
Time Trends in Ischemic Heart Disease Mortality Attributable to PM2.5 Exposure in Southeastern China from 1990 to 2019: An Age-Period-Cohort Analysis

Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Statistical Analyses
3. Results
3.1. Trends in IHD Mortality Attributable to PM2.5 Exposure
3.2. ASMR for IHD Attributable to PM2.5 Exposure
3.3. Net Drift and Local Drift in Age Groups
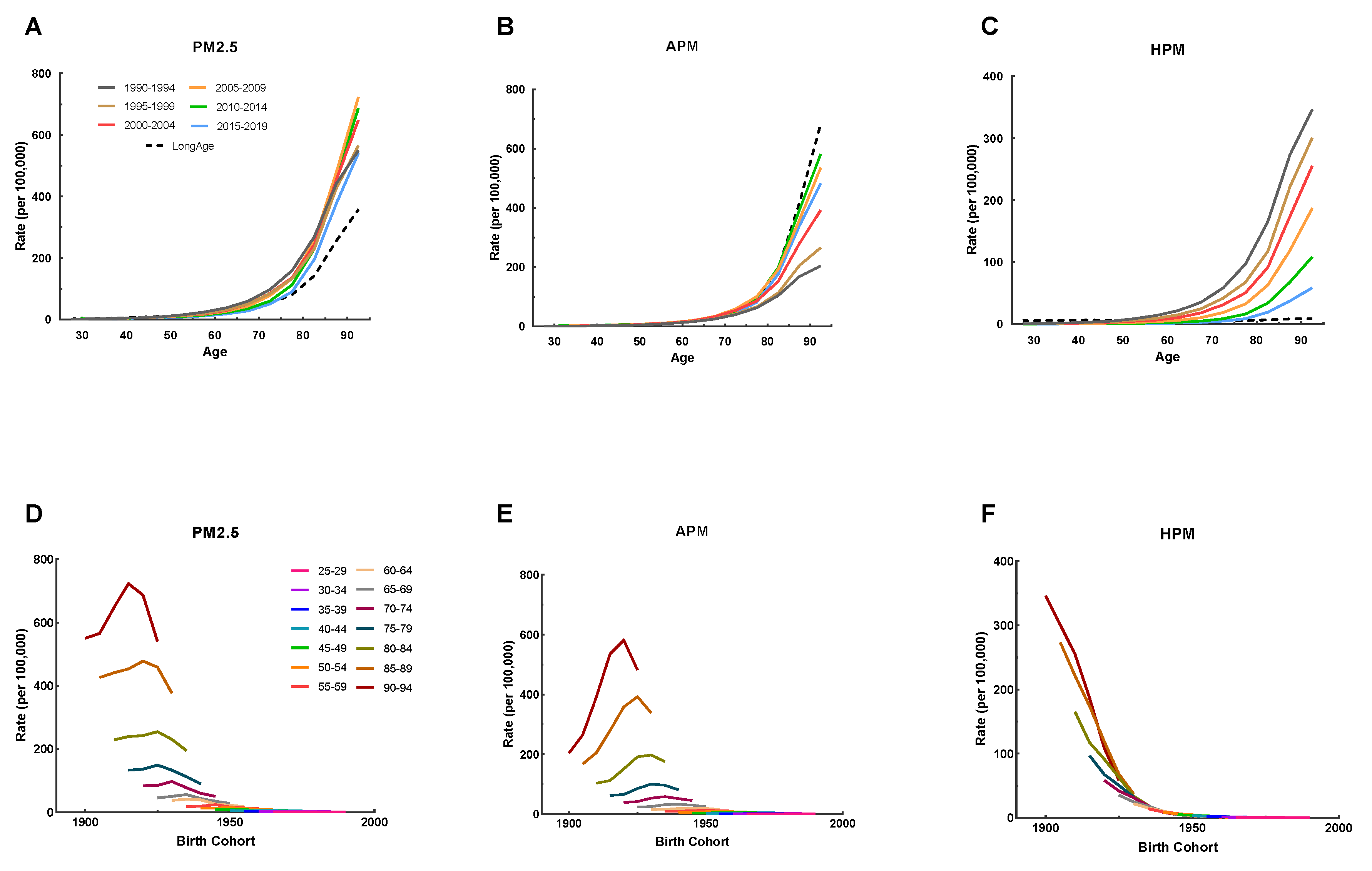
3.4. APC Effects on IHD Mortality Attributable to PM2.5 Exposure
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Wang, L.; Wu, X.; Du, J.; Cao, W.; Sun, S. Global burden of ischemic heart disease attributable to ambient PM2.5 pollution from 1990 to 2017. Chemosphere 2021, 263, 128134. [Google Scholar] [CrossRef]
- Hystad, P.; Duong, M.; Brauer, M.; Larkin, A.; Arku, R.; Kurmi, O.P.; Fan, W.Q.; Avezum, A.; Azam, I.; Chifamba, J.; et al. Health Effects of Household Solid Fuel Use: Findings from 11 Countries within the Prospective Urban and Rural Epidemiology Study. Environ. Health Perspect. 2019, 127, 57003. [Google Scholar] [CrossRef] [PubMed]
- Bu, X.; Xie, Z.; Liu, J.; Wei, L.; Wang, X.; Chen, M.; Ren, H. Global PM2.5-attributable health burden from 1990 to 2017: Estimates from the Global Burden of disease study 2017. Environ. Res. 2021, 197, 111123. [Google Scholar] [CrossRef] [PubMed]
- Institute for Health Metrics and Evaluation (IHME). GBD Results Tool. Available online: http://ghdx.healthdata.org/gbd-results-tool (accessed on 20 November 2022).
- Chen, J.; Hoek, G. Long-term exposure to PM and all-cause and cause-specific mortality: A systematic review and meta-analysis. Environ. Int. 2020, 143, 105974. [Google Scholar] [CrossRef]
- Hystad, P.; Larkin, A.; Rangarajan, S.; AlHabib, K.F.; Avezum, Á.; Calik, K.; Chifamba, J.; Dans, A.; Diaz, R.; du Plessis, J.L.; et al. Associations of outdoor fine particulate air pollution and cardiovascular disease in 157,436 individuals from 21 high-income, middle-income, and low-income countries (PURE): A prospective cohort study. Lancet Planet. Health 2020, 4, e235–e245. [Google Scholar] [CrossRef]
- Huang, J.; Li, G.; Qian, X.; Xu, G.; Zhao, Y.; Huang, J.; Liu, Q.; He, T.; Guo, X. The burden of ischemic heart disease related to ambient air pollution exposure in a coastal city in South China. Environ. Res. 2018, 164, 255–261. [Google Scholar] [CrossRef]
- Yu, W.; Liu, S.; Jiang, J.; Chen, G.; Luo, H.; Fu, Y.; Xie, L.; Li, B.; Li, N.; Chen, S. Burden of ischemic heart disease and stroke attributable to exposure to atmospheric PM2.5 in Hubei province, China. Atmos. Environ. 2019, 221, 117079. [Google Scholar] [CrossRef]
- Alexeeff, S.E.; Liao, N.S.; Liu, X.; Van Den Eeden, S.K.; Sidney, S. Long-Term PM2.5 Exposure and Risks of Ischemic Heart Disease and Stroke Events: Review and Meta-Analysis. J. Am. Heart Assoc. 2021, 10, e016890. [Google Scholar] [CrossRef]
- Burnett, R.; Chen, H.; Szyszkowicz, M.; Fann, N.; Hubbell, B.; Pope, C.A., III; Apte, J.S.; Brauer, M.; Cohen, A.; Weichenthal, S.; et al. Global estimates of mortality associated with long-term exposure to outdoor fine particulate matter. Proc. Natl. Acad. Sci. USA 2018, 115, 9592–9597. [Google Scholar] [CrossRef]
- Xue, T.; Zhu, T.; Zheng, Y.; Liu, J.; Li, X.; Zhang, Q. Change in the number of PM2.5-attributed deaths in China from 2000 to 2010: Comparison between estimations from census-based epidemiology and pre-established exposure-response functions. Environ. Int. 2019, 129, 430–437. [Google Scholar] [CrossRef]
- Vancheri, F.; Tate, A.R.; Henein, M.; Backlund, L.; Donfrancesco, C.; Palmieri, L.; Strender, L.E. Time trends in ischaemic heart disease incidence and mortality over three decades (1990–2019) in 20 Western European countries: Systematic analysis of the Global Burden of Disease Study 2019. Eur. J. Prev. Cardiol. 2022, 29, 396–403. [Google Scholar] [CrossRef]
- Rosenberg, P.S.; Anderson, W.F. Proportional hazards models and age-period-cohort analysis of cancer rates. Stat. Med. 2010, 29, 1228–1238. [Google Scholar] [CrossRef]
- Zhou, M.; Wang, H.; Zeng, X.; Yin, P.; Zhu, J.; Chen, W.; Li, X.; Wang, L.; Wang, L.; Liu, Y.; et al. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 394, 1145–1158. [Google Scholar] [CrossRef]
- Brauer, M.; Freedman, G.; Frostad, J.; van Donkelaar, A.; Martin, R.V.; Dentener, F.; van Dingenen, R.; Estep, K.; Amini, H.; Apte, J.S.; et al. Ambient Air Pollution Exposure Estimation for the Global Burden of Disease 2013. Environ. Sci. Technol. 2016, 50, 79–88. [Google Scholar] [CrossRef]
- Zhao, B.; Zheng, H.; Wang, S.; Smith, K.R.; Lu, X.; Aunan, K.; Gu, Y.; Wang, Y.; Ding, D.; Xing, J.; et al. Change in household fuels dominates the decrease in PM2.5 exposure and premature mortality in China in 2005–2015. Proc. Natl. Acad. Sci. USA 2018, 115, 12401–12406. [Google Scholar] [CrossRef]
- Wang, Z.; Li, C.; Cui, C.; Liu, H.; Cai, B. Cleaner heating choices in northern rural China: Household factors and the dual substitution policy. J. Environ. Manag. 2019, 259, 109433. [Google Scholar] [CrossRef]
- Xie, Y.; Dai, H.; Dong, H.; Hanaoka, T.; Masui, T. Economic Impacts from PM2.5 Pollution-Related Health Effects in China: A Provincial-Level Analysis. Environ. Sci. Technol. 2016, 50, 4836–4843. [Google Scholar] [CrossRef]
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef]
- Meng, W.; Zhong, Q.; Chen, Y.; Shen, H.; Yun, X.; Smith, K.R.; Li, B.; Liu, J.; Wang, X.; Ma, J.; et al. Energy and air pollution benefits of household fuel policies in northern China. Proc. Natl. Acad. Sci. USA 2019, 116, 16773–16780. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Hu, S.; Sang, S.; Luo, L.; Yu, C. Age-Period-Cohort Analysis of Stroke Mortality in China: Data From the Global Burden of Disease Study 2013. Stroke 2017, 48, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Zhu, B.; Zhou, J.; Bi, Y.; Xu, S.; Zhou, B. The epidemiological trends in the burden of lung cancer attributable to PM2.5 exposure in China. BMC Public Health 2021, 21, 737. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Rajagopalan, S.; Pope, C.A., III; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A.; et al. Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the American Heart Association. Circulation 2010, 121, 2331–2378. [Google Scholar] [CrossRef] [PubMed]
- Corlin, L.; Woodin, M.; Hart, J.E.; Simon, M.C.; Gute, D.M.; Stowell, J.; Tucker, K.L.; Durant, J.L.; Brugge, D. Longitudinal associations of long-term exposure to ultrafine particles with blood pressure and systemic inflammation in Puerto Rican adults. Environ. Health 2018, 17, 33. [Google Scholar] [CrossRef]
- Xu, M.; Guo, Y.; Zhang, Y.; Westerdahl, D.; Mo, Y.; Liang, F.; Pan, X. Spatiotemporal analysis of particulate air pollution and ischemic heart disease mortality in Beijing, China. Environ. Health 2014, 13, 109. [Google Scholar] [CrossRef]
- Yang, Y.; Tang, R.; Qiu, H.; Lai, P.C.; Wong, P.; Thach, T.Q.; Allen, R.; Brauer, M.; Tian, L.; Barratt, B. Long term exposure to air pollution and mortality in an elderly cohort in Hong Kong. Environ. Int. 2018, 117, 99–106. [Google Scholar] [CrossRef]
- Yap, J.; Ng, Y.; Yeo, K.K.; Sahlén, A.; Lam, C.; Lee, V.; Ma, S. Particulate air pollution on cardiovascular mortality in the tropics: Impact on the elderly. Environ. Health 2019, 18, 24. [Google Scholar] [CrossRef]
- Cai, S.; Li, Q.; Wang, S.; Chen, J.; Ding, D.; Zhao, B.; Yang, D.; Hao, J. Pollutant emissions from residential combustion and reduction strategies estimated via a village-based emission inventory in Beijing. Environ. Pollut. 2018, 238, 230–237. [Google Scholar] [CrossRef]
- Chuang, H.C.; Ho, K.F.; Lin, L.Y.; Chang, T.Y.; Hong, G.B.; Ma, C.M.; Liu, I.J.; Chuang, K.J. Long-term indoor air conditioner filtration and cardiovascular health: A randomized crossover intervention study. Environ. Int. 2017, 106, 91–96. [Google Scholar] [CrossRef]
- Wang, Z.; Pei, J.; Zhang, J.S. Experimental investigation of the formaldehyde removal mechanisms in a dynamic botanical filtration system for indoor air purification. J. Hazard. Mater. 2014, 280, 235–243. [Google Scholar] [CrossRef]
- Liu, J.; Han, Y.; Tang, X.; Zhu, J.; Zhu, T. Estimating adult mortality attributable to PM2.5 exposure in China with assimilated PM2.5 concentrations based on a ground monitoring network. Sci. Total Environ. 2016, 568, 1253–1262. [Google Scholar] [CrossRef]
- Huang, J.; Pan, X.; Guo, X.; Li, G. Health impact of China’s Air Pollution Prevention and Control Action Plan: An analysis of national air quality monitoring and mortality data. Lancet Planet. Health 2018, 2, e313–e323. [Google Scholar] [CrossRef]
- Yang, X.; Wang, Y.; Chen, D.; Tan, X.; Tian, X.; Shi, L. Does the “Blue Sky Defense War Policy” Paint the Sky Blue?—A Case Study of Beijing-Tianjin-Hebei Region, China. Int. J. Environ. Res. Public Health 2021, 18, 12397. [Google Scholar] [CrossRef]
- Kampa, M.; Castanas, E. Human health effects of air pollution. Environ. Pollut. 2008, 151, 362–367. [Google Scholar] [CrossRef]
- World Health Organization, Regional Office for the Western Pacific. The Bill China Cannot Afford: Health, Economic and Social Costs of China’s Tobacco Epidemic. Manila, Philippines: WHO Regional Office for the Western Pacific. 2017. Available online: https://apps.who.int/iris/handle/10665/255469 (accessed on 20 November 2022).
- Jiangsu Provincial People’s Government. Available online: http://www.jiangsu.gov.cn/art/2018/2/5/art_60037_7479480.html (accessed on 20 November 2022).
- Jiangsu Commission of Health. Available online: http://wjw.jiangsu.gov.cn/art/2017/2/10/art_49495_6030604.html (accessed on 20 November 2022).
- Liu, S.; Li, Y.; Zeng, X.; Wang, H.; Yin, P.; Wang, L.; Liu, Y.; Liu, J.; Qi, J.; Ran, S.; et al. Burden of Cardiovascular Diseases in China, 1990–2016: Findings From the 2016 Global Burden of Disease Study. JAMA Cardiol. 2019, 4, 342–352. [Google Scholar] [CrossRef]
- Zhao, Y.F.; Zhang, T.; Wang, Z.Q.; Chen, X.R.; Wang, C.X.; Qi, J.L.; Yang, J.; Wu, J.; Zhou, M.G. Burden of cardiovascular disease from 1990 to 2017 in Henan Province, China. Glob. Health Action 2021, 14, 1959708. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Sex | PM2.5 Exposure | APM Exposure | HPM Exposure | ||||||
|---|---|---|---|---|---|---|---|---|---|
| ASMR (1990) (95%UI) | ASMR (2019) (95%UI) | AAPC% (95%CI) | ASMR (1990) (95%UI) | ASMR (2019) (95%UI) | AAPC% (95%CI) | ASMR (1990) (95%UI) | ASMR (2019) (95%UI) | AAPC% (95%CI) | |
| Both | 18.90 (15.55~23.33) | 11.53 (9.12~14.90) | −1.71 a (−2.02~−1.40) | 6.84 (3.36~11.44) | 10.57 (8.24~13.83) | 1.45 a (1.18~1.72) | 12.06 (7.99~16.22) | 0.96 (0.33~2.16) | −8.27 a (−8.84~−7.69) |
| Male | 23.32 (18.80~29.66) | 15.81 (11.98~20.81) | −1.44 a (−1.93~−0.95) | 9.61 (4.61~15.82) | 14.73 (11.10~19.32) | 1.38 (0.90~1.86) | 13.71 (8.10~19.73) | 1.08 (0.36~2.59) | −8.29 a (−8.64~−7.94) |
| Female | 15.55 (12.01~20.10) | 8.64 (6.24~12.86) | −2.06 a (−2.26~−1.85) | 4.89 (2.37~8.56) | 7.77 (5.56~11.66) | 1.57 a (1.33~1.81) | 10.66 (7.13~14.73) | 0.87 (0.31~1.89) | −8.20 a (−8.74~−7.65) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, W.; Zhou, N.; Yu, H.; Yang, H.; Zhou, J.; Hong, X. Time Trends in Ischemic Heart Disease Mortality Attributable to PM2.5 Exposure in Southeastern China from 1990 to 2019: An Age-Period-Cohort Analysis. Int. J. Environ. Res. Public Health 2023, 20, 973. https://doi.org/10.3390/ijerph20020973
Wang W, Zhou N, Yu H, Yang H, Zhou J, Hong X. Time Trends in Ischemic Heart Disease Mortality Attributable to PM2.5 Exposure in Southeastern China from 1990 to 2019: An Age-Period-Cohort Analysis. International Journal of Environmental Research and Public Health. 2023; 20(2):973. https://doi.org/10.3390/ijerph20020973
Chicago/Turabian StyleWang, Weiwei, Nan Zhou, Hao Yu, Huafeng Yang, Jinyi Zhou, and Xin Hong. 2023. "Time Trends in Ischemic Heart Disease Mortality Attributable to PM2.5 Exposure in Southeastern China from 1990 to 2019: An Age-Period-Cohort Analysis" International Journal of Environmental Research and Public Health 20, no. 2: 973. https://doi.org/10.3390/ijerph20020973
APA StyleWang, W., Zhou, N., Yu, H., Yang, H., Zhou, J., & Hong, X. (2023). Time Trends in Ischemic Heart Disease Mortality Attributable to PM2.5 Exposure in Southeastern China from 1990 to 2019: An Age-Period-Cohort Analysis. International Journal of Environmental Research and Public Health, 20(2), 973. https://doi.org/10.3390/ijerph20020973