
Inconsistent Association between Perceived Air Quality and Self-Reported Respiratory Symptoms: A Pilot Study and Implications for Environmental Health Studies




Abstract
1. Introduction
2. Materials and Methods
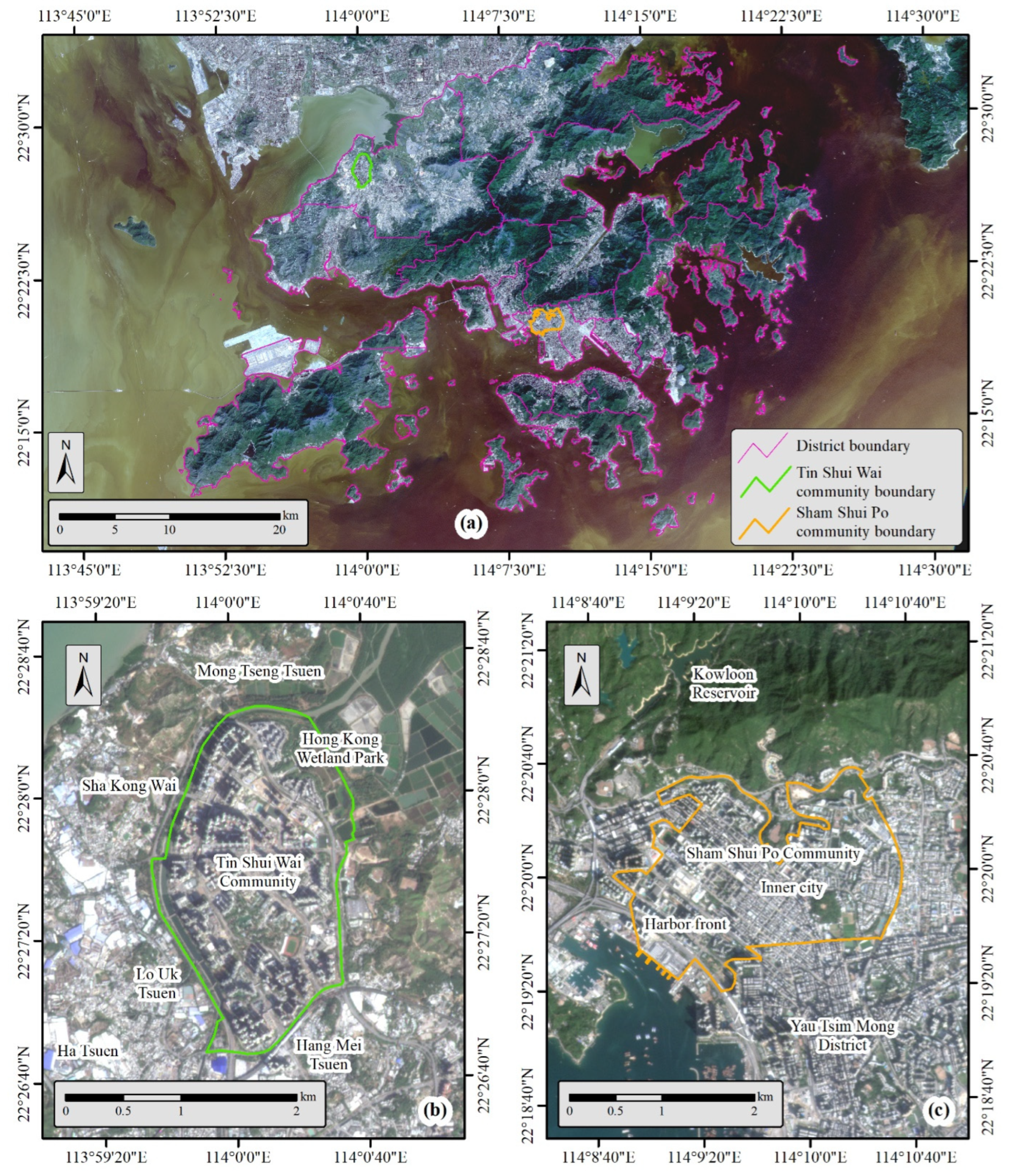
2.1. Survey Area and Study Population
2.2. Questionnaire Design and Data Collection
2.3. Statistical Analysis
3. Results
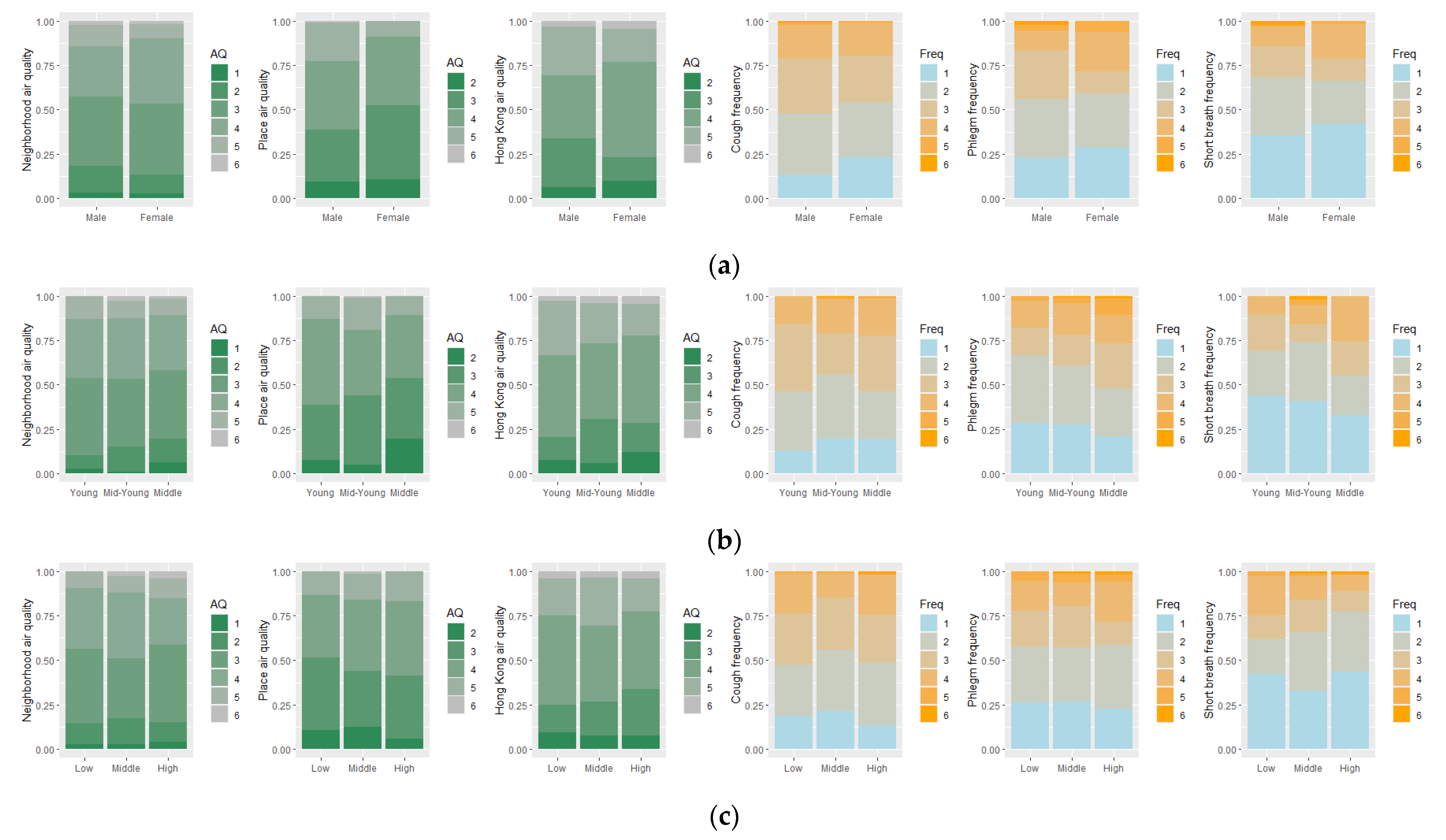
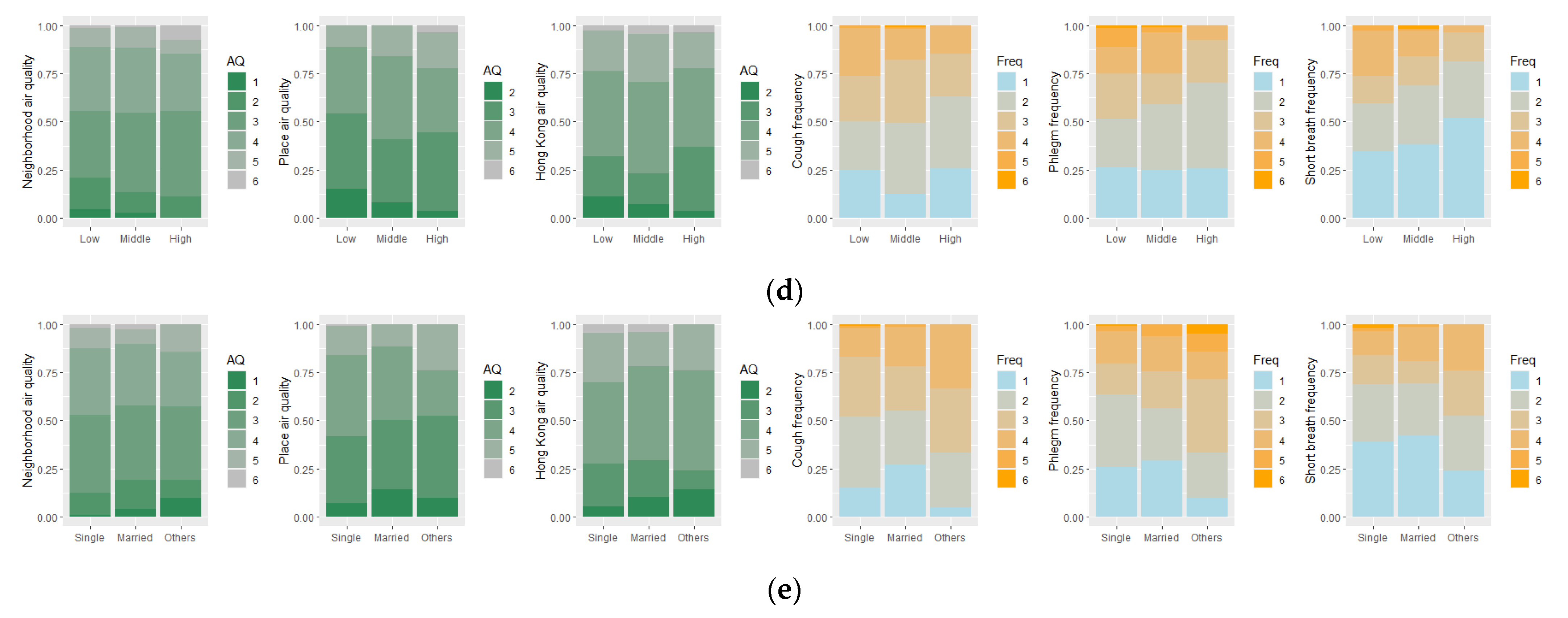
3.1. Descriptive Analyses of the Collected Data
3.2. Overall Associations between People’s Perceived Air Quality and Their Self-Reported Frequency of Respiratory Symptoms
3.3. Disparities in Associations between Different Socio-Demographic Groups
3.4. Disparities in Associations between Different Geographic Contexts
3.5. Predicting the Frequency of Respiratory Symptoms Using People’s Perceived Air Quality
4. Discussion
4.1. Interpretation of the Study Results
4.2. Implications for Environmental Justice Studies
4.3. Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, S.; Chiu, M.; Ho, K.; Zou, S.; Wang, X. Volatile organic compounds (VOCs) in urban atmosphere of Hong Kong. Chemosphere 2002, 48, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Brimblecombe, P. Trends in secondary inorganic particles in Hong Kong, 1995–2020. Atmos. Environ. 2022, 268, 118801. [Google Scholar] [CrossRef]
- Fang, X.; Fan, Q.; Liao, Z.; Xie, J.; Xu, X.; Fan, S. Spatial-temporal characteristics of the air quality in the Guangdong–Hong Kong–Macau Greater Bay Area of China during 2015–2017. Atmos. Environ. 2019, 210, 14–34. [Google Scholar] [CrossRef]
- Manisalidis, I.; Stavropoulou, E.; Stavropoulos, A.; Bezirtzoglou, E. Environmental and health impacts of air pollution: A review. Front. Public Health 2020, 8, 14. [Google Scholar] [CrossRef]
- Bakolis, I.; Hammoud, R.; Stewart, R.; Beevers, S.; Dajnak, D.; MacCrimmon, S.; Broadbent, M.; Pritchard, M.; Shiode, N.; Fecht, D. Mental health consequences of urban air pollution: Prospective population-based longitudinal survey. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 1587–1599. [Google Scholar] [CrossRef] [PubMed]
- Tao, Y.; Kou, L.; Chai, Y.; Kwan, M.-P. Associations of co-exposures to air pollution and noise with psychological stress in space and time: A case study in Beijing, China. Environ. Res. 2021, 196, 110399. [Google Scholar] [CrossRef]
- Meng, Y.; Wong, M.S.; Kwan, M.-P.; Zhu, R. Association between Global Air Pollution and COVID-19 Mortality: A Study of Forty-Six Cities in the World. Ann. Am. Assoc. Geogr. 2022, 112, 1777–1793. [Google Scholar] [CrossRef]
- Lan, G.-L.; Yuan, Z.-K.; Maddock, J.E.; Cook, A.; Chu, Y.-Y.; Pan, B.-B.; Tu, H.; Fan, S.; Liao, X.; Lu, Y. Public perception of air pollution and health effects in Nanchang, China. Air Qual. Atmos. Health 2016, 9, 951–959. [Google Scholar] [CrossRef]
- Zárate Valencia, A.R.; Reyes Umaña, M.; Arellano Wences, H.J.; Rodríguez Rosales, A.A.; Rodríguez Alviso, C.; González González, J. The air quality perception of residents in the metropolitan zone of acapulco who live around intersections with intense traffic. Environments 2020, 7, 21. [Google Scholar] [CrossRef]
- Al-Shidi, H.K.; Ambusaidi, A.K.; Sulaiman, H. Public awareness, perceptions and attitudes on air pollution and its health effects in Muscat, Oman. J. Air Waste Manag. Assoc. 2021, 71, 1159–1174. [Google Scholar] [CrossRef]
- Zhao, Q.; Yao, W.; Zhang, C.; Wang, X.; Wang, Y. Study on the influence of fog and haze on solar radiation based on scattering-weakening effect. Renew. Energy 2019, 134, 178–185. [Google Scholar] [CrossRef]
- Hofflinger, Á.; Boso, À.; Oltra, C. The home halo effect: How air quality perception is influenced by place attachment. Hum. Ecol. 2019, 47, 589–600. [Google Scholar] [CrossRef]
- Kampa, M.; Castanas, E. Human health effects of air pollution. Environ. Pollut. 2008, 151, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Cori, L.; Donzelli, G.; Gorini, F.; Bianchi, F.; Curzio, O. Risk perception of air pollution: A systematic review focused on particulate matter exposure. Int. J. Environ. Res. Public Health 2020, 17, 6424. [Google Scholar] [CrossRef] [PubMed]
- Pantavou, K.; Lykoudis, S.; Psiloglou, B. Air quality perception of pedestrians in an urban outdoor Mediterranean environment: A field survey approach. Sci. Total Environ. 2017, 574, 663–670. [Google Scholar] [CrossRef]
- Zakaria, M.; Ezani, E.; Hassan, N.; Ramli, N.; Wahab, M. Traffic-related air pollution (TRAP), air quality perception and respiratory health symptoms of active commuters in a university outdoor environment. In Proceedings of the IOP Conference Series: Earth and Environmental Science, Moscow, Russia, 27 May–6 June 2019; p. 012017. [Google Scholar]
- Shi, X.; Li, X.; Chen, X.; Zhang, L. Objective air quality index versus subjective perception: Which has a greater impact on life satisfaction? Environ. Dev. Sustain. 2021, 24, 6860–6877. [Google Scholar] [CrossRef]
- Jerrett, M.; Burnett, R.T.; Kanaroglou, P.; Eyles, J.; Finkelstein, N.; Giovis, C.; Brook, J.R. A GIS—Environmental justice analysis of particulate air pollution in Hamilton, Canada. Environ. Plan. A 2001, 33, 955–973. [Google Scholar] [CrossRef]
- Tsui, J.K.-Y.; Guenther, A.; Yip, W.-K.; Chen, F. A biogenic volatile organic compound emission inventory for Hong Kong. Atmos. Environ. 2009, 43, 6442–6448. [Google Scholar] [CrossRef]
- Johnston, J.E.; Juarez, Z.; Navarro, S.; Hernandez, A.; Gutschow, W. Youth engaged participatory air monitoring: A ‘day in the life’in urban environmental justice communities. Int. J. Environ. Res. Public Health 2020, 17, 93. [Google Scholar] [CrossRef]
- Shan, S.; Ju, X.; Wei, Y.; Wang, Z. Effects of PM2. 5 on People’s Emotion: A Case Study of Weibo (Chinese Twitter) in Beijing. Int. J. Environ. Res. Public Health 2021, 18, 5422. [Google Scholar] [CrossRef]
- Wang, S.; Paul, M.J.; Dredze, M. Social media as a sensor of air quality and public response in China. J. Med. Internet Res. 2015, 17, e22. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Lachlan, K.A.; Spence, P.R. Exploring extreme events on social media: A comparison of user reposting/retweeting behaviors on Twitter and Weibo. Comput. Hum. Behav. 2016, 65, 576–581. [Google Scholar] [CrossRef]
- Jiang, W.; Wang, Y.; Tsou, M.-H.; Fu, X. Using social media to detect outdoor air pollution and monitor air quality index (AQI): A geo-targeted spatiotemporal analysis framework with Sina Weibo (Chinese Twitter). PLoS ONE 2015, 10, e0141185. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Liu, F.; Lu, Y.; Mao, Z.; Lu, H.; Wu, Y.; Chu, Y.; Yu, L.; Liu, Y.; Ren, M. Factors affecting parent’s perception on air quality—From the individual to the community level. Int. J. Environ. Res. Public Health 2016, 13, 493. [Google Scholar] [CrossRef]
- Ban, J.; Zhou, L.; Zhang, Y.; Anderson, G.B.; Li, T. The health policy implications of individual adaptive behavior responses to smog pollution in urban China. Environ. Int. 2017, 106, 144–152. [Google Scholar] [CrossRef]
- Cisneros, R.; Brown, P.; Cameron, L.; Gaab, E.; Gonzalez, M.; Ramondt, S.; Veloz, D.; Song, A.; Schweizer, D. Understanding public views about air quality and air pollution sources in the San Joaquin Valley, California. J. Environ. Public Health 2017, 2017, 453514. [Google Scholar] [CrossRef]
- King, K.E. Chicago residents’ perceptions of air quality: Objective pollution, the built environment, and neighborhood stigma theory. Popul. Environ. 2015, 37, 1–21. [Google Scholar] [CrossRef]
- Gouveia, N.; Fletcher, T. Time series analysis of air pollution and mortality: Effects by cause, age and socioeconomic status. J. Epidemiol. Community Health 2000, 54, 750–755. [Google Scholar] [CrossRef]
- Kwok, C.Y.T.; Wong, M.S.; Chan, K.L.; Kwan, M.-P.; Nichol, J.E.; Liu, C.H.; Wong, J.Y.H.; Wai, A.K.C.; Chan, L.W.C.; Xu, Y. Spatial analysis of the impact of urban geometry and socio-demographic characteristics on COVID-19, a study in Hong Kong. Sci. Total Environ. 2021, 764, 144455. [Google Scholar] [CrossRef]
- Huang, J.; Kwan, M.-P. Examining the Influence of Housing Conditions and Daily Greenspace Exposure on People’s Perceived COVID-19 Risk and Distress. Int. J. Environ. Res. Public Health 2022, 19, 8876. [Google Scholar] [CrossRef]
- Kan, Z.; Kwan, M.-P.; Ng, M.K.; Tieben, H. The Impacts of Housing Characteristics and Built-Environment Features on Mental Health. Int. J. Environ. Res. Public Health 2022, 19, 5143. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Wong, M.S.; Kwan, M.P.; Nichol, J.E.; Zhu, R.; Heo, J.; Chan, P.W.; Chin, D.C.; Kwok, C.Y.T.; Kan, Z. COVID-19 Infection and Mortality: Association with PM2. 5 Concentration and Population Density—An Exploratory Study. ISPRS Int. J. Geo-Inf. 2021, 10, 123. [Google Scholar] [CrossRef]
- Schönbrodt, F.D.; Perugini, M. At what sample size do correlations stabilize? J. Res. Personal. 2013, 47, 609–612. [Google Scholar] [CrossRef]
- Kwan, M.P. Gender differences in space-time constraints. Area 2000, 32, 145–156. [Google Scholar] [CrossRef]
- Lo, A.-T.; Houston, D. How do compact, accessible, and walkable communities promote gender equality in spatial behavior? J. Transp. Geogr. 2018, 68, 42–54. [Google Scholar] [CrossRef]
- Loo, B.P.; Lam, W. A multilevel investigation of differential individual mobility of working couples with children: A case study of Hong Kong. Transp. A Transp. Sci. 2013, 9, 629–652. [Google Scholar] [CrossRef]
- Carvalho-Oliveira, R.; Amato-Lourenço, L.F.; Almeida, P.S.; Garcia, B.B.; Vieira, W.K.; Santana, A.; Godinho-Netto, M.C.M.; Carretero, M.E.; Saldiva, P.H.N.; Mauad, T. Effects of long-standing exposure to heavy-duty diesel vehicle traffic on respiratory symptoms and airway inflammation in older adults. Environ. Pollut. 2021, 268, 115893. [Google Scholar] [CrossRef]
- Kwan, M.-P. The stationarity bias in research on the environmental determinants of health. Health Place 2021, 70, 102609. [Google Scholar] [CrossRef]
- Kwan, M.-P. The uncertain geographic context problem. Ann. Assoc. Am. Geogr. 2012, 102, 958–968. [Google Scholar] [CrossRef]
- Mah, A. Environmental justice in the age of big data: Challenging toxic blind spots of voice, speed, and expertise. Environ. Sociol. 2017, 3, 122–133. [Google Scholar] [CrossRef]
- Bullard, R.D. The Quest for Environmental Justice: Human Rights and the Politics of Pollution; Sierra Club Books San Francisco: San Francisco, CA, USA, 2005; Volume 19. [Google Scholar]
- Taylor, D. Toxic Communities; New York University Press: New York, NY, USA, 2014. [Google Scholar]
- Boone, C.G.; Fragkias, M.; Buckley, G.L.; Grove, J.M. A long view of polluting industry and environmental justice in Baltimore. Cities 2014, 36, 41–49. [Google Scholar] [CrossRef]
- Schlosberg, D. Reconceiving environmental justice: Global movements and political theories. Environ. Politics 2004, 13, 517–540. [Google Scholar] [CrossRef]
- Gabrys, J. Programming environments: Environmentality and citizen sensing in the smart city. Environ. Plan. D Soc. Space 2014, 32, 30–48. [Google Scholar] [CrossRef]
- English, P.B.; Richardson, M.J.; Garzón-Galvis, C. From crowdsourcing to extreme citizen science: Participatory research for environmental health. Annu. Rev. Public Health 2018, 39, 335–350. [Google Scholar] [CrossRef]
- Yan, L.; Duarte, F.; Wang, D.; Zheng, S.; Ratti, C. Exploring the effect of air pollution on social activity in China using geotagged social media check-in data. Cities 2019, 91, 116–125. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Socio-Demographic Characteristics | SSP (Old Town) | TSW (New Town) | Both | ||||
|---|---|---|---|---|---|---|---|
| Sample | Census Statistics | Sample | Census Statistics | Sample | Census Statistics | ||
| Gender | Male | 47 (44.8%) | 46% | 51 (48.1%) | 47% | 98 (46.4%) | 47% |
| Female | 58 (55.2%) | 54% | 55 (51.9%) | 53% | 113 (53.6%) | 53% | |
| Age | Young 18–24 | 17 (16.2%) | 14% | 22 (20.8%) | 16% | 39 (18.5%) | 15% |
| Mid-young 25–44 | 51 (48.6%) | 42% | 54 (50.9%) | 39% | 105 (49.8%) | 40% | |
| Middle 45–64 | 37 (35.2%) | 44% | 30 (28.3%) | 46% | 67 (31.8%) | 45% | |
| Monthly household Income 1 | Low | 47 (44.8%) | 55% | 29 (27.4%) | 45% | 76 (36.0%) | 50% |
| Middle | 34 (32.4%) | 27% | 48 (45.3%) | 34% | 82 (38.9%) | 30% | |
| High | 24 (22.9%) | 18% | 29 (27.4%) | 21% | 53 (25.1%) | 20% | |
| Chronic health conditions | Respiratory | 2 (1.9%) | - | 4 (3.8%) | - | 6 (2.8%) | - |
| Others | 17 (16.2%) | - | 14 (13.2%) | - | 31 (14.7%) | - | |
| None | 86 (81.9%) | - | 88 (83.0%) | - | 174 (82.5%) | - | |
| Education level 2 | Low | 37 (35.2%) | - | 35 (33.0%) | - | 72 (34.1%) | - |
| Middle | 55 (52.4%) | - | 57 (53.8%) | - | 112 (53.1%) | - | |
| High | 13 (12.4%) | - | 14 (13.2%) | - | 27 (12.8%) | - | |
| Marital status | Single | 53 (50.5%) | - | 59 (55.7%) | - | 112 (53.1%) | - |
| Married | 41 (39.0%) | - | 37 (34.9%) | - | 78 (37.0%) | - | |
| Others 3 | 11 (10.5%) | - | 10 (9.4%) | - | 21 (10.0%) | - | |
| Total | 105 (100%) | 100% | 106 (100%) | 100% | 211 (100%) | 100% | |
| Axis | Paired Groups | Neighborhood Air Quality | Place Air Quality | Hong Kong Air Quality | ||||
|---|---|---|---|---|---|---|---|---|
| U | p-Value | U | p-Value | U | p-Value | |||
| Gender | Male | Female | 5334 | 0.630 | 6542 * | 0.016 | 5474 | 0.881 |
| Age | Young | Mid-young | 2085 | 0.860 | 2030 | 0.937 | 2256 | 0.322 |
| Young | Middle | 1428 | 0.403 | 1543 | 0.102 | 1480 | 0.225 | |
| Mid-young | Middle | 3781 | 0.385 | 4182 * | 0.027 | 3626 | 0.718 | |
| Household income | Low | Middle | 2984 | 0.629 | 2920 | 0.473 | 3020 | 0.722 |
| Low | High | 1995 | 0.925 | 1776 | 0.225 | 2159 | 0.460 | |
| Middle | High | 2236 | 0.768 | 2064 | 0.604 | 2388 | 0.306 | |
| Education level | Low | Middle | 3829 | 0.545 | 3394 | 0.055 | 3581 | 0.174 |
| Low | High | 893 | 0.518 | 788 | 0.127 | 988 | 0.898 | |
| Middle | High | 1468 | 0.806 | 1460 | 0.771 | 1715 | 0.251 | |
| Marital status | Single | Married | 4741 | 0.292 | 4884 | 0.142 | 4740 | 0.291 |
| Single | Others | 1261 | 0.582 | 1232 | 0.719 | 1244 | 0.659 | |
| Married | Others | 813 | 0.961 | 764 | 0.626 | 793 | 0.814 | |
| Community | SSP | TSW | 7678 ** | <0.001 | 6330 | 0.068 | 6150 | 0.162 |
| Axis | Paired Groups | Cough | Phlegm | Short Breath | ||||
|---|---|---|---|---|---|---|---|---|
| U | p-Value | U | p-Value | U | p-Value | |||
| Gender | Male | Female | 6082 | 0.202 | 5566 | 0.946 | 5606 | 0.870 |
| Age | Young | Mid-young | 2196 | 0.490 | 1946 | 0.639 | 2010 | 0.862 |
| Young | Middle | 1295 | 0.940 | 1055 | 0.090 | 1064 | 0.099 | |
| Mid-young | Middle | 3282 | 0.445 | 3028 | 0.113 | 2978 | 0.076 | |
| Household income | Low | Middle | 3471 | 0.201 | 3141 | 0.930 | 3082 | 0.903 |
| Low | High | 1972 | 0.837 | 1930 | 0.678 | 2234 | 0.269 | |
| Middle | High | 1875 | 0.163 | 2066 | 0.618 | 2484 | 0.142 | |
| Education level | Low | Middle | 3925 | 0.754 | 4225 | 0.574 | 4417 | 0.255 |
| Low | High | 1096 | 0.316 | 1150 | 0.149 | 1244 * | 0.026 | |
| Middle | High | 1785 | 0.129 | 1720 | 0.251 | 1800 | 0.107 | |
| Marital status | Single | Married | 4639 | 0.452 | 4226 | 0.694 | 4447 | 0.825 |
| Single | Others | 880 | 0.056 | 807 * | 0.018 | 946 | 0.140 | |
| Married | Others | 588 * | 0.042 | 608 | 0.065 | 652 | 0.136 | |
| Community | SSP | TSW | 6034 | 0.272 | 6145 | 0.177 | 6002 | 0.302 |
| (N = 211) | Neighborhood Air Quality | Place Air Quality | Hong Kong Air Quality | |||
|---|---|---|---|---|---|---|
| p-Value | p-Value | p-Value | ||||
| Cough | 0.002 | 0.486 | 0.086 | 0.106 | 0.113 | 0.051 |
| Phlegm | −0.007 | 0.461 | 0.086 | 0.107 | 0.154 * | 0.013 |
| Short breath | 0.075 | 0.139 | 0.096 | 0.082 | 0.091 | 0.094 |
| Category | Neighborhood Air Quality | Place Air Quality | Hong Kong Air Quality | ||||
|---|---|---|---|---|---|---|---|
| p-Value | p-Value | p-Value | |||||
| Male (N = 98) | Cough | 0.027 | 0.396 | 0.120 | 0.119 | 0.190 * | 0.031 |
| Phlegm | 0.112 | 0.137 | 0.205 * | 0.021 | 0.198 * | 0.026 | |
| Short breath | 0.195 * | 0.027 | 0.169 * | 0.049 | 0.190 * | 0.031 | |
| Female (N = 113) | Cough | −0.010 | 0.460 | 0.033 | 0.365 | 0.055 | 0.282 |
| Phlegm | −0.110 | 0.122 | −0.017 | 0.431 | 0.122 | 0.099 | |
| Short breath | −0.029 | 0.381 | 0.040 | 0.336 | 0.002 | 0.490 | |
| Socio-Demographic Characteristics | N | Perceived Air Quality | Respiratory Symptom | rs | p-Value 2 | |
|---|---|---|---|---|---|---|
| Axis | Group | |||||
| Age | Young | 39 | Place air quality | Short breath | 0.290 | 0.037 |
| Middle-Young | 105 | HK air quality | Phlegm | 0.254 | 0.004 | |
| Middle | 67 | Place air quality | Cough | 0.244 | 0.023 | |
| Household income | Low | 76 | Place air quality | Short breath | 0.209 | 0.035 |
| Middle | 82 | HK air quality | Cough | 0.188 | 0.046 | |
| Education level | Low | 72 | Place air quality | Short breath | 0.211 | 0.038 |
| Middle | 112 | HK air quality | Phlegm | 0.170 | 0.037 | |
| Marital status | Single | 112 | HK air quality | Cough | 0.190 | 0.022 |
| Single | 112 | HK air quality | Phlegm | 0.217 | 0.011 | |
| Category | Neighborhood Air Quality | Place Air Quality | Hong Kong Air Quality | ||||
|---|---|---|---|---|---|---|---|
| p-Value | p-Value | p-Value | |||||
| SSP (N = 105) | Cough | −0.006 | 0.474 | 0.183 * | 0.031 | 0.202 * | 0.019 |
| Phlegm | 0.002 | 0.494 | 0.217 * | 0.013 | 0.270 ** | 0.003 | |
| Short breath | 0.096 | 0.165 | 0.164 * | 0.048 | 0.126 | 0.100 | |
| TSW (N = 106) | Cough | −0.065 | 0.253 | −0.024 | 0.402 | −0.003 | 0.488 |
| Phlegm | −0.084 | 0.196 | −0.066 | 0.251 | −0.004 | 0.485 | |
| Short breath | −0.007 | 0.470 | 0.012 | 0.451 | 0.023 | 0.408 | |
| Variables | Cough | Phlegm | Short Breath | ||||
|---|---|---|---|---|---|---|---|
| Type I | Type II | Type I | Type II | Type I | Type II | ||
| Constant | −2.143 ** | −2.221 * | −2.093 ** | −2.757 ** | −2.435 ** | −4.533 ** | |
| Neighborhood air quality | −0.198 | −0.159 | −0.172 | −0.215 | −0.048 | −0.039 | |
| Place air quality | 0.174 | 0.105 | −0.003 | 0.148 | −0.076 | 0.105 | |
| Hong Kong air quality | 0.157 | 0.238 | 0.313 | 0.300 | 0.368 | 0.330 | |
| Geographic context | SSP | 0.373 | 0.347 | 0.402 | 0.388 | −0.262 | −0.557 |
| TSW | Reference | ||||||
| Gender | Male | 0.388 | −0.765 ** | −0.325 | |||
| Female | Reference | ||||||
| Age | Young | 0.084 | −0.652 | −1.718 ** | |||
| Middle-Young | 0.375 | −0.340 | −0.631 | ||||
| Middle | Reference | ||||||
| Monthly household income | Low | −0.546 | −0.870 * | 0.681 | |||
| Middle | −0.898 * | −0.779 * | 0.074 | ||||
| High | Reference | ||||||
| Education level | Low | 1.151 | 1.649 * | 2.030 * | |||
| Middle | 0.351 | 1.752 ** | 1.703 | ||||
| High | Reference | ||||||
| Marital status | Single | −0.684 | 0.023 | 0.737 | |||
| Married | −0.660 | −0.118 | 0.031 | ||||
| Others | Reference | ||||||
| Nagelkerke R2 | 0.019 | 0.084 | 0.028 | 0.125 | 0.026 | 0.146 | |
| Cox & Snell R2 | 0.012 | 0.054 | 0.019 | 0.082 | 0.016 | 0.089 | |
| −2 Log likelihood | 210.746 | 201.760 | 222.296 | 208.147 | 195.644 | 179.339 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.; Kwan, M.-P.; Kan, Z. Inconsistent Association between Perceived Air Quality and Self-Reported Respiratory Symptoms: A Pilot Study and Implications for Environmental Health Studies. Int. J. Environ. Res. Public Health 2023, 20, 1491. https://doi.org/10.3390/ijerph20021491
Liu Y, Kwan M-P, Kan Z. Inconsistent Association between Perceived Air Quality and Self-Reported Respiratory Symptoms: A Pilot Study and Implications for Environmental Health Studies. International Journal of Environmental Research and Public Health. 2023; 20(2):1491. https://doi.org/10.3390/ijerph20021491
Chicago/Turabian StyleLiu, Yang, Mei-Po Kwan, and Zihan Kan. 2023. "Inconsistent Association between Perceived Air Quality and Self-Reported Respiratory Symptoms: A Pilot Study and Implications for Environmental Health Studies" International Journal of Environmental Research and Public Health 20, no. 2: 1491. https://doi.org/10.3390/ijerph20021491
APA StyleLiu, Y., Kwan, M.-P., & Kan, Z. (2023). Inconsistent Association between Perceived Air Quality and Self-Reported Respiratory Symptoms: A Pilot Study and Implications for Environmental Health Studies. International Journal of Environmental Research and Public Health, 20(2), 1491. https://doi.org/10.3390/ijerph20021491