
The Impact of Culture-, Health- and Nature-Based Engagement on Mitigating the Adverse Effects of Public Health Restrictions on Wellbeing, Social Connectedness and Loneliness during COVID-19: Quantitative Evidence from a Smaller- and Larger-Scale UK Survey

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Analysis of the Community COVID Survey
3.1.1. Community COVID Questions
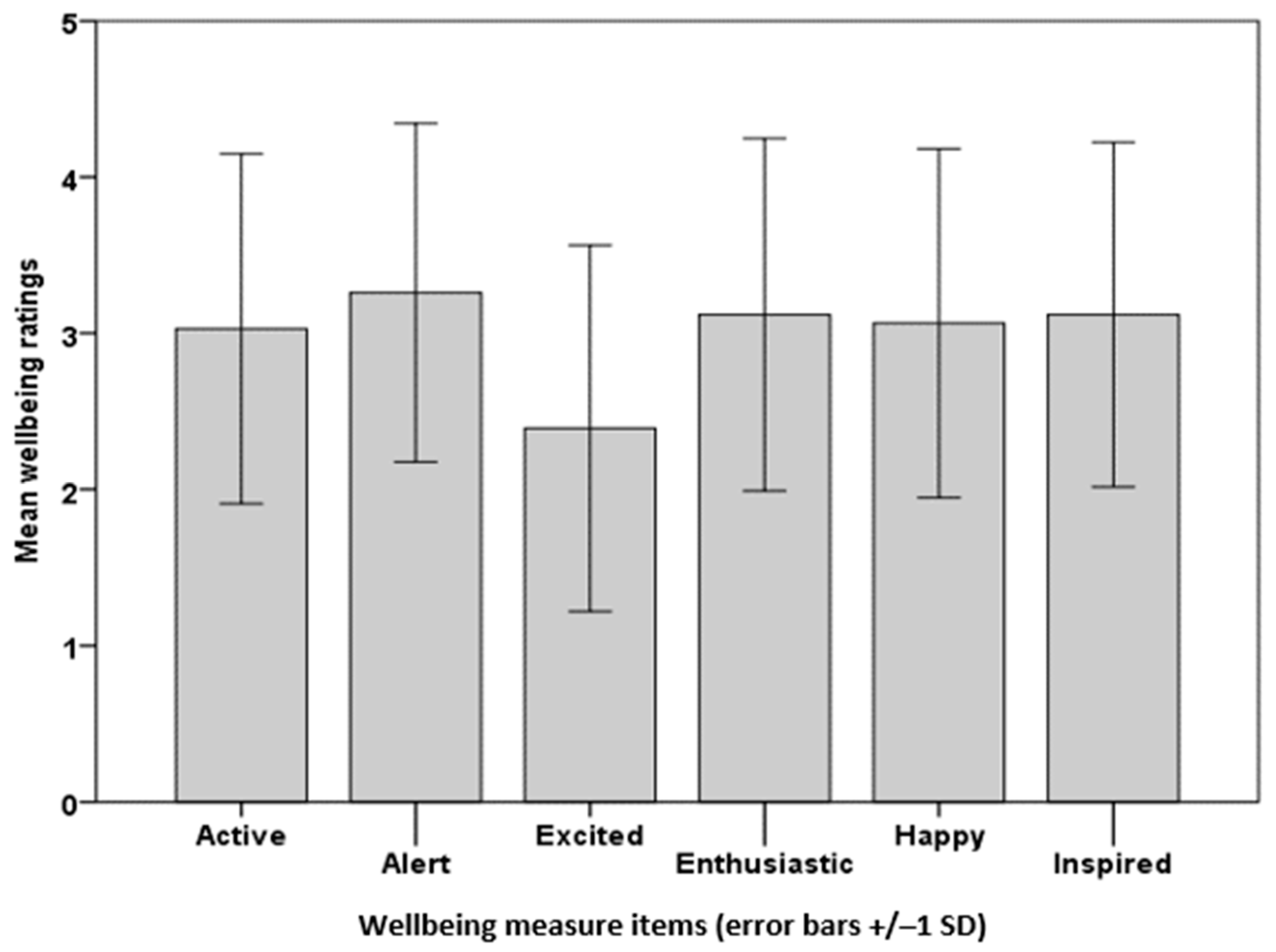
3.1.2. Predictor Variables for Wellbeing
3.2. Analysis of Both Surveys
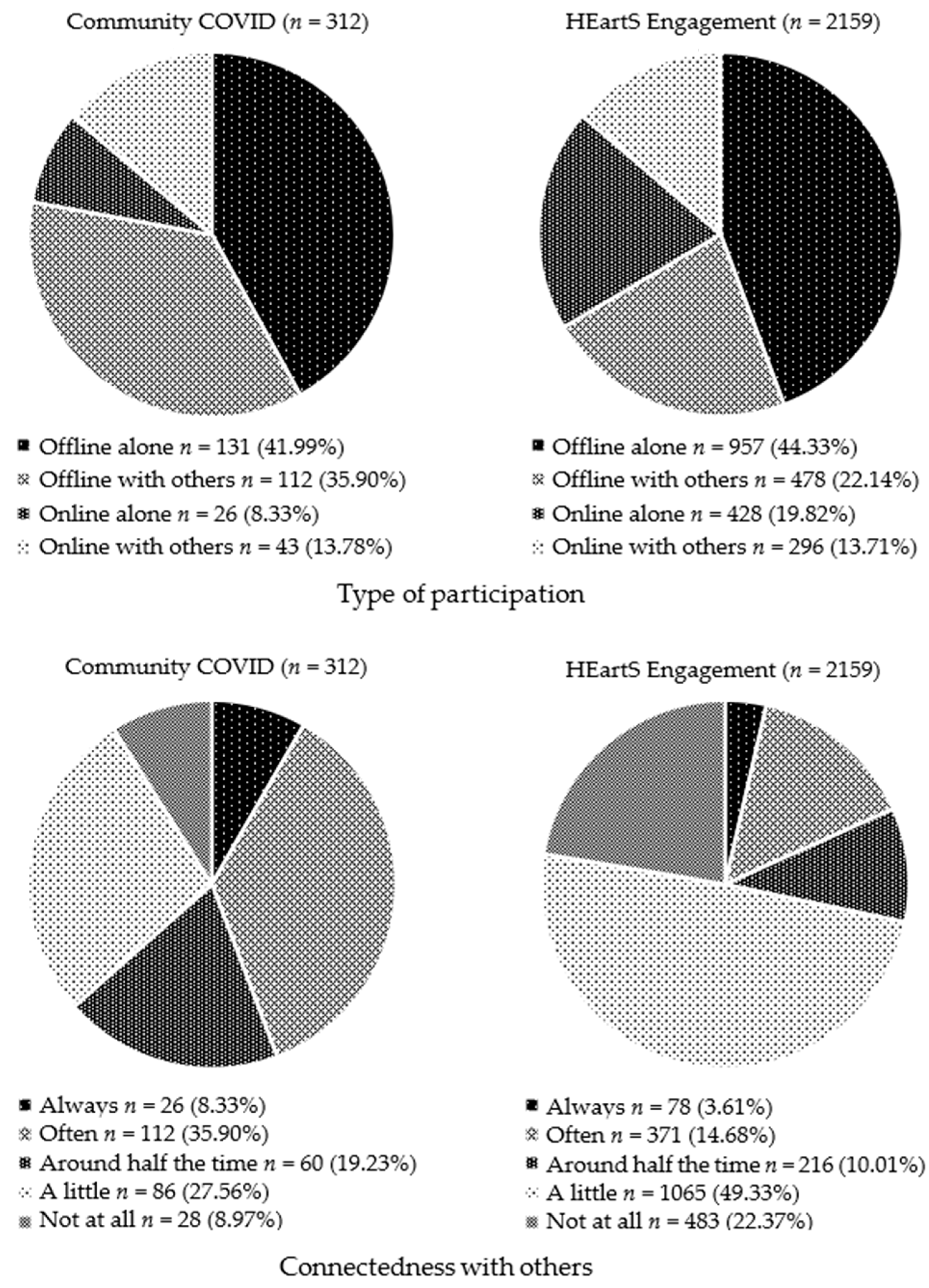
3.2.1. Type of Participation and Connectedness with Others
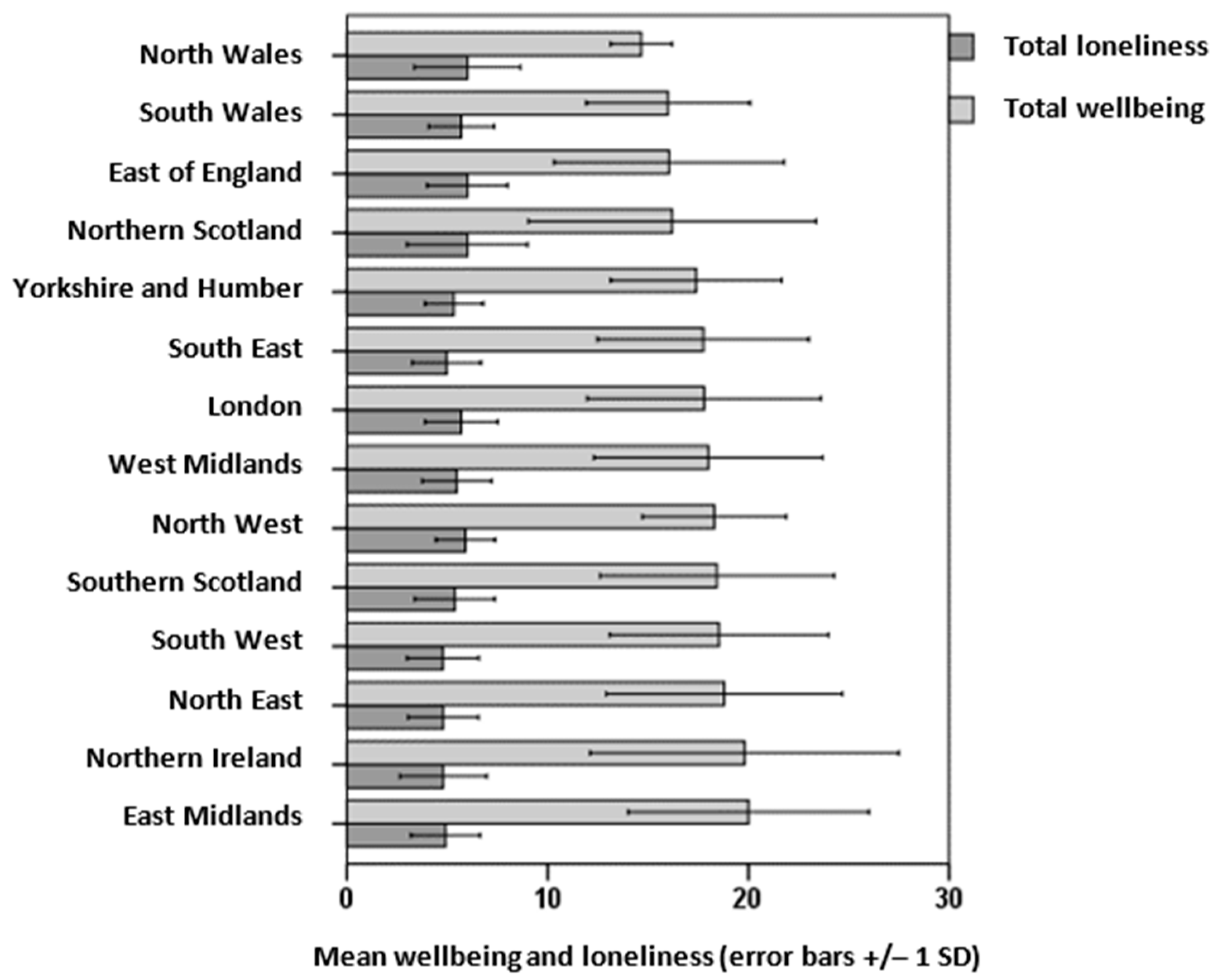
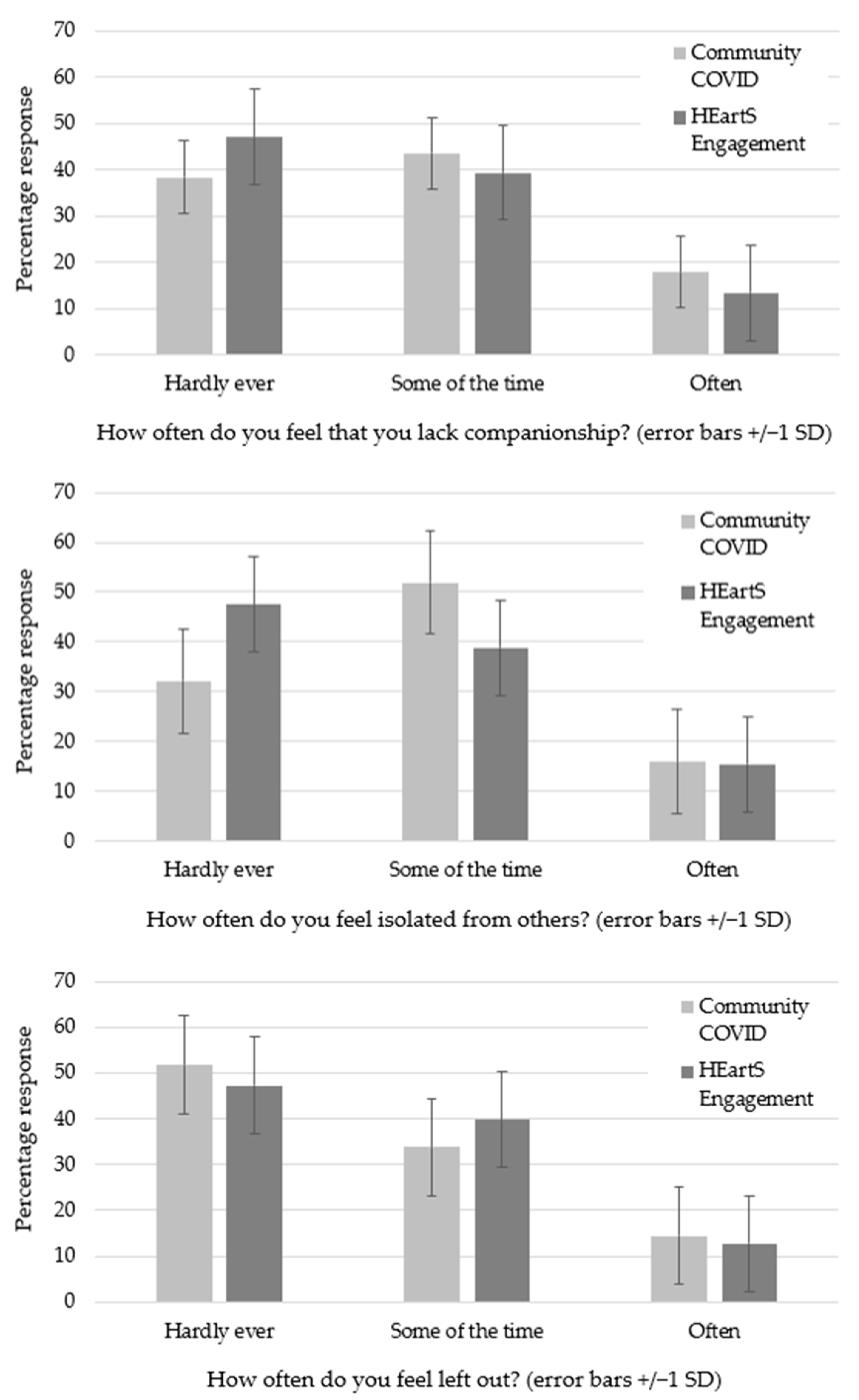
3.2.2. Loneliness
3.2.3. Correlation of Respondents
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Community COVID: What Have You Been Doing? Survey Questions
- What have you done with your free time during COVID-19 restrictions? Please list your main activities below: (These could include arts, crafts, choirs, dance, DIY, fitness, games, gardening, music, nature, puzzles, reading, volunteering, walking, writing, etc.)
- What are the advantages of taking part in these activities?
- What are the disadvantages of taking part in these activities?
- How often have you taken part in these activities compared with before COVID-19 restrictions? (Please select one) [Options: Much less often; Quite a lot less often; A little less often; No change; A little more often; Quite a lot more often; Much more often]
- How do you usually take part in these activities? (Please select one) ‘Online’ means social media, websites, apps, live streaming, online forums, etc. and ‘Offline’ means in person, in a garden or park, at a venue, etc. [Options: Online alone; Online with other people; Offline alone; Offline with other people]
- How much have these activities helped you feel connected with other people? (Please select one) [Options: Not at all; A little; Around half the time; Often; Always]
- Please select one box (out of five) for each word to indicate how you feel on a typical day: [Words: Active; Alert; Enthusiastic; Excited; Happy; Inspired] [Options: 1 = I don’t feel…; 2 = I feel a little bit…; 3 = I feel fairly…; 4 = I feel quite a bit…; 5 = I feel extremely…]
- Please select one box (out of three) for each question to indicate how you feel on a typical day: [Questions: How often do you feel that you lack companionship?; How often do you feel left out?; How often do you feel isolated from others?] [Options: 1 = Hardly ever; 2 Some of the time; 3 = Often]
- Which age group are you in? [Options: 18–29; 30–39; 40–49; 50–59; 60–69; 70–79; 80+; Prefer not to say]
- Where do you live? [Options: Northern Scotland; Southern Scotland; North East; North West; Yorkshire and the Humber; East Midlands; West Midlands; East of England; South East England; South West England; London; North Wales; South Wales; Northern Ireland]
Appendix A.2. Health, Economic, and Social Impact of the Arts (HEartS) Engagement Survey: Culture-, Health- and Nature-Based Engagement Questions

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Range | ||||||||||
| UK Region | 18–29 | 30–39 | 40–49 | 50–59 | 60–69 | 70–79 | 80+ | Total | Percentage | |
| Community COVID What have you been doing? survey | Scotland | 2 | 2 | 6 | 1 | 7 | 3 | 0 | 21 | 6.73% |
| North East | 1 | 0 | 3 | 2 | 1 | 2 | 1 | 10 | 3.21% | |
| North West | 1 | 1 | 2 | 1 | 6 | 8 | 1 | 20 | 6.41% | |
| Yorkshire and Humber | 0 | 2 | 4 | 5 | 2 | 2 | 0 | 15 | 4.81% | |
| East Midlands | 0 | 3 | 2 | 4 | 6 | 8 | 0 | 23 | 7.37% | |
| West Midlands | 1 | 2 | 4 | 3 | 4 | 1 | 0 | 15 | 4.81% | |
| East of England | 0 | 2 | 2 | 3 | 9 | 3 | 1 | 20 | 6.41% | |
| South East | 7 | 8 | 9 | 24 | 19 | 15 | 4 | 86 | 27.56% | |
| South West | 0 | 3 | 6 | 9 | 8 | 9 | 6 | 41 | 13.14% | |
| London | 1 | 5 | 5 | 14 | 7 | 10 | 1 | 43 | 13.78% | |
| Wales | 0 | 3 | 1 | 0 | 8 | 1 | 0 | 13 | 4.17% | |
| Northern Ireland | 1 | 0 | 0 | 2 | 2 | 0 | 0 | 5 | 1.60% | |
| Total | 14 | 31 | 44 | 68 | 79 | 62 | 14 | 312 | ||
| Percentage | 4.48% | 9.94% | 14.10% | 21.79% | 25.32% | 19.87% | 4.49% | 100% | ||
| AgeRange | ||||||||||
| UK Region | 18–29 | 30–39 | 40–49 | 50–59 | 60–69 | 70–79 | 80+ | Total | Percentage | |
| Health, Economic and Social Impacts of the Arts (HEartS) Engagement survey | Scotland | 22 | 44 | 35 | 57 | 66 | 28 | 1 | 253 | 6.94% |
| North East | 18 | 22 | 20 | 35 | 24 | 11 | 2 | 132 | 3.62% | |
| North West | 32 | 81 | 90 | 90 | 83 | 34 | 5 | 415 | 11.38% | |
| Yorkshire and Humber | 39 | 51 | 77 | 64 | 54 | 23 | 4 | 312 | 8.55% | |
| East Midlands | 34 | 46 | 47 | 68 | 43 | 27 | 2 | 267 | 7.32% | |
| West Midlands | 37 | 55 | 66 | 56 | 54 | 24 | 1 | 293 | 8.03% | |
| East of England | 40 | 85 | 89 | 84 | 69 | 46 | 5 | 418 | 11.46% | |
| South East | 56 | 77 | 103 | 137 | 101 | 54 | 4 | 532 | 14.59% | |
| South West | 29 | 49 | 51 | 74 | 73 | 37 | 5 | 318 | 8.72% | |
| London | 52 | 101 | 88 | 90 | 52 | 35 | 0 | 418 | 11.46% | |
| Wales | 16 | 27 | 40 | 51 | 39 | 20 | 2 | 195 | 5.35% | |
| Northern Ireland | 6 | 11 | 16 | 34 | 24 | 3 | 0 | 94 | 2.58% | |
| Total | 381 | 649 | 722 | 840 | 682 | 342 | 31 | 3647 | ||
| Percentage | 10.45% | 17.80% | 19.80% | 23.03% | 18.79% | 9.38% | 0.85% | 100% | ||
| Activities | Frequency | Activity Category | Total Frequency | Percentage of Activities | Percentage of Respondents |
|---|---|---|---|---|---|
| Walking for fitness | 163 | Sport/fitness activities | 269 | 16.41% | 86.22% |
| Keep fit and exercise | 61 | ||||
| Running and jogging | 25 | ||||
| Cycling/biking | 8 | ||||
| Swimming/free swimming | 9 | ||||
| Tennis | 3 | ||||
| Quilting/patchwork | 86 | Crafts, textiles or decorative arts | 208 | 12.69% | 66.67% |
| Sewing/dressmaking | 66 | ||||
| Embroidery/stitching | 25 | ||||
| Knitting and crochet | 23 | ||||
| Clay work and pottery | 4 | ||||
| Paper crafts | 4 | ||||
| Gardening/planting | 146 | Gardening/looking after plants | 166 | 10.13% | 53.21% |
| Growing fruit and veg | 9 | ||||
| Allotments/horticulture | 7 | ||||
| House/balcony plants | 4 | ||||
| Art/painting | 89 | Painting, drawing, printmaking, sculpture, etc. | 129 | 7.87% | 41.35% |
| Drawing/sketching | 26 | ||||
| Printmaking | 8 | ||||
| Collage | 6 | ||||
| Volunteering | 48 | Volunteering and community activities | 99 | 6.04% | 31.73% |
| Community activities | 22 | ||||
| Sewing scrubs and masks | 18 | ||||
| Food bank/distribution | 11 | ||||
| Reading for pleasure | 75 | Reading as a pastime | 75 | 4.58% | 24.04% |
| Cooking and baking | 71 | Cooking and baking | 74 | 4.51% | 23.72% |
| Bread making | 3 | ||||
| Catching up with friends | 47 | Talking to friends and family/socializing | 65 | 3.97% | 20.83% |
| Talking to family | 14 | ||||
| Social activities | 4 | ||||
| Sudoku/number puzzles | 41 | Crosswords and other puzzles | 64 | 3.90% | 20.51% |
| Crosswords/word puzzles | 14 | ||||
| Jigsaw puzzles | 9 | ||||
| Writing/writing poetry | 47 | Writing as a pastime | 54 | 3.29% | 17.31% |
| Keeping journal/diary | 7 | ||||
| Singing and choirs | 26 | Singing/playing musical instrument | 50 | 3.05% | 16.03% |
| Playing musical instrument | 24 | ||||
| Do-it-yourself (DIY) | 45 | DIY/home improvements | 48 | 2.93% | 15.38% |
| Home improvements | 3 | ||||
| Watching films/videos | 15 | Watching films or dramas | 40 | 2.44% | 12.82% |
| Watching TV dramas/films | 25 | ||||
| Shopping for self/family | 12 | Housework/domestic tasks | 38 | 2.32% | 12.18% |
| Housework | 9 | ||||
| Tidying and decluttering | 4 | ||||
| Playing video games | 18 | Games and gaming | 36 | 2.20% | 11.54% |
| Playing board/card games | 18 | ||||
| Working | 15 | Working, studying and training courses | 32 | 1.95% | 10.26% |
| Studying and learning | 14 | ||||
| Attending training courses | 3 | ||||
| Yoga | 19 | Yoga/meditation/ mindfulness | 31 | 1.89% | 9.94% |
| Meditation | 6 | ||||
| Mindfulness | 6 | ||||
| Visiting nature | 24 | Visiting natural environments | 29 | 1.77% | 9.29% |
| Birdwatching | 5 | ||||
| Photography | 12 | Photography, film/video making | 21 | 1.28% | 6.41% |
| Film and video making | 9 | ||||
| Dog walking | 15 | Dog walking/looking after pets | 20 | 1.22% | 6.41% |
| Looking after pets | 5 | ||||
| Childcare | 15 | Caring for others | 17 | 1.04% | 5.45% |
| Carer | 2 | ||||
| Listening to music | 13 | Listening to recorded music | 16 | .98% | 5.13% |
| Listening to music on radio | 3 | ||||
| Quizzing and quizzes | 12 | Quizzes | 12 | 0.73% | 3.85% |
| Dancing | 10 | Practicing/performing dance | 10 | 0.61% | 3.21% |
| Audio books | 4 | Listening to audio books/podcasts | 8 | 0.49% | 2.56% |
| Podcasts | 4 | ||||
| Creative ideas | 5 | Creative thinking | 8 | 0.49% | 2.56% |
| Thinking/reflecting | 3 | ||||
| Church, mosque, religion | 7 | Religious practice | 7 | 0.43% | 2.24% |
| Eating | 4 | Eating and drinking | 6 | 0.37% | 1.92% |
| Drinking | 2 | ||||
| Acting for play/drama | 5 | Practicing/performing play | 5 | 0.31% | 1.60% |
| Collecting | 2 | Collecting | 2 | 0.12% | 0.64% |
| Type of Participation | Frequency | Activity Category | Total Frequency | Percentage of Activities | Percentage of Respondents |
|---|---|---|---|---|---|
| Online alone | 521 | Watching films or dramas | 2701 | 10.02% | 74.06% |
| Online with others | 641 | ||||
| Offline alone | 613 | ||||
| Offline with others | 926 | ||||
| Online alone | 608 | Reading as a pastime | 2634 | 9.78% | 72.22% |
| Online with others | 189 | ||||
| Offline alone | 1755 | ||||
| Offline with others | 82 | ||||
| Online alone | 109 | Gardening/looking after plants | 2391 | 8.87% | 65.56% |
| Online with others | 127 | ||||
| Offline alone | 1328 | ||||
| Offline with others | 827 | ||||
| Online alone | 837 | Listening to recorded music | 2335 | 8.70% | 64.03% |
| Online with others | 318 | ||||
| Offline alone | 886 | ||||
| Offline with others | 294 | ||||
| Online alone | 412 | Crosswords and other puzzles | 1959 | 7.27% | 53.72% |
| Online with others | 156 | ||||
| Offline alone | 1221 | ||||
| Offline with others | 170 | ||||
| Online alone | 169 | Sport/fitness activities | 1900 | 7.05% | 52.10% |
| Online with others | 161 | ||||
| Offline alone | 1052 | ||||
| Offline with others | 518 | ||||
| Online alone | 652 | Games and gaming | 1747 | 6.48% | 47.90% |
| Online with others | 358 | ||||
| Offline alone | 447 | ||||
| Offline with others | 290 | ||||
| Online alone | 92 | Visiting natural environments | 1597 | 5.93% | 43.79% |
| Online with others | 117 | ||||
| Offline alone | 381 | ||||
| Offline with others | 1007 | ||||
| Online alone | 88 | Dog walking/looking after pets | 1516 | 5.63% | 41.57% |
| Online with others | 137 | ||||
| Offline alone | 613 | ||||
| Offline with others | 678 | ||||
| Online alone | 138 | DIY/home improvements | 1505 | 5.59% | 41.24% |
| Online with others | 139 | ||||
| Offline alone | 1153 | ||||
| Offline with others | 74 | ||||
| Online alone | 713 | Listening to audio books or podcasts | 1176 | 4.36% | 32.25% |
| Online with others | 170 | ||||
| Offline alone | 252 | ||||
| Offline with others | 41 | ||||
| Online alone | 114 | Crafts, textiles or decorative arts | 886 | 3.20% | 24.29% |
| Online with others | 122 | ||||
| Offline alone | 555 | ||||
| Offline with others | 95 | ||||
| Online alone | 226 | Writing as a pastime | 727 | 2.70% | 19.93% |
| Online with others | 171 | ||||
| Offline alone | 298 | ||||
| Offline with others | 32 | ||||
| Online alone | 168 | Yoga/meditation/mindfulness | 719 | 2.66% | 19.71% |
| Online with others | 133 | ||||
| Offline alone | 325 | ||||
| Offline with others | 93 | ||||
| Online alone | 106 | Painting, drawing, printmaking, sculpture, etc. | 680 | 2.52% | 18.65% |
| Online with others | 126 | ||||
| Offline alone | 365 | ||||
| Offline with others | 83 | ||||
| Online alone | 94 | Playing musical instrument or singing | 661 | 2.45% | 18.12% |
| Online with others | 142 | ||||
| Offline alone | 358 | ||||
| Offline with others | 67 | ||||
| Online alone | 157 | Photography, film making, video, etc. | 589 | 2.19% | 16.15% |
| Online with others | 135 | ||||
| Offline alone | 261 | ||||
| Offline with others | 36 | ||||
| Online alone | 88 | Volunteering/community activities | 542 | 2.01% | 14.86% |
| Online with others | 141 | ||||
| Offline alone | 149 | ||||
| Offline with others | 164 | ||||
| Online alone | 87 | Practicing, performing dance | 383 | 1.42% | 10.50% |
| Online with others | 128 | ||||
| Offline alone | 127 | ||||
| Offline with others | 41 | ||||
| Online alone | 76 | Practicing, performing play | 298 | 1.11% | 8.17% |
| Online with others | 134 | ||||
| Offline alone | 60 | ||||
| Offline with others | 28 |
References
- Williams, D.M.; Conti, G.; Chaturvedi, N.; Hughes, A.; Ploubidis, G.B.; Silverwood, R.J. Prevalence of COVID-19, symptoms and testing: Initial findings from the COVID-19 Survey in Five National Longitudinal Studies; UCL Centre for Longitudinal Studies: London, UK, 2020; Available online: https://cls.ucl.ac.uk/wp-content/uploads/2020/12/Prevalence-of-COVID-19-symptoms-and-testing-in-the-UK-Initial-findings-from-COVID-19-survey.pdf (accessed on 16 May 2023).
- Pouwels, K.B.; House, T.; Pritchard, E.; Robotham, J.V.; Birrell, P.J.; Gelman, A.; Vihta, K.-D.; Bowers, N.; Boreham, I.; Thomas, H.; et al. Community Prevalence of SARS-COV-2 in England from April to November, 2020: Results from the ONS Coronavirus Infection Survey. Lancet Public Health 2021, 6, e30–e38. [Google Scholar] [CrossRef]
- Walker, A.S.; Vihta, K.; Gethings, O.; Pritchard, E.; Jones, J.; House, T.; Bell, I.; Bell, J.I.; Newton, J.N.; Farrar, J.; et al. Increased infections, but not viral burden, with a new SARS-CoV-2 variant. medRxiv 2021. Preprint. [Google Scholar] [CrossRef]
- Wei, J.; Stoesser, N.; Matthews, P.C.; Ayoubkhani, D.; Studley, R.; Bell, I.; Bell, J.I.; Newton, J.N.; Farrar, J.; Diamond, I.; et al. The impact of SARS-CoV-2 vaccines on antibody responses in the general population in the United Kingdom. Nat. Microbiol. 2021, 6, 1140–1149. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, E.; Matthews, P.C.; Stoesser, N.; Eyre, D.W.; Gethings, O.; Vihta, K.-D.; Jones, J.; House, T.; VanSteenHouse, H.; Bell, I.; et al. Impact of vaccination on SARS-CoV-2 cases in the community: A population-based study using the UK’s COVID-19 Infection Survey. Nat. Med. 2021, 27, 1370–1378. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Mental Health and Psychosocial Considerations during the COVID-19 Outbreak; WHO: Geneva, Switzerland, 2021; Available online: https://www.who.int/docs/default-source/coronaviruse/mental-health-considerations.pdf (accessed on 16 May 2023).
- Young Minds. Coronavirus: Impact on Young People with Mental Health Needs; Young Minds: London, UK, 2020; Available online: https://youngminds.org.uk/media/3708/coronavirus-report_march2020.pdf (accessed on 16 May 2023).
- Young Minds. Coronavirus: Impact on Young People with Mental Health Needs, Survey 2: Summer 2020; Young Minds: London, UK, 2020b; Available online: https://youngminds.org.uk/media/3904/coronavirus-report-summer-2020-final.pdf (accessed on 16 May 2023).
- Young Minds. Coronavirus: Impact on Young People with Mental Health Needs, Survey 3: Autumn 2020—Return to School; Young Minds: London, UK, 2020; Available online: https://youngminds.org.uk/media/4119/youngminds-survey-with-young-people-returning-to-school-coronavirus-report-autumn-report.pdf (accessed on 16 May 2023).
- Young Minds. Coronavirus: Impact on Young People with Mental Health Needs, Survey 4: February 2021; Young Minds: London, UK, 2021; Available online: https://youngminds.org.uk/media/4350/coronavirus-report-winter.pdf (accessed on 16 May 2023).
- Giebel, C.; Pulford, D.; Cooper, C.; Lord, K.; Shenton, J.; Cannon, J.; Shaw, L.; Tetlow, H.; Limbert, S.; Callaghan, S.; et al. COVID-19-related social support service closures and mental well-being in older adults and those affected by dementia: A UK longitudinal survey. BMJ Open 2021, 11, 1–8. [Google Scholar] [CrossRef]
- Carpentieri, J.; Wielgoszewska, B.; Church, D.; Goodman, A. their own words: Five generations of Britons describe their experiences of the coronavirus pandemic: Initial findings from the COVID-19 Survey in Five National Longitudinal Studies; UCL Centre for Longitudinal Studies: London, UK, 2020; Available online: https://cls.ucl.ac.uk/wp-content/uploads/2020/11/In-their-own-words-Initial-findings-from-COVID-19-survey.pdf (accessed on 16 May 2023).
- Henderson, M.; Fitzsimons, E.; Ploubidis, G.; Richards, M.; Patalay, P. Mental Health during Lockdown: Evidence from Four Generations—Initial Findings from the COVID-19 Survey in Five National Longitudinal Studies; UCL Centre for Longitudinal Studies: London, UK, 2020; Available online: https://cls.ucl.ac.uk/wp-content/uploads/2017/02/Mental-health-during-lockdown-%E2%80%93-initial-findings-from-COVID-19-survey-1.pdf (accessed on 16 May 2023).
- Zilanawala, A.; Chanfreau, J.; Sironi, M.; Palma, M. Household Composition, Couples’ Relationship Quality, and Social Support during Lockdown: Initial Findings from the COVID-19 Survey in Five National Longitudinal Studies; UCL Centre for Longitudinal Studies: London, UK, 2020; Available online: https://cls.ucl.ac.uk/wp-content/uploads/2020/11/Household-composition-couples-relationship-quality-and-social-support-during-lockdown-%E2%80%93-Initial-findings-from-COVID.pdf (accessed on 16 May 2023).
- Rathod, S.; Pallikadavath, S.; Young, A.H.; Graves, L.; Mahbubur, M.; Brooks, A.; Soomro, M.; Rathod, P.; Phiri, P. Psychological impact of COVID-19 pandemic: Protocol and results of first three weeks from an international cross-section survey—Focus on health professionals. J. Affect. Disord. Rep. 2020, 1, 10005. [Google Scholar] [CrossRef]
- British Medical Association (BMA). COVID-19 Tracker Survey February 2021. Available online: https://www.bma.org.uk/media/3810/bma-covid-tracker-survey-february-2021.pdf (accessed on 16 May 2023).
- Jones, B.A.; Bowe, M.; McNamara, N.; Guerin, E.; Carter, T. Exploring the mental health experiences of young trans and gender diverse people during the COVID-19 pandemic. Int. J. Transgend. Health 2021, 24, 292–304. [Google Scholar] [CrossRef]
- Perez, A.; Panagiotopoulou, E.; Curtis, P.; Roberts, R. Barriers and facilitators to mood and confidence in pregnancy and early parenthood during COVID-19 in the UK: Mixed-methods synthesis survey. B. J. Psych. Open 2021, 7, e107. [Google Scholar] [CrossRef]
- Sideropoulos, V.; Dukes, D.; Hanley, M.; Palikara, O.; Rhodes, S.; Riby, D.M.; Samson, A.C.; Van Herwegen, J. The impact of COVID-19 on anxiety and wellbeing for families of individuals with special education needs and disabilities in the UK. J. Autism Dev. Disord. 2022, 52, 2656–2669. [Google Scholar] [CrossRef]
- Davillas, A.; Jones, A.M. The first wave of the COVID-19 pandemic and its impact on socioeconomic inequality in psychological distress in the UK. Health Econ. 2021, 30, 1668–1683. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Davillas, A.; Jones, A.M. The COVID-19 pandemic and its impact on socioeconomic inequality in psychological distress in the UK: An update. Bonn IZA Inst. Labor Econ. 2021, 14790, 912–920. [Google Scholar] [CrossRef]
- Bu, F.; Bone, J.K.; Mitchell, J.J.; Steptoe, A.; Fancourt, D. Longitudinal changes in physical activity during and after the first national lockdown due to the COVID-19 pandemic in England. Sci. Rep.-UK 2021, 11, 17723. [Google Scholar] [CrossRef] [PubMed]
- Mak, H.W.; Fluharty, M.; Fancourt, D. Predictors and impact of arts engagement during the COVID-19 pandemic: Analyses of data from 19,384 adults in the COVID-19 Social Study. Front. Psychol. 2021, 12, 626263. [Google Scholar] [CrossRef] [PubMed]
- Cowan, K. Understanding People’s Concerns About the Mental Health Impacts of the COVID-19 Pandemic; The Academy of Mental Sciences: London, UK, 2020; Available online: https://acmedsci.ac.uk/file-download/99436893 (accessed on 16 May 2023).
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiat. 2020, 7, 547–560. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.E.; Waite, L.J.; Hawkley, L.C.; Cacioppo, J.T. A short scale for measuring loneliness in large surveys: Results from two population-based studies. Res. Aging 2004, 26, 655–672. [Google Scholar] [CrossRef]
- Department for Culture, Media and Sport. Taking Part 2013/14, Focus on: Art Forms: Statistical Release; DCMS: London, UK, 2015. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/802735/Y10_Art_forms_-_FINAL.pdf (accessed on 16 May 2023).
- Taylor, M. Non-participation or different styles of participation? Alternative interpretations from Taking Part. Cult. Trends 2016, 25, 169–181. [Google Scholar] [CrossRef]
- Taylor, M. Taking Part: The next five years (2016) by the Department for Culture, Media and Sport. Cult. Trends 2016, 25, 291–294. [Google Scholar] [CrossRef]
- Fancourt, D.; Baxter, L. Differential participation in community cultural activities amongst those with poor mental health: Analyses of the UK Taking Part Survey. Soc. Sci. Med. 2020, 261, 113221. [Google Scholar] [CrossRef]
- Department for Culture, Media and Sport. Understanding Society: The UK Household Longitudinal Study; DCMS: London, UK, 2015. Available online: https://www.understandingsociety.ac.uk/2022/06/29/new-government-research-identifies-clear-links-between-loneliness-and-mental-health-distress (accessed on 16 May 2023).
- Fujiwara, D.; Kudrna, L.; Dolan, P. Quantifying and Valuing the Wellbeing Impacts of Culture and Sport; DCMS: London, UK, 2014. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/304899/Quantify-ing_and_valuing_the_wellbeing_impacts_of_sport_and_culture.pdf (accessed on 16 May 2023).
- Tymoszuk, U.; Spiro, N.; Perkins, R.; Mason-Bertrand, A.; Gee, K.; Williamon, A. Arts engagement trends in the United Kingdom and their mental and social wellbeing implications: HEartS Survey. PLoS ONE 2021, 16, e0246078. [Google Scholar] [CrossRef]
- Marmot, M.; Brunner, E. Cohort Profile: The Whitehall II study. Int. J. Epidemiol. 2005, 34, 251–256. [Google Scholar] [CrossRef]
- Tymoszuk, U.; Perkins, R.; Fancourt, D.; Williamon, A. Cross-sectional and longitudinal associations between receptive arts engagement and loneliness among older adults. Soc. Psych. Psych. Epid. 2019, 55, 891–900. [Google Scholar] [CrossRef] [PubMed]
- Department for Culture, Media and Sport. The Culture White Paper; Crown: London, UK, 2016. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/510798/DCMS_The_Culture_White_Paper__3_.pdf (accessed on 22 August 2023).
- Landry, C.; Bianchini, F.; Maguire, M. The Social Impact of the Arts: A Discussion; Comedia: Gloucs, UK, 1995. [Google Scholar]
- Selwood, S. Making a Difference: The Cultural Impact of Museums; Sarah Selwood Associates: London, UK, 2010. Available online: https://www.nationalmuseums.org.uk/media/documents/publications/cultural_impact_final.pdf (accessed on 1 August 2023).
- Partal, A.; Dunphy, K. Cultural impact assessment: A systematic literature review of current methods and practice around the world. Impact Assess. Proj. Apprais. 2016, 34, 1–13. [Google Scholar] [CrossRef]
- Mindell, J.; Ison, E.; Joffe, M. A Glossary for health impact assessment. J. Epidemiol. Community Health 2003, 57, 647–651. [Google Scholar] [CrossRef]
- World Health Organization. Community Engagement: A Health Promotion Guide for Universal Health Coverage in the Hands of the People; WHO: Geneva, Switzerland, 2021; Available online: https://www.who.int/docs/default-source/coronaviruse/mental-health-considerations.pdf (accessed on 22 August 2023).
- Shrestha, T.; Choon, C.V.Y.; Cassarino, M.; Foley, S.; Di Blasi, Z. Factors influencing the effectiveness of nature-based interventions (NBIs) aimed at improving mental health and wellbeing: Protocol of an umbrella review. PLoS ONE 2023, 18, e0273139. [Google Scholar] [CrossRef] [PubMed]
- Deci, E.L.; Ryan, R.M. The ‘what’ and ‘why’ of goal pursuits: Human needs and the self-determination of behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Hodge, A.M.; English, D.R.; Giles, G.G.; Flicker, L. Social connectedness and predictors of successful ageing. Maturitas 2013, 75, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Bannerjee, D.; Rai, M. Social isolation in Covid-19: The impact of loneliness. Int. J. Soc. Psychiatr. 2020, 66, 525–527. [Google Scholar] [CrossRef]
- Perlman, D.; Peplau, L.A. Towards a social psychology of loneliness. In Personal Relationships in Disorder; Duck, S., Gilmore, R., Eds.; Academic Press: London, UK, 1981; pp. 31–56. Available online: file:///C:/Users/ucwelth/Documents/Journal%20Articles/ComCOV_Quant_CultureHealthNature-based_18Nov21/References%20for%20PH%20article/Perlman-Peplau-81.pdf (accessed on 16 May 2023).
- New Economics Foundation. National Accounts of Wellbeing: Bringing Real Wealth onto the Balance Sheet; NEF: London, UK, 2009; Available online: http://www.nationalaccountsofwellbeing.org/learn/download-report.html (accessed on 16 May 2023).
- Lin, H.-F. The role of online and offline features in sustaining virtual communities: An empirical study. Internet Res. 2007, 17, 119–138. [Google Scholar] [CrossRef]
- Ho, C.-I.; Lin, M.-H.; Chen, H.-M. Web users’ behavioral patterns of tourism information search: From online to offline. Tour. Manag. 2012, 33, 1468–1482. [Google Scholar] [CrossRef]
- Office for National Statistics. Measuring Loneliness: Guidance for Use of the National Indicators on Surveys; Office for National Statistics: London, UK, 2018. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/wellbeing/methodologies/measuringlonelinessguidanceforuseofthenationalindicatorsonsurveys (accessed on 1 August 2023).
- Thomson, L.J.; Chatterjee, H.J. Measuring the impact of museum activities on wellbeing: Developing the Museum Wellbeing Measures Toolkit. Mus. Manag. Curatorship 2015, 30, 44–62. [Google Scholar] [CrossRef]
- Thomson, L.J.; Chatterjee, H.J. Assessing well-being outcomes for arts and heritage activities: Development of a Museum Wellbeing Measures Toolkit. J. Appl. Arts Health 2014, 5, 29–50. [Google Scholar] [CrossRef] [PubMed]
- Brace, N.; Kemp, R.; Snelgar, R. SPSS for Psychologists; Macmillan Publishers: Basingstoke, UK, 2009. [Google Scholar]
- Office for National Statistics. 2011 Census; ONS: London, UK, 2011. Available online: https://www.ons.gov.uk/census/2011census (accessed on 16 May 2023).
- Institute for Government. Timeline of UK coronavirus lockdowns, March 2020 to March 2021; IfG: London, UK, 2021; Available online: https://www.instituteforgovernment.org.uk/sites/default/files/timeline-lockdown-web.pdf (accessed on 16 May 2023).
- Natural England. People and Nature Survey: How Has COVID-19 Changed the Way We Engage with Nature? Gov.UK: London, UK, 2022. Available online: https://naturalengland.blog.gov.uk/2022/05/18/people-and-nature-survey-how-has-covid-19-changed-the-way-we-engage-with-nature/ (accessed on 16 May 2023).
- Mak, H.W.; Coulter, R.; Fancourt, D. Patterns of social inequality in arts and cultural participation: Findings from a nationally representative sample of adults living in the United Kingdom of Great Britain and Northern Ireland. Public Health Panor. 2020, 6, 55–68. Available online: https://www.researchgate.net/publication/340284890_Patterns_of_social_inequality_in_arts_and_cultural_participation_Findings_from_a_nationally_representative_sample_of_adults_living_in_the_United_Kingdom_of_Great_Britain_and_Northern_Ireland#fullTextFileContent (accessed on 16 May 2023). [PubMed]
- Lakey, J.; Smith, R.N.; Oskala, A.; McManus, S. Culture, Sport and Wellbeing: Findings from the Understanding Society Adult Survey; Culture and Sport Evidence (CASE): London, UK, 2017. Available online: https://www.understandingsociety.ac.uk/research/publications/524810 (accessed on 16 May 2023).




| Question | Responses | Frequency | Percentage |
|---|---|---|---|
| How often have you taken part in these activities compared with before COVID-19 restrictions? (Please select one) | Much less often | 14 | 4.49% |
| Quite a lot less often | 13 | 4.17% | |
| A little less often | 13 | 4.17% | |
| No change | 13 | 4.17% | |
| A little more often | 66 | 21.15% | |
| Quite a lot more often | 116 | 37.18% | |
| Much more often | 77 | 24.68% | |
| How do you usually take part in these activities? (Please select one) | Offline alone | 130 | 41.67% |
| Offline with other people | 112 | 35.90% | |
| Online alone | 26 | 8.33% | |
| Online with other people | 43 | 13.78% | |
| How much have these activities helped you feel connected with other people? (Please select one) | Not at all | 30 | 9.62% |
| A little | 86 | 27.56% | |
| Around half the time | 60 | 19.23% | |
| Often | 110 | 35.26% | |
| Always | 26 | 8.33% |
| Measurement Scales | Items | Mean (SD) |
|---|---|---|
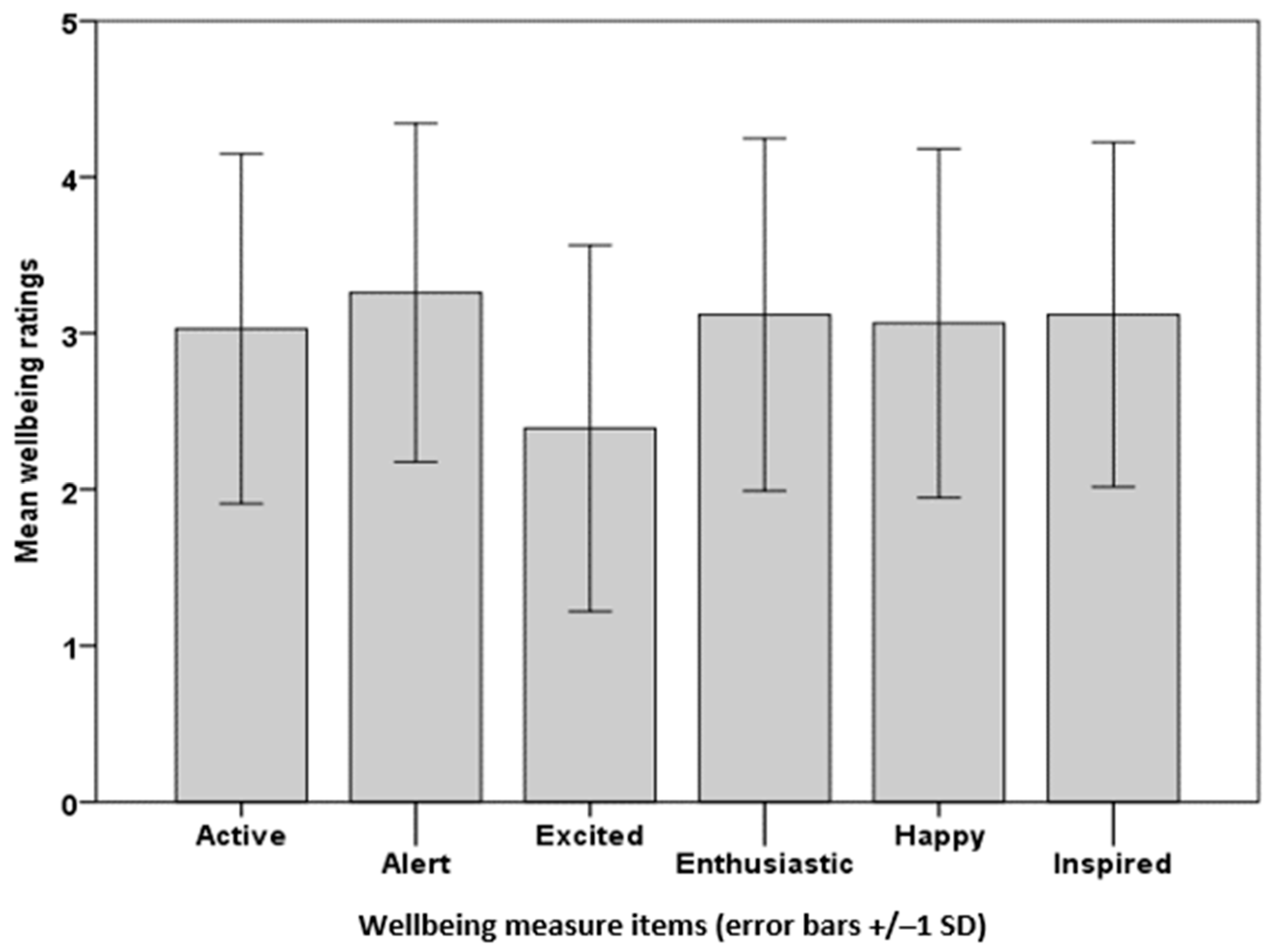
| Please select one box (out of five: 1 = I don’t feel; 2 = I feel a little bit; 3 = I feel fairly; I feel quite a bit;5 = I feel extremely) for each word to indicate how you feel on a typical day. (UCL Museum Wellbeing Measure: range 6–30; total score ≥ 18 indicates high wellbeing) | Active | 3.03 (1.12) |
| Alert | 3.26 (1.08) | |
| Enthusiastic | 3.12 (1.13) | |
| Excited | 2.39 (1.17) | |
| Happy | 3.06 (1.12) | |
| Inspired | 3.12 (1.10) | |
| Total wellbeing (out of 30) | 17.98 (6.72) | |
| Please select one box (out of three: 1 = Hardly ever;2 = Some of the time; 3 = Often) for each question to indicate how you feel on a typical day. (UCLA 3-Item Loneliness Scale: range 3–9; total score ≥ 6 indicates high loneliness) | How often do you feel that you lack companionship? | 1.79 (0.72) |
| How often do you feel isolated from others? | 1.84 (0.68) | |
| How often do you feel left out? | 1.63 (0.72) | |
| Total loneliness (out of 9) | 5.27 (1.80) |
| Predictor Variables | B | Std. Error B | Beta | Sig. |
|---|---|---|---|---|
| Frequency of participation | 0.38 | 0.16 | 0.11 | 0.020 |
| Connectedness score | 1.35 | 0.24 | 0.29 | 0.001 |
| Type of participation—offline or online | −0.12 | 0.63 | −0.01 | 0.979 |
| Type of participation—alone or with others | −0.01 | 0.54 | −0.001 | 0.880 |
| Age range | 0.27 | 0.17 | 0.08 | 0.110 |
| Loneliness score | −1.21 | 0.15 | −0.40 | 0.001 |
| Mean (SD) | Significance | |||
|---|---|---|---|---|
| Loneliness Scale Questions | Community COVID | HEartS Engagement | Two-Tailed Probability | Bonferroni Correction |
| How often do you feel that you lack companionship? | 1.79 (0.72) | 1.66 (0.70) | 0.01 ** | 0.04 * |
| How often do you feel isolated from others? | 1.84 (0.64) | 1.70 (0.72) | 0.02 * | 0.08 |
| How often do you feel left out? | 1.63 (0.72) | 1.65 (0.69) | 0.95 | 3.80 |
| Total loneliness (out of 9) | 5.27 (1.80) | 5.01 (1.88) | 0.90 | 3.60 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thomson, L.J.M.; Spiro, N.; Williamon, A.; Chatterjee, H.J. The Impact of Culture-, Health- and Nature-Based Engagement on Mitigating the Adverse Effects of Public Health Restrictions on Wellbeing, Social Connectedness and Loneliness during COVID-19: Quantitative Evidence from a Smaller- and Larger-Scale UK Survey. Int. J. Environ. Res. Public Health 2023, 20, 6943. https://doi.org/10.3390/ijerph20206943
Thomson LJM, Spiro N, Williamon A, Chatterjee HJ. The Impact of Culture-, Health- and Nature-Based Engagement on Mitigating the Adverse Effects of Public Health Restrictions on Wellbeing, Social Connectedness and Loneliness during COVID-19: Quantitative Evidence from a Smaller- and Larger-Scale UK Survey. International Journal of Environmental Research and Public Health. 2023; 20(20):6943. https://doi.org/10.3390/ijerph20206943
Chicago/Turabian StyleThomson, Linda J. M., Neta Spiro, Aaron Williamon, and Helen J. Chatterjee. 2023. "The Impact of Culture-, Health- and Nature-Based Engagement on Mitigating the Adverse Effects of Public Health Restrictions on Wellbeing, Social Connectedness and Loneliness during COVID-19: Quantitative Evidence from a Smaller- and Larger-Scale UK Survey" International Journal of Environmental Research and Public Health 20, no. 20: 6943. https://doi.org/10.3390/ijerph20206943
APA StyleThomson, L. J. M., Spiro, N., Williamon, A., & Chatterjee, H. J. (2023). The Impact of Culture-, Health- and Nature-Based Engagement on Mitigating the Adverse Effects of Public Health Restrictions on Wellbeing, Social Connectedness and Loneliness during COVID-19: Quantitative Evidence from a Smaller- and Larger-Scale UK Survey. International Journal of Environmental Research and Public Health, 20(20), 6943. https://doi.org/10.3390/ijerph20206943