
Nature-Based Interventions in the UK: A Mixed Methods Study Exploring Green Prescribing for Promoting the Mental Wellbeing of Young Pregnant Women



Abstract
:1. Introduction
2. Materials and Methods
2.1. Mapping Survey of Nature-Based Activities
2.2. Qualitative Focus Groups
2.2.1. Young Women
2.2.2. Nature Providers
2.3. Ethics
3. Results
3.1. Mapping Exercise
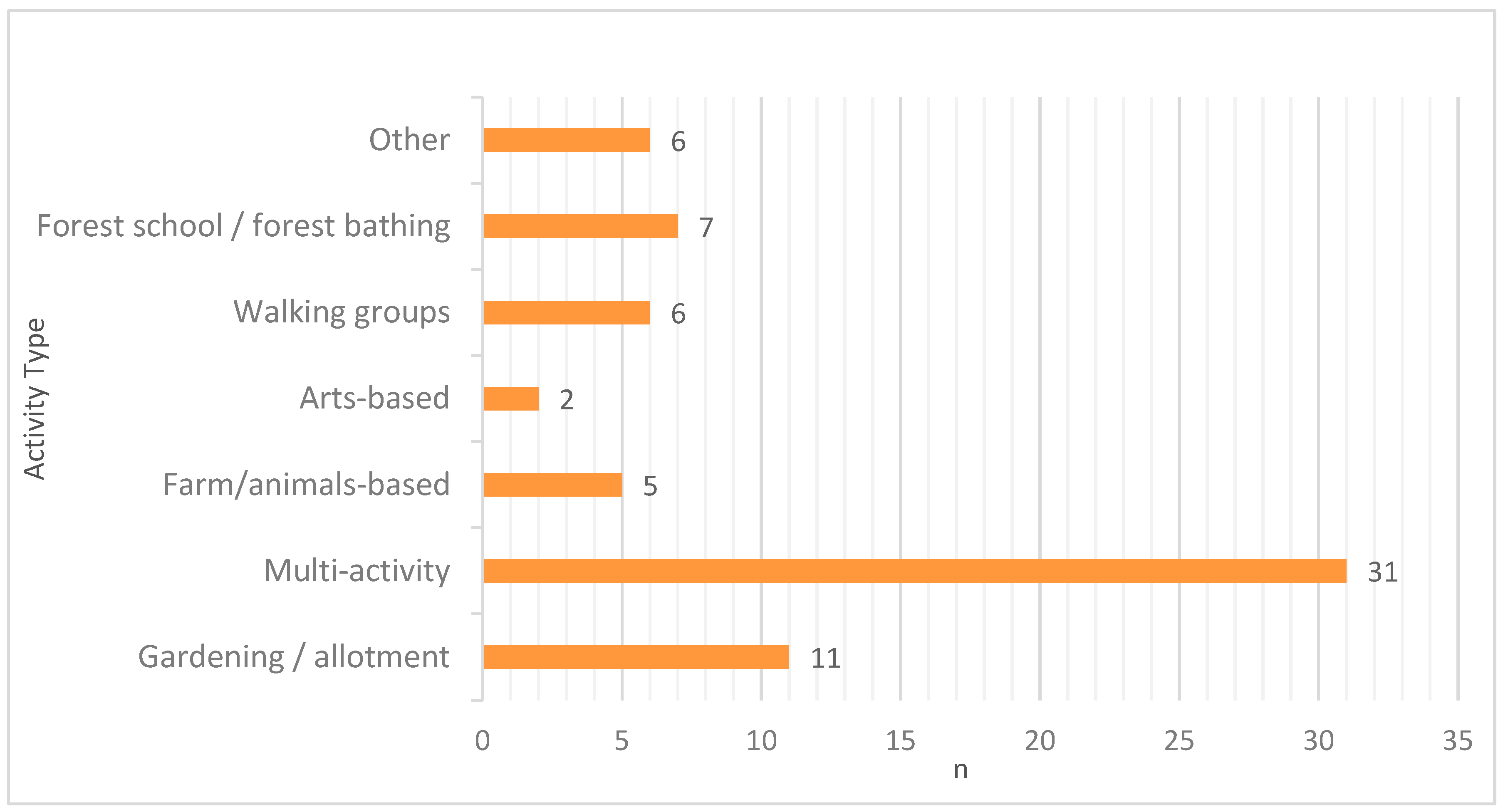
3.1.1. Types of Activity
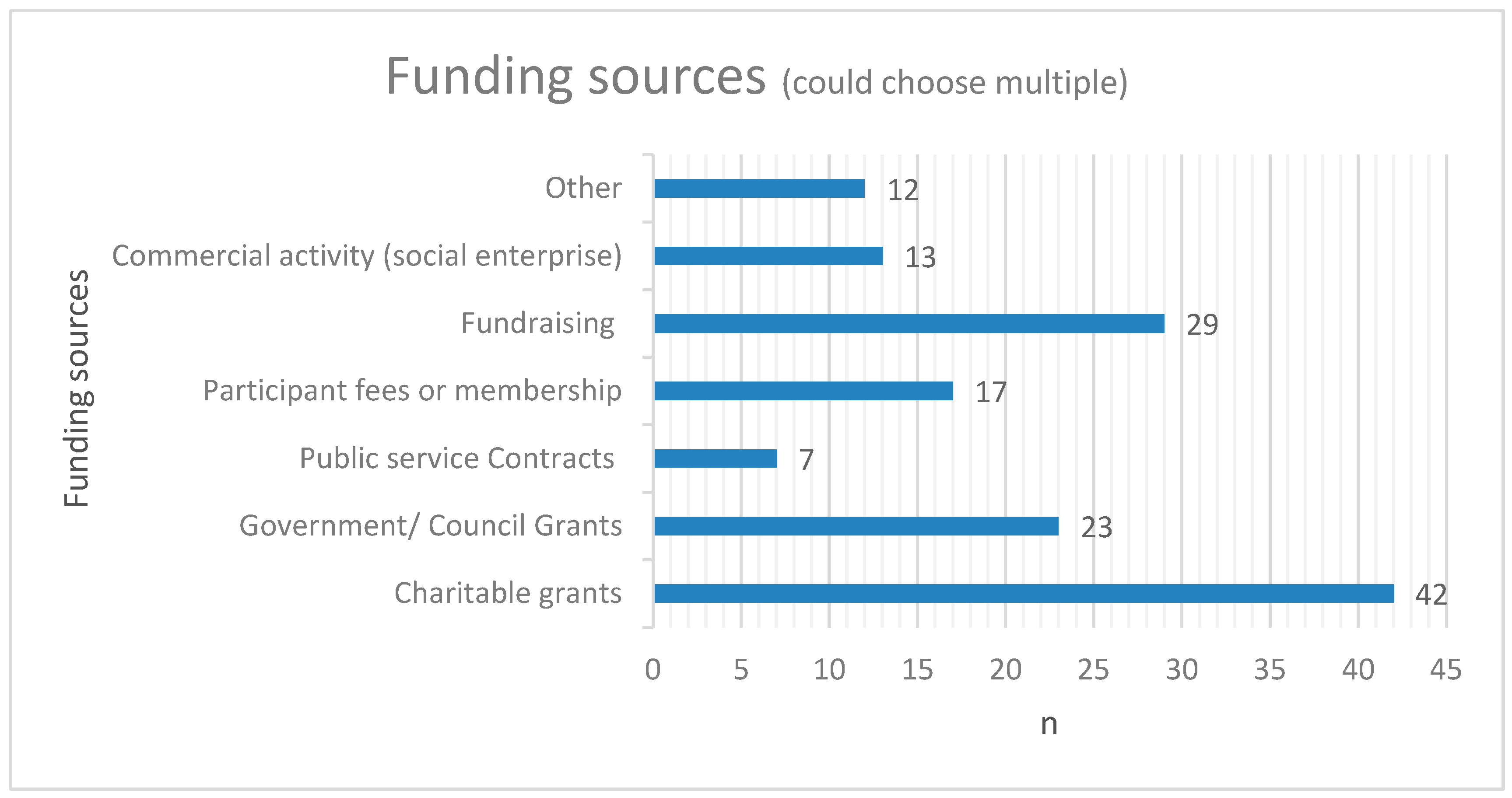
3.1.2. Governance, Evaluation, and Funding
3.1.3. Access and Attendance
3.1.4. Pregnancy and Future Research
3.2. Women’s Focus Groups
3.2.1. Experiences and Perceptions of Nature-Activities
3.2.2. Types of Activities
3.2.3. Perceived Challenges and Solutions
3.3. Provider Focus Groups
3.3.1. Impact of Nature-Based Activities
3.3.2. Barriers and Facilitators to Activity Provision
3.3.3. Experiences of Green Prescribing Systems
3.3.4. Nature-Based Activities and Pregnancy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coventry, P.A.; Brown, J.V.E.; Pervin, J.; Brabyn, S.; Pateman, R.; Breedvelt, J.; Gilbody, S.; Stancliffe, R.; McEachan, R.; White, P.C.L. Nature-based outdoor activities for mental and physical health: Systematic review and meta-analysis. SSM-Popul. Health 2021, 16, 100934. [Google Scholar] [CrossRef]
- Callaghan, A.; McCombe, G.; Harrold, A.; McMeel, C.; Mills, G.; Moore-Cherry, N.; Cullen, W. The impact of green spaces on mental health in urban settings: A scoping review. J. Ment. Health 2021, 2, 179–193. [Google Scholar] [CrossRef] [PubMed]
- White, M.P.; Pahl, S.; Wheeler, B.W.; Depledge, M.H.; Fleming, L.E. Natural environments and subjective wellbeing: Different types of exposure are associated with different aspects of wellbeing. Health Place 2017, 45, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Thomas, F. The role of natural environments within women’s everyday health and wellbeing in Copenhagen, Denmark. Health Place 2015, 35, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, A.; Richardson, M.; Sheffield, D.; McEwan, K. The Relationship Between Nature Connectedness and Eudaimonic Well-Being: A Meta-analysis. J. Happiness Stud. 2020, 21, 1145–1167. [Google Scholar] [CrossRef]
- Mitchell, R.; Popham, F. Effect of exposure to natural environment on health inequalities: An observational population study. Lancet 2008, 372, 1655–1660. [Google Scholar] [CrossRef]
- Müller-Riemenschneider, F.; Petrunoff, N.; Yao, J.; Ng, A.; Sia, A.; Ramiah, A.; Wong, M.; Han, J.; Tai, B.C.; Uijtdewilligen, L. Effectiveness of prescribing physical activity in parks to improve health and wellbeing—The park prescription randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 42. [Google Scholar] [CrossRef]
- Foster, A.; Thompson, J.; Holding, E.; Ariss, S.; Mukuria, C.; Jacques, R.; Akparido, R.; Haywood, A. Impact of social prescribing to address loneliness: A mixed methods evaluation of a national social prescribing programme. Health Soc. Care Community 2021, 29, 1439–1449. [Google Scholar] [CrossRef]
- Kotera, Y.; Richardson, M.; Sheffield, D. Effects of Shinrin-Yoku (Forest Bathing) and Nature Therapy on Mental Health: A Systematic Review and Meta-analysis. Int. J. Ment. Health Addict. 2022, 20, 337–361. [Google Scholar] [CrossRef]
- British Medical Association (BMA). Addressing Unmet Needs in Women’s Mental Health. 2018. Available online: https://www.bma.org.uk/media/2115/bma-womens-mental-health-report-aug-2018.pdf (accessed on 1 September 2023).
- NHS Digital. Adult Psychiatric Morbidity Survey: Survey of Mental Health and Wellbeing, England, 2014. 2016. Available online: https://digital.nhs.uk/catalogue/PUB21748 (accessed on 1 September 2023).
- Howard, L.M.; Khalifeh, H. Perinatal mental health: A review of progress and challenges. World Psychiatry 2020, 19, 313–327. [Google Scholar] [CrossRef]
- Lee, D.T.S.; Chung, T.K.H. Postnatal depression: An update. Best. Pract. Res. Clin. Obstet. Gynaecol. 2007, 21, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Ghimire, U.; Papabathini, S.S.; Kawuki, J.; Obore, N.; Musa, T.A. Depression during pregnancy and the risk of low birth weight, preterm birth and intrauterine growth restriction—An updated meta-analysis. Early Hum. Human. Dev. 2021, 152, 105243. [Google Scholar] [CrossRef] [PubMed]
- Bauer, A.; Knapp, M.; Parsonage, M. Lifetime costs of perinatal anxiety and depression. J. Affect. Disord. 2016, 192, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Netsi, E.; Pearson, R.M.; Murray, L.; Cooper, P.; Craske, M.G.; Stein, A. Association of Persistent and Severe Postnatal Depression With Child Outcomes. JAMA Psychiatry 2018, 75, 247–253. [Google Scholar] [CrossRef]
- Biaggi, A.; Conroy, S.; Pawlby, S.; Pariante, C.M. Identifying the women at risk of antenatal anxiety and depression: A systematic review. J. Affect. Disord. 2016, 191, 62–77. [Google Scholar] [CrossRef]
- Dennis, C.L.; Falah-Hassani, K.; Shiri, R. Prevalence of antenatal and postnatal anxiety: Systematic review and meta-analysis. Br. J. Psychiatry 2017, 210, 315–323. [Google Scholar] [CrossRef]
- Fawcett, E.J.; Fairbrother, N.; Cox, M.L.; White, I.R.; Fawcett, J.M. The Prevalence of Anxiety Disorders During Pregnancy and the Postpartum Period: A Multivariate Bayesian Meta-Analysis. J. Clin. Psychiatry 2019, 80, 18r12527. [Google Scholar] [CrossRef]
- Shorey, S.; Chee, C.Y.; Ng, E.D.; Chan, Y.H.; San Tam, W.W.; Chong, Y.S. Prevalence and incidence of postpartum depression among healthy mothers: A systematic review and meta-analysis. J. Psychiatr. Res. 2018, 104, 235–248. [Google Scholar] [CrossRef]
- Siegel, R.S.; Brandon, A.R. Adolescents, Pregnancy, and Mental Health. J. Pediatr. Adolesc. Gynecol. 2014, 27, 138–150. [Google Scholar] [CrossRef]
- Wong, S.P.W.; Twynstra, J.; Gilliland, J.A.; Cook, J.L.; Seabrook, J.A. Risk Factors and Birth Outcomes Associated with Teenage Pregnancy: A Canadian Sample. J. Pediatr. Adolesc. Gynecol. 2020, 33, 153–159. [Google Scholar] [CrossRef]
- Liu, H.; Ren, H.; Remme, R.P.; Nong, H.; Sui, C. The effect of urban nature exposure on mental health—A case study of Guangzhou. J. Clean. Prod. 2021, 304, 127100. [Google Scholar] [CrossRef]
- McEachan, R.R.C.; Prady, S.L.; Smith, G.; Fairley, L.; Cabieses, B.; Gidlow, C.; Wright, J.; Dadvand, P.; van Gent, D.; Nieuwenhuijsen, M.J. The association between green space and depressive symptoms in pregnant women: Moderating roles of socioeconomic status and physical activity. J. Epidemiol. Community Health 2016, 70, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.Z.; Johnston, J.; Sly, P.D. Green space and early childhood development: A systematic review. Rev. Environ. Health 2020, 35, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Lumber, R.; Richardson, M.; Sheffield, D. Beyond knowing nature: Contact, emotion, compassion, meaning, and beauty are pathways to nature connection. PLoS ONE 2017, 12, e0177186. [Google Scholar] [CrossRef]
- McEwan, K.; Richardson, M.; Sheffield, D.; Ferguson, F.J.; Brindley, P. A smartphone app for improving mental health through connecting with urban nature. Int. J. Environ. Res. Public Health 2019, 16, 3373. [Google Scholar] [CrossRef]
- Greenblatt, M.; Becerra, R.M.; Serafetinides, E.A. Social networks and mental health: An overview. Am. J. Psychiatry 1982, 139, 977–984. [Google Scholar] [CrossRef]
- Anderson, K.; Laxhman, N.; Priebe, S. Can mental health interventions change social networks? A systematic review. BMC Psychiatry 2015, 15, 297. [Google Scholar] [CrossRef]
- Elsenbruch, S.; Benson, S.; Rücke, M.; Rose, M.; Dudenhausen, J.; Pincus-Knackstedt, M.K.; Klapp, B.F.; Arck, P.C. Social support during pregnancy: Effects on maternal depressive symptoms, smoking and pregnancy outcome. Hum. Human. Reprod. 2007, 22, 869–877. [Google Scholar] [CrossRef]
- Morikawa, M.; Okada, T.; Ando, M.; Aleksic, B.; Kunimoto, S.; Nakamura, Y.; Kubota, C.; Uno, Y.; Tamaji, A.; Hayakawa, N.; et al. Relationship between social support during pregnancy and postpartum depressive state: A prospective cohort study. Sci. Rep. 2015, 5, 10520. [Google Scholar] [CrossRef]
- Racine, N.; Madigan, S.; Plamondon, A.; Hetherington, E.; McDonald, S.; Tough, S. Maternal adverse childhood experiences and antepartum risks: The moderating role of social support. Arch. Womens Ment. Health 2018, 21, 663–670. [Google Scholar] [CrossRef]
- Oakley, A.; Hickey, D.; Rajan, L.; Rigby, A.S. Social support in pregnancy: Does it have long-term effects? J. Reprod. Infant. Psychol. 1996, 14, 7–22. [Google Scholar] [CrossRef]
- Grady, M.A.; Bloom, K.C. Pregnancy outcomes of adolescents enrolled in a Centering Pregnancy program. J. Midwifery Womens Health 2004, 49, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Megnin-Viggars, O.; Symington, I.; Howard, L.M.; Pilling, S. Experience of care for mental health problems in the antenatal or postnatal period for women in the UK: A systematic review and meta-synthesis of qualitative research. Arch. Womens Ment. Health 2015, 18, 745–759. [Google Scholar] [CrossRef]
- Price, A.; Janssens, A.; Dunn-Morua, S.; Eke, H.; Asherson, P.; Lloyd, T.; Ford, T. Seven steps to mapping health service provision: Lessons learned from mapping services for adults with Attention-Deficit/Hyperactivity Disorder (ADHD) in the UK. BMC Health Serv. Res. 2019, 19, 468. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef]
- Sandhu, S.; Alderwick, H.; Gottlieb, L. Financing Approaches to Social Prescribing Programs in England and the United States. Milbank Q. 2022, 100, 393–423. [Google Scholar] [CrossRef]
- Husk, K.; Blockley, K.; Lovell, R.; Bethel, A.; Lang, I.; Byng, R.; Garside, R. What approaches to social prescribing work, for whom, and in what circumstances? A realist review. Health Soc. Care Community 2020, 28, 309–324. [Google Scholar] [CrossRef]
- Robinson, J.M.; Breed, M.F. Green Prescriptions and Their Co-Benefits: Integrative Strategies for Public and Environmental Health. Challenges 2019, 10, 9. [Google Scholar] [CrossRef]
- Cooper, M.; Flynn, D.; Avery, L.; Ashley, K.; Jordan, C.; Errington, L.; Scott, J. Service user perspectives on social prescribing services for mental health in the UK: A systematic review. Perspect. Public. Health 2023, 143, 135–144. [Google Scholar] [CrossRef]
- Liebmann, M.; Pitman, A.; Hsueh, Y.C.; Bertotti, M.; Pearce, E. Do people perceive benefits in the use of social prescribing to address loneliness and/or social isolation? A qualitative meta-synthesis of the literature. BMC Health Serv. Res. 2022, 22, 1264. [Google Scholar] [CrossRef]
- Nguyen, P.; Astell-Burt, T.; Rahimi-Ardabili, H.; Feng, X. Effect of nature prescriptions on cardiometabolic and mental health, and physical activity: A systematic review. Lancet Planet. Health 2023, 7, E313–E328. [Google Scholar] [CrossRef] [PubMed]
- Astell-Burt, T.; Hartig, T.; Gusti Ngurah Edi Putra, I.; Walsan, R.; Dendup, T.; Feng, X. Green space and loneliness: A systematic review with theoretical and methodological guidance for future research. Sci. Total Environ. 2022, 847, 157521. [Google Scholar] [CrossRef] [PubMed]
- Razani, N.; Morshed, S.; Kohn, M.A.; Wells, N.M.; Thompson, D.; Alqassari, M.; Agodi, A.; Rutherford, G.W. Effect of park prescriptions with and without group visits to parks on stress reduction in low-income parents: SHINE randomized trial. PLoS ONE 2018, 13, e0192921. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Length of Time Project Established | n (%) | Fee Charging to Attendees | n (%) |
|---|---|---|---|
| <1 year | 9 (13%) | Yes | 13 (19%) |
| 1–2 years | 15 (22%) | No | 37 (54%) |
| 2–5 years | 10 (15%) | Sometimes | 18 (27%) |
| 5–10 years | 11 (16%) | ||
| >10 years | 23 (34%) |
| Number of People Accessing Nature Activity per Year | n (%) | Activity Access Route | n * |
|---|---|---|---|
| 0–49 | 15 (22%) | Via Social/Green Prescribing Link Workers | 38 |
| 50–99 | 15 (22%) | Via other professional referral (e.g., GP, mental health services) | 32 |
| 100–149 | 10 (15%) | Self-referral | 45 |
| 150–199 | 5 (7%) | Informal—just turn up | 40 |
| 200+ | 23 (34%) | Other | 18 |
| Theme | Illustrative Notes |
|---|---|
| Impact of nature-based activities |
|
| Barriers and facilitators to activity provision |
|
| Experiences of green prescribing systems |
|
| Nature-based activities and pregnancy |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sands, G.; Blake, H.; Carter, T.; Spiby, H. Nature-Based Interventions in the UK: A Mixed Methods Study Exploring Green Prescribing for Promoting the Mental Wellbeing of Young Pregnant Women. Int. J. Environ. Res. Public Health 2023, 20, 6921. https://doi.org/10.3390/ijerph20206921
Sands G, Blake H, Carter T, Spiby H. Nature-Based Interventions in the UK: A Mixed Methods Study Exploring Green Prescribing for Promoting the Mental Wellbeing of Young Pregnant Women. International Journal of Environmental Research and Public Health. 2023; 20(20):6921. https://doi.org/10.3390/ijerph20206921
Chicago/Turabian StyleSands, Gina, Holly Blake, Tim Carter, and Helen Spiby. 2023. "Nature-Based Interventions in the UK: A Mixed Methods Study Exploring Green Prescribing for Promoting the Mental Wellbeing of Young Pregnant Women" International Journal of Environmental Research and Public Health 20, no. 20: 6921. https://doi.org/10.3390/ijerph20206921
APA StyleSands, G., Blake, H., Carter, T., & Spiby, H. (2023). Nature-Based Interventions in the UK: A Mixed Methods Study Exploring Green Prescribing for Promoting the Mental Wellbeing of Young Pregnant Women. International Journal of Environmental Research and Public Health, 20(20), 6921. https://doi.org/10.3390/ijerph20206921