
3.5.4. Overall Directionality of Findings
4. Discussion
4.1. Summary of Findings
4.2. Quality of Evidence
4.3. Limitations and Biases in the Current Review
4.4. Comparison to Previous Reviews
4.5. Recommendations for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B

{kind=link}
{kind=link}
{kind=link}
| Outcome Category | Discrete Outcomes (Measure) |
|---|---|
| PSYCHOLOGICAL HEALTH | |
| Affective Valence | general mood (Feeling Scale) |
| Positive Emotions | positive engagement (Exercise-Induced Feeling Inventory, EFI), positive affect (Physical Activity Affective Scale, PAAS), enjoyment of exercise (0–10 scale) |
| Depression | depression (Beck Depression Inventory) |
| Affective Activation | arousal state (Felt Arousal Scale) |
| Tranquility | tranquillity (EFI and PAAS) |
| Restoration | perceived environmental restorativeness (Perceived Restorativeness Scale: Fascination and Being Away subscales) |
| Energy | revitalization (EFI) |
| Fatigue | physical exhaustion (EFI), fatigue (Fatigue Scale-Adolescent) |
| Self-Efficacy and Self-Determination | social activity self-efficacy (scale NR), exercise self-efficacy (Exercise Self-Efficacy Scale), general self-efficacy (New Generalized Self-Efficacy Scale), psychological needs: autonomy, competence, and relatedness (Psychological Need Satisfaction in Exercise) |
| Motivation | exercise motivation (Achievement Goals Questionnaire for Sport; Behavioral Regulation in Exercise Questionnaire-2), global approach motivation (Appetitive Motivation Scale) |
| PHYSICAL HEALTH | |
| Weight | weight |
| Body Composition | body mass index, body fat %, fat mass, lean body mass, muscle mass index, waist circumference, waist-to-hip ratio |
| Systolic Blood Pressure | systolic blood pressure |
| Diastolic Blood Pressure | diastolic blood pressure |
| Plasma Lipids | triglycerides, total cholesterol, cholesterol–low-density lipoprotein, cholesterol–high-density lipoprotein |
| Glucose and Insulin Profile | fasting glucose, fasting insulin, HOMA-IR (Insulin Resistance based on the “Homeostasis Model Assessment”) |
| Hormones and Neuropeptides | cortisol, vitamin D, orexin A, irisin, adropin |
| Flexibility | flexibility (Sit and Reach Test) |
| Mobility | agility (Shuttle Run Test), functional mobility (Timed Up and Go Test), Timed 10-Meter Walk Test, 2-min walk test, multisurface terrain walk test |
| VO2max | maximum oxygen uptake |
| Muscle Strength | leg press, bench press, and lat pull down (one-repetition maximum, 1-RM) |
| Muscle Endurance | leg press, bench press, and lat pull down (maximum repetitions of 70% 1-RM) |
| Balance | single-leg standing test with eyes open, single-leg standing test with eyes closed, closed-cycles test |
| PHYSICAL ACTIVITY BEHAVIOUR | |
| Future Exercise Intention | intention to exercise in future (3-item scale) |
| Physical Activity Level | total weekly physical activity (Physical Activity Scale for the Elderly; Leisure Time Exercise Questionnaire; actigraphy), frequency of specific activities at follow-up (biking, strength) |
| Exercise Adherence | percentage of exercise sessions attended |
References
- World Health Organization. Physical Activity Fact Sheet. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 9 March 2018).
- Pedersen, B.K.; Saltin, B. Exercise as Medicine-Evidence for Prescribing Exercise as Therapy in 26 Different Chronic Diseases. Scand. J. Med. Sci. Sport. 2015, 25, 1–72. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.R.; Bredin, S.S.D. Health Benefits of Physical Activity: A Systematic Review of Current Systematic Reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef]
- Rebar, A.L.; Stanton, R.; Geard, D.; Short, C.; Duncan, M.J.; Vandelanotte, C. A Meta-Meta-Analysis of the Effect of Physical Activity on Depression and Anxiety in Non-Clinical Adult Populations. Health Psychol. Rev. 2015, 9, 366–378. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- de Souto Barreto, P. Why Are We Failing to Promote Physical Activity Globally? Bull. World Health Organ. 2013, 91, 390–390A. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide Trends in Insufficient Physical Activity from 2001 to 2016: A Pooled Analysis of 358 Population-Based Surveys with 1·9 Million Participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef]
- Pretty, J.; Griffin, M.; Sellens, M.; Pretty, C. Green Exercise: Complementary Roles of Nature, Exercise and Diet in Physical and Emotional Well-Being and Implications for Public Health Policy. CES Occas. Pap. Univ. Essex 2003, 1, 7. [Google Scholar]
- Menardo, E.; Brondino, M.; Hall, R.; Pasini, M. Restorativeness in Natural and Urban Environments: A Meta-Analysis. Psychol. Rep. 2021, 124, 417–437. [Google Scholar] [CrossRef]
- Norwood, M.F.; Lakhani, A.; Maujean, A.; Zeeman, H.; Creux, O.; Kendall, E. Brain Activity, Underlying Mood and the Environment: A Systematic Review. J. Environ. Psychol. 2019, 65, 101321. [Google Scholar] [CrossRef]
- Bratman, G.N.; Hamilton, J.P.; Hahn, K.S.; Daily, G.C.; Gross, J.J. Nature Experience Reduces Rumination and Subgenual Prefrontal Cortex Activation. Proc. Natl. Acad. Sci. USA 2015, 112, 8567–8572. [Google Scholar] [CrossRef]
- Bratman, G.N.; Daily, G.C.; Levy, B.J.; Gross, J.J. The Benefits of Nature Experience: Improved Affect and Cognition. Landsc. Urban Plan. 2015, 138, 41–50. [Google Scholar] [CrossRef]
- Stenfors, C.U.D.; Van Hedger, S.C.; Schertz, K.E.; Meyer, F.A.C.; Smith, K.E.L.; Norman, G.J.; Bourrier, S.C.; Enns, J.T.; Kardan, O.; Jonides, J.; et al. Positive Effects of Nature on Cognitive Performance across Multiple Experiments: Test Order but Not Affect Modulates the Cognitive Effects. Front. Psychol. 2019, 10, 1413. [Google Scholar] [CrossRef] [PubMed]
- Bowler, D.E.; Buyung-Ali, L.M.; Knight, T.M.; Pullin, A.S. A Systematic Review of Evidence for the Added Benefits to Health of Exposure to Natural Environments. BMC Public Health 2010, 10, 456. [Google Scholar] [CrossRef]
- Thompson Coon, J.; Boddy, K.; Stein, K.; Whear, R.; Barton, J.; Depledge, M.H. Does Participating in Physical Activity in Outdoor Natural Environments Have a Greater Effect on Physical and Mental Wellbeing than Physical Activity Indoors? A Systematic Review. Environ. Sci. Technol. 2011, 45, 1761–1772. [Google Scholar] [CrossRef] [PubMed]
- Lahart, I.; Darcy, P.; Gidlow, C.; Calogiuri, G. The Effects of Green Exercise on Physical and Mental Wellbeing: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 1352. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.M.; Sadak, K.T.; Shahriar, A.A.; Wilson, N.J.; Hampton, M.; Bhattacharya, M.; Towle, A.; Turcotte, L.M. Cancer Survivors Exercise at Higher Intensity in Outdoor Settings: The GECCOS Trial. Pediatr. Blood Cancer 2021, 68, e28850. [Google Scholar] [CrossRef]
- Moslehi, E.; Moslehi, Z.; Khalvati, B. Playing in Form of Outdoor Aerobic Exercise Is More Effective than Indoor Treadmill Exercise on Serum Orexin-A and Weight Loss in Obese Adolescent Boys. Obes. Med. 2019, 15, 100104. [Google Scholar] [CrossRef]
- Özbay, S.; Ulupinar, S.; Şebin, E.; Altinkaynak, K. Acute and Chronic Effects of Aerobic Exercise on Serum Irisin, Adropin, and Cholesterol Levels in the Winter Season: Indoor Training versus Outdoor Training. Chin. J. Physiol. 2020, 63, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.Y.; Yuan, X.M.; Ma, X.J. Canan Outdoor Multisurface Terrain Enhance the Effects of Fall Prevention Exercise in Older Adults? A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 7023. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Veritas Health Innovation. Covidence Systematic Review Software. Melbourne, Australia. Available online: www.covidence.org (accessed on 22 November 2022).
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-Bias VISualization (Robvis): An R Package and Shiny Web App for Visualizing Risk-of-Bias Assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Pasek, M.; Michalowska-Sawczyn, M.; Nowak-Zaleska, A. Changes in Maximal Aerobic Fitness and Students’ Attitude towards Physical Effort during Outdoor and Indoor School Lessons of Physical Education. Balt. J. Heal. Phys. Act. 2014, 6, 3. [Google Scholar] [CrossRef]
- Pasek, M.; Szark-Eckardt, M.; Wilk, B.; Zuzda, J.; Zukowska, H.; Opanowska, M.; Kuska, M.; Drozdz, R.; Kusmierczyk, M.; Saklak, W.; et al. Physical Fitness as Part of the Health and Well-Being of Students Participating in Physical Education Lessons Indoors and Outdoors. Int. J. Environ. Res. Public Health 2020, 17, 309. [Google Scholar] [CrossRef] [PubMed]
- Calogiuri, G.; Nordtug, H.; Weydahl, A. The Potential of Using Exercise in Nature as an Intervention to Enhance Exercise Behavior: Results from a Pilot Study. Percept. Mot. Skills 2015, 121, 350–370. [Google Scholar] [CrossRef] [PubMed]
- Calogiuri, G.; Evensen, K.; Weydahl, A.; Andersson, K.; Patil, G.; Ihlebæk, C.; Raanaas, R.K. Green Exercise as a Workplace Intervention to Reduce Job Stress. Results from a Pilot Study. Work 2016, 53, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Irandoust, K.; Taheri, M. The Effect of Vitamin D Supplement and Indoor Vs Outdoor Physical Activity on Depression of Obese Depressed Women. Asian J. Sports Med. 2017, 8, e13311. [Google Scholar] [CrossRef]
- Lacharité-Lemieux, M.; Brunelle, J.P.; Dionne, I.J. Adherence to Exercise and Affective Responses: Comparison between Outdoor and Indoor Training. Menopause 2015, 22, 731–740. [Google Scholar] [CrossRef]
- Lacharité-Lemieux, M.; Dionne, I.J. Physiological Responses to Indoor versus Outdoor Training in Postmenopausal Women. J. Aging Phys. Act. 2016, 24, 275–283. [Google Scholar] [CrossRef]
- Duranso, C.W. Walk for Well-Being: The Main Effects of Walking on Approach Motivation. Motiv. Emot. 2019, 43, 93–102. [Google Scholar] [CrossRef]
- Abdel-Rahman, O.; Magdy, S. The Impact of Green Exercise on Test of Performance Strategies, Physical Variables and Counter-Time Performance for Egyptian Epee Fencers. Ovidius Univ. Ann. Ser. Phys. Educ. Sport Sci. Mov. Health 2014, 14, 154–158. [Google Scholar]
- Anandh, S.; Varadharajulu, G.; Alate, M.M. Influence of Dual Task Training in Indoor versus Outdooenvironment on Physical Function and Social Activity among Elderly. Med. Legal Updat. 2020, 20, 495–499. [Google Scholar] [CrossRef]
- Miller, J.R.; Van Hooren, B.; Bishop, C.; Buckley, J.D.; Willy, R.W.; Fuller, J.T. A Systematic Review and Meta-Analysis of Crossover Studies Comparing Physiological, Perceptual and Performance Measures Between Treadmill and Overground Running. Sport. Med. 2019, 49, 763–782. [Google Scholar] [CrossRef]
- Van Hooren, B.; Fuller, J.T.; Buckley, J.D.; Miller, J.R.; Sewell, K.; Rao, G.; Barton, C.; Bishop, C.; Willy, R.W. Is Motorized Treadmill Running Biomechanically Comparable to Overground Running? A Systematic Review and Meta-Analysis of Cross-Over Studies. Sports Med. 2020, 50, 785–813. [Google Scholar] [CrossRef] [PubMed]
- Bertucci, W.; Grappe, F.; Groslambert, A. Laboratory versus Outdoor Cycling Conditions: Differences in Pedaling Biomechanics. J. Appl. Biomech. 2007, 23, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Garber, C.E.; Blissmer, B.; Deschenes, M.; Franklin, B.A.; LaMonte, M.J.; Lee, I.; Nieman, D.; Swain, D. American College of Sports Medicine Position Stand. Quantity and Quality of Exercise for Developing and Maintaining Cardiorespiratory, Musculoskeletal, and Neuromotor Fitness in Apparently Healthy Adults: Guidance for Prescribing Exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription; Wolters Kluwer Health: Philadelphia, PA, USA, 2018. [Google Scholar]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Meta-Analysis Methods Based on Direction and p-Values. In Introduction to Meta-Analysis; John Wiley & Sons, Ltd.: Chichester, UK, 2009; pp. 325–330. [Google Scholar]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. J. Clin. Epidemiol. 2010, 63, 834–840. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, S. The Restorative Benefits of Nature: Toward an Integrative Framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- Ulrich, R.S.; Simonst, R.F.; Lositot, B.D.; Fioritot, E.; Milest, M.A.; Zelsont, M. STRESS RECOVERY DURING EXPOSURE TO NATURAL AND URBAN ENVIRONMENTS. J. Environ. Psychol. 1991, 11, 201–230. [Google Scholar] [CrossRef]
- Gladwell, V.F.; Brown, D.K.; Wood, C.; Sandercock, G.R.; Barton, J.L. The Great Outdoors: How a Green Exercise Environment Can Benefit All. Extrem. Physiol. Med. 2013, 2, 3. [Google Scholar] [CrossRef]
- Stevenson, M.P.; Schilhab, T.; Bentsen, P. Attention Restoration Theory II: A Systematic Review to Clarify Attention Processes Affected by Exposure to Natural Environments. J. Toxicol. Environ. Health Part B Crit. Rev. 2018, 21, 227–268. [Google Scholar] [CrossRef]
- Jimenez, M.P.; DeVille, N.V.; Elliott, E.G.; Schiff, J.E.; Wilt, G.E.; Hart, J.E.; James, P. Associations between Nature Exposure and Health: A Review of the Evidence. Int. J. Environ. Res. Public Health 2021, 18, 4790. [Google Scholar] [CrossRef] [PubMed]
- Song, C.; Ikei, H.; Miyazaki, Y. Physiological Effects of Nature Therapy: A Review of the Research in Japan. Int. J. Environ. Res. Public Health 2016, 13, 781. [Google Scholar] [CrossRef] [PubMed]
- Hug, S.M.; Hartig, T.; Hansmann, R.; Seeland, K.; Hornung, R. Restorative Qualities of Indoor and Outdoor Exercise Settings as Predictors of Exercise Frequency. Health Place 2009, 15, 971–980. [Google Scholar] [CrossRef] [PubMed]
- Fraser, M.; Munoz, S.A.; Macrury, S. Does the Mode of Exercise Influence the Benefits Obtained by Green Exercise? Int. J. Environ. Res. Public Health 2019, 16, 3004. [Google Scholar] [CrossRef]
- Richardson, E.A.; Mitchell, R. Gender Differences in Relationships between Urban Green Space and Health in the United Kingdom. Soc. Sci. Med. 2010, 71, 568–575. [Google Scholar] [CrossRef]
- Marselle, M.R.; Irvine, K.N.; Warber, S.L. Walking for Well-Being: Are Group Walks in Certain Types of Natural Environments Better for Well-Being than Group Walks in Urban Environments? Int. J. Environ. Res. Public Health 2013, 10, 5603. [Google Scholar] [CrossRef]


| Search terms | Category | |
|---|---|---|
| 1 | (green exercis* or green gym* or blue exercis* or blue gym* or ecotherap*).ti,ab. | Outdoor Exercise |
| 2 | (exercis* or physical activit* or walk* or physical fit* or run* or athlet*).ti,ab. | Exercise |
| 3 | (outdoor* or outside* or park* or greenspace* or green space* or bluespace* or blue space* or natural environment* or nature or forest* or biodivers* or horticultur*).ti,ab | Outdoors |
| 4 | (indoor* or inside* or laboratory or gym* or home* or buil*).ti,ab. | Indoors |
| 5 | 2 and 3 | |
| 6 | 1 or 5 | |
| 7 | 4 and 6 | |
| 8 | limit 7 to English language |
| PICOS | Inclusion Criteria |
|---|---|
| Population | No restrictions |
| Intervention | Two or more exercise bouts in an outdoor environment |
| Comparison | Two or more exercise bouts performed indoors with no exposure to actual or simulated nature |
| Outcome | Primary: at least one outcome related to physical or psychological health Secondary: any outcomes related to physical activity behaviour |
| Study design | Randomized or non-randomized trials |
| Term Related to Exercise Intensity | Operational Definition |
|---|---|
| Prescribe | Were participants instructed to exercise at a target intensity (either objective or subjective)? |
| Monitor | Did instructors measure exercise intensity (using either objective or subjective measures)? |
| Control or Regulate | Did instructors advise participants to maintain or adjust their intensity as necessary to match the target? |
| Measure/analyze as an outcome or as a control variable | Was intensity treated as an outcome (a dependent variable upon which the effect of the intervention is being investigated), as a control variable (intended to be equal to the prospectively defined target and equal in both groups), or inappropriately as both? |
| Outcome Category | Author, Year | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Abdel-Rahman et al., 2014 [33] | Anandh, Varadha-rajulu, & Alate, 2020 [34] | Calogiuri, Nordtug, & Weydahl, 2015 [Intervention] [27] | Calogiuri et al., 2016 [28] | Duranso, 2018 [32] | Irandoust & Taheri, 2017 [29] | Lacharité-Lemieux, Brunelle, & Dionne, 2015 [30] | Lacharité-Lemieux & Dionne, 2016 [31] | Miller et al., 2020 [17] | Moslehi, Moslehi, & Khalvati, 2019 [18] | Özbay et al., 2020 [19] | Zhou et al., 2020 [20] | |||
| PSYCHOLOGICAL | Affective Valence | NS 2/2 | ||||||||||||
| Positive Emotions | OE 1/2 | OE 2/3 | NS | |||||||||||
| NS 1/2 | NS 1/3 | |||||||||||||
| Depression | NS | NS | ||||||||||||
| Affective Activation | NS 2/2 | |||||||||||||
| Tranquility | NS 2/2 | OE | ||||||||||||
| Restoration | OE 2/2 | OE 2/2 | ||||||||||||
| Energy | NS | |||||||||||||
| Fatigue | NS | NS 2/2 | ||||||||||||
| Self-Efficacy and Self-Determination | NS | NS 2/2 | NS 3/3 | |||||||||||
| Motivation | NS 2/2 | OE 1/6 | ||||||||||||
| NS 5/6 | ||||||||||||||
| PHYSICAL | Anthro-pometric | Weight | NS | NS | OE | NS | ||||||||
| Body Composition | NS 3/3 | NS 6/6 | OE 2/2 | NS | ||||||||||
| Physio-logical | Systolic Blood Pressure | NS | NS | |||||||||||
| Diastolic Blood Pressure | OE | NS | ||||||||||||
| Plasma Lipids | NS 4/4 | OE 1/3 | ||||||||||||
| NS 2/3 | ||||||||||||||
| Glucose and Insulin Profile | NS 3/3 | |||||||||||||
| Hormones and Neuropeptides | OE 1/3 | OE | OE | NS 2/2 | ||||||||||
| NS 2/3 | ||||||||||||||
| Physical Fitness | Flexibility | OE | ||||||||||||
| Mobility | OE | OE 1/2 | OE 3/4 | |||||||||||
| NS 1/2 | NS 1/4 | |||||||||||||
| VO2max | NS | NS | ||||||||||||
| Muscle Strength | NS 3/3 | |||||||||||||
| Muscle Endurance | OE 1/3 | |||||||||||||
| NS 2/3 | ||||||||||||||
| Balance | NS 3/3 | |||||||||||||
| BEHAVIOUR | Future Exercise Intention | OE | ||||||||||||
| Physical Activity Level | OE 1/4 | NS | NS | |||||||||||
| NS 3/4 | ||||||||||||||
| Exercise Adherence | OE | |||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noseworthy, M.; Peddie, L.; Buckler, E.J.; Park, F.; Pham, M.; Pratt, S.; Singh, A.; Puterman, E.; Liu-Ambrose, T. The Effects of Outdoor versus Indoor Exercise on Psychological Health, Physical Health, and Physical Activity Behaviour: A Systematic Review of Longitudinal Trials. Int. J. Environ. Res. Public Health 2023, 20, 1669. https://doi.org/10.3390/ijerph20031669
Noseworthy M, Peddie L, Buckler EJ, Park F, Pham M, Pratt S, Singh A, Puterman E, Liu-Ambrose T. The Effects of Outdoor versus Indoor Exercise on Psychological Health, Physical Health, and Physical Activity Behaviour: A Systematic Review of Longitudinal Trials. International Journal of Environmental Research and Public Health. 2023; 20(3):1669. https://doi.org/10.3390/ijerph20031669
Chicago/Turabian StyleNoseworthy, Matt, Luke Peddie, E. Jean Buckler, Faith Park, Margaret Pham, Spencer Pratt, Arpreet Singh, Eli Puterman, and Teresa Liu-Ambrose. 2023. "The Effects of Outdoor versus Indoor Exercise on Psychological Health, Physical Health, and Physical Activity Behaviour: A Systematic Review of Longitudinal Trials" International Journal of Environmental Research and Public Health 20, no. 3: 1669. https://doi.org/10.3390/ijerph20031669
APA StyleNoseworthy, M., Peddie, L., Buckler, E. J., Park, F., Pham, M., Pratt, S., Singh, A., Puterman, E., & Liu-Ambrose, T. (2023). The Effects of Outdoor versus Indoor Exercise on Psychological Health, Physical Health, and Physical Activity Behaviour: A Systematic Review of Longitudinal Trials. International Journal of Environmental Research and Public Health, 20(3), 1669. https://doi.org/10.3390/ijerph20031669