
Physiotherapy-Led Health Promotion Strategies for People with or at Risk of Cardiovascular Diseases: A Scoping Review

Abstract
:1. Introduction
- To assess the characteristics of existing evidence on PLHP for pwCVDs globally.
- To identify the interventional approaches that have been used in PLHP strategies for pwCVDs.
- To evaluate the type of population groups included in the PLHP research.
2. Methodology
2.1. Identifying the Research Question
2.2. Identifying Relevant Studies (Database and Search Strategy)
2.3. Eligibility Criteria
2.4. Study Selection (Screening)
2.5. Data Charting (Data Extraction)
2.6. Quality Appraisal
2.7. Consultation
2.8. Collating, Summarising, and Reporting
3. Results
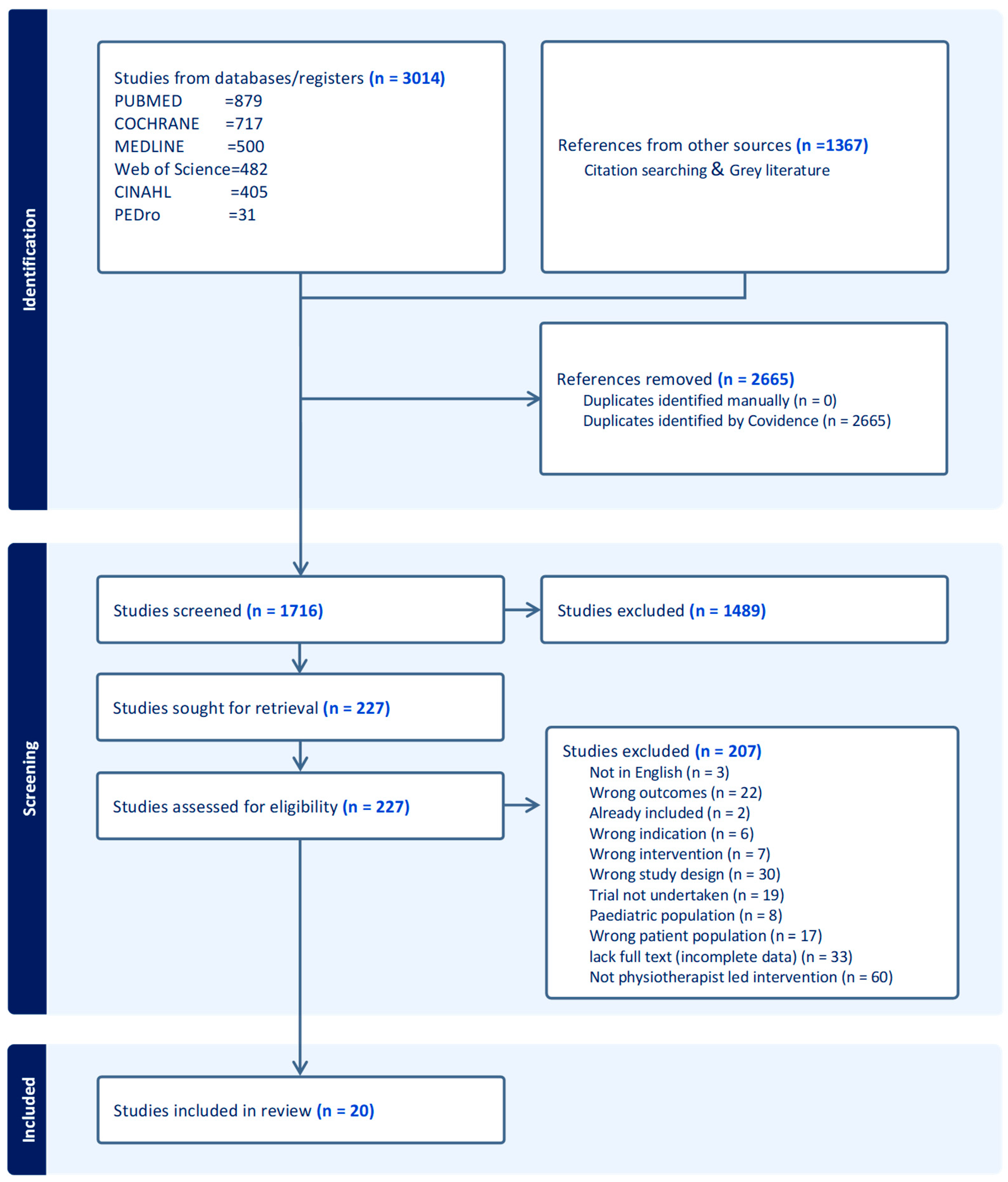
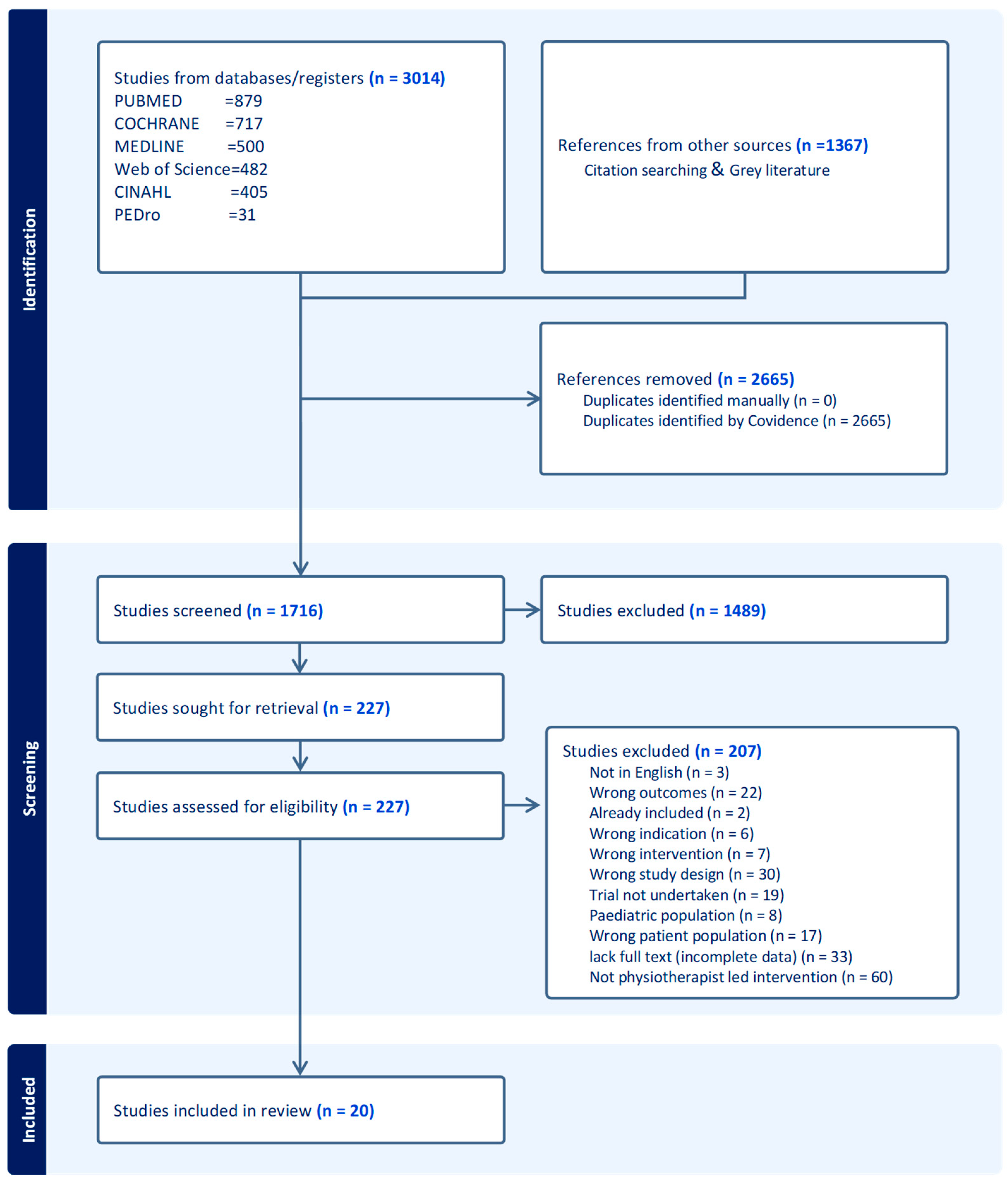
3.1. Literature Search and Included Studies
3.2. Characteristics of Included Studies
3.3. Characteristics of the Included Interventions

{kind=link}
| Overall Aim of Intervention | Education on Lifestyle | Dietary Education and Physiotherapy | Exercise and/or Physical Activity | Self-Management and Home Programmes | Behaviour Change Programmes on Physical Activity Uptake | Individualised Coaching on Physical Activity and Exercise | Health Improvement Card (HIC) | Provision of Educational Materials/Resources Such as Brochures on Healthy Lifestyle Practices and Lifestyle Behaviour Change | Workbook | Written Instructions and Recommendations | Handouts Following Each Session | Technology Based | Theory-Based Intervention | Supplemented by Telephone Calls | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fowler et al., 2002 [45] | Improving maximum walking distance in early peripheral arterial disease | ✓ | ✓ | ✓ | |||||||||||
| Bonet et al., 2003 [46] | Evaluate, in women with grade 1 essential hypertension, the response of cardio-respiratory and blood pressure after 6 weeks of supervised physical exercise vs. only recommended exercise | ✓ | ✓ | ||||||||||||
| Eriksson et al., 2006 [47] | Lifestyle intervention programme in primary healthcare | ✓ | ✓ | ✓ | |||||||||||
| Quinn et al., 2008 [61] | The effect of a physical activity group-based education programme on weight reduction, physical activity, cardiovascular fitness, quality of life | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||
| Pariser et al., 2010 [60] | Active Steps for Diabetes | ✓ | ✓ | ✓ | ✓ | ||||||||||
| Wisse et al., 2010 [48] | Assess the impact of personalized exercise prescription on habitual physical activity and glycemic control in sedentary, insulin treated type 2 diabetes patients | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||
| Molenaar et al., 2010 [49] | Nutritional counselling and nutritional plus exercise counselling in overweight adults | ✓ | ✓ | ✓ | ✓ | ||||||||||
| Wu et al., 2011 [50] | Evaluate short- and long-term effects of home-based exercise on adiponectin, exercise behaviour and metabolic risk factors in middle-aged adults at diabetic risk | ✓ | ✓ | ✓ | |||||||||||
| Reid et al., 2012 [51] | Evaluate long-term physical activity levels between a theoretically guided motivational counselling (MC) intervention group and a usual care | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||
| Oerkild et al., 2012 [52] | Home-based cardiac rehabilitation | ✓ | ✓ | ✓ | ✓ | ||||||||||
| Takatori et al., 2012 [53] | Investigate the effect of intensive rehabilitation on physical and arterial function among community-dwelling stroke survivors | ✓ | ✓ | ||||||||||||
| Preston et al., 2016 [57] | Improving self-management | ✓ | ✓ | ||||||||||||
| Higgs et al., 2016 [59] | Acceptability of a community-based lifestyle programme for adults with diabetes/prediabetes | ✓ | ✓ | ✓ | |||||||||||
| Gunnes et al., 2018 [58] | To investigate adherence to an 18-month physical activity and exercise programme | ✓ | ✓ | ✓ | ✓ | ||||||||||
| Gunnes et al., 2019 [64] | To assess the associations between participants’ degree of adherence to physical activity and exercise and motor function 18 months after inclusion | ✓ | ✓ | ✓ | |||||||||||
| Bai et al., 2020 [54] | Health improvement card (HIC) on lifestyle practices and biometric variables in community-dwelling Chinese participants | ✓ | ✓ | ✓ | |||||||||||
| Gerage et al., 2020 [55] | To investigate the efficacy of a behaviour change programme on cardiovascular parameters in hypertensive patients | ✓ | ✓ | ✓ | ✓ | ||||||||||
| Batsis et al., 2021 [62] | Technology-based weight management intervention for rural older adults with obesity | ✓ | ✓ | ✓ | ✓ | ||||||||||
| Bearne et al., 2022 [56] | The effect of a home-based, walking exercise behaviour change intervention in adults with peripheral arterial disease and intermittent claudication | ✓ | ✓ | ✓ | |||||||||||
| Deka et al., 2022 [63] | The effectiveness of a dietary-education and high-intensity interval resistance training programme on healthy food choices and associated anthropometric variables | ✓ | ✓ | ✓ | ✓ |
| Author Year | Country | N | Study Design | Population | Nature of the Intervention | Intervention Duration | Theory Use | Mode of, and Delivered by | Setting(s) | Educational Component | Delivery Format | Number of Sessions | Technology | Tailoring | Fidelity |
| Fowler et al., 2002 [45] | Australia | 882 | RCT | Males aged 65 to 79 years with PAD | Individual and community intervention, advised participants to walk >30 min daily | Short (12 months) | No | Educational materials and f-t-f by PT | Combined | Yes | Combined | High | No | Yes | No |
| Bone et al., 2003 [46] | Spain | 18 | RCT | Overweight women of 30–50 years with grade 1 hypertension | Supervised physical exercise | Short (6 months) | No | Educational materials and f-t-f by PT | Combined | No | Group | High | No | Yes | No |
| Eriksson et al., 2006 [47] | Sweden | 151 | Randomised controlled parallel group trial | Patients diagnosed with hypertension, dyslipidaemia, type 2 diabetes, obesity, or any combination thereof are aged 18–65 | Lifestyle intervention in primary healthcare | Short (3 months) | No | f-t-f by PT and assistants, dietician and a physician | Clinic | Yes | Group | High | No | Yes | No |
| Quinn et al., 2007 [61] | Ireland | 18 | Pre-post-test design | Obese females | Physical activity education | Short (4 months) | No | f-t-f by PT | Clinic | Yes | Individual | Low | No | No | No |
| Pariser et al., 2010 [60] | USA | 22 | Pre-post-test design | Type 2 Diabetes patients with impaired mobility issues | Active steps for diabetes (exercise and educational intervention) | Short (2 months) | No | f-t-f by PT (assisted by PT student or nurse/diabetes educator) | Combined | No | Combined | High | Yes | Yes | No |
| Wisse et al., 2010 [48] | The Netherlands | 74 | RCT | Sedentary, insulin-treated type 2 diabetes | Regular, structured, and personalised exercise prescription | Long (24 months) | No | f-t-f by PT supplemented with telephone calls | Combined | Yes | Individual | Low | Yes | Yes | No |
| Molenaar et al., 2010 [49] | The Netherlands | 203 | RCT | Men and non-pregnant women aged 18–65 years with a BMI of 28–35 kg/m2 | Nutritional counselling and nutritional plus exercise counselling in overweight adults. | long (13.7 months) | No | f-t-f by Dietician and PT | Clinic | Yes | Individual | Low | No | Yes | Yes |
| Wu et al., 2011 [50] | Taiwan | 135 | RCT | People 45 to 64 years old are at risk of developing diabetes | Home-based exercise | Short (6 months) | Yes | f-t-f supplemented with telephone calls by PT | Community | Yes | Individual | High | Yes | Yes | Yes |
| Reid et al., 2011 [51] | Canada | 141 | RCT | Patients with acute coronary syndromes | Motivational counselling intervention | Short (12 months) | Yes | f-t-f supplemented by telephone calls | Combined | Yes | Individual | Low | Yes | Yes | Yes |
| Oerkild et al., 2012 [52] | Denmark | 40 | RCT | Elderly coronary heart disease above 65 years | Cardiac home programme for the elderly | Short (12 months) | No | home visits in person, follow-up with telephone calls by PT | Community | Yes | Individual | Low | Yes | Yes | No |
| Takatori et al., 2012 [53] | Japan | 44 | RCT | Chronic stroke survivors 57–89 years | Exercise therapy | Short (3 monhs) | No | f-t-f by PT | Clinic | No | Individual | High | No | Yes | No |
| Higgs et al., 2016 [59] | New Zealand | 36 | Prospective observational | Diabetic or at a high risk of developing diabetes | Education and exercise | Short (3 months) | No | f-t-f by PT, PT students and a nurse. | Clinic | Yes | Individual | High | No | Yes | Yes |
| Preston et al., 2017 [57] | Australia | 20 | pre-post-test intervention | Patients with mild to moderate acute stroke | Self-management | Short (3 months) | No | f-t-f by PT | Community | Yes | Individual | Low | No | Yes | Yes |
| Gunnes et al., 2018 [58] | Norway | 186 | Prospective longitudinal | Adult stroke patients | Physical activity and exercise programme | Long (18 months) | Yes (MI) | f-t-f and over the phone by PT | Community | Yes | Individual | High | Yes | Yes | Yes |
| Gunnes et al., 2019 [64] | Norway | 186 | Secondary analyses of multisite RCT | Stroke patients | Individualised coaching on physical activity and exercise | Long (18 months) | Yes (MI) | f-t-f supplemented by telephone calls by PT | Clinic | Yes | Individual | High | Yes | Yes | Yes |
| Bai et al., 2020 [54] | China | 200 | RCT | 50–90 years | Health education based on the HIC, individualised exercise programme. Standard brochure on healthy lifestyle practices | Short (3 months) | Yes (HIC) | f-t-f by PT students supervised by PT. | Community | Yes | Individual | Low | No | Yes | No |
| Gerage et al., 2020 [55] | Brazil | 90 | RCT | Patients with primary hypertension | Behavioural change programme supplemented with educational materials | Short (3 months) | Yes (VAMOS) | f-t-f by PT | Clinic | Yes | Group | Low | No | No | No |
| Batsis et al., 2021 [62] | USA | 54 | Single-arm trial | Older (65+) adults with obesity (BMI > 30 kg/m2) residing in rural New Hampshire and Vermont | Technology-based weight management intervention | Short (6 months) | Yes (social cognitive theory, MI) | f-t-f and telemedicine (video conferencing, remote use of Fitbit) and periodic face-to-face interaction onsite. By dietitian and PT | Community | Yes | Combined | High | Yes | Yes | Yes |
| Bearne et al., 2022 [56] | England | 190 | RCT | Adults with peripheral arterial disease and intermittent claudication | Walking Exercise Behaviour Change Intervention | Short (6 months) | Yes (theory of planned behaviour and the common sense model of illness representation) | f-t-f and supplemented by telephone calls by PT | Clinic | Yes | Individual | Low | Yes | Yes | Yes |
| Deka et al., 2022 [63] | Spain | 22 | Single-arm trial | Patients with coronary artery diseases | Dietary education and a high-intensity interval resistance training programme (DE–HIIRT) | Short (3 months) | Yes (Bandura’ self-efficacy theory) | f-t-f by dietician and PT | Clinic | Yes | Combined | 22 | No | Yes | Yes |
4. Discussion
4.1. Implications for Clinical Practice
4.2. Research Implications
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Medline Search Strings
References
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practiceThe Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef]
- Non Communicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 19 July 2021).
- Tulu, S.N.; Al Salmi, N.; Jones, J. Understanding cardiovascular disease in day-to-day living for African people: A qualitative metasynthesis. BMC Public Health 2021, 21, 745. [Google Scholar] [CrossRef] [PubMed]
- Cardiovascular Diseases (CVDs). Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 21 November 2021).
- Gaziano, T.A. Reducing the Growing Burden of Cardiovascular Disease in The Developing World. Health Aff. 2007, 26, 13–24. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.J.; Chin, S.L.; Rangarajan, S.; Xavier, D.; Liu, L.; Zhang, H.; Rao-Melacini, P.; Zhang, X.; Pais, P.; Agapay, S.; et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): A case-control study. Lancet 2016, 388, 761–775. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Roth, G.A.; Naghavi, M.; Parmar, P.; Krishnamurthi, R.; Chugh, S.; Mensah, G.A.; Norrving, B.; Shiue, I.; Ng, M.; et al. Global burden of stroke and risk factors in 188 countries, during 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet Neurol. 2016, 15, 913–924. [Google Scholar] [CrossRef] [PubMed]
- Strong, K.; Mathers, C.; Bonita, R. Preventing stroke: Saving lives around the world. Lancet Neurol. 2007, 6, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Mohan, K.M.; Wolfe, C.D.A.; Rudd, A.G.; Heuschmann, P.U.; Kolominsky-Rabas, P.L.; Grieve, A.P. Risk and Cumulative Risk of Stroke Recurrence: A Systematic Review and Meta-Analysis. Stroke 2011, 42, 1489–1494. [Google Scholar] [CrossRef] [PubMed]
- Dhamoon, M.S.; Sciacca, R.R.; Rundek, T.; Sacco, R.L.; Elkind, M.S.V. Recurrent stroke and cardiac risks after first ischemic stroke: The Northern Manhattan Study. Neurology 2006, 66, 641–646. [Google Scholar] [CrossRef]
- Ruan, Y.; Guo, Y.; Zheng, Y.; Huang, Z.; Sun, S.; Kowal, P.; Shi, Y.; Wu, F. Cardiovascular disease (CVD) and associated risk factors among older adults in six low-and middle-income countries: Results from SAGE Wave 1. BMC Public Health 2018, 18, 778. [Google Scholar] [CrossRef]
- Yusuf, S.; Hawken, S.; Ôunpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Bigna, J.J.; Noubiap, J.J. The rising burden of non-communicable diseases in sub-Saharan Africa. Lancet Glob. Health 2019, 7, e1295–e1296. [Google Scholar] [CrossRef] [PubMed]
- Bowry, A.D.K.; Lewey, J.; Dugani, S.B.; Choudhry, N.K. The Burden of Cardiovascular Disease in Low- and Middle-Income Countries: Epidemiology and Management. Can. J. Cardiol. 2015, 31, 1151–1159. [Google Scholar] [CrossRef] [PubMed]
- 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease—American College of Cardiology. Available online: https://www.acc.org/latest-in-cardiology/ten-points-to-remember/2019/03/07/16/00/2019-acc-aha-guideline-on-primary-prevention-gl-prevention (accessed on 15 August 2020).
- Li, D.; Jia, Y.; Yu, J.; Liu, Y.; Li, F.; Liu, Y.; Wu, Q.; Liao, X.; Zeng, Z.; Wan, Z.; et al. Adherence to a Healthy Lifestyle and the Risk of All-Cause Mortality and Cardiovascular Events in Individuals with Diabetes: The ARIC Study. Front. Nutr. 2021, 8, 698608. [Google Scholar] [CrossRef] [PubMed]
- Schuett, K.A.; Lehrke, M.; Marx, N.; Burgmaier, M. High-Risk Cardiovascular Patients: Clinical Features, Comorbidities, and Interconnecting Mechanisms. Front. Immunol. 2015, 6, 591. [Google Scholar] [CrossRef] [PubMed]
- Bellmann, B.; Lin, T.; Greissinger, K.; Rottner, L.; Rillig, A.; Zimmerling, S. The Beneficial Effects of Cardiac Rehabilitation. Cardiol. Ther. 2020, 9, 35–44. [Google Scholar] [CrossRef]
- Dietary Restrictions and Nutrition in the Prevention and Treatment of Cardiovascular Disease|Circulation Research. Available online: https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.118.313352 (accessed on 1 August 2021).
- Darden, D.; Richardson, C.; Jackson, E.A. Physical Activity and Exercise for Secondary Prevention among Patients with Cardiovascular Disease. Curr. Cardiovasc. Risk Rep. 2013, 7, 411–416. [Google Scholar] [CrossRef]
- Smyth, A.; Teo, K.K.; Rangarajan, S.; O’Donnell, M.; Zhang, X.; Rana, P.; Leong, D.P.; Dagenais, G.; Seron, P.; Rosengren, A.; et al. Alcohol consumption and cardiovascular disease, cancer, injury, admission to hospital, and mortality: A prospective cohort study. Lancet 2015, 386, 1945–1954. [Google Scholar] [CrossRef]
- Tobacco Smoking and Risk of 36 Cardiovascular Disease Subtypes: Fatal and Non-Fatal Outcomes in a Large Prospective Australian Study|BMC Medicine|Full Text. Available online: https://bmcmedicine.biomedcentral.com/articles/10.1186/s12916-019-1351-4 (accessed on 1 August 2021).
- Nagai, M.; Hoshide, S.; Kario, K. Sleep Duration as a Risk Factor for Cardiovascular Disease—A Review of the Recent Literature. CCR 2010, 6, 54–61. [Google Scholar] [CrossRef]
- Gomes, M.J.; Pagan, L.U.; Okoshi, M.P. Non-Pharmacological Treatment of Cardiovascular Disease|Importance of Physical Exercise. Arq. Bras. Cardiol. 2019, 113, 9–10. [Google Scholar] [CrossRef]
- How Is Stress and Heart Disease Related?—Cleveland Clinic. Available online: https://health.clevelandclinic.org/how-is-stress-and-heart-disease-related/ (accessed on 1 August 2021).
- Kisling, L.A.; Das, J.M. Prevention Strategies. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: http://www.ncbi.nlm.nih.gov/books/NBK537222/ (accessed on 10 August 2021).
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease. J. Am. Coll. Cardiol. 2019, 74, e177–e232. [Google Scholar] [CrossRef]
- Lowe, A.; Gee, M.; McLean, S.; Littlewood, C.; Lindsay, C.; Everett, S. Physical activity promotion in physiotherapy practice: A systematic scoping review of a decade of literature. Br. J. Sports Med. 2018, 52, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Korn, L.; Ben-Ami, N.; Azmon, M.; Einstein, O.; Lotan, M. Evaluating the Effectiveness of a Health Promotion Intervention Program Among Physiotherapy Undergraduate Students. Med. Sci. Monit. 2017, 23, 3518–3527. [Google Scholar] [CrossRef] [PubMed]
- Maguire, A. Physiotherapy and Cardiovascular Disease: What Can It Do to Help? Ballsbridge Physiotherapy Clinic. 2015. Available online: https://ballsbridgephysio.ie/news/physiotherapy-and-cardiovascular-disease-what-can-it-do-to-help/ (accessed on 10 August 2021).
- Turk-Adawi, K.; Supervia, M.; Lopez-Jimenez, F.; Pesah, E.; Ding, R.; Britto, R.R.; Bjarnason-Wehrens, B.; Derman, W.; Abreu, A.; Babu, A.S.; et al. Cardiac Rehabilitation Availability and Density around the Globe. EClinicalMedicine 2019, 13, 31–45. [Google Scholar] [CrossRef]
- Ragupathi, L.; Stribling, J.; Yakunina, Y.; Fuster, V.; McLaughlin, M.A.; Vedanthan, R. Availability, Use, and Barriers to Cardiac Rehabilitation in LMIC. Glob. Heart 2017, 12, 323. [Google Scholar] [CrossRef] [PubMed]
- Gimigliano, F.; Negrini, S. The World Health Organization “Rehabilitation 2030: A call for action”. Eur. J. Phys. Rehabil. Med. 2017, 53, 155–168. [Google Scholar] [CrossRef] [PubMed]
- Bäck, M.; Öberg, B.; Krevers, B. Important aspects in relation to patients’ attendance at exercise-based cardiac rehabilitation—Facilitators, barriers and physiotherapist’s role: A qualitative study. BMC Cardiovasc. Disord. 2017, 17, 77. [Google Scholar] [CrossRef] [PubMed]
- Alexander, J.; Bambury, E.; Mendoza, A.; Reynolds, J.; Veronneau, R.; Dean, E. Health education strategies used by physical therapists to promote behaviour change in people with lifestyle-related conditions: A systematic review. Hong Kong Physiother. J. 2012, 30, 57–75. [Google Scholar] [CrossRef]
- Kunstler, B.E.; Cook, J.L.; Freene, N.; Finch, C.F.; Kemp, J.L.; O’Halloran, P.D.; Gaida, J.E. Physiotherapists use a small number of behaviour change techniques when promoting physical activity: A systematic review comparing experimental and observational studies. J. Sci. Med. Sport 2018, 21, 609–615. [Google Scholar] [CrossRef]
- Cox, N.S.; Alison, J.A.; Holland, A.E. Interventions for promoting physical activity in people with cystic fibrosis. Cochrane Database Syst. Rev. 2013, 2022, CD009448. [Google Scholar] [CrossRef]
- Lockwood, C.; Dos Santos, K.B.; Pap, R. Practical Guidance for Knowledge Synthesis: Scoping Review Methods. Asian Nurs. Res. 2019, 13, 287–294. [Google Scholar] [CrossRef]
- Munn, Z.; Stern, C.; Aromataris, E.; Lockwood, C.; Jordan, Z. What kind of systematic review should I conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med. Res. Methodol. 2018, 18, 5. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Social. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Implement. 2021, 19, 3–10. [Google Scholar] [CrossRef]
- Daudt, H.M.; van Mossel, C.; Scott, S.J. Enhancing the scoping study methodology: A large, inter-professional team’s experience with Arksey and O’Malley’s framework. BMC Med. Res. Methodol. 2013, 13, 48. [Google Scholar] [CrossRef]
- Fowler, B.; Jamrozik, K.; Norman, P.; Allen, Y.; Wilkinson, E. Improving maximum walking distance in early peripheral arterial disease: Randomised controlled trial. Aust. J. Physiother. 2002, 48, 269–275. [Google Scholar] [CrossRef]
- Bonet, J.; Coll, R.; Rocha, E.; Romero, R. Supervised versus recommended physical exercise in hypertensive women. Is its recommendation enough? Blood Press. 2003, 12, 139–144. [Google Scholar] [CrossRef]
- Eriksson, K.M.; Westborg, C.; Eliasson, M.C.E. A randomized trial of lifestyle intervention in primary healthcare for the modification of cardiovascular risk factors. Scand. J. Public. Health 2006, 34, 453–461. [Google Scholar] [CrossRef]
- Wisse, W.; Boer Rookhuizen, M.; de Kruif, M.D.; van Rossum, J.; Jordans, I.; ten Cate, H.; van Loon, L.J.C.; Meesters, E.W. Prescription of physical activity is not sufficient to change sedentary behavior and improve glycemic control in type 2 diabetes patients. Diabetes Res. Clin. Pract. 2010, 88, e10–e13. [Google Scholar] [CrossRef]
- Molenaar, E.A.; van Ameijden, E.J.C.; Vergouwe, Y.; Grobbee, D.E.; Numans, M.E. Effect of nutritional counselling and nutritional plus exercise counselling in overweight adults: A randomized trial in multidisciplinary primary care practice. Fam. Pract. 2010, 27, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-T.; Hwang, C.-L.; Chen, C.-N.; Chuang, L.-M. Home-based exercise improves exercise behavior and metabolic risk factors in middle-aged adults at diabetic risk. Physiotherapy 2011, 97, eS523. [Google Scholar] [CrossRef]
- Reid, R.D.; Morrin, L.I.; Higginson, L.A.J.; Wielgosz, A.; Blanchard, C.; Beaton, L.J.; Nelson, C.; McDonnell, L.; Oldridge, N.; Wells, G.A.; et al. Motivational counselling for physical activity in patients with coronary artery disease not participating in cardiac rehabilitation. Eur. J. Prev. Cardiol. 2012, 19, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Oerkild, B.; Frederiksen, M.; Hansen, J.F.; Prescott, E. Home-based cardiac rehabilitation is an attractive alternative to no cardiac rehabilitation for elderly patients with coronary heart disease: Results from a randomised clinical trial. BMJ Open 2012, 2, e001820. [Google Scholar] [CrossRef] [PubMed]
- Takatori, K.; Matsumoto, D.; Okada, Y.; Nakamura, J.; Shomoto, K. Effect of intensive rehabilitation on physical function and arterial function in community-dwelling chronic stroke survivors. Top. Stroke Rehabil. 2012, 19, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Wu, X.; Tsang, R.C.; Yun, R.; Lu, Y.; Dean, E.; Jones, A.Y. A Randomised Controlled Trial to Evaluate the Administration of the Health Improvement Card as a Health Promotion Tool: A Physiotherapist-Led Community-Based Initiative. Int. J. Environ. Res. Public Health 2020, 17, 8065. [Google Scholar] [CrossRef]
- Gerage, A.M.; Benedetti, T.R.B.; Cavalcante, B.R.; Farah, B.Q.; Ritti-Dias, R.M. Efficacy of a behavior change program on cardiovascular parameters in patients with hypertension: A randomized controlled trial. Einstein 2020, 18, eAO5227. [Google Scholar] [CrossRef]
- Bearne, L.M.; Volkmer, B.; Peacock, J.; Sekhon, M.; Fisher, G.; Galea Holmes, M.N.; Douiri, A.; Amirova, A.; Farran, D.; Quirke-McFarlane, S.; et al. Effect of a Home-Based, Walking Exercise Behavior Change Intervention vs Usual Care on Walking in Adults with Peripheral Artery Disease: The MOSAIC Randomized Clinical Trial. JAMA 2022, 327, 1344–1355. [Google Scholar] [CrossRef]
- Preston, E.; Dean, C.M.; Ada, L.; Stanton, R.; Brauer, S.; Kuys, S.; Waddington, G. Promoting physical activity after stroke via self-management: A feasibility study. Top. Stroke Rehabil. 2017, 24, 353–360. [Google Scholar] [CrossRef]
- Gunnes, M.; Langhammer, B.; Aamot, I.-L.; Lydersen, S.; Ihle-Hansen, H.; Indredavik, B.; Reneflot, K.H.; Schroeter, W.; Askim, T.; LAST Collaboration group. Adherence to a Long-Term Physical Activity and Exercise Program After Stroke Applied in a Randomized Controlled Trial. Phys. Ther. 2019, 99, 74–85. [Google Scholar] [CrossRef]
- Higgs, C.; Skinner, M.; Hale, L. Outcomes of a community-based lifestyle programme for adults with diabetes or pre-diabetes. J. Prim. Health Care 2016, 8, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Pariser, G.; Ann Demeuro, M.; Gillette, P.; Stephen, W. Outcomes of an Education and Exercise Program for Adults with Type 2 Diabetes, and Comorbidities that Limit their Mobility: A Preliminary Project Report. Cardiopulm. Phys. Ther. J. 2010, 21, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Quinn, A.; Doody, C.; O’Shea, D. The effect of a physical activity education programme on physical activity, fitness, quality of life and attitudes to exercise in obese females. J. Sci. Med. Sport 2008, 11, 469–472. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Petersen, C.L.; Clark, M.M.; Cook, S.B.; Lopez-Jimenez, F.; Al-Nimr, R.I.; Pidgeon, D.; Kotz, D.; Mackenzie, T.A.; Bartels, S.J. A Weight Loss Intervention Augmented by a Wearable Device in Rural Older Adults with Obesity: A Feasibility Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2021, 76, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Deka, P.; Blesa, J.; Pathak, D.; Sempere-Rubio, N.; Iglesias, P.; Micó, L.; Soriano, J.M.; Klompstra, L.; Marques-Sule, E. Combined Dietary Education and High-Intensity Interval Resistance Training Improve Health Outcomes in Patients with Coronary Artery Disease. Int. J. Environ. Res. Public Health 2022, 19, 1402. [Google Scholar] [CrossRef]
- Gunnes, M.; Indredavik, B.; Langhammer, B.; Lydersen, S.; Ihle-Hansen, H.; Dahl, A.E.; Askim, T. Associations Between Adherence to the Physical A ctivity and Exercise Program Applied in the LAST Study and Functional Recovery After Stroke. Arch. Phys. Med. Rehabil. 2019, 100, 2251–2259. [Google Scholar] [CrossRef]
- Dean, E. Physical therapy in the 21st century (Part I): Toward practice informed by epidemiology and the crisis of lifestyle conditions. Physiother. Theory Pract. 2009, 25, 330–353. [Google Scholar] [CrossRef]
- Dean, E.; Skinner, M.; Myezwa, H.; Mkumbuzi, V.; Mostert, K.; Parra, D.C.; Shirley, D.; Söderlund, A.; de Andrade, A.D.; Abaraogu, U.O.; et al. Health Competency Standards in Physical Therapist Practice. Phys. Ther. 2019, 99, 1242–1254. [Google Scholar] [CrossRef]
- Dean, E.; Creig, A.; Murphy, S.; Roots, R.; Nembhard, N.; Rankin, A.; Bainbridge, L.; Anthony, J.; Hoens, A.M.; Garland, S.J. Raising the Priority of Lifestyle-Related Noncommunicable Diseases in Physical Therapy Curricula. Phys. Ther. 2016, 96, 940–948. [Google Scholar] [CrossRef]
- Anand, S.; Bradshaw, C.; Prabhakaran, D. Prevention and management of CVD in LMICs: Why do ethnicity, culture, and context matter? BMC Med. 2020, 18, 7. [Google Scholar] [CrossRef]
- Minja, N.W.; Nakagaayi, D.; Aliku, T.; Zhang, W.; Ssinabulya, I.; Nabaale, J.; Amutuhaire, W.; De Loizaga, S.R.; Ndagire, E.; Rwebembera, J.; et al. Cardiovascular diseases in Africa in the twenty-first century: Gaps and priorities going forward. Front. Cardiovasc. Med. 2022, 9, 1008335. [Google Scholar] [CrossRef] [PubMed]
- Dzudie, A.; Rayner, B.; Ojji, D.; Schutte, A.E.; Twagirumukiza, M.; Damasceno, A.; Ba, S.A.; Kane, A.; Kramoh, E.; Kacou, J.B.A.; et al. Roadmap to achieve 25% hypertension control in Africa by 2025. CVJA 2017, 28, 261–272. [Google Scholar] [CrossRef]
- Ngeh, E.N. Research among undergraduate biomedical students in Cameroon: Contextual barriers, room for improvement. Pan Afr. Med. J. 2019, 33, 149. [Google Scholar] [CrossRef] [PubMed]
- Ngeh Ngeh, E.; Chigbo, N.N.; Whitehouse, Z.; Anekwu, E.M.; Mukaruzima, L.M.; Mtsetfwa, L.; Kitur, R.; Agoriwo, M.W.; Ondogah, P.; Douryang, M.; et al. A report on the development of COVID-19 guidelines for rehabilitation professionals in African settings. Pan Afr. Med. J. 2021, 38, 129. [Google Scholar] [CrossRef] [PubMed]
- Bennell, K.L.; Lawford, B.J.; Keating, C.; Brown, C.; Kasza, J.; Mackenzie, D.; Metcalf, B.; Kimp, A.J.; Egerton, T.; Spiers, L.; et al. Comparing Video-Based, Telehealth-Delivered Exercise and Weight Loss Programs with Online Education on Outcomes of Knee Osteoarthritis: A Randomized Trial. Ann. Intern. Med. 2022, 175, 198–209. [Google Scholar] [CrossRef] [PubMed]
| Participants/Population | Concept/Intervention |
|---|---|
| Cardiovascular disease and risk factors block keywords, cardiovascular diseases, heart diseases, coronary artery disease, coronary heart disease, myocardial infarction, heart failure, angina, cerebrovascular disease, stroke patients, and aortic atherosclerosis patients—overweight, obesity, diabetes, blood pressure, hypertension, dyslipidaemia. | Physiotherapy block keywords: Physiotherapist(s), physiotherapy, kinesiotherapy, physical therapist(s), physiotherapy assistant. Health promotion block keywords: Patient education, health promotion, health education, health behaviour, educational technology, diet therapy, educational health promotion, group-based, individual, home and hospital-based approaches, lifestyle modification, lifestyle change recommendations, physical activity and exercise promotion, brief counselling, face to face, group sessions, skill training, visual presentation, handouts, brochures and diaries, motivational prompts, individualised plan, goal setting, nutrition and weight management, smoking cessation, tobacco exposure, sleep, stress management. |
| Participants/Population | Concept/Intervention | Context | Study Types and Design |
|---|---|---|---|
| Inclusion Criteria | |||
|
|
|
|
| Exclusion Criteria | |||
| Studies on pwCVD with relevant outcomes were initiated and implemented by clinicians other than physiotherapists. |
|
| |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ngeh, E.N.; Lowe, A.; Garcia, C.; McLean, S. Physiotherapy-Led Health Promotion Strategies for People with or at Risk of Cardiovascular Diseases: A Scoping Review. Int. J. Environ. Res. Public Health 2023, 20, 7073. https://doi.org/10.3390/ijerph20227073
Ngeh EN, Lowe A, Garcia C, McLean S. Physiotherapy-Led Health Promotion Strategies for People with or at Risk of Cardiovascular Diseases: A Scoping Review. International Journal of Environmental Research and Public Health. 2023; 20(22):7073. https://doi.org/10.3390/ijerph20227073
Chicago/Turabian StyleNgeh, Etienne Ngeh, Anna Lowe, Carol Garcia, and Sionnadh McLean. 2023. "Physiotherapy-Led Health Promotion Strategies for People with or at Risk of Cardiovascular Diseases: A Scoping Review" International Journal of Environmental Research and Public Health 20, no. 22: 7073. https://doi.org/10.3390/ijerph20227073
APA StyleNgeh, E. N., Lowe, A., Garcia, C., & McLean, S. (2023). Physiotherapy-Led Health Promotion Strategies for People with or at Risk of Cardiovascular Diseases: A Scoping Review. International Journal of Environmental Research and Public Health, 20(22), 7073. https://doi.org/10.3390/ijerph20227073