
Long-Term Effects of Mountain Hiking vs. Forest Therapy on Physical and Mental Health of Couples: A Randomized Controlled Trial


 ,
,  , ,
, ,  , ,
, ,
Abstract
Highlights
- Highly functioning adults with a sedentary lifestyle benefit physically and mentally from forest therapy and mountain hiking.
- Women predominantly benefited highly from mountain hiking regarding hemopoietic system and aerobic capacity. Both genders profited mentally from contact with nature.
- Forest therapy and mountain hiking could be safe and health-promoting interventions for high-functioning adults with a sedentary lifestyle and could be applied in primary prevention as well as in secondary prevention.
Abstract
1. Introduction
2. Materials and Methods
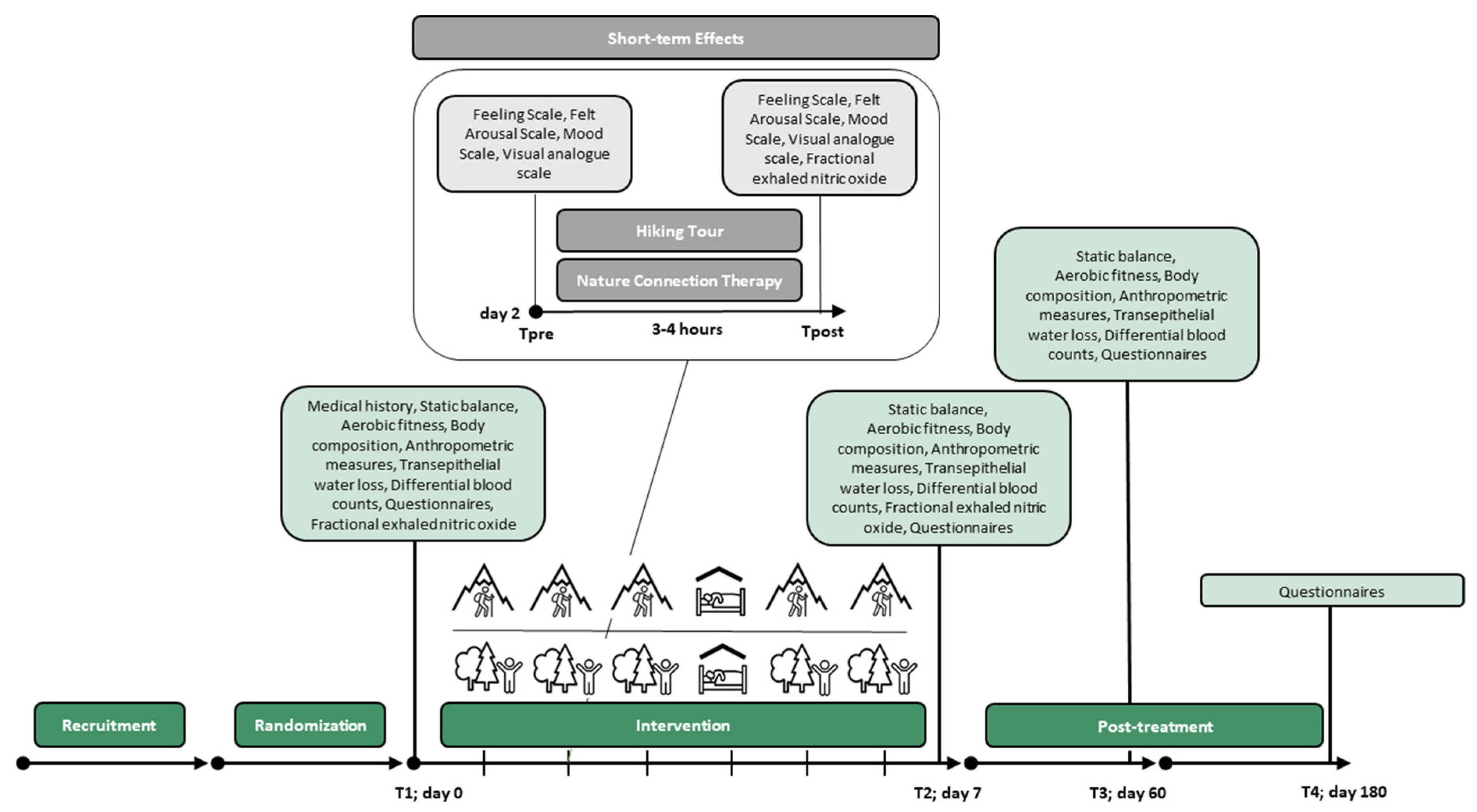
2.1. Study Design and Settings
2.2. Participants
2.3. Intervention
2.4. Data Collection and Outcomes
2.5. Statistical Analysis
2.6. Randomization and Sample Size
3. Results
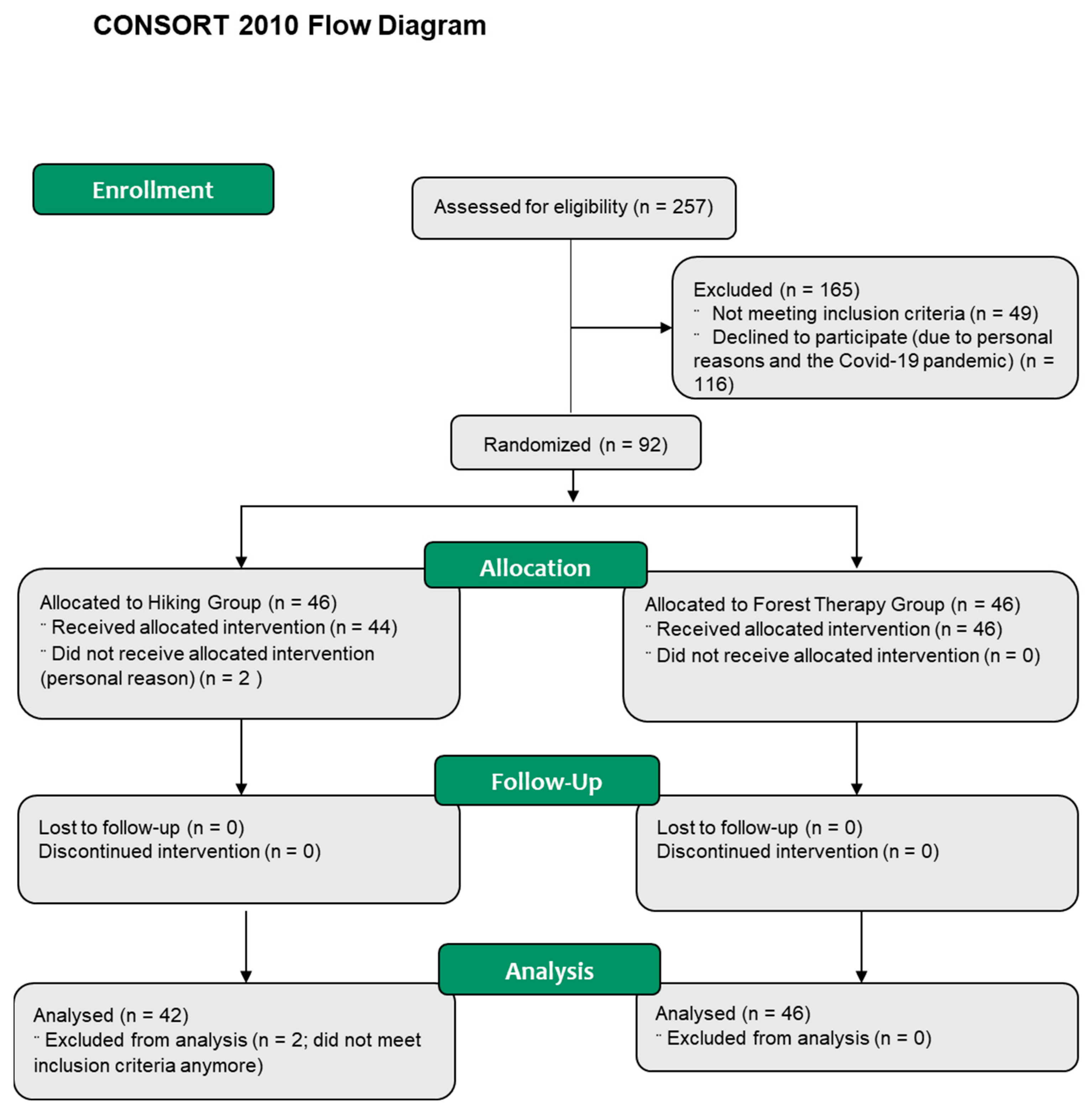
3.1. Study Participants and Baseline Characteristics
3.2. Tour Data
3.3. Primary Outcomes
3.4. Differential Blood Count
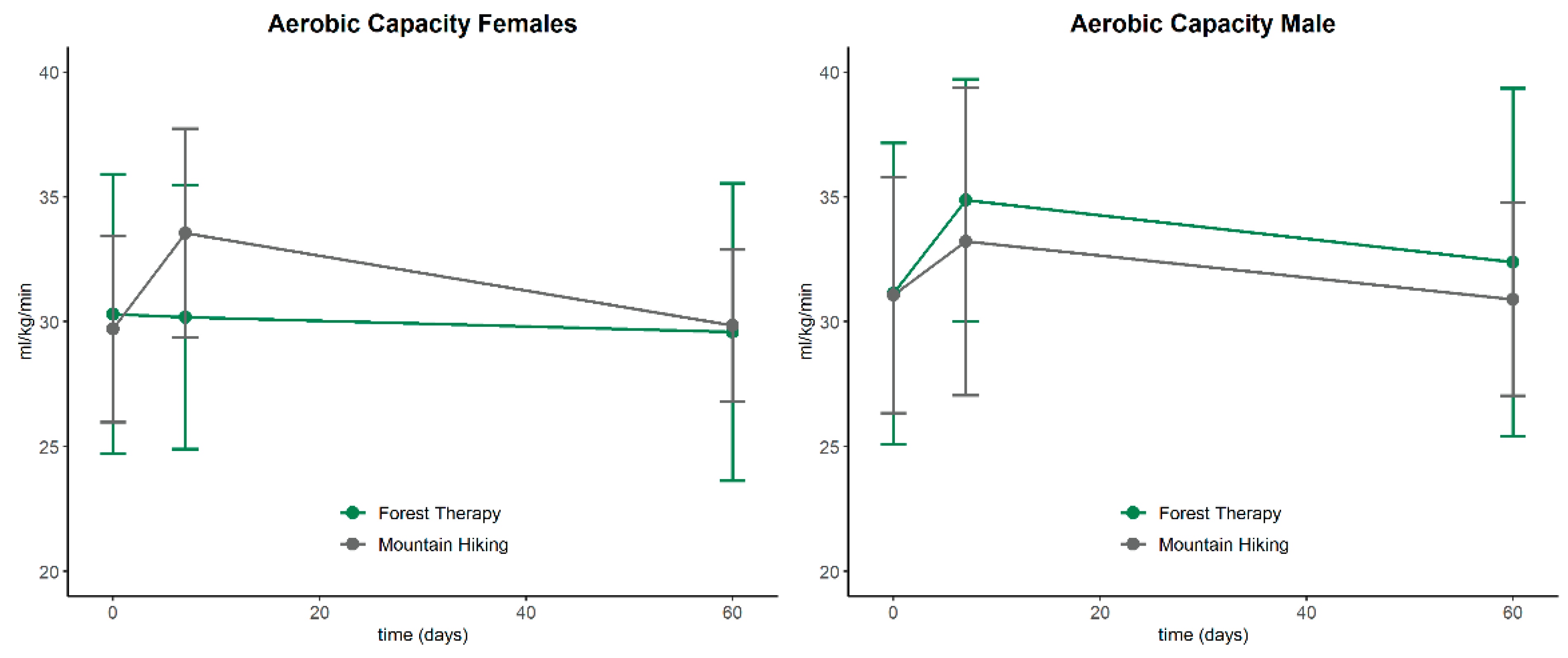
3.5. Aerobic Capacity, Balance, Vital Parameters and Skin Quality
3.6. Body Composition
3.7. Questionnaires
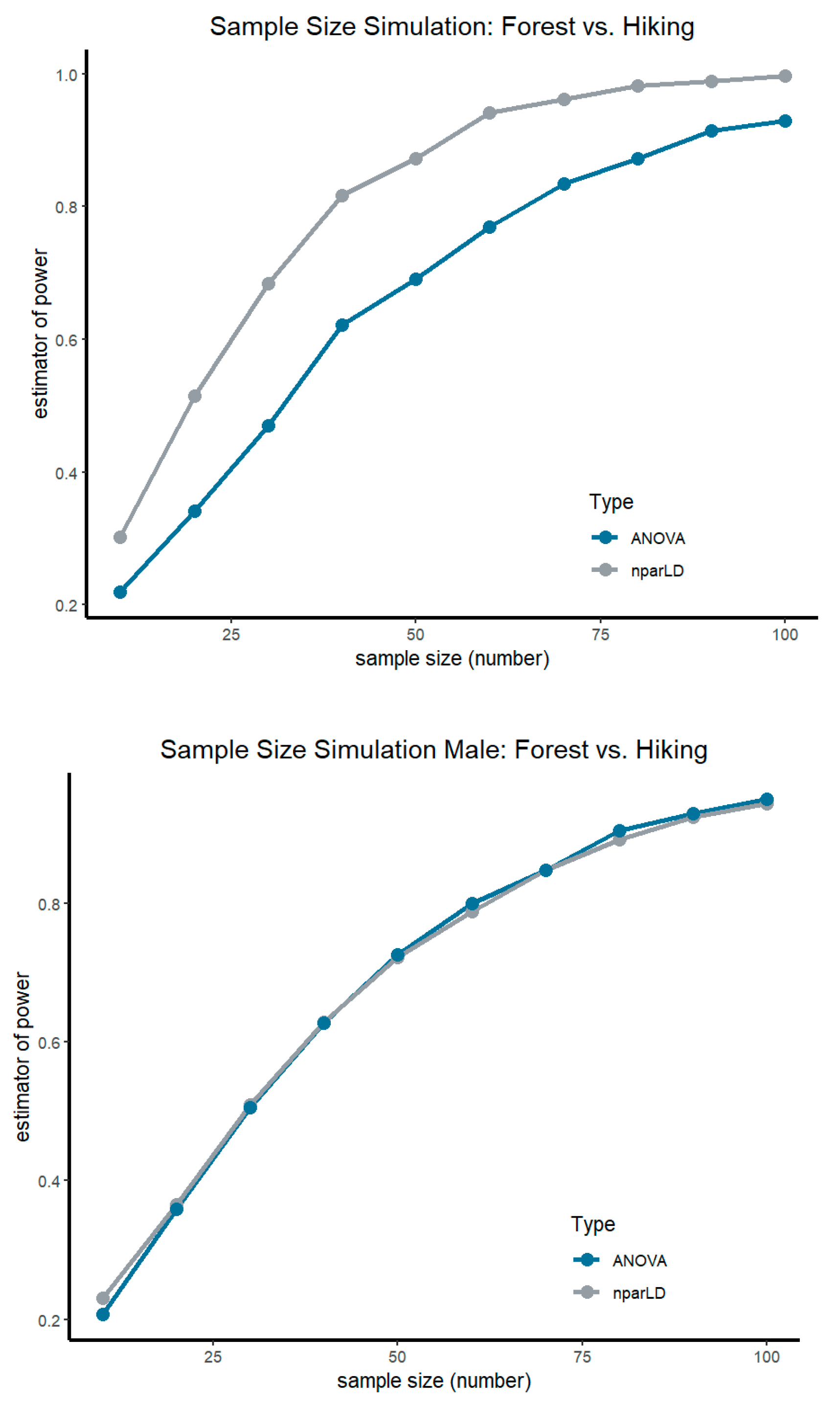
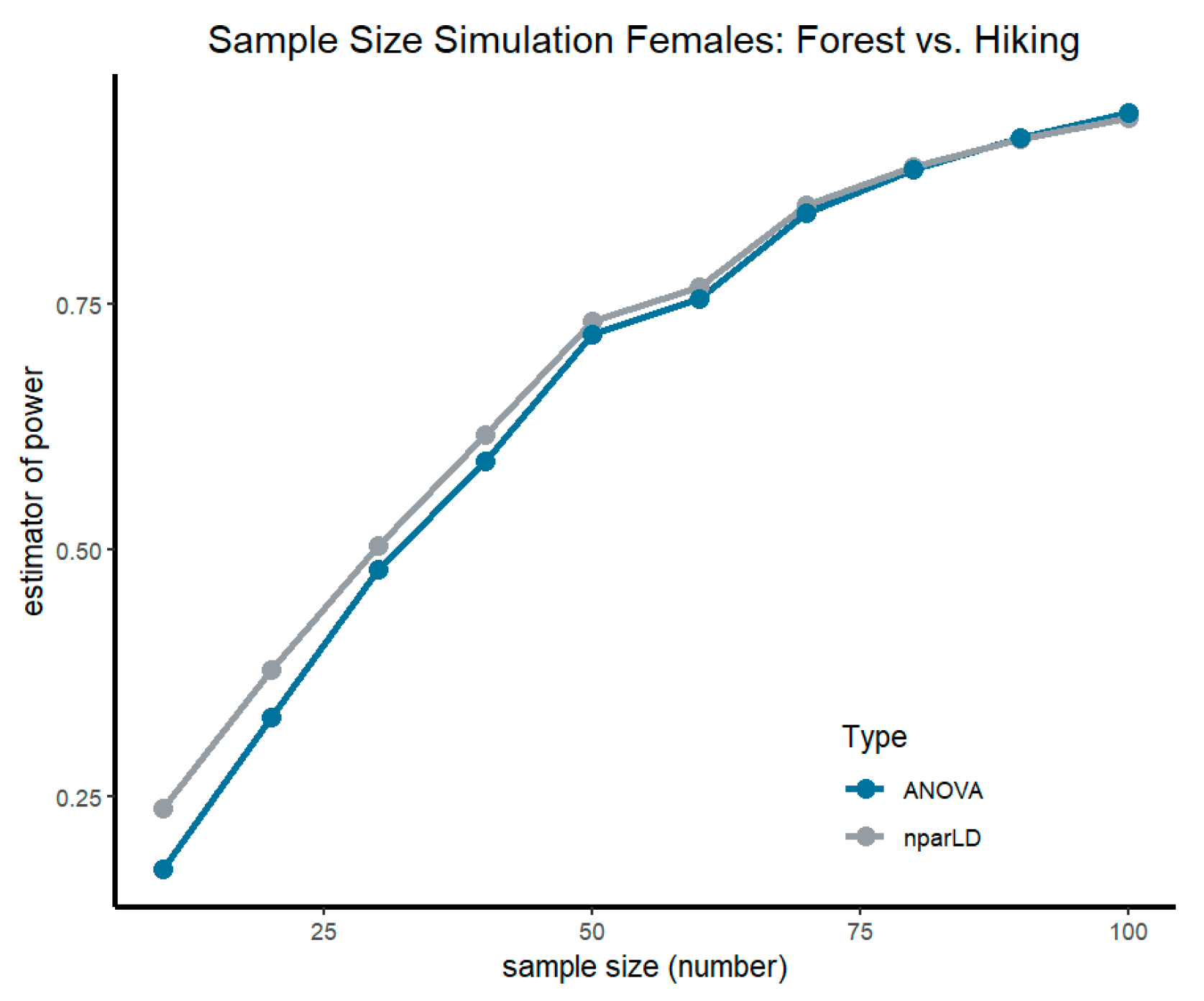
3.8. Sample Size Simulation
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Warburton, D.E.R.; Bredin, S.S.D. Health Benefits of Physical Activity: A Systematic Review of Current Systematic Reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef] [PubMed]
- Arem, H.; Moore, S.C.; Patel, A.; Hartge, P.; de Gonzalez, A.B.; Visvanathan, K.; Campbell, P.T.; Freedman, M.; Weiderpass, E.; Adami, H.O.; et al. Leisure Time Physical Activity and Mortality: A Detailed Pooled Analysis of the Dose-Response Relationship. JAMA Intern. Med. 2015, 175, 959–967. [Google Scholar] [CrossRef] [PubMed]
- Peluso, M.A.M.; Andrade, L.H.S.G. de Physical Activity and Mental Health: The Association between Exercise and Mood. Clinics 2005, 60, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Ruegsegger, G.N.; Booth, F.W. Health Benefits of Exercise. Cold Spring Harb. Perspect. Med. 2018, 8, a029694. [Google Scholar] [CrossRef] [PubMed]
- Sato, M.; Du, J.; Inoue, Y.; Funk, D.C.; Weaver, F. Older Adults’ Physical Activity and Healthcare Costs, 2003–2014. Am. J. Prev. 2020, 58, e141–e148. [Google Scholar] [CrossRef]
- Sedentary Behaviour Research Network Letter to the Editor: Standardized Use of the Terms “Sedentary” and “Sedentary Behaviours”. Appl. Physiol. Nutr. Metab. 2012, 37, 540–542. [CrossRef]
- Ildefonzo Arocha Rodulfo, J. Sedentarismo, la enfermedad del siglo xxi. Clín. Investig. Arterioscler. 2019, 31, 233–240. [Google Scholar] [CrossRef]
- Martins, L.C.G.; de Lopes, M.V.O.; Diniz, C.M.; Guedes, N.G. The Factors Related to a Sedentary Lifestyle: A Meta-analysis Review. J. Adv. Nurs. 2021, 77, 1188–1205. [Google Scholar] [CrossRef]
- Després, J.-P. Physical Activity, Sedentary Behaviours, and Cardiovascular Health: When Will Cardiorespiratory Fitness Become a Vital Sign? Can. J. Cardiol. 2016, 32, 505–513. [Google Scholar] [CrossRef]
- Blüher, M. Obesity: Global Epidemiology and Pathogenesis. Nat. Rev. Endocrinol. 2019, 5, 288–298. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for Europe Supplement to the European Health Report 2021: Projections for a Selection of Indicators for Health-Related Sustainable Development Goals; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2022; ISBN 978-92-890-5763-9. [Google Scholar]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide Trends in Insufficient Physical Activity from 2001 to 2016: A Pooled Analysis of 358 Population-Based Surveys with 1·9 Million Participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [PubMed]
- Granger, E.; Di Nardo, F.; Harrison, A.; Patterson, L.; Holmes, R.; Verma, A. A Systematic Review of the Relationship of Physical Activity and Health Status in Adolescents. Eur. J. Public Health 2017, 27, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Martínez-de-Quel, Ó.; Suárez-Iglesias, D.; López-Flores, M.; Pérez, C.A. Physical Activity, Dietary Habits and Sleep Quality before and during COVID-19 Lockdown: A Longitudinal Study. Appetite 2021, 158, 105019. [Google Scholar] [CrossRef]
- Fukushima, N.; Machida, M.; Kikuchi, H.; Amagasa, S.; Hayashi, T.; Odagiri, Y.; Takamiya, T.; Inoue, S. Associations of Working from Home with Occupational Physical Activity and Sedentary Behavior under the COVID-19 Pandemic. J. Occup. Health 2021, 63, e12212. [Google Scholar] [CrossRef]
- Holt-Lunstad, J. Why Social Relationships Are Important for Physical Health: A Systems Approach to Understanding and Modifying Risk and Protection. Annu. Rev. Psychol. 2018, 69, 437–458. [Google Scholar] [CrossRef]
- Langgartner, D.; Lowry, C.A.; Reber, S.O. Old Friends, Immunoregulation, and Stress Resilience. Pflugers Arch. 2019, 471, 237–269. [Google Scholar] [CrossRef]
- Freidl, J.; Huber, D.; Braunschmid, H.; Romodow, C.; Pichler, C.; Weisböck-Erdheim, R.; Mayr, M.; Hartl, A. Winter Exercise and Speleotherapy for Allergy and Asthma: A Randomized Controlled Clinical Trial. JCM 2020, 9, 3311. [Google Scholar] [CrossRef]
- Hanski, I.; von Hertzen, L.; Fyhrquist, N.; Koskinen, K.; Torppa, K.; Laatikainen, T.; Karisola, P.; Auvinen, P.; Paulin, L.; Mäkelä, M.J.; et al. Environmental Biodiversity, Human Microbiota, and Allergy Are Interrelated. Proc. Natl. Acad. Sci. USA 2012, 109, 8334–8339. [Google Scholar] [CrossRef] [PubMed]
- Blaser, M.J. The Theory of Disappearing Microbiota and the Epidemics of Chronic Diseases. Nat. Rev. Immunol. 2017, 17, 461–463. [Google Scholar] [CrossRef] [PubMed]
- Rook, G.A.W.; Lowry, C.A.; Raison, C.L. Microbial ‘Old Friends’, Immunoregulation and Stress Resilience. Evol. Med. Public Health 2013, 2013, 46–64. [Google Scholar] [CrossRef]
- Mcdade, T.W.; Tallman, P.S.; Madimenos, F.C.; Liebert, M.A.; Cepon, T.J.; Sugiyama, L.S.; Snodgrass, J.J. Analysis of Variability of High Sensitivity C-reactive Protein in Lowland Ecuador Reveals No Evidence of Chronic Low-grade Inflammation. Am. J. Hum. Biol. 2012, 24, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Lowry, C.A.; Smith, D.G.; Siebler, P.H.; Schmidt, D.; Stamper, C.E.; Hassell, J.E.; Yamashita, P.S.; Fox, J.H.; Reber, S.O.; Brenner, L.A.; et al. The Microbiota, Immunoregulation, and Mental Health: Implications for Public Health. Curr. Envir. Health Rep. 2016, 3, 270–286. [Google Scholar] [CrossRef] [PubMed]
- United Nations, Department of Economic and Social Affairs, Population Division. World Urbanization Prospects: The 2018 Revision; United Nations: New York, NY, USA, 2019. [Google Scholar]
- Faulhaber, M.; Pocecco, E.; Niedermeier, M.; Ruedl, G.; Walter, D.; Sterr, R.; Ebner, H.; Schobersberger, W.; Burtscher, M. Fall-Related Accidents among Hikers in the Austrian Alps: A 9-Year Retrospective Study. BMJ Open Sport Exerc. Med. 2017, 3, e000304. [Google Scholar] [CrossRef] [PubMed]
- Burtscher, M. Endurance Performance of the Elderly Mountaineer: Requirements, Limitations, Testing, and Training. Wien. Klin. Wochenschr. 2004, 116, 703–714. [Google Scholar] [CrossRef] [PubMed]
- Richins, H.; Hull, J.S. Mountain Tourism: Experiences, Communities, Environments and Sustainable Futures; CABI: Wallingford, UK, 2016. [Google Scholar]
- Evju, M.; Hagen, D.; Jokerud, M.; Olsen, S.L.; Selvaag, S.K.; Vistad, O.I. Effects of Mountain Biking versus Hiking on Trails under Different Environmental Conditions. J. Environ. Manag. 2021, 278, 111554. [Google Scholar] [CrossRef]
- Pomfret, G. Mountaineering Adventure Tourists: A Conceptual Framework for Research. Tour. Manag. 2006, 27, 113–123. [Google Scholar] [CrossRef]
- Niedermeier, M.; Grafetstätter, C.; Kopp, M.; Huber, D.; Mayr, M.; Pichler, C.; Hartl, A. The Role of Anthropogenic Elements in the Environment for Affective States and Cortisol Concentration in Mountain Hiking—A Crossover Trial. Int. J. Environ. Res. Public Health 2019, 16, 290. [Google Scholar] [CrossRef]
- Schobersberger, W.; Leichtfried, V.; Mueck-Weymann, M.; Humpeler, E. Austrian Moderate Altitude Studies (AMAS): Benefits of Exposure to Moderate Altitudes (1500–2500 m). Sleep Breath 2010, 14, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Yeon, P.-S.; Jeon, J.-Y.; Jung, M.-S.; Min, G.-M.; Kim, G.-Y.; Han, K.-M.; Shin, M.-J.; Jo, S.-H.; Kim, J.-G.; Shin, W.-S. Effect of Forest Therapy on Depression and Anxiety: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 12685. [Google Scholar] [CrossRef]
- Oh, K.H.; Shin, W.S.; Khil, T.G.; Kim, D.J. Six-Step Model of Nature-Based Therapy Process. Int. J. Environ. Res. Public Health 2020, 17, 685. [Google Scholar] [CrossRef]
- Chae, Y.; Lee, S.; Jo, Y.; Kang, S.; Park, S.; Kang, H. The Effects of Forest Therapy on Immune Function. Int. J. Environ. Res. Public Health 2021, 18, 8440. [Google Scholar] [CrossRef] [PubMed]
- Roviello, V.; Roviello, G.N. Less COVID-19 Deaths in Southern and Insular Italy Explained by Forest Bathing, Mediterranean Environment, and Antiviral Plant Volatile Organic Compounds. Environ. Chem. Lett. 2022, 20, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Stier-Jarmer, M.; Throner, V.; Kirschneck, M.; Immich, G.; Frisch, D.; Schuh, A. The Psychological and Physical Effects of Forests on Human Health: A Systematic Review of Systematic Reviews and Meta-Analyses. Int. J. Environ. Res. Public Health 2021, 18, 1770. [Google Scholar] [CrossRef] [PubMed]
- Hansen, M.M.; Jones, R.; Tocchini, K. Shinrin-Yoku (Forest Bathing) and Nature Therapy: A State-of-the-Art Review. Int. J. Environ. Res. Public Health 2017, 14, 851. [Google Scholar] [CrossRef] [PubMed]
- Wen, Y.; Yan, Q.; Pan, Y.; Gu, X.; Liu, Y. Medical Empirical Research on Forest Bathing (Shinrin-Yoku): A Systematic Review. Environ. Health Prev. Med. 2019, 24, 70. [Google Scholar] [CrossRef]
- Oh, B.; Lee, K.J.; Zaslawski, C.; Yeung, A.; Rosenthal, D.; Larkey, L.; Back, M. Health and Well-Being Benefits of Spending Time in Forests: Systematic Review. Environ. Health Prev. Med. 2017, 22, 71. [Google Scholar] [CrossRef]
- Pichler, C.; Freidl, J.; Bischof, M.; Kiem, M.; Erdheim-Weißböck, R.; Huber, D.; Squarra, G.; Murschetz, P.; Hartl, A. Mountain Hiking vs. Forest Therapy. A Study Protocol of Novel Types of Nature-Based Intervention. Int. J. Environ. Res. Public Health 2022, 19, 3888. [Google Scholar] [CrossRef]
- Vectorstall Man Free Icon. Available online: https://www.flaticon.com (accessed on 3 October 2022).
- Nadiinko Sleeping Icon. Available online: https://www.flaticon.com (accessed on 3 October 2022).
- Noguchi, K.; Gel, Y.R.; Brunner, E.; Konietschke, F. NparLD: An R Software Package for the Nonparametric Analysis of Longitudinal Data in Factorial Experiments. J. Stat. Soft. 2012, 50, 1–23. [Google Scholar] [CrossRef]
- Kraus, D. Consolidated Data Analysis and Presentation Using an Open-Source Add-in for the Microsoft Excel® Spreadsheet Software. Medical Writing 2014, 23, 25–28. [Google Scholar] [CrossRef]
- Prossegger, J. Effects of Moderate Mountain Hiking and Balneotherapy on Community-Dwelling Older People: A Randomized Controlled Trial. Exp. Gerontol. 2019, 11, 74–84. [Google Scholar] [CrossRef]
- Morse, J.W.; Gladkikh, T.M.; Hackenburg, D.M.; Gould, R.K. COVID-19 and Human-Nature Relationships: Vermonters’ Activities in Nature and Associated Nonmaterial Values during the Pandemic. PLoS ONE 2020, 15, e0243697. [Google Scholar] [CrossRef] [PubMed]
- Almeida, M.; Shrestha, A.D.; Stojanac, D.; Miller, L.J. The Impact of the COVID-19 Pandemic on Women’s Mental Health. Arch. Women’s Ment. Health 2020, 23, 741–748. [Google Scholar] [CrossRef]
- Smith, D.T.; Mouzon, D.M.; Elliott, M. Reviewing the Assumptions About Men’s Mental Health: An Exploration of the Gender Binary. Am. J. Men’s Health 2018, 12, 78–89. [Google Scholar] [CrossRef] [PubMed]
- Estlein, R.; Gewirtz-Meydan, A.; Opuda, E. Love in the Time of COVID-19: A Systematic Mapping Review of Empirical Research on Romantic Relationships One Year into the COVID-19 Pandemic. Fam. Process 2022, 61, 963–1357. [Google Scholar] [CrossRef] [PubMed]
- Mallet, R.T.; Burtscher, J.; Richalet, J.-P.; Millet, G.P.; Burtscher, M. Impact of High Altitude on Cardiovascular Health: Current Perspectives. Vasc. Health Risk Manag. 2021, 17, 317–335. [Google Scholar] [CrossRef] [PubMed]
- Gatterer, H.; Raab, C.; Pramsohler, S.; Faulhaber, M.; Burtscher, M.; Netzer, N. Effect of Weekly Hiking on Cardiovascular Risk Factors in the Elderly. Z. Für Gerontol. Und Geriatr. 2015, 48, 150–153. [Google Scholar] [CrossRef]
- Neumayr, G.; Fries, D.; Mittermayer, M.; Humpeler, E.; Klingler, A.; Schobersberger, W.; Spiesberger, R.; Pokan, R.; Schmid, P.; Berent, R. Effects of Hiking at Moderate and Low Altitude on Cardiovascular Parameters in Male Patients With Metabolic Syndrome: Austrian Moderate Altitude Study. Wilderness Environ. Med. 2014, 25, 329–334. [Google Scholar] [CrossRef]
- Stoltzfus, K.B.; Naylor, D.; Cattermole, T.; Ankeney, A.; Mount, R.; Chang, R.; Gibson, C.A. Blood Pressure Changes While Hiking at Moderate Altitudes: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 7978. [Google Scholar] [CrossRef]
- Kim, J.-G.; Shin, W.-S. Forest Therapy Alone or with a Guide: Is There a Difference between Self-Guided Forest Therapy and Guided Forest Therapy Programs? Int. J. Environ. Res. Public Health 2021, 15, 6957. [Google Scholar] [CrossRef]
- Banerjee, D.; Rai, M. Social Isolation in Covid-19: The Impact of Loneliness. Int. J. Soc. Psychiatry 2020, 66, 525–527. [Google Scholar] [CrossRef]
- Smith, B.; Lim, M. How the COVID-19 Pandemic Is Focusing Attention on Loneliness and Social Isolation. Public Health Res. Pract. 2020, 30, 3022008. [Google Scholar] [CrossRef]
- Castañeda-Babarro, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B.; Coca, A. Physical Activity Change during COVID-19 Confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef]
- Ya’qoub, L.; Elgendy, I.Y.; Pepine, C.J. Sex and Gender Differences in COVID-19: More to Be Learned! Am. Heart J. Plus 2021, 3, 100011. [Google Scholar] [CrossRef]
- Amgalan, A.; Malinowski, A.K.; Othman, M. COVID-19 and Sex/Gender-Specific Differences: Understanding the Discrimination. Semin. Thromb. Hemost. 2021, 47, 7. [Google Scholar] [CrossRef] [PubMed]
- Koprowicz, A.; Korzeniewicz, R.; Pusz, W.; Baranowska, M. Sociodemographic Determinants of Poles’ Attitudes towards the Forest during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 1537. [Google Scholar] [CrossRef]
- Park, B.-J.; Shin, C.-S.; Shin, W.-S.; Chung, C.-Y.; Lee, S.-H.; Kim, D.-J.; Kim, Y.-H.; Park, C.-E. Effects of Forest Therapy on Health Promotion among Middle-Aged Women: Focusing on Physiological Indicators. Int. J. Environ. Res. Public Health 2020, 17, 4348. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Kim, J.; Ju, H.J.; Jang, B.J.; Wang, T.K.; Kim, Y.I. Effect of Forest Therapy for Menopausal Women with Insomnia. Int. J. Environ. Res. Public Health 2020, 17, 6548. [Google Scholar] [CrossRef] [PubMed]
- Song, C.; Ikei, H.; Kagawa, T.; Miyazaki, Y. Effects of Walking in a Forest on Young Women. Int. J. Environ. Res. Public Health 2019, 16, 229. [Google Scholar] [CrossRef] [PubMed]
- Grilli, G.; Sacchelli, S. Health Benefits Derived from Forest: A Review. Int. J. Environ. Res. Public Health 2020, 17, 6125. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.-W.; Tetzlaff, J.M.; Altman, D.G.; Laupacis, A.; Gøtzsche, P.C.; Krleža-Jerić, K.; Hróbjartsson, A.; Mann, H.; Dickersin, K.; Berlin, J.A.; et al. SPIRIT 2013 Statement: Defining Standard Protocol Items for Clinical Trials. Ann. Intern. Med. 2013, 158, 200. [Google Scholar] [CrossRef]
- Buckley, R.C.; Brough, P. Nature, Eco, and Adventure Therapies for Mental Health and Chronic Disease. Front. Public Health 2017, 5, 220. [Google Scholar] [CrossRef] [PubMed]
- Buckley, R.C.; Brough, P.; Westaway, D. Bringing Outdoor Therapies Into Mainstream Mental Health. Front. Public Health 2018, 6, 119. [Google Scholar] [CrossRef] [PubMed]
- Cuschieri, S. The CONSORT Statement. Saudi J. Anaesth. 2019, 13, S27–S30. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hiking Group (n = 42) | Forest Therapy Group (n = 46) | Baseline Tests | ||||
|---|---|---|---|---|---|---|
| Mean ± SD | Median ± IQR | Mean ± SD | Median ± IQR | |||
| Gender | male n = 21 | female n = 21 | male n = 23 | female n = 23 | 1 | χ² Test |
| Age (years) | 58.57 ± 5.14 | 59 ± 7 | 58.89 ± 5.67 | 60 ± 9 | 0.67 | U-Test |
| Duration of relationship (years) | 22.57 ± 13.84 | 26 ± 26 | 28.39 ± 11.66 | 33 ± 18.25 | 0.06 | U-Test |
| BMI (kg/m2) | 27.46 ± 2.04 | 27.61 ± 2.88 | 27.90 ± 3.48 | 27.09 ± 3.68 | 0.86 | U-Test |
| IPAQ-Short Score (MET-min/week) | 1757.78 ± 1768.94 | 1074.25 ± 1845.5 | 4853.12 ± 14,078.25 | 974 ± 3609.13 | 0.82 | U-Test |
| NRS-6 | 21 ± 5.6 | 21.5 ± 8 | 21.83 ± 4 | 22 ± 4 | 0.52 | U-Test |
| PHQ-9 | 2.71 ± 2.56 | 2 ± 3 | 3.41 ± 3.17 | 3 ± 4 | 0.31 | U-Test |
| Mountain Hiking | Forest Therapy * | |||||||
|---|---|---|---|---|---|---|---|---|
| Time | Intervention | Duration (hours/min) | Distance (km) | Altitude ** (hm) | Duration (hours/min) | Distance (km) | Altitude (m) | |
| Day 1 | 1 | 04:07 | 12.6 | ↑334 | ↓334 | 03:10 | - | - |
| Day 2 | 2 | 03:06 | 8.0 | ↑214 | ↓787 | 03:50 | - | - |
| Day 3 | 3 | 04:01 | 10.0 | ↑639 | ↓639 | 03:50 | - | - |
| Day 4 | Recovery | Recovery | ||||||
| Day 5 | 4 | 03:38 | 9.8 | ↑569 | ↓569 | 03:45 | - | - |
| Day 6 | 5 | 02:30 | 4.8 | ↑745 | ↓745 | 03:20 | - | - |
| Average | 03:28 | 9.04 | ↑500 | ↓615 | 03:35 | Max. 3 | Max. 100 | |
| Parameter | F1-LD-F1 Model | Relative Treatment Effects (RTE) | Descriptive Statistics | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | p | adj. p | Time | Hiking | Forest Therapy | Hiking | Forest Therapy | |||||
| SF-12 | Group | 2.89 (1.00, ∞) | 0.09 | Hiking | 0.55 | Forest T. | 0.46 | mean ± SD | mean ± SD | |||
| Total Score | Time | 8.07 (2.61, ∞) | <0.01 ** | T1 | 0.43 | Hi. x T1 | 0.47 | FT. x T1 | 0.40 | 82.90 ± 9.32 | 81.17 ± 8.05 | |
| Group*Time | 0.45 (2.61, ∞) | 0.69 | T2 | 0.53 | Hi. x T2 | 0.57 | FT. x T2 | 0.49 | 85.31 ± 10.54 | 83.95 ± 8.51 | ||
| Group*T2 | 0.04 (1.00, ∞) | 0.84 | 0.84 | T3 | 0.54 | Hi. x T3 | 0.60 | FT. x T3 | 0.48 | 86.88 ± 8.07 | 83.49 ± 8.33 | |
| Group*T3 | 1.07 (1.00, ∞) | 0.30 | 0.60 | T4 | 0.51 | Hi. x T4 | 0.56 | FT. x T4 | 0.46 | 85.56 ± 9.46 | 82.24 ± 9.91 | |
| Group*T4 | 0.43 (1.00, ∞) | 0.51 | 0.60 | |||||||||
| SF-12 | Group | 8.22 (1.00, ∞) | <0.01 ** | Hiking | 0.57 | Forest T. | 0.43 | mean ± SD | mean ± SD | |||
| Physical | Time | 12.48 (2.76, ∞) | <0 01 ** | T1 | 0.41 | Hi. x T1 | 0.48 | FT. x T1 | 0.34 | 85.89 ± 8.80 | 81.30 ± 9.51 | |
| Component | Group*Time | 0.78 (2.76, ∞) | 0.05 | T2 | 0.52 | Hi. x T2 | 0.58 | FT. x T2 | 0.46 | 88.57 ± 9.13 | 85.22 ± 9.31 | |
| Group*T2 | 0.36 (1.00, ∞) | 0.55 | 1.00 | T3 | 0.55 | Hi. x T3 | 0.61 | FT. x T3 | 0.48 | 89.52 ± 8.47 | 85.22 ± 10.70 | |
| Group*T3 | 0.02 (1.00, ∞) | 0.89 | 1.00 | T4 | 0.54 | Hi. x T4 | 0.63 | FT. x T4 | 0.44 | 90.36 ± 7.52 | 84.13 ± 10.66 | |
| Group*T4 | 0.91 (1.00, ∞) | 0.34 | 1.00 | |||||||||
| SF-12 | Group | 0.39 (1.00, ∞) | 0.53 | Hiking | 0.52 | Forest T. | 0.48 | mean ± SD | mean ± SD | |||
| Mental | Time | 3.31 (2.66, ∞) | 0.02 * | T1 | 0.46 | Hi. x T1 | 0.46 | FT. x T1 | 0.46 | 80.69 ± 11.29 | 81.08 ± 10.37 | |
| Component | Group*Time | 0.69 (2.66, ∞) | 0.54 | T2 | 0.53 | Hi. x T2 | 0.54 | FT. x T2 | 0.51 | 82.89 ± 13.34 | 83.01 ± 10.52 | |
| Group*T2 | 0.73 (1.00, ∞) | 0.39 | 0.78 | T3 | 0.53 | Hi. x T3 | 0.57 | FT. x T3 | 0.49 | 84.92 ± 9.62 | 82.21 ± 10.14 | |
| Group*T3 | 2.24 (1.00, ∞) | 0.13 | 0.40 | T4 | 0.49 | Hi. x T4 | 0.51 | FT. x T4 | 0.48 | 82.01 ± 12.56 | 80.84 ± 12.18 | |
| Group*T4 | 0.32 (1.00, ∞) | 0.40 | 0.57 | |||||||||
| EQ5D-5L | Group | 0.40 (1.00, ∞) | 0.53 | Hiking | 0.52 | Forest T. | 0.49 | mean ± SD | mean ± SD | |||
| Visual | Time | 11.25 (2.80, ∞) | <0.01 ** | T1 | 0.43 | Hi. x T1 | 0.45 | FT. x T1 | 0.40 | 82.14 ± 11.59 | 80.87 ± 10.92 | |
| Analogue | Group*Time | 0.15 (2.80, ∞) | 0.92 | T2 | 0.58 | Hi. x T2 | 0.58 | FT. x T2 | 0.57 | 87.38 ± 10.83 | 85.22 ± 15.74 | |
| Scale (VAS) | Group*T2 | 0.33 (1.00, ∞) | 0.57 | 1.00 | T3 | 0.52 | Hi. x T3 | 0.54 | FT. x T3 | 0.51 | 85.95 ± 9.64 | 83.26 ± 13.34 |
| Group*T3 | 0.02 (1.00, ∞) | 0.90 | 1.00 | T4 | 0.48 | Hi. x T4 | 0.50 | FT. x T4 | 0.46 | 84.05 ± 12.31 | 81.74 ± 12.88 | |
| Group*T4 | 0.00 (1.00, ∞) | 0.99 | 1.00 | |||||||||
| EQ5D-5L | Group | 5.20 (1.00, ∞) | 0.02 * | Hiking | 0.56 | Forest T. | 0.45 | mean ± SD | mean ± SD | |||
| Index | Time | 10.19 (2.78, ∞) | <0.01 ** | T1 | 0.44 | Hi. x T1 | 0.48 | FT. x T1 | 0.39 | 0.90 ± 0.14 | 0.90 ± 0.07 | |
| Group*Time | 0.88 (2.78, ∞) | 0.45 | T2 | 0.47 | Hi. x T2 | 0.52 | FT. x T2 | 0.42 | 0.93 ± 0.07 | 0.90 ± 0.08 | ||
| Group*T2 | 0.01 (1.00, ∞) | 0.92 | 1.00 | T3 | 0.57 | Hi. x T3 | 0.62 | FT. x T3 | 0.52 | 0.94 ± 0.07 | 0.93 ± 0.06 | |
| Group*T3 | 0.06 (1.00, ∞) | 0.81 | 1.00 | T4 | 0.53 | Hi. x T4 | 0.61 | FT. x T4 | 0.45 | 0.95 ± 0.06 | 0.90 ± 0.09 | |
| Group*T4 | 1.80 (1.00, ∞) | 0.18 | 1.00 | |||||||||
| Partnership | Group | 0.26 (1.00, ∞) | 0.61 | Hiking | 0.52 | Forest T. | 0.49 | mean ± SD | mean ± SD | |||
| Questionnaire | Time | 5.71 (2.65, ∞) | <0.01 ** | T1 | 0.50 | Hi. x T1 | 0.51 | FT. x T1 | 0.48 | 61.10 ± 12.24 | 59.64 ± 13.13 | |
| Total Score | Group*Time | 0.15 (2.65, ∞) | 0.91 | T2 | 0.53 | Hi. x T2 | 0.54 | FT. x T2 | 0.51 | 62.64 ± 14.06 | 60.62 ± 13.62 | |
| Group*T2 | 0.00 (1.00, ∞) | 0.99 | 1.00 | T3 | 0.52 | Hi. x T3 | 0.53 | FT. x T3 | 0.51 | 62.31 ± 13.29 | 60.48 ± 13.51 | |
| Group*T3 | 0.01 (1.00, ∞) | 0.91 | 1.00 | T4 | 0.46 | Hi. x T4 | 0.48 | FT. x T4 | 0.44 | 60.02 ± 15.16 | 57.02 ± 14.91 | |
| Group*T4 | 0.13 (1.00, ∞) | 0.72 | 1.00 | |||||||||
| Partnership | Group | 0.52 (1.00, ∞) | 0.47 | Hiking | 0.48 | Forest T. | 0.52 | mean ± SD | mean ± SD | |||
| Questionnaire | Time | 5.69 (2.55, ∞) | <0.01 ** | T1 | 0.52 | Hi. x T1 | 0.49 | FT. x T1 | 0.55 | 3.93 ± 0.95 | 4.14 ± 0.86 | |
| Happiness | Group*Time | 2.51 (2.55, ∞) | 0.07 | T2 | 0.52 | Hi. x T2 | 0.51 | FT. x T2 | 0.53 | 4.05 ± 0.73 | 4.03 ± 0.99 | |
| Group*T2 | 1.17 (1.00, ∞) | 0.28 | 0.84 | T3 | 0.52 | Hi. x T3 | 0.47 | FT. x T3 | 0.57 | 3.81 ± 1.11 | 4.20 ± 0.83 | |
| Group*T3 | 0.63 (1.00, ∞) | 0.43 | 0.85 | T4 | 0.44 | Hi. x T4 | 0.45 | FT. x T4 | 0.42 | 3.74 ± 1.15 | 3.67 ± 1.08 | |
| Group*T4 | 2.33 (1.00, ∞) | 0.13 | 0.85 | |||||||||
| Problem List | Group | 0.11 (1.00, ∞) | 0.74 | Hiking | 0.49 | Forest T. | 0.51 | mean ± SD | mean ± SD | |||
| Time | 3.43 (2.72, ∞) | 0.02 * | T1 | 0.52 | Hi. x T1 | 0.51 | FT. x T1 | 0.53 | 0.81 ± 1.45 | 1.04 ± 2.01 | ||
| Group*Time | 3.12 (2.72, ∞) | 0.03 * | T2 | 0.49 | Hi. x T2 | 0.47 | FT. x T2 | 0.51 | 0.50 ± 1.02 | 0.74 ± 1.34 | ||
| Group*T2 | 0.30 (1.00, ∞) | 0.58 | 1.00 | T3 | 0.47 | Hi. x T3 | 0.43 | FT. x T3 | 0.50 | 0.38 ± 1.08 | 0.91 ± 2.29 | |
| Group*T3 | 0.34 (1.00, ∞) | 0.34 | 1.00 | T4 | 0.53 | Hi. x T4 | 0.56 | FT. x T4 | 0.49 | 1.40 ± 2.47 | 0.78 ± 1.65 | |
| Group*T4 | 3.09 (1.00, ∞) | 0.08 | 1.00 | |||||||||
| Parameter | F1-LD-F1 Model | Relative Treatment Effects (RTE) | Descriptive Statistics | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | p | adj. p | Time | Hiking | Forest Therapy | Hiking | Forest Therapy | |||||
| Female | Group | 0.26 (1.00, ∞) | 0.61 | Hiking | 0.52 | Forest T. | 0.48 | mean ± SD | mean ± SD | |||
| erythrocytes | Time | 7.62 (1.83, ∞) | <0.01 ** | T1 | 0.54 | Hi. x T1 | 0.56 | FT. x T1 | 0.52 | 4.67 ± 0.36 | 4.61 ± 0.27 | |
| (106 µL) | Group*Time | 7.37 (1.83, ∞) | <0.01 ** | T2 | 0.44 | Hi. x T2 | 0.40 | FT. x T2 | 0.47 | 4.48 ± 0.31 | 4.56 ± 0.35 | |
| Group*T2 | 5.45 (1.00, ∞) | 0.02 * | 0.04 * | T3 | 0.52 | Hi. x T3 | 0.60 | FT. x T3 | 0.45 | 4.74 ± 0.41 | 4.52 ± 0.28 | |
| Group*T3 | 3.07 (1.00, ∞) | 0.08 | 0.08 | |||||||||
| Male | Group | 1.85 (1.00, ∞) | 0.17 | Hiking | 0.45 | Forest T. | 0.55 | mean ± SD | mean ± SD | |||
| erythrocytes | Time | 7.50 (1.74, ∞) | <0.01 ** | T1 | 0.56 | Hi. x T1 | 0.52 | FT. x T1 | 0.60 | 4.88 ± 0.29 | 4.99 ± 0.40 | |
| (106 µL) | Group*Time | 1.01 (1.74, ∞) | 0.36 | T2 | 0.44 | Hi. x T2 | 0.36 | FT. x T2 | 0.52 | 4.70 ± 0.28 | 4.87 ± 0.33 | |
| Group*T2 | 2.58 (1.00, ∞) | 0.11 | 0.22 | T3 | 0.49 | Hi. x T3 | 0.45 | FT. x T3 | 0.53 | 4.82 ± 0.28 | 4.91 ± 0.39 | |
| Group*T3 | 0.01 (1.00, ∞) | 0.92 | 0.92 | |||||||||
| Female | Group | 0.24 (1.00, ∞) | 0.97 | Hiking | 0.50 | Forest T. | 0.50 | mean ± SD | mean ± SD | |||
| hematocrit | Time | 9.92 (1.89, ∞) | <0.01 ** | T1 | 0.52 | Hi. x T1 | 0.53 | FT. x T1 | 0.51 | 42.01 ± 2.73 | 41.87 ± 2.08 | |
| (g/dL) | Group*Time | 3.67 (1.89, ∞) | 0.03 * | T2 | 0.42 | Hi. x T2 | 0.38 | FT. x T2 | 0.47 | 40.57 ± 2.80 | 41.46 ± 2.68 | |
| Group*T2 | 4.03 (1.00, ∞) | 0.04 * | 0.09 | T3 | 0.56 | Hi. x T3 | 0.60 | FT. x T3 | 0.52 | 42.74 ± 3.05 | 41.83 ± 2.19 | |
| Group*T3 | 0.66 (1.00, ∞) | 0.42 | 0.42 | |||||||||
| Male | Group | 5.23 (1.00, ∞) | 0.02 * | Hiking | 0.41 | Forest T. | 0.58 | mean ± SD | mean ± SD | |||
| hematocrit | Time | 9.23 (1.72, ∞) | <0.01 ** | T1 | 0.53 | Hi. x T1 | 0.46 | FT. x T1 | 0.60 | 44.60 ± 2.21 | 45.62 ± 3.15 | |
| (g/dL) | Group*Time | 1.18 (1.72, ∞) | 0.30 | T2 | 0.42 | Hi. x T2 | 0.30 | FT. x T2 | 0.53 | 43.10 ± 2.15 | 44.87 ± 2.53 | |
| Group*T2 | 3.11 (1.00, ∞) | 0.08 | 0.16 | T3 | 0.54 | Hi. x T3 | 0.47 | FT. x T3 | 0.61 | 44.75 ± 2.34 | 45.78 ± 2.99 | |
| Group*T3 | 0.02 (1.00, ∞) | 0.90 | 0.90 | |||||||||
| Reticulocytes | Group | 0.07 (1.00, ∞) | 0.79 | Hiking | 0.49 | Forest T. | 0.51 | mean ± SD | mean ± SD | |||
| (%) | Time | 24.78 (1.98, ∞) | <0.01 ** | T1 | 0.46 | Hi. x T1 | 0.47 | FT. x T1 | 0.46 | 1.51 ± 0.38 | 1.50 ± 0.35 | |
| Group*Time | 0.65 (1.98, ∞) | 0.52 | T2 | 0.61 | Hi. x T2 | 0.60 | FT. x T2 | 0.61 | 1.71 ± 0.41 | 1.72 ± 0.48 | ||
| Group*T2 | 0.23 (1.00, ∞) | 0.63 | 0.63 | T3 | 0.43 | Hi. x T3 | 0.41 | FT. x T3 | 0.45 | 1.42 ± 0.38 | 1.49 ± 0.36 | |
| Group*T3 | 0.18 (1.00, ∞) | 0.28 | 0.56 | |||||||||
| Immature | Group | 3.37 (1.00, ∞) | 0.07 | Hiking | 0.54 | Forest T. | 0.46 | mean ± SD | mean ± SD | |||
| reticulocyte | Time | 73.35 (1.98, ∞) | <0.01 ** | T1 | 0.47 | Hi. x T1 | 0.49 | FT. x T1 | 0.44 | 10.74 ± 4.10 | 9.98 ± 3.69 | |
| fraction (IRF) | Group*Time | 2.99 (1.98, ∞) | 0.05 | T2 | 0.67 | Hi. x T2 | 0.74 | FT. x T2 | 0.59 | 14.64 ± 4.42 | 12.31 ± 4.91 | |
| (%) | Group*T2 | 4.35 (1.00, ∞) | 0.04 * | 0.07 | T3 | 0.44 | Hi. x T3 | 0.39 | FT. x T3 | 0.35 | 9.06 ± 3.00 | 8.81 ± 3.41 |
| Group*T3 | 0.95 (1.00, ∞) | 0.95 | 0.95 | |||||||||
| Leukocytes | Group | 0.21 (1.00, ∞) | 0.65 | Hiking | 0.51 | Forest T. | 0.49 | mean ± SD | mean ± SD | |||
| (10³ µL) | Time | 14.76 (1.94, ∞) | <0.01 * | T1 | 0.53 | Hi. x T1 | 0.54 | FT. x T1 | 0.53 | 6.96 ± 1.47 | 7.10 ± 1.81 | |
| Group*Time | 0.47 (1.94, ∞) | 0.62 | T2 | 0.43 | Hi. x T2 | 0.44 | FT. x T2 | 0.41 | 6.43 ± 1.39 | 6.54 ± 1.93 | ||
| Group*T2 | 0.22 (1.00, ∞) | 0.64 | 0.64 | T3 | 0.54 | Hi. x T3 | 0.56 | FT. x T3 | 0.52 | 7.17 ± 1.76 | 6.89 ± 1.57 | |
| Group*T3 | 1.27 (1.00, ∞) | 0.26 | 0.52 | |||||||||
| Female | Group | 0.41 (1.00, ∞) | 0.52 | Hiking | 0.53 | Forest T. | 0.47 | mean ± SD | mean ± SD | |||
| aerobic | Time | 4.94 (1.94, ∞) | 0.01 * | T1 | 0.46 | Hi. x T1 | 0.42 | FT. x T1 | 0.49 | 29.71 ± 3.73 | 30.31 ± 5.60 | |
| capacity | Group*Time | 4.68 (1.94, ∞) | 0.01 * | T2 | 0.59 | Hi. x T2 | 0.70 | FT. x T2 | 0.48 | 33.56 ± 4.18 | 30.19 ± 5.29 | |
| (mlO2/kg/min) | Group*T2 | 7.95 (1.00, ∞) | <0.01 ** | 0.01 * | T3 | 0.46 | Hi. x T3 | 0.53 | FT. x T3 | 0.45 | 30.90 ± 3.87 | 29.60 ± 5.96 |
| Group*T3 | 1.11 (1.00, ∞) | 0.29 | 0.29 | |||||||||
| Male | Group | 0.87 (1.00, ∞) | 0.35 | Hiking | 0.46 | Forest T. | 0.54 | mean ± SD | mean ± SD | |||
| aerobic | Time | 3.49 (1.72, ∞) | 0.04 * | T1 | 0.42 | Hi. x T1 | 0.43 | FT. x T1 | 0.42 | 31.07 ± 4.73 | 31.13 ± 6.04 | |
| capacity | Group*Time | 0.88 (1.72, ∞) | 0.40 | T2 | 0.58 | Hi. x T2 | 0.52 | FT. x T2 | 0.65 | 33.21 ± 6.17 | 34.86 ± 4.85 | |
| (mlO2/kg/min) | Group*T2 | 0.96 (1.00, ∞) | 0.33 | 0.38 | T3 | 0.48 | Hi. x T3 | 0.42 | FT. x T3 | 0.54 | 30.90 ± 3.87 | 32.39 ± 6.97 |
| Group*T3 | 1.72 (1.00, ∞) | 0.19 | 0.38 | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huber, D.; Freidl, J.; Pichler, C.; Bischof, M.; Kiem, M.; Weisböck-Erdheim, R.; Squarra, G.; De Nigris, V.; Resnyak, S.; Neberich, M.; et al. Long-Term Effects of Mountain Hiking vs. Forest Therapy on Physical and Mental Health of Couples: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2023, 20, 1469. https://doi.org/10.3390/ijerph20021469
Huber D, Freidl J, Pichler C, Bischof M, Kiem M, Weisböck-Erdheim R, Squarra G, De Nigris V, Resnyak S, Neberich M, et al. Long-Term Effects of Mountain Hiking vs. Forest Therapy on Physical and Mental Health of Couples: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2023; 20(2):1469. https://doi.org/10.3390/ijerph20021469
Chicago/Turabian StyleHuber, Daniela, Johanna Freidl, Christina Pichler, Michael Bischof, Martin Kiem, Renate Weisböck-Erdheim, Gabriella Squarra, Vincenzo De Nigris, Stefan Resnyak, Marcel Neberich, and et al. 2023. "Long-Term Effects of Mountain Hiking vs. Forest Therapy on Physical and Mental Health of Couples: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 20, no. 2: 1469. https://doi.org/10.3390/ijerph20021469
APA StyleHuber, D., Freidl, J., Pichler, C., Bischof, M., Kiem, M., Weisböck-Erdheim, R., Squarra, G., De Nigris, V., Resnyak, S., Neberich, M., Bordin, S., Zechner, R., & Hartl, A. (2023). Long-Term Effects of Mountain Hiking vs. Forest Therapy on Physical and Mental Health of Couples: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 20(2), 1469. https://doi.org/10.3390/ijerph20021469