


Perception among NHIS–HMO Enrolees of the Attitudes of Medical Personnel during Outpatient Care in Lagos Hospitals
 ,
,  ,
,
Abstract
:1. Introduction
1.1. Theoretical Framework
Assessment of the Quality of Medical Care through the Lens of Social Phenomenology
2. Materials and Methods
2.1. Sample Size and Sampling Procedure
2.1.1. Quantitative Sample Size Determination
2.1.2. Study Population
2.1.3. Justification for HCPs/HCFs Selection
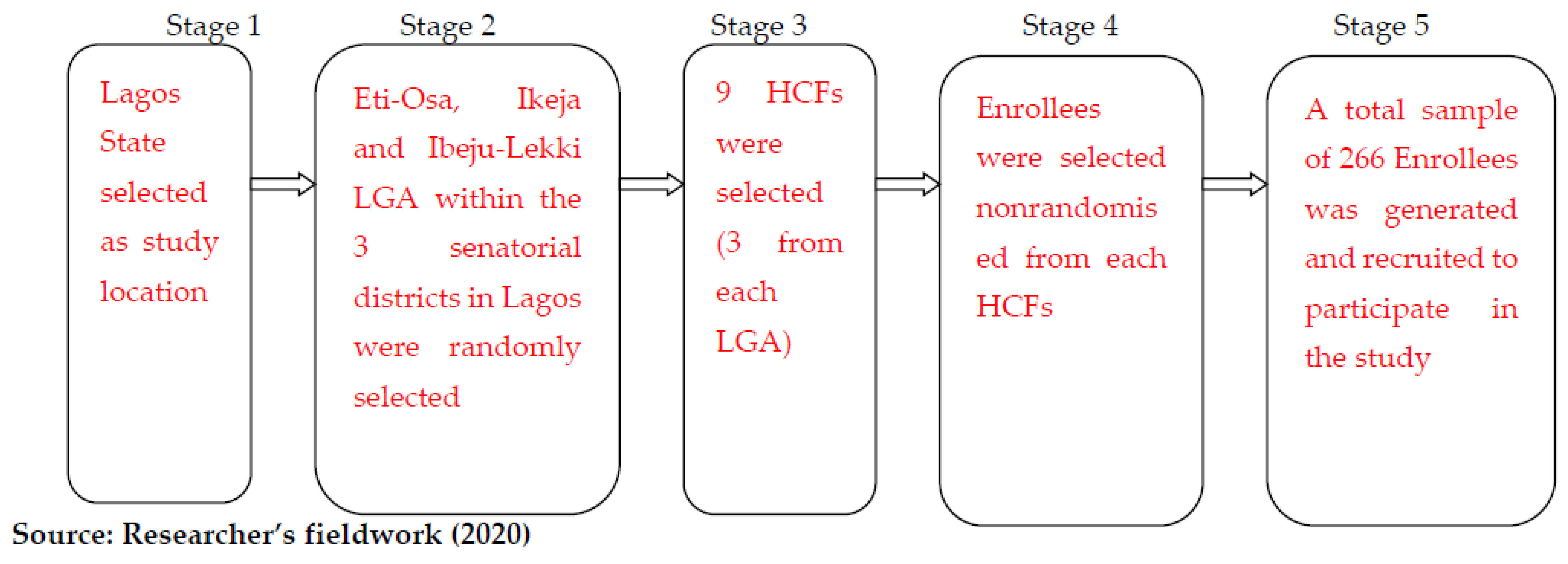
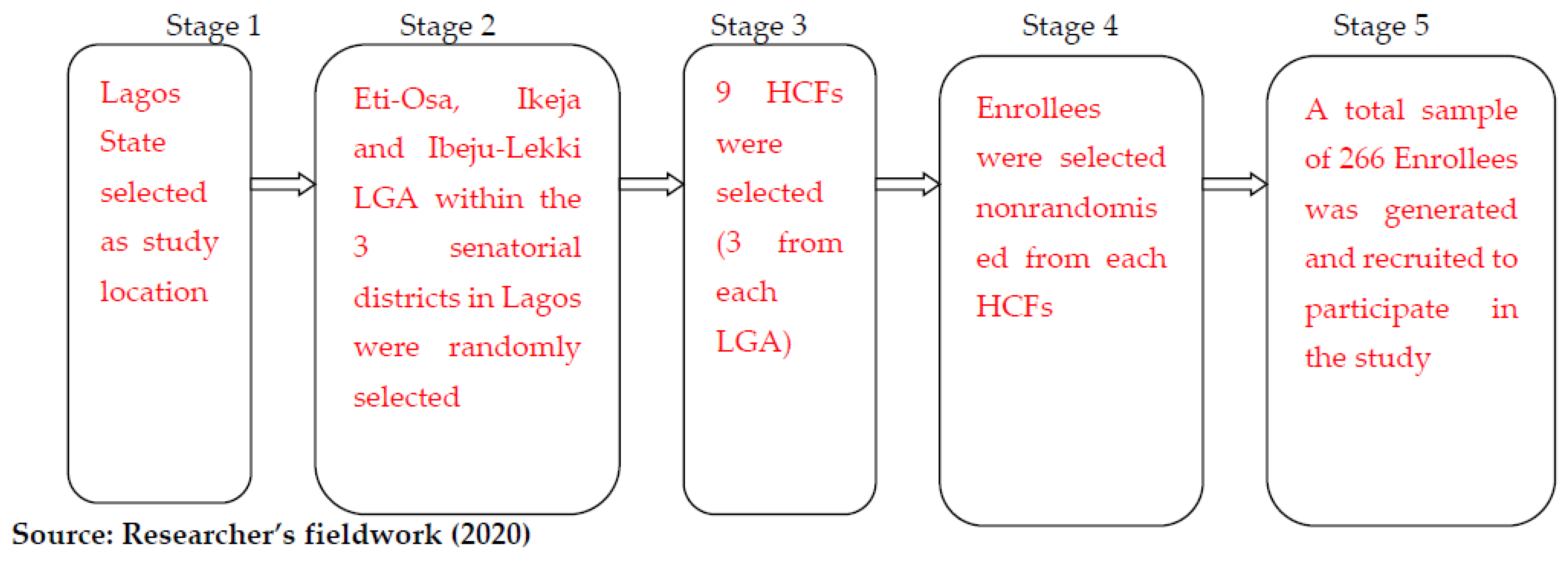
2.1.4. Quantitative Sampling Technique
2.1.5. Validity and Reliability of the Research Instrument
2.1.6. Method of Data Collection
2.2. Research Instruments
Quantitative Data Collection Instrument
2.3. Questionnaires and Scales
2.3.1. Attitude Questionnaire
2.3.2. Self-Efficacy for Attitude Perception Scale
2.4. Qualitative Data Collection Instrument
In-Depth Interview (IDI)
2.5. Method of Data Analysis
2.5.1. Quantitative Data Analysis
2.5.2. Qualitative Data Analysis
2.6. Ethical Approval and Informed Consent
3. Results
“The level of empathy from the healthcare workers beginning from the gate is so appalling”.(IDI 4. Male, 60)
“I am still in pain, but what can I do? If you complain, you get delayed, or you are labelled a troublemaker”.(IDI 1. Female, 25)
“The medical facility needs to employ more personnel or refer to other facilities to ensure personnel do not feel burdened as this is obvious in the way they tend to relate with us, the patients”.(IDI 3. Female, 28)
Test of Hypothesis
4. Discussion
4.1. Strength and Limitations of the Study
- The study was limited to enrolees visiting the selected hospitals for outpatient care not inclusive of enrolees who were present at the selected hospitals for inpatient care during the study period.
- The study was also limited to enrolees visiting selected HCFs in Lagos State; therefore, the result is not relevant to the other thirty-five (35) states in Nigeria.
- The qualitative study was limited to IDI.
- The qualitative method of analysis was limited to inductive content analysis while the quantitative was limited to Chi-square and Spearman’s correlation analysis.
4.2. Prospect for Future Research
- The same study should be replicated in the other seventeen (17) local government areas of the state, and the results should be compared.
- Research should also be conducted to find out the determining factors responsible for enrolees’ choice of hospital utilization and its consequences on the perceived quality of medical personnel attitudes.
- Considering the methods of analysis in this study, studies should be conducted with other methods of analysis for the purpose of replicability.
- Furthermore, a comparative study should be carried out on the same study.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Entwistle, V.A.; Alan, C.; John, O. Why health and social care support for people with long-term conditions should be oriented towards enabling them to live well. Health Care Anal. 2018, 26, 48–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- British Medical Association. The Medical Profession and Human Rights: Handbook for a Changing Agenda. Zed Books. 2001. Available online: https://guide-humanitarian-law.org/content/article/3/medical-personnel/ (accessed on 15 December 2022).
- Albinsson, G.; Carlsson-Blomster, M.; Gunilla, L. In search of a caring relationship-Nursing students’ notions of interactions in the nurse-patient relationship. Nurse Educ. Pract. 2021, 50, 102954. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Tsung-hsi, F. Policies and transformation of long-term care system in Taiwan. Ann. Geriatr. Med. Res. 2020, 24, 187. [Google Scholar] [CrossRef] [PubMed]
- Manyisa, Z.M.; Elsie, J.V. Factors affecting working conditions in public hospitals: A literature review. Int. J. Afr. Nurs. Sci. 2017, 6, 28–38. [Google Scholar] [CrossRef]
- Mosadeghrad, A.M. A conceptual framework for quality of care. Mater. Socio-Med. 2012, 24, 251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adeniran, A.S.; Aun, I.I.; Fawole, A.A.; Aboyeji, A.P. Comparative analysis of caesarean delivery among out-of-pocket and health insurance clients in Ilorin, Nigeria. Niger. Postgrad. Med. J. 2020, 27, 108. [Google Scholar] [CrossRef] [PubMed]
- Abba-Aji, M.; Balabanova, D.; Hutchinson, E.; McKee, M. How do Nigerian newspapers report corruption in the health system? Int. J. Health Policy Manag. 2021, 10, 77. [Google Scholar] [CrossRef]
- Sui, Y.; Ahuru, R.R.; Huang, K.; Anser, M.K.; Osabohien, R. Household socioeconomic status and antenatal care utilization among women in the reproductive-age. Front. Public Health 2021, 9, 724337. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Anser, M.K.; Ahuru, R.R.; Zhang, Z.; Peng, M.Y.; Osabohien, R.; Mirza, M. Do Predictors of Health Facility Delivery Among Reproductive-Age Women Differ by Health Insurance Enrollment? A Multi-Level Analysis of Nigeria’s Data. Front. Public Health 2022, 10, 797272. [Google Scholar] [CrossRef] [PubMed]
- Levesque, J.; Mark, H.; Grant, R. Patient-centred access to health care: Conceptualising access at the interface of health systems and populations. Int. J. Equity Health 2013, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Henderson, S.; Maria, H.; Ruth, H.; Elizabeth, K. Cultural competence in healthcare in the community: A concept analysis. Health Soc. Care Community 2018, 26, 590–603. [Google Scholar] [CrossRef]
- Schutz, A. Collected Papers I. The problem of Social Reality. 11; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Kim, K.; Tim, B. Typification in society and social science: The continuing relevance of Schutz’s social phenomenology. Hum. Stud. 2009, 32, 263–289. [Google Scholar] [CrossRef]
- Lehman, B.J.; Diana, M.D.; Jennifer, A.G. Rethinking the biopsychosocial model of health: Understanding health as a dynamic system. Soc. Personal. Psychol. Compass 2017, 11, e12328. [Google Scholar] [CrossRef] [Green Version]
- Mkperedem, A.A.; Ogunlade, P.; Igbolekwu, C.O.; Asamu, F.; Rasak, B.; Arisukwu, O.C. Impact of Quality Healthcare Equipment And Physical Structure on Nhis-Hmo Outpatient Enrollees’ Perception In Lagos Hospitals. Res. Sq. 2020. [Google Scholar] [CrossRef]
- Garson, G.D. Testing Statistical Assumptions; Statistical Associates Publishing: Asheboro, NC, USA, 2012; pp. 15–40. [Google Scholar]
- Pett, M.A.; Nancy, R.L.; John, J.S. Making Sense of Factor Analysis: The Use of Factor Analysis for Instrument Development in Health Care Research; Sage: Thousand Oaks, CA, USA, 2003; Volume 1, pp. 121–152. Available online: https://books.google.com.ng/books?hl=en&lr=&id=9kB5jE2IjS4C&oi=fnd&pg=PR9&dq=17.%09Pett,+M.+A.%3B+Nancy,+R.+L.%3B+John,+J.+S.+Making+sense+of+factor+analysis:+The+use+of+factor+analysis+for+instrument+development+in+health+care+research.+Sage,+2003&ots=yZv23xlre6&sig=mjUUssdGwGt5Gnri4GQcjfnTCcg&redir_esc=y#v=onepage&q=17.%09Pett%2C%20M.%20A.%3B%20Nancy%2C%20R.%20L.%3B%20John%2C%20J.%20S.%20Making%20sense%20of%20factor%20analy-sis%3A%20The%20use%20of%20factor%20analysis%20for%20instrument%20development%20in%20health%20care%20research.%20Sage%2C%202003&f=false (accessed on 15 December 2022).
- Ndiyo, N.A. Fundamentals of Research in Behavioural Sciences and Humanities 2005. Available online: https://scholar.google.com/scholar?hl=en&as_sdt=0%2C5&q=Ndiyo%2C+N.+A.+Fundamentals+of+Research+in+Behavioural+Sciences+and+Humanities.+2005.&btnG= (accessed on 15 December 2022).
- Donabedian, A. Quality Assessment and Assurance: Unity of Purpose, Diversity of Means. Inquiry 1988, 1, 173–192. Available online: https://www.jstor.org/stable/29771941 (accessed on 15 December 2022).
- Danaa, S.; Kim, P.S. Health Care Reform in Ghana: Factors Affecting Insurance Enrollment. J. Korean Afr. Soc. 2019, 57, 119–157. Available online: https://www.dbpia.co.kr/Journal/articleDetail?nodeId=NODE09221220 (accessed on 15 December 2022).
- Hussien, M.; Azage, M.; Bayou, N.B. A mixed methods study of community-based health insurance enrollment trends and underlying challenges in two districts of northeast Ethiopia: A proxy for its sustainability. PLoS ONE 2022, 17, e0266583. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | Label | Frequency (N = 252) | Percentage (%) |
|---|---|---|---|
| Marital Status | Single | 70 | 27.8 |
| Married | 134 | 53.2 | |
| Other | 48 | 19.0 | |
| Sex | Male | 82 | 32.5 |
| Female | 170 | 67.5 | |
| Age | 18–20 | 22 | 8.7 |
| 21–30 | 66 | 26.2 | |
| 31–40 | 93 | 36.9 | |
| 41–50 | 25 | 9.9 | |
| 51–65 | 46 | 18.3 | |
| Educational Qualification | No Formal Education | 22 | 8.7 |
| First Leaving School Certificate | 15 | 6.0 | |
| Secondary School | 34 | 13.5 | |
| OND/NCE | 32 | 12.7 | |
| HND/B.Sc | 101 | 40.1 | |
| M.Sc/MBA/M.Ed | 38 | 15.1 | |
| Ph.D. | 10 | 4.0 | |
| Public–Private Partnership Enrolment | Public NHIS | 47 | 18.7 |
| Private HMO | 205 | 81.3 | |
| Healthcare Facility/Healthcare Provider (HCFs/HCPs) Utilization | Public/Government HCFs/HCPs | 44 | 17.5 |
| Private HCFs/HCPs | 208 | 82.5 |
| Variable | Responses | Frequency | Percentage (%) |
|---|---|---|---|
| The medical personnel’s attitude during my outpatient care was humane and respectful | Strongly Agreed | 79 | 31.3 |
| Agreed | 97 | 38.5 | |
| Undecided | 1 | 0.5 | |
| Disagree | 49 | 19.4 | |
| Strongly Disagree | 26 | 10.3 | |
| Total (%) | 252 | 100 | |
| My medical history (previous illnesses and family history) was factored in during treatment | Strongly Agreed | 62 | 24.6 |
| Agreed | 114 | 45.2 | |
| Undecided | 18 | 7.1 | |
| Disagree | 47 | 18.7 | |
| Strongly Disagree | 11 | 4.4 | |
| Total (%) | 252 | 100 | |
| The medical personnel’s attitude motivated me to follow the treatment prescribed. | Strongly Agreed | 47 | 18.7 |
| Agreed | 87 | 34.5 | |
| Undecided | 29 | 11.5 | |
| Disagree | 33 | 13.1 | |
| Strongly Disagree | 56 | 22.2 | |
| Total (%) | 252 | 100 |
| Variable | Perception | Frequency | Percentage (%) |
|---|---|---|---|
| Respondents’ ratings of medical personnel attitude | Good | 135 | 53.6 |
| Average | 40 | 15.9 | |
| Bad | 77 | 30.5 | |
| Total | 252 | 100 |
| Response | Good | Average | Bad | Total | χ2 |
|---|---|---|---|---|---|
| Perception (%) | Perception (%) | Perception (%) | |||
| Attitude | |||||
| Very Good | 24 (29.8) | 7 (14.9) | 16 (34) | 47 (100.0) | χ2 = 82.265 |
| Good | 67 (77) | 8 (9.2) | 12 (13.8) | 87 (100.0) | r = 0.219 |
| Neutral | 12 (41.3) | 5 (19.4) | 12 (41.4) | 29 (100.0) | p = 0.000 |
| Bad | 12 (36.4) | 7 (17.2) | 14 (42.4) | 33 (100.0) | df = 16 |
| Very bad | 20 (35.7) | 13 (21.2) | 23 (41.1) | 56 (100.0) | |
| Total | 135 (53.6) | 40 (15.9) | 77 (30.6) | 252 (100.0) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mkperedem, A.A.; Ogunlade, P.; Igbolekwu, C.; Arisukwu, O.; Owa, S.O.; Afolabi, A.O.; Etta-Oyong, S.O. Perception among NHIS–HMO Enrolees of the Attitudes of Medical Personnel during Outpatient Care in Lagos Hospitals. Int. J. Environ. Res. Public Health 2023, 20, 1218. https://doi.org/10.3390/ijerph20021218
Mkperedem AA, Ogunlade P, Igbolekwu C, Arisukwu O, Owa SO, Afolabi AO, Etta-Oyong SO. Perception among NHIS–HMO Enrolees of the Attitudes of Medical Personnel during Outpatient Care in Lagos Hospitals. International Journal of Environmental Research and Public Health. 2023; 20(2):1218. https://doi.org/10.3390/ijerph20021218
Chicago/Turabian StyleMkperedem, Abigail Affiong, Peter Ogunlade, Chisaa Igbolekwu, Ogadimma Arisukwu, Stephen Olugbenga Owa, Abiodun Olawale Afolabi, and Stephen Otu Etta-Oyong. 2023. "Perception among NHIS–HMO Enrolees of the Attitudes of Medical Personnel during Outpatient Care in Lagos Hospitals" International Journal of Environmental Research and Public Health 20, no. 2: 1218. https://doi.org/10.3390/ijerph20021218
APA StyleMkperedem, A. A., Ogunlade, P., Igbolekwu, C., Arisukwu, O., Owa, S. O., Afolabi, A. O., & Etta-Oyong, S. O. (2023). Perception among NHIS–HMO Enrolees of the Attitudes of Medical Personnel during Outpatient Care in Lagos Hospitals. International Journal of Environmental Research and Public Health, 20(2), 1218. https://doi.org/10.3390/ijerph20021218