

Beyond Information Provision: Analysis of the Roles of Structure and Agency in COVID-19 Vaccine Confidence in Ethnic Minority Communities

 , , ,
, , ,
Abstract
:1. Introduction
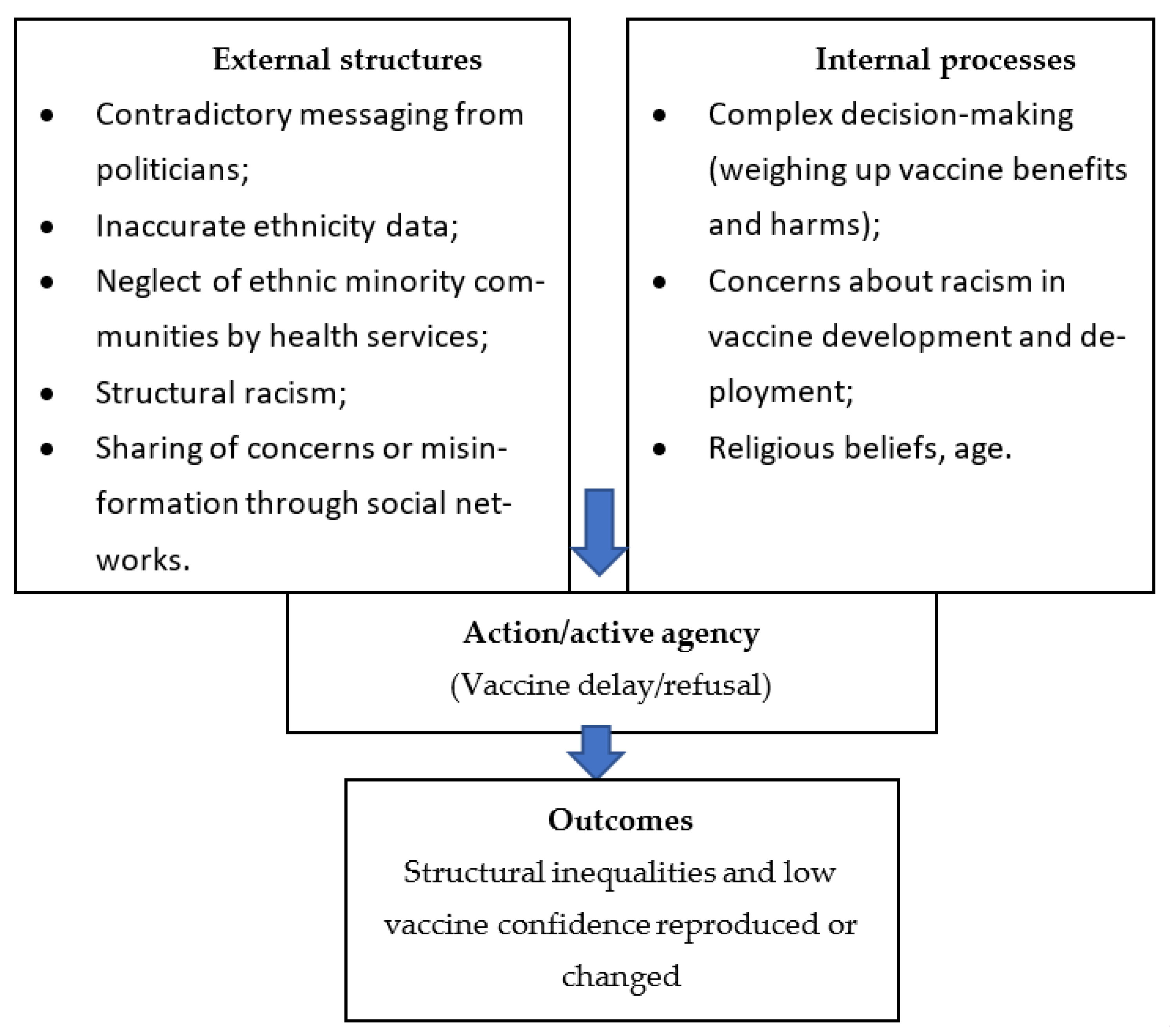
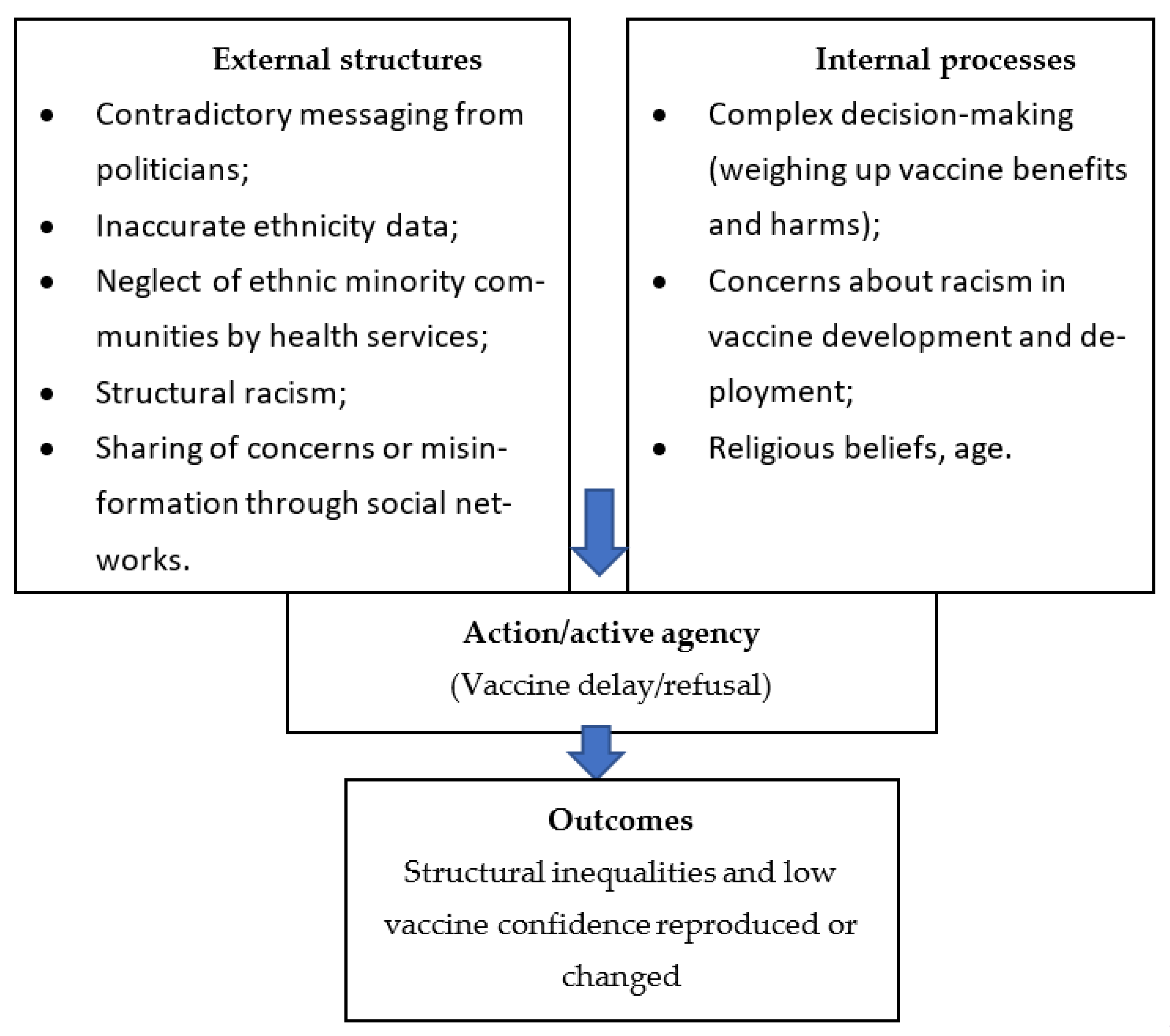
1.1. Theoretical Underpinnings
1.2. Aim and Objectives
- Explore which structural factors influence decision-making, including external structures (education, employment, income, social identity, positioning and networks and experiences of structural racism) and internal structures (morals, values, attitudes and knowledge);
- Explore actions that would enable primary care and public health campaigns to improve confidence in COVID-19 vaccination in ethnic minority groups.
2. Materials and Methods
2.1. Study Design
2.2. Study Setting
2.3. Patient and Public Involvement (PPI)
2.4. Sampling and Recruitment
2.5. Data Collection and Analysis
3. Results
3.1. Participants
3.2. First-Level Analysis
- Lack of information credibility and clarity;
- Discrimination and barriers to healthcare;
- Personal beliefs, characteristics and experiences influencing vaccine choice;
- Social networks and community cohesion.
3.2.1. Lack of Information Credibility and Clarity
“I find that it is a bit misleading. I don’t know, I haven’t seen enough reports that make me feel encouraged by the data that’s been given. As I said, when they ask me my own ethnicity, I always say unknown, I would prefer not to say, but for me the figures are not correct anyway. They’re not really reflecting the fact that there may be other people who don’t put down their ethnicity or race, they just don’t do that. So I don’t think the figures are really a true reflection of what is happening.”(P01, ethnicity not disclosed, 57 years, female).
“I trust the government information that they give. I don’t think there is any difference between member of the—of any community. If people, they want to pick up on this, saying that, you know, the government didn’t’ do enough for BME (Black and minority ethnic people) or whatever, I don’t think it’s true”.(P05, Pakistani, 36 years, female).
“Compared to other countries our government has been very inconsistent. One example I think I do have is like maybe New Zealand. And I think it was a Scandinavian country, they were very clear, they were very like, “Well, this is how we’re doing it and this is why we’re doing it.” And they spoke directly to the people. In the UK, it’s the Prime Minister says this, and the health secretary is saying that and they’re just contradicting themselves. So that confuses people.”(P03, mixed race African/Caribbean/White, 61 years, female).
“The problem with me is that they said that, if you’ve got underlying health conditions, take the vaccine, it’s going to protect you. Then, when you hear a story about people dying of the vaccine—and they said no, they took the vaccine but they had underlying health conditions, that’s why they died. But surely the aim of the vaccine is to protect them so they don’t die, and if they’re going to die they might as well not have the vaccine you know? So I don’t know. It’s complicated.”(P07, Pakistani, 54 years, female).
“Often where people don’t follow—I talk a lot on webinars to people, individuals—and where they stop to basically listen is when you say, “Well, you’re vaccinating to protect yourself from severe illness and death”, they can follow that. But if you then say, “Vaccination doesn’t mean that you can’t harbour the virus and that you may still be experiencing symptoms”, that’s when people, I think, make their own internal risk benefit analysis. And they come to the conclusion that that’s not a good enough reason.”(P14, Consultant in Public Health).
3.2.2. Discrimination and Barriers to Healthcare
“So I did quite a few webinars and actually did a face-to-face event with young Black people in August 2021, and that was, again, really interesting. Young people with their parents came in and there was quite a lot of anger around, ‘you’re coming to talk to us about this vaccine’—first of all, just concerns about the vaccine and actually that it was going to be harming people. But actually more than that, someone stood up and said, “Look, you’ve never bothered about anything else. Why are you coming to talk to us about the vaccines?” And I think that’s why I got involved in that. I thought it was a good opportunity that if we can really reach into underserved communities for this, then there should be no reason why we can’t do the same for other health conditions, whether it’s long-term conditions or childhood immunisations, etc.”(P16, GP and Clinical Advisor to NHS England).
“I think health needs to be helped, especially in ethnic minorities, especially I think obesity is a huge problem with ethnic minorities and diabetes obviously is, and that’s kind of related. It’s not just COVID, it’s other things as well which can affect you in the lon- term with these diseases. So I think just improving your overall health instead of just saying, “Just have the vaccine and everything will be better”, because it won’t.”(P09, Indian, 42 years, male).
“You know some people said things like “are you aware that they’ve developed it so fast because they want to test it on people of African descent first.””(P21, chief executive of a VCSO supporting Black communities).
“I had one woman early on, say, “Why did you ask my ethnicity?” and I said, “So we can make sure it’s equally distributed.” And she looked at me and I was like, “Do you think there’s like a White cupboard and a Black cupboard?” She was like, “Yeah, basically”, and told me a story of a friend of hers, who was also Black, who was a carer, who had a person she was caring who was White. And so she had her vaccine because it came out of the same vial. So I think we have to be really respectful now, in particular, of people’s decisions.”(P17, Head of Community Public Health for a Local Authority).
“Other things that I think worked well outside when it came to the uptake of the vaccines, especially in ethnic minority communities, was a recognition of the historical injustice and this idea of trust. I think trust was a big issue. I found that in spaces where there was good uptake, when there was good engagement, there were places where professionals and practitioners acknowledged the historical wrongs and were willing to kind of say, ‘you know what, I understand why you do not trust us. We understand that you were wronged, we are partners on this journey together, I would like you to….’ I think that actually did work well, especially you know, where communities were hesitant.
And I find that that is a model that we would have to adopt moving forward. I think we’ve done some good work, some fantastic work in trying to engage with communities, in trying to gain trust around COVID. I think it will be terrible and incredibly dangerous if we do not apply the same amount of energy, energy and drive to diabetes to mental health, to prostate cancer etc.”(P18, Public Health programme Lead for a Local Authority).
3.2.3. Personal Beliefs, Characteristics and Experiences Influencing Vaccine Choice
“Some people think, “Oh, if I’m going to die of COVID, I might as well take the vaccine and get less side-effects from it, from the severe form of the virus, and then at least I won’t die.” But whether you’re going to die or you’re not going to die, as a Muslim we leave that in the hands of God. So God decides who’s going to die and who’s going to live. So you know, it’s not in our hands. So you could take the double-jab, get COVID, get it severe and pass away. It can, it can happen. It’s happened to family members.”(P07, Pakistani, 54 years, female).
“The problem with mandatory vaccination is that from my personal view, you’re asking somebody to say we’re going to force you to put a chemical into your body against your will. And I think that’s how it should be presented, because ultimately that is what we’re asking people to do if we’re saying it’s mandatory. We’re saying you have to put this chemical into your body, regardless of your opinion, whether it’s personal or political or religious or spiritual, whatever it is. And I just think that’s completely wrong to do that.”(P09, Indian, 42 years, male).
“For me, it’s not about information, it’s about how comfortable you are about putting something in your body. It’s just a question of are you comfortable or not, and at this point, I’m thinking about it but I’m actually thinking to myself that actually I’m ready to leave the NHS [laughs] rather than take it. Because it’s that serious where they’re giving you this ultimatum that you take it or leave your job.”(P10, Black African, 43 years, female).
3.2.4. Social Networks and Community Cohesion
“A lot of the webinars that I’ve been on, you can sense those undertones of mistrust in the Government and the NHS, exacerbated by a restricted channel of information and education that people have. Which means that people are more reliant on word-of-mouth and also, social media—WhatsApp videos, I think, has a lot to answer for. I think they’ve allowed fringe ideas to become very mainstreamed and spread very quickly. So that’s kind of what we were up against and a lot of that came out at the webinars that I’ve done since then, these myths that started right at the start.
And some of them are actually not necessarily myths. Some things are based on a couple of scientific reports that then got blown out of proportion. And even though they were disproven after a while, the damage was already done.”(P16, GP and Clinical Advisor to NHS England).
“When people are at home, because you cannot go out, the only source they get information from is the internet and social media and news, you know? Because you will only believe whatever you see on those. Like, you can access information from here.”(P06, Bangladeshi, 32 years, male).
“You look at Instagram just like a new generation of the newspaper, so you look at it as your daily news.”(P08, Bangladeshi, 21 years, male).
“There was a respect in terms of age, there was a respect in terms of people’s belief system. Because what we recognised was that we had to do things in the context of people’s historical relationship with medicines and so forth, particularly when they were designed at such rapid speed. So people’s suspicions, we had to roll with that resistance. And what happened is the wonderful thing about being culturally informed and culturally aware was that we gained much more rich information about the individual because they were comfortable in conversing with us.”(P21, chief executive of a VCSO supporting Black communities).
“There’s about three or four of us, sometimes. We’re like little old ladies, standing on the landing, talking about all sorts of issues, and the COVID and the vaccination and, you know? And I think, out of us, only one’s had it. You know? And the rest of them has the similar feeling that I’ve got, you know what I mean? We just talk about the same thing and, the way I say I feel, that’s them, as well.”(P12, Black Caribbean, 67 years, female).
“Champions programmes are where public health teams or the NHS (the statutory body) provides tailored, simple information to people in a form that is easy for them to digest and share…And in Newham, we’ve used WhatsApp as well as email and Zoom. I live in [London borough] and I’m a champion, and we get our information by email. And to be honest with you, I don’t share it, because it’s a lot of words and I have to cut and paste it into WhatsApp and I don’t. Whereas in Newham, we did one page infographics as JPEGs that people could send on, and we were told that they were really powerful. And the biggest lessons from that are—these are really like pedantic—but make stuff that’s easy for people to share. So put stuff in JPEG, not PDF, send it on WhatsApp, not email, and do it quickly when the information changes so that people trust it and they’re able to use it.”(P17, head of community public health for a local authority).
3.3. Second-Level Analysis
4. Discussion
4.1. Key Findings
4.2. Strengths and Limitations
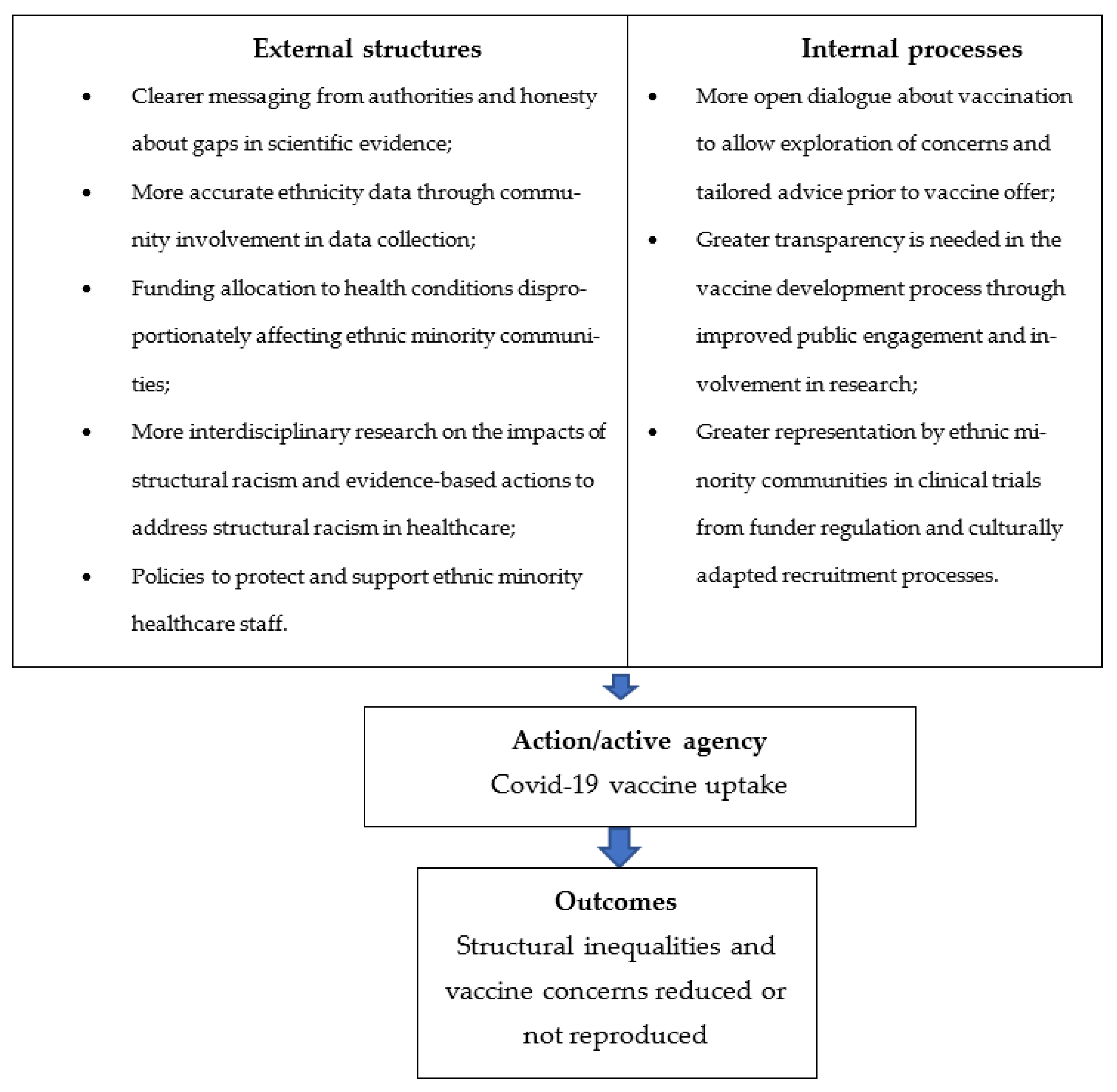
4.3. Implications for Research, Policy and Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- NHS England. COVID-19 Vaccination Deployment Strategy and Operational Readiness; NHS England: London, UK, 2020.
- Office for National Statistics. Coronavirus and Vaccination Rates in Adults by Socio-Demographic Characteristic and Occupation, England: December 2020 to March 2023. 2023. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthinequalities/bulletins/coronavirusandvaccinationratesinadultsbysociodemographiccharacteristicandoccupationengland/december2020tomarch2023#sociodemographic-characteristics (accessed on 18 August 2023).
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Report of the SAGE Working Group on Vaccine Hesitancy; World Health Organization: Geneva, Switzerland, 2014.
- Office for National Statistics. Coronavirus and Vaccine Hesitancy, Great Britain: 13 January to 7 February 2021; Office for National Statistics: London, UK, 2021.
- NHS Race and Health Observatory. Maximising Uptake of the COVID-19 Vaccine for Ethnic Minority People; NHS Race and Health Observatory: London, UK, 2021. [Google Scholar]
- Woodhead, C.; Onwumere, J.; Rhead, R.; Bora-White, M.; Chui, Z.; Clifford, N.; Connor, L.; Gunasinghe, C.; Harwood, H.; Meriez, P.; et al. Race, ethnicity and COVID-19 vaccination: A qualitative study of UK healthcare staff. Ethn. Health 2021, 27, 1555–1574. [Google Scholar] [CrossRef] [PubMed]
- Rhead, R.D.; Chui, Z.; Bakolis, I.; Gazard, B.; Harwood, H.; MacCrimmon, S.; Woodhead, C.; Hatch, S.L. Impact of workplace discrimination and harassment among National Health Service staff working in London trusts: Results from the TIDES study. BJPsych Open 2021, 7, e10. [Google Scholar] [CrossRef] [PubMed]
- Kline, R.; Naqvi, H.; Razaq, S.A.; Wilhelm, R. NHS Workforce Race Equality Standard: 2016 Data Analysis Report for NHS Trusts; NHS England: Leeds, UK, 2017. [Google Scholar]
- Nazroo, J.Y. Addressing Inequalities in Healthy Life Expectancy; Government Office for Science: London, UK, 2015. [Google Scholar]
- Amin, A.B.; Bednarczyk, R.A.; Ray, C.E.; Melchiori, K.J.; Graham, J.; Huntsinger, J.R.; Omer, S.B. Association of moral values with vaccine hesitancy. Nat. Hum. Behav. 2017, 1, 873–880. [Google Scholar] [CrossRef]
- Opel, D.J.; Mangione-Smith, R.; Robinson, J.D.; Heritage, J.; DeVere, V.; Salas, H.S.; Zhou, C.; Taylor, J.A. The influence of provider communication behaviors on parental vaccine acceptance and visit experience. Am. J. Public Health 2015, 105, 1998–2004. [Google Scholar] [CrossRef]
- Sales, J.M.; Painter, J.E.; Pazol, K.; Gargano, L.M.; Orenstein, W.; Hughes, J.M.; DiClemente, R.J. Rural parents’ vaccination-related attitudes and intention to vaccinate middle and high school children against influenza following educational influenza vaccination intervention. Hum. Vaccines 2011, 7, 1146–1152. [Google Scholar] [CrossRef]
- Spleen, A.M.; Kluhsman, B.C.; Clark, A.D.; Dignan, M.B.; Lengerich, E.J. An increase in HPV-related knowledge and vaccination intent among parental and non-parental caregivers of adolescent girls, age 9–17 years, in Appalachian Pennsylvania. J. Cancer Educ. 2012, 27, 312–319. [Google Scholar] [CrossRef]
- Stones, R. Structuration Theory; Bloomsbury Publishing: London, UK, 2017; ISBN 0230213642. [Google Scholar]
- Archer, M.S. Realist Social Theory: The Morphogenetic Approach; Cambridge University Press: Cambridge, UK, 1995; ISBN 0521484421. [Google Scholar]
- Donati, P. The ‘Relational Subject’ According to a Critical Realist Relational Sociology. J. Crit. Realism 2016, 15, 352–375. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Stones, R.; Swinglehurst, D. Choose and Book: A sociological analysis of ‘resistance’ to an expert system. Soc. Sci. Med. 2014, 104, 210–219. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Swinglehurst, D.; Stones, R. Health Services and Delivery Research. Rethinking resistance to ‘big IT’: A sociological study of why and when healthcare staff do not use nationally mandated information and communication technologies. Health Serv. Deliv. Res. 2014, 2, 2390. [Google Scholar] [CrossRef]
- Misir, P. Dismantling Systemic Racism and Structuration Theory. In COVID-19 and Health System Segregation in the US: Racial Health Disparities and Systemic Racism; Misir, P., Ed.; Springer International Publishing: Cham, Switzerland, 2022; pp. 101–117. [Google Scholar]
- Sen, A. The idea of justice. J. Hum. Dev. 2008, 9, 331–342. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Stones, R. Theorising big IT programmes in healthcare: Strong structuration theory meets actor-network theory. Soc. Sci. Med. 2010, 70, 1285–1294. [Google Scholar] [CrossRef] [PubMed]
- Haigh, F.; Kemp, L.; Bazeley, P.; Haigh, N. Developing a critical realist informed framework to explain how the human rights and social determinants of health relationship works. BMC Public Health 2019, 19, 1571. [Google Scholar] [CrossRef] [PubMed]
- Scambler, G.; Scambler, S. Theorizing health inequalities: The untapped potential of dialectical critical realism. Soc. Theory Health 2015, 13, 340–354. [Google Scholar] [CrossRef]
- Greenwood, N.; Ellmers, T.; Holley, J. The influence of ethnic group composition on focus group discussions. BMC Med. Res. Methodol. 2014, 14, 107. [Google Scholar] [CrossRef]
- Kidd, P.S.; Parshall, M.B. Getting the focus and the group: Enhancing analytical rigor in focus group research. Qual. Health Res. 2000, 10, 293–308. [Google Scholar] [CrossRef]
- Focus Group Methodology: Principles and Practice. London. 2011. Available online: https://methods.sagepub.com/book/focus-group-methodology (accessed on 18 August 2023).
- Halcomb, E.J.; Gholizadeh, L.; DiGiacomo, M.; Phillips, J.; Davidson, P.M. Literature review: Considerations in undertaking focus group research with culturally and linguistically diverse groups. J. Clin. Nurs. 2007, 16, 1000–1011. [Google Scholar] [CrossRef]
- NHS England. COVID-19 Vaccinations 2021. Available online: https://www.england.nhs.uk/statistics/statistical-work-areas/covid-19-vaccinations/ (accessed on 18 August 2023).
- Public Health England. Coronavirus (COVID-19) Vaccinations in the United Kingdom. 2021. Available online: https://coronavirus.data.gov.uk/details/vaccinations (accessed on 2 September 2021).
- Poduval, S.; Kaviraj, C. Research Department of Primary Care and Population Health Blog. 2022. Available online: https://blogs.ucl.ac.uk/pcph-blog/2022/03/04/diverse-voices-a-ucl-community-engagement-project-on-diversity-in-health-research-participation/ (accessed on 18 August 2023).
- National Institute for Health Research. Being Inclusive in Public Involvement in Health and Care Research. 2021. Available online: https://www.nihr.ac.uk/documents/being-inclusive-in-public-involvement-in-health-and-care-research/27365#how-to-cite-this-guidance (accessed on 10 January 2023).
- NIHR CLAHRC East Midlands Centre for BME Health. Toolkit for Increasing Participation of BAME Groups in Health and Social Care Research; NIHR CLAHRC East Midlands Centre for BME Health: London, UK, 2018. [Google Scholar]
- QSR International Pty Ltd. NVivo (Version 12). 2018. Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 10 January 2023).
- Terry, G.; Hayfield, N.; Clarke, V.; Braun, V. Thematic analysis. SAGE Handbook Qual. Res. Psychol. 2017, 2, 17–37. [Google Scholar]
- Pope, C. Qualitative Research in Health Care, 4th ed.; Pope, C., Mays, N., Eds.; Wiley Blackwell: Hoboken, NJ, USA, 2020. [Google Scholar]
- Canesqui, A.M.; Ritchie, J.; Lewis, J. Qualitative Research Practice: A Guide for Social Science Studentes and Researchers; Interface: Botucatu, Brazil, 2010. [Google Scholar]
- Baum, F.; MacDougall, C.; Smith, D. Participatory action research. J. Epidemiol. Community Health 2006, 60, 854–857. [Google Scholar] [CrossRef]
- Co-Production Collective. 2021. Available online: https://www.coproductioncollective.co.uk/ (accessed on 30 April 2021).
- NIHR ARC West. A Map of Resources for Co-Producing Research in Health and Social. Care; NIHR ARC West: Bristol, UK, 2020. [Google Scholar]
- Google. What’s Jamboard? 2023. Available online: https://support.google.com/jamboard/answer/7424836?hl=en (accessed on 18 August 2023).
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic Analysis: Striving to Meet the Trustworthiness Criteria. Int. J. Qual. Methods 2017, 16, 1609406917733847. [Google Scholar] [CrossRef]
- Routen, A.; Akbari, A.; Banerjee, A.; Katikireddi, S.V.; Mathur, R.; McKee, M.; Nafilyan, V.; Khunti, K. Strategies to record and use ethnicity information in routine health data. Nat. Med. 2022, 28, 1338–1342. [Google Scholar] [CrossRef] [PubMed]
- Mathur, R.; Rentsch, C.T.; Venkataraman, K.; Fatumo, S.; Jobe, M.; Angkurawaranon, C.; Ong, S.E.; Wong, A.Y.; Siddiqui, M.K. How do we collect good-quality data on race and ethnicity and address the trust gap? Lancet 2022, 400, 2028–2030. [Google Scholar] [CrossRef] [PubMed]
- Bignall, T.; Phillips, J. Improving the Recording of Ethnicity in Health Datasets; Wellcome Trust: London, UK, 2022. [Google Scholar]
- Collaboration for Change. Collaboration for Change: Promoting Vaccine Uptake. 2021. Available online: https://collaborationforchange.co.uk/wp-content/uploads/2023/08/report.pdf (accessed on 18 August 2023).
- Devakumar, D.; Selvarajah, S.; Abubakar, I.; Kim, S.S.; McKee, M.; Sabharwal, N.S.; Saini, A.; Shannon, G.; White, A.I. Racism, xenophobia, discrimination, and the determination of health. Lancet 2022, 400, 2097–2108. [Google Scholar] [CrossRef]
- Selvarajah, S.; Maioli, S.C.; Abi Deivanayagam, T.; de Morais Sato, P.; Devakumar, D.; Kim, S.S.; Wells, J.C.; Yoseph, M.; Abubakar, I.; Paradies, Y. Racism, xenophobia, and discrimination: Mapping pathways to health outcomes. Lancet 2022, 400, 2109–2124. [Google Scholar] [CrossRef] [PubMed]
- Race and Health Observatory. Ethnic Inequalities in Healthcare: A Rapid Evidence Review; Race and Health Observatory: London, UK, 2022. [Google Scholar]
- Ekezie, W.; Czyznikowska, B.M.; Rohit, S.; Harrison, J.; Miah, N.; Campbell-Morris, P.; Khunti, K. The views of ethnic minority and vulnerable communities towards participation in COVID-19 vaccine trials. J. Public Health 2021, 43, e258–e260. [Google Scholar] [CrossRef]
- Kadambari, S.; Vanderslott, S. Lessons about COVID-19 vaccine hesitancy among minority ethnic people in the UK. Lancet Infect. Dis. 2021, 21, 1204–1206. [Google Scholar] [CrossRef]
- Murali, M.; Gumber, L.; Jethwa, H.; Ganesh, D.; Hartmann-Boyce, J.; Sood, H.; Zaccardi, F.; Khunti, K. Ethnic minority representation in UK COVID-19 trials: Systematic review and meta-analysis. BMC Med. 2023, 21, 111. [Google Scholar] [CrossRef]
- Sides, E.; Jones, L.F.; Kamal, A.; Thomas, A.; Syeda, R.; Kaissi, A.; Lecky, D.M.; Patel, M.; Nellums, L.; Greenway, J.; et al. Attitudes towards coronavirus (COVID-19) vaccine and sources of information across diverse ethnic groups in the UK: A qualitative study from June to October 2020. BMJ Open 2022, 12, e060992. [Google Scholar] [CrossRef]
- Gogoi, M.; Wobi, F.; Qureshi, I.; Al-Oraibi, A.; Hassan, O.; Chaloner, J.; Nellums, L.B.; Pareek, M.; UK-REACH Collaborative Group. “The vaccination is positive; I don’t think it’s the panacea”: A qualitative study on COVID-19 vaccine attitudes among ethnically diverse healthcare workers in the United Kingdom. PLoS ONE 2022, 17, e0273687. [Google Scholar] [CrossRef]
- Magee, L.; Knights, F.; McKechnie, D.G.J.; Al-bedaery, R.; Razai, M.S. Facilitators and barriers to COVID-19 vaccination uptake among ethnic minorities: A qualitative study in primary care. PLoS ONE 2022, 17, e0270504. [Google Scholar] [CrossRef]
- Regnier-Davies, J.; Edge, S.; Austin, N. The intersection of structure and agency within charitable community food programs in Toronto, Canada, during the COVID-19 pandemic: Cultivating systemic change. Crit. Public Health 2023, 33, 355–362. [Google Scholar] [CrossRef]
- Dean, W.R.; Sharkey, J.R.; Johnson, C.M. The Possibilities and Limits of Personal Agency. Food Cult. Soc. 2016, 19, 129–149. [Google Scholar] [CrossRef]
- Corbie-Smith, G. Vaccine Hesitancy Is a Scapegoat for Structural Racism. JAMA Health Forum 2021, 2, e210434. [Google Scholar] [CrossRef] [PubMed]
- Hussain, B.; Latif, A.; Timmons, S.; Nkhoma, K.; Nellums, L.B. Overcoming COVID-19 vaccine hesitancy among ethnic minorities: A systematic review of UK studies. Vaccine 2022, 40, 3413–3432. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | Mean (SD) or Frequency (%) |
|---|---|
| Age (years) | 45.3 (12.9) |
| Gender | |
| Male | 5 (35.7) |
| Female | 9 (64.3) |
| Ethnicity | |
| Bangladeshi | 4 (28.6) |
| Caribbean | 3 (21.4) |
| Pakistani | 2 (14.3) |
| Mixed | 2 (14.3) |
| African | 1 (7.1) |
| Indian | 1 (7.1) |
| Prefer not to say | 1 (7.1) |
| Country of birth | |
| UK | 7 (50) |
| Pakistan | 2 (14.3) |
| Bangladesh | 1 (7.1) |
| France | 1 (7.1) |
| St Kitts | 1 (7.1) |
| First Language | |
| English | 9 (64.3) |
| Bengali | 3 (21.4) |
| French | 1 (7.1) |
| Punjabi | 1 (7.1) |
| Highest level qualification | |
| No formal qualification | 0 |
| GCSE or equivalent | 3 (21.4) |
| Apprenticeship | 0 |
| A Level or equivalent | 2 (14.3) |
| Bachelor’s degree or postgraduate qualification | 7 (50) |
| Other qualifications of unknown level | 2 (14.3) |
| Vaccine status | |
| Unvaccinated | 5 (35.7) |
| One dose | 1 (7.1) |
| Two doses | 4 (28.6) |
| Fully Vaccinated | 2 (14.3) |
| Prefer not to say | 2 (14.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poduval, S.; Kamal, A.; Martin, S.; Islam, A.; Kaviraj, C.; Gill, P. Beyond Information Provision: Analysis of the Roles of Structure and Agency in COVID-19 Vaccine Confidence in Ethnic Minority Communities. Int. J. Environ. Res. Public Health 2023, 20, 7008. https://doi.org/10.3390/ijerph20217008
Poduval S, Kamal A, Martin S, Islam A, Kaviraj C, Gill P. Beyond Information Provision: Analysis of the Roles of Structure and Agency in COVID-19 Vaccine Confidence in Ethnic Minority Communities. International Journal of Environmental Research and Public Health. 2023; 20(21):7008. https://doi.org/10.3390/ijerph20217008
Chicago/Turabian StylePoduval, Shoba, Atiya Kamal, Sam Martin, Amin Islam, Chandrika Kaviraj, and Paramjit Gill. 2023. "Beyond Information Provision: Analysis of the Roles of Structure and Agency in COVID-19 Vaccine Confidence in Ethnic Minority Communities" International Journal of Environmental Research and Public Health 20, no. 21: 7008. https://doi.org/10.3390/ijerph20217008
APA StylePoduval, S., Kamal, A., Martin, S., Islam, A., Kaviraj, C., & Gill, P. (2023). Beyond Information Provision: Analysis of the Roles of Structure and Agency in COVID-19 Vaccine Confidence in Ethnic Minority Communities. International Journal of Environmental Research and Public Health, 20(21), 7008. https://doi.org/10.3390/ijerph20217008