
The Impact of the First Wave of the COVID-19 Pandemic on University Staff Dietary Behaviours, Sleeping Patterns, and Well-Being: An International Comparison Study

 , , ,
, , ,
Abstract
:1. Introduction
- Dietary behaviour, sleeping patterns, and well-being differed during the first wave of COVID-19 compared to pre-pandemic times;
- Dietary behaviour and sleeping were associated with well-being;
- Differences occurred between the countries involved in the study.
2. Materials and Methods
2.1. Study Design and Settings
2.2. Data Collection and Procedure
2.3. Sampling Technique and Sample Size
2.4. Questionnaire
2.5. Variables and Data Measures
2.5.1. Dietary Behaviours
- ▪
- Changes in emotionally driven food behaviours (i.e., buying and eating more food out of boredom, fear, or anxiety) that were measured using six questions (on a 5-point scale, from “Definitely disagree” to “Definitely agree”).
- ▪
- Changes in food acquisition location (i.e., eating outside the home) were measured using four questions (on a 5-point scale, from “decreased” to “increased”).
- ▪
- Changes in food shopping experience were measured using four items (on a 5-point scale, from “Not at all” to “Very much”).
- ▪
- Changes in fresh food consumption were measured using two questions (on a 5-point scale, from “Definitely don’t agree” to “Definitely agree”).
- ▪
- Changes in consuming food reserves (i.e., eating more canned fruit and vegetables) were measured using four questions (on a 5-point scale, from “Definitely don’t agree” to “Definitely agree”).
- ▪
- Changes in home cooking behaviour were measured using three items (on a 5-point scale, ranging from “decreased” to “increased”).
- ▪
- Changes in skipping meals were assessed using two items (on a 5-point scale, from “Definitely don’t agree” to “Definitely agree”).
2.5.2. Well-Being and Sleep
2.6. Data Analysis
2.7. Missing Data Analysis
3. Results
3.1. Sociodemographic Characteristics of Study Population
3.2. Impact of COVID-19 on Dietary Behaviours, Sleeping Patterns, and Well-Being
3.3. Impact of Dietary Outcomes on Well-Being
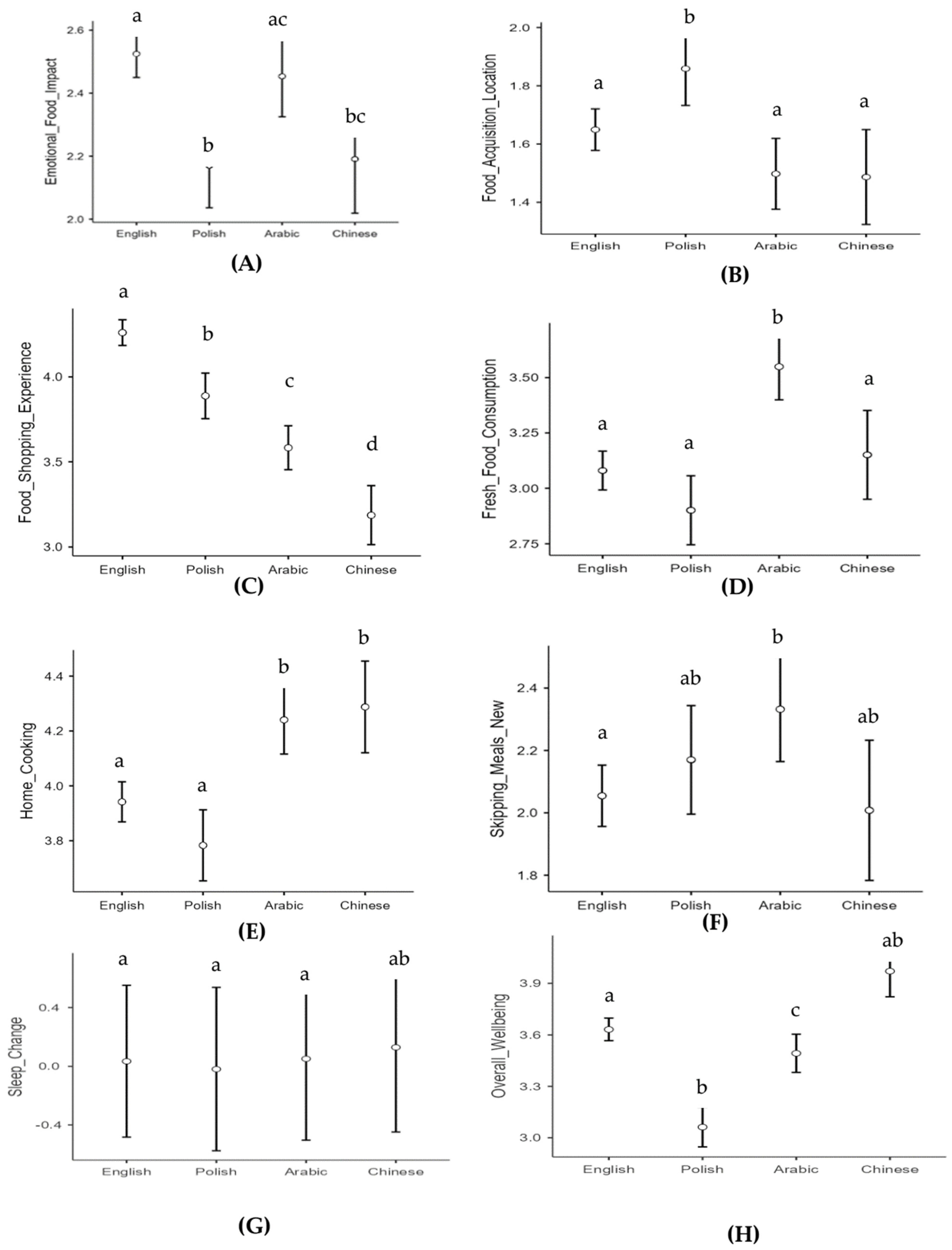
3.4. Impact of Sociodemographic Groups on Findings
3.4.1. Emotionally Driven Food Behaviour
3.4.2. Food Acquisition Location
3.4.3. Food Shopping Experience
3.4.4. Fresh Food Consumption
3.4.5. Consuming Food Reserves
3.4.6. Home Cooking
3.4.7. Skipping Meals
3.4.8. Change in Sleep
3.4.9. Overall Well-Being
4. Discussion
5. Strengths and Limitations
6. Conclusions and Implications for Public Health
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. WHO COVID-19 Dashboard. Available online: https://covid19.who.int (accessed on 22 June 2021).
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef] [PubMed]
- Ingram, J.; Maciejewski, G.; Hand, C.J. Changes in Diet, Sleep, and Physical Activity Are Associated With Differences in Negative Mood During COVID-19 Lockdown. Front. Psychol. 2020, 11, 588604. [Google Scholar] [CrossRef] [PubMed]
- De Sio, S.; Buomprisco, G.; La Torre, G.; Lapteva, E.; Perri, R.; Greco, E.; Mucci, N.; Cedrone, F. The impact of COVID-19 on doctors’ well-being: Results of a web survey during the lockdown in Italy. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 7869–7879. [Google Scholar] [CrossRef]
- Pieh, C.; Budimir, S.; Probst, T. The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (COVID-19) lockdown in Austria. J. Psychosom. Res. 2020, 136, 110186. [Google Scholar] [CrossRef] [PubMed]
- Faghri, P.D.; Dobson, M.; Landsbergis, P.; Schnall, P.L. COVID-19 pandemic: What has work got to do with it? J. Occup. Environ. Med. 2021, 63, e245–e249. [Google Scholar] [CrossRef]
- Rozin, P. The meaning of food in our lives: A cross-cultural perspective on eating and well-being. J. Nutr. Educ. Behav. 2005, 37, S107–S112. [Google Scholar] [CrossRef]
- Boesveldt, S.; Parma, V. The importance of the olfactory system in human well-being, through nutrition and social behavior. Cell Tissue Res. 2021, 383, 559–567. [Google Scholar] [CrossRef]
- Brown, F.C.; Buboltz Jr, W.C.; Soper, B. Relationship of sleep hygiene awareness, sleep hygiene practices, and sleep quality in university students. Behav. Med. 2002, 28, 33–38. [Google Scholar] [CrossRef]
- Odriozola-Gonzalez, P.; Planchuelo-Gomez, A.; Irurtia, M.J.; de Luis-Garcia, R. Psychological effects of the COVID-19 outbreak and lockdown among students and workers of a Spanish university. Psychiatry Res. 2020, 290, 113108. [Google Scholar] [CrossRef]
- Marelli, S.; Castelnuovo, A.; Somma, A.; Castronovo, V.; Mombelli, S.; Bottoni, D.; Leitner, C.; Fossati, A.; Ferini-Strambi, L. Impact of COVID-19 lockdown on sleep quality in university students and administration staff. J. Neurol. 2021, 268, 8–15. [Google Scholar] [CrossRef]
- Alhusseini, N.; Alqahtani, A. COVID-19 pandemic’s impact on eating habits in Saudi Arabia. J. Public Health Res. 2020, 9, jphr-2020. [Google Scholar] [CrossRef] [PubMed]
- Coulthard, H.; Sharps, M.; Cunliffe, L.; van den Tol, A. Eating in the lockdown during the COVID 19 pandemic; self-reported changes in eating behaviour, and associations with BMI, eating style, coping and health anxiety. Appetite 2021, 161, 105082. [Google Scholar] [CrossRef] [PubMed]
- Gornicka, M.; Drywien, M.E.; Zielinska, M.A.; Hamulka, J. Dietary and Lifestyle Changes During COVID-19 and the Subsequent Lockdowns among Polish Adults: A Cross-Sectional Online Survey PLifeCOVID-19 Study. Nutrients 2020, 12, 2324. [Google Scholar] [CrossRef]
- Yang, G.-Y.; Lin, X.-L.; Fang, A.-P.; Zhu, H.-L. Eating Habits and Lifestyles during the Initial Stage of the COVID-19 Lockdown in China: A Cross-Sectional Study. Nutrients 2021, 13, 970. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef]
- Rabiee, E.A. Protocol—Changes in Nutritional Behaviour during COVID-19_V1.2.pdf (Version: 1). Available online: https://osf.io/a23xn/ (accessed on 4 April 2022).
- Rossi, R.; Socci, V.; Pacitti, F.; Di Lorenzo, G.; Di Marco, A.; Siracusano, A.; Rossi, A. Mental health outcomes among frontline and second-line health care workers during the coronavirus disease 2019 (COVID-19) pandemic in Italy. JAMA Netw. Open 2020, 3, e2010185. [Google Scholar] [CrossRef] [PubMed]
- UNSCN. UNSCN COVID-19 Questionnaire, United Nation Standing Committee on Nutrition. Available online: https://docs.google.com/forms/d/e/1FAIpQLScHHxy3YIiphMDQUazAVcSN-gt4zUpf2KAayYaSqseNEgcTqw/viewform?fbzx=6018486058396910573 (accessed on 4 April 2022).
- Van de Velde, S.; Buffel, V.; Bracke, P.; Van Hal, G.; Somogyi, N.M.; Willems, B.; Wouters, E.; C19 ISWS Consortium. The COVID-19 International Student Well-being Study. Scand. J. Public Health 2021, 49, 114–122. [Google Scholar] [CrossRef]
- Tsang, S.; Royse, C.F.; Terkawi, A.S. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J. Anaesth. 2017, 11, S80–S89. [Google Scholar] [CrossRef]
- Catalán, H.E.N. Reliability, population classification and weighting in multidimensional poverty measurement: A Monte Carlo study. Soc. Indic. Res. 2019, 142, 887–910. [Google Scholar] [CrossRef]
- Radloff, L. The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Siddaway, A.P.; Wood, A.M.; Taylor, P.J. The Center for Epidemiologic Studies-Depression (CES-D) scale measures a continuum from well-being to depression: Testing two key predictions of positive clinical psychology. J. Affect Disord. 2017, 213, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Baayen, R.H.; Davidson, D.J.; Bates, D.M. Mixed-effects modeling with crossed random effects for subjects and items. J. Mem. Lang. 2008, 59, 390–412. [Google Scholar] [CrossRef]
- The Jamovi Project (2021). Jamovi (Version 1.8.2) [Windows 10]. Available online: https://www.jamovi.org (accessed on 4 April 2022).
- IBMCorp SPSS Statistics. Statistics for Windows, Version 28.0; IBM Corp: Armonk, NY, USA, 2021. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Cheikh Ismail, L.; Osaili, T.M.; Mohamad, M.N.; Al Marzouqi, A.; Jarrar, A.H.; Abu Jamous, D.O.; Magriplis, E.; Ali, H.I.; Al Sabbah, H.; Hasan, H.; et al. Eating Habits and Lifestyle during COVID-19 Lockdown in the United Arab Emirates: A Cross-Sectional Study. Nutrients 2020, 12, 3314. [Google Scholar] [CrossRef]
- Sidor, A.; Rzymski, P. Dietary Choices and Habits during COVID-19 Lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef] [PubMed]
- Madan, J.; Blonquist, T.; Rao, E.; Marwaha, A.; Mehra, J.; Bharti, R.; Sharma, N.; Samaddar, R.; Pandey, S.; Mah, E.; et al. Effect of COVID-19 Pandemic-Induced Dietary and Lifestyle Changes and Their Associations with Perceived Health Status and Self-Reported Body Weight Changes in India: A Cross-Sectional Survey. Nutrients 2021, 13, 3682. [Google Scholar] [CrossRef]
- Bakhsh, M.A.; Khawandanah, J.; Naaman, R.K.; Alashmali, S. The impact of COVID-19 quarantine on dietary habits and physical activity in Saudi Arabia: A cross-sectional study. BMC Public Health 2021, 21, 1487. [Google Scholar] [CrossRef]
- Gómez-Corona, C.; Ramaroson Rakotosamimanana, V.; Sáenz-Navajas, M.P.; Rodrigues, H.; Franco-Luesma, E.; Saldaña, E.; Valentin, D. To fear the unknown: COVID-19 confinement, fear, and food choice. Food Qual. Prefer. 2021, 92, 104251. [Google Scholar] [CrossRef]
- Crush, J.; Si, Z. COVID-19 Containment and Food Security in the Global South. J. Agric. Food Syst. Community Dev. 2020, 9, 149–151. [Google Scholar] [CrossRef]
- Spence, J.C.; Rhodes, R.E.; McCurdy, A.; Mangan, A.; Hopkins, D.; Mummery, W.K. Determinants of physical activity among adults in the United Kingdom during the COVID-19 pandemic: The DUK-COVID study. Br. J. Health Psychol. 2020, 26, 588–605. [Google Scholar] [CrossRef]
- Hale, T.; Angrist, N.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S. Variation in Government Responses to COVID-19; University of Oxford: Oxford, UK, 2020. [Google Scholar]
- Deschasaux-Tanguy, M.; Druesne-Pecollo, N.; Esseddik, Y.; de Edelenyi, F.S.; Alles, B.; Andreeva, V.A.; Baudry, J.; Charreire, H.; Deschamps, V.; Egnell, M.; et al. Diet and physical activity during the coronavirus disease 2019 (COVID-19) lockdown (March-May 2020): Results from the French NutriNet-Sante cohort study. Am. J. Clin. Nutr. 2021, 113, 924–938. [Google Scholar] [CrossRef]
- Bin Sunaid, F.F.; Al-Jawaldeh, A.; Almutairi, M.W.; Alobaid, R.A.; Alfuraih, T.M.; Bensaidan, F.N.; Alragea, A.S.; Almutairi, L.A.; Duhaim, A.F.; Alsaloom, T.A. Saudi Arabia’s healthy food strategy: Progress & hurdles in the 2030 road. Nutrients 2021, 13, 2130. [Google Scholar] [PubMed]
- Food, S.; Authority, D. Putting Calories on Food Establishments Menu’s Selling Away-From-Home Foods. 2019. Available online: https://eparticipation.my.gov.sa/en/e-consultations/consultations/legal/legal-consultation-24753/ (accessed on 4 April 2022).
- Ben Hassen, T.; El Bilali, H.; Allahyari, M.S. Impact of COVID-19 on Food Behavior and Consumption in Qatar. Sustainability 2020, 12, 6973. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef] [PubMed]
- Bolek, S. Food purchasing, preservation, and eating behavior during COVID-19 pandemic: A consumer analysis. Ital. J. Food Sci. 2021, 33, 14–24. [Google Scholar] [CrossRef]
- Banna, J.C.; Gilliland, B.; Keefe, M.; Zheng, D. Cross-cultural comparison of perspectives on healthy eating among Chinese and American undergraduate students. BMC Public Health 2016, 16, 1015. [Google Scholar] [CrossRef]
- Moynihan, A.B.; van Tilburg, W.A.; Igou, E.R.; Wisman, A.; Donnelly, A.E.; Mulcaire, J.B. Eaten up by boredom: Consuming food to escape awareness of the bored self. Front. Psychol. 2015, 6, 369. [Google Scholar] [CrossRef]
- Lee, G.; Han, K.; Kim, H. Risk of mental health problems in adolescents skipping meals: The Korean National Health and Nutrition Examination Survey 2010 to 2012. Nurs. Outlook 2017, 65, 411–419. [Google Scholar] [CrossRef]
- Debeuf, T.; Verbeken, S.; Van Beveren, M.L.; Michels, N.; Braet, C. Stress and Eating Behavior: A Daily Diary Study in Youngsters. Front. Psychol. 2018, 9, 2657. [Google Scholar] [CrossRef]
- Xiao, H.; Zhang, Y.; Kong, D.; Li, S.; Yang, N. The Effects of Social Support on Sleep Quality of Medical Staff Treating Patients with Coronavirus Disease 2019 (COVID-19) in January and February 2020 in China. Med. Sci. Monit. 2020, 26, e923549. [Google Scholar] [CrossRef]
- Lopez-Bueno, R.; Calatayud, J.; Casana, J.; Casajus, J.A.; Smith, L.; Tully, M.A.; Andersen, L.L.; Lopez-Sanchez, G.F. COVID-19 Confinement and Health Risk Behaviors in Spain. Front. Psychol. 2020, 11, 1426. [Google Scholar] [CrossRef] [PubMed]
- Blog, F. The Impact of COVID-19 On Global Sleep Patterns—Fitbit Blog. Available online: https://blog.fitbit.com/covid-19-sleep-patterns/ (accessed on 20 April 2022).
- Kilani, H.A.; Bataineh, M.F.; Al-Nawayseh, A.; Atiyat, K.; Obeid, O.; Abu-Hilal, M.M.; Mansi, T.; Al-Kilani, M.; Al-Kitani, M.; El-Saleh, M.; et al. Healthy lifestyle behaviors are major predictors of mental wellbeing during COVID-19 pandemic confinement: A study on adult Arabs in higher educational institutions. PLoS ONE 2020, 15, e0243524. [Google Scholar] [CrossRef] [PubMed]
- Killgore, W.D.S.; Taylor, E.C.; Cloonan, S.A.; Dailey, N.S. Psychological resilience during the COVID-19 lockdown. Psychiatry Res. 2020, 291, 113216. [Google Scholar] [CrossRef]
- Oberauer, K. Declarative and procedural working memory: Common principles, common capacity limits? Psychol. Belg. 2010, 50, 277–308. [Google Scholar] [CrossRef]
- DeSimone, J.A.; Harms, P.D.; DeSimone, A.J. Best practice recommendations for data screening. J. Organ. Behav. 2015, 36, 171–181. [Google Scholar] [CrossRef]
- Adler, N.E.; Snibbe, A.C. The role of psychosocial processes in explaining the gradient between socioeconomic status and health. Curr. Dir. Psychol. Sci. 2003, 12, 119–123. [Google Scholar] [CrossRef]
- Adler, N.E.; Epel, E.S.; Castellazzo, G.; Ickovics, J.R. Relationship of subjective and objective social status with psychological and physiological functioning: Preliminary data in healthy, White women. Health Psychol. 2000, 19, 586. [Google Scholar] [CrossRef]
- Wilkinson, R.; Pickett, K. The Spirit Level: Why Greater Equality Makes Societies Stronger; Bloomsbury Publishing: New York, NY, USA, 2011. [Google Scholar]
- Mækelæ, M.J.; Reggev, N.; Dutra, N.; Tamayo, R.M.; Silva-Sobrinho, R.A.; Klevjer, K.; Pfuhl, G. Perceived efficacy of COVID-19 restrictions, reactions and their impact on mental health during the early phase of the outbreak in six countries. R. Soc. Open Sci. 2020, 7, 200644. [Google Scholar] [CrossRef]

{kind=link}
| Variables | N | Mean | Std. Deviation | Missing N (%) | No. of Extremes Low |
|---|---|---|---|---|---|
| Age | 887 | 42.05 | 11.559 | 15 (1.7) | 2 |
| Emotionally driven food behaviour | 856 | 2.4068 | 0.84017 | 46 (5.1) | 0 |
| Food acquisition location | 866 | 1.6459 | 0.79195 | 36 (4.0) | 0 |
| Food shopping experience | 848 | 3.9567 | 0.91336 | 54 (6.0) | 23 |
| Fresh food consumption | 857 | 3.1289 | 0.97006 | 45 (5.0) | 0 |
| Consuming food reserves | 857 | 2.8054 | 0.56850 | 45 (5.0) | 0 |
| Home cooking | 866 | 3.9913 | 0.81580 | 36 (4.0) | 18 |
| Skipping meals | 857 | 2.1219 | 1.09267 | 45 (5.0) | 0 |
| Change in sleep pattern before | 829 | 6.9180 | 1.08816 | 73 (8.1) | 4 |
| Sleep pattern during | 829 | 7.2292 | 1.36664 | 73 (8.1) | 7 |
| Overall well-being | 808 | 3.5380 | 0.76316 | 94 (10.4) | 1 |
| Country | 902 | 0 (0.0) | |||
| Gender | 900 | 2 (0.2) |
| Sociodemographic Characteristics * | UK | Saudi Arabia | China | Poland | p-Value | |
|---|---|---|---|---|---|---|
| Gender | Male | 152 (31.5%) | 78 (46.7%) | 20 (23.3%) | 32 (20.9%) | <0.001 |
| Female | 330 (68.5%) | 89 (53.3%) | 66 (76.7%) | 121 (79.1%) | ||
| Occupation | Teaching staff | 143 (30.8%) | 48 (30.4%) | 15 (18.1%) | 29 (19.5%) | <0.001 |
| Research staff | 22 (4.7%) | 27 (17.1%) | 20 (24.1%) | 24 (16.1%) | ||
| Both teaching and research | 76 (16.4%) | 50 (31.6%) | 38 (45.8%) | 85 (57%) | ||
| Management and administration | 223 (48.1%) | 33 (20.9%) | 10 (12%) | 11 (7.4%) | ||
| Variables | N | Statistic | df | p | Mean Difference | SD | Effect Size (d) |
|---|---|---|---|---|---|---|---|
| Emotionally driven food behaviour | 902 | −20.87 | 901.00 | <0.001 | −0.58 | 0.84 | −0.69 |
| Food acquisition location | 902 | −51.55 | 901.00 | <0.001 | −1.36 | 0.79 | −1.72 |
| Food shopping experience | 902 | 31.70 | 901.00 | <0.001 | 0.96 | 0.91 | 1.06 |
| Fresh food consumption | 902 | 4.53 | 901.00 | <0.001 | 0.15 | 0.98 | 0.15 |
| Consuming food reserves | 902 | −10.18 | 901.00 | <0.001 | −0.19 | 0.57 | −0.34 |
| Home cooking | 902 | 36.61 | 901.00 | <0.001 | 1.00 | 0.82 | 1.22 |
| Skipping meals | 902 | −24.32 | 901.00 | <0.001 | −0.88 | 1.08 | −0.81 |
| Overall well-being | 902 | 21.11 | 901.00 | <0.001 | 0.54 | 0.77 | 0.70 |
| Variables | F | Num df | Den df | p |
|---|---|---|---|---|
| Age | 12.85 | 1 | 871.29 | <0.001 |
| Gender | 0.97 | 3 | 870.47 | 0.407 |
| Emotionally driven food behaviour | 28.36 | 1 | 871.56 | <0.001 |
| Food acquisition location | 0.68 | 1 | 870.42 | 0.411 |
| Food shopping experience | 1.16 | 1 | 872.83 | 0.281 |
| Fresh food consumption | 0.00 | 1 | 870.94 | 0.970 |
| Consuming food reserves | 0.56 | 1 | 870.65 | 0.454 |
| Home cooking | 0.74 | 1 | 871.78 | 0.391 |
| Skipping meals | 43.63 | 1 | 870.61 | <0.001 |
| Change in sleep | 25.49 | 1 | 871.04 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rabiee Khan, F.; Abdelraheim Titi, M.; Frankowska, N.; Kowalczyk, K.; Alziedan, R.; Yin-Kei Lau, C.; Biernat, K.; Brown, K.G. The Impact of the First Wave of the COVID-19 Pandemic on University Staff Dietary Behaviours, Sleeping Patterns, and Well-Being: An International Comparison Study. Int. J. Environ. Res. Public Health 2023, 20, 6941. https://doi.org/10.3390/ijerph20206941
Rabiee Khan F, Abdelraheim Titi M, Frankowska N, Kowalczyk K, Alziedan R, Yin-Kei Lau C, Biernat K, Brown KG. The Impact of the First Wave of the COVID-19 Pandemic on University Staff Dietary Behaviours, Sleeping Patterns, and Well-Being: An International Comparison Study. International Journal of Environmental Research and Public Health. 2023; 20(20):6941. https://doi.org/10.3390/ijerph20206941
Chicago/Turabian StyleRabiee Khan, Fatemeh, Maher Abdelraheim Titi, Natalia Frankowska, Katarzyna Kowalczyk, Rasmieh Alziedan, Christine Yin-Kei Lau, Karolina Biernat, and Kyle Gavin Brown. 2023. "The Impact of the First Wave of the COVID-19 Pandemic on University Staff Dietary Behaviours, Sleeping Patterns, and Well-Being: An International Comparison Study" International Journal of Environmental Research and Public Health 20, no. 20: 6941. https://doi.org/10.3390/ijerph20206941
APA StyleRabiee Khan, F., Abdelraheim Titi, M., Frankowska, N., Kowalczyk, K., Alziedan, R., Yin-Kei Lau, C., Biernat, K., & Brown, K. G. (2023). The Impact of the First Wave of the COVID-19 Pandemic on University Staff Dietary Behaviours, Sleeping Patterns, and Well-Being: An International Comparison Study. International Journal of Environmental Research and Public Health, 20(20), 6941. https://doi.org/10.3390/ijerph20206941