



Effect of Resistance Exercise Order on Cardiovascular Disease Risk Factors in Older Women: A Randomized Controlled Trial
 , , , ,
, , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Design
2.2. Participants
2.3. Fat Mass and Trunk Fat
2.4. Metabolic Biomarkers
2.5. Dietary Intake
2.6. Muscular Strength
2.7. Resistance Training Program
2.8. Statistical Analyses
3. Results
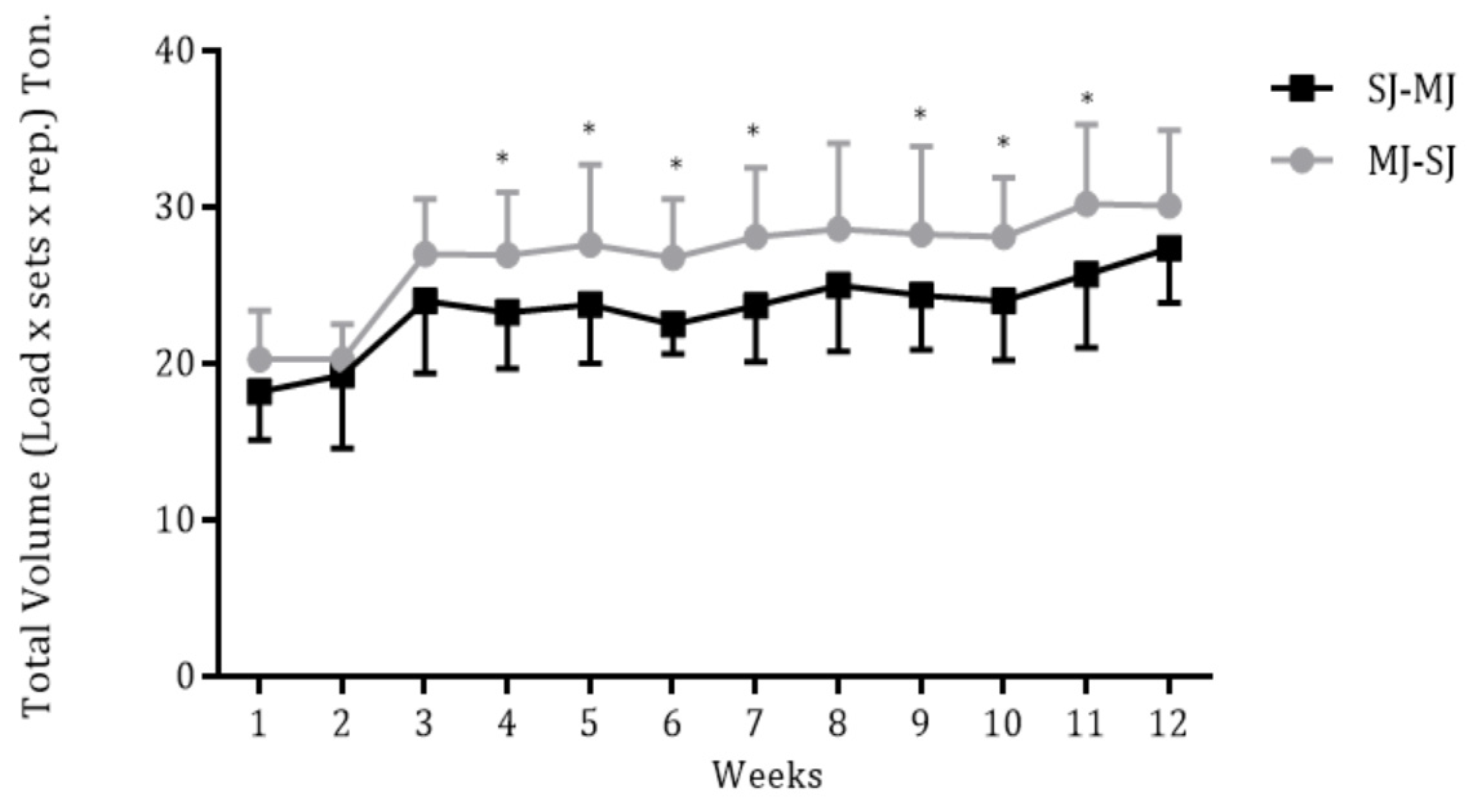
3.1. Volume Load
3.2. Dietary Intake and Main Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Appelman, Y.; van Rijn, B.B.; Ten Haaf, M.E.; Boersma, E.; Peters, S.A. Sex differences in cardiovascular risk factors and disease prevention. Atherosclerosis 2015, 241, 211–218. [Google Scholar] [CrossRef]
- Kengne, A.P.; Batty, G.D.; Hamer, M.; Stamatakis, E.; Czernichow, S. Association of C-reactive protein with cardiovascular disease mortality according to diabetes status: Pooled analyses of 25,979 participants from four U.K. prospective cohort studies. Diabetes Care 2012, 35, 396–403. [Google Scholar] [CrossRef]
- Maltais, M.L.; Desroches, J.; Dionne, I.J. Changes in muscle mass and strength after menopause. J. Musculoskelet Neuronal Interact. 2009, 9, 186–197. [Google Scholar]
- Pearson, T.A.; Mensah, G.A.; Alexander, R.W.; Anderson, J.L.; Cannon, R.O., 3rd; Criqui, M.; Fadl, Y.Y.; Fortmann, S.P.; Hong, Y.; Myers, G.L.; et al. Markers of inflammation and cardiovascular disease: Application to clinical and public health practice: A statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation 2003, 107, 499–511. [Google Scholar] [CrossRef]
- Ihalainen, J.K.; Inglis, A.; Mäkinen, T.; Newton, R.U.; Kainulainen, H.; Kyröläinen, H.; Walker, S. Strength training improves metabolic health markers in older individual regardless of training frequency. Front. Physiol. 2019, 10, 32. [Google Scholar] [CrossRef] [PubMed]
- Cunha, P.M.; Tomeleri, C.M.; Nascimento, M.A.; Mayhew, J.L.; Fungari, E.; Cyrino, L.T.; Barbosa, D.S.; Venturini, D.; Cyrino, E.S. Comparision of low and high volume of resistance training on body fat and blood biomarkers in untrained older women: A randomized clinical trial. J. Strength Cond. Res. 2021, 35, 1–8. [Google Scholar] [CrossRef] [PubMed]
- ACSM American College of Sports Medicine Position Stand. Progression models in resistance training for healthy adults. Med. Sci. Sports Exerc. 2009, 41, 687–708. [Google Scholar] [CrossRef] [PubMed]
- Westcott, W.L. Resistance training is medicine: Effects of strength training on health. Curr. Sports Med. Rep. 2012, 11, 209–216. [Google Scholar] [CrossRef]
- Bezerra, E.S.; Schoenfeld, B.J.; Paz, G.; Farias, D.A.; Sakugawa, R.L.; Vieira, I.; Rossato, M.; Miranda, H. Effect of exercise order with barbell and machine modalities on upper body volume load and myoelectric activity. Sports Biomech. 2020, 19, 778–791. [Google Scholar] [CrossRef] [PubMed]
- Nunes, J.P.; Grgic, J.; Cunha, P.M.; Ribeiro, A.S.; Schoenfeld, B.J.; de Salles, B.F.; Cyrino, E.S. What influence does resistance exercise order have on muscular strength gains and muscle hypertrophy? A systematic review and meta-analysis. Eur. J. Sport Sci. 2021, 21, 149–157. [Google Scholar] [CrossRef]
- Tomeleri, C.M.; Ribeiro, A.S.; Nunes, J.P.; Schoenfeld, B.J.; Souza, M.F.; Schiavoni, D.; Junior, P.S.; Cavaglieri, C.R.; Cunha, P.M.; Venturini, D.; et al. Influence of resistance training exercise order on muscle strength, hypertrophy, and anabolic hormones in older women: A randomized controlled trial. J. Strength Cond. Res. 2020, 34, 3103–3109. [Google Scholar] [CrossRef] [PubMed]
- Sforzo, G.A.; Touey, P.R. Manipulating exercise order affects muscular performance during a resistance exercise training session. J. Strength Cond. Res. 1996, 10, 20–24. [Google Scholar]
- Avelar, A.; Ribeiro, A.S.; Nunes, J.P.; Schoenfeld, B.J.; Papst, R.R.; Trindade, M.C.C.; Bottaro, M.; Cyrino, E.S. Effects of order of resistance training exercises on muscle hypertrophy in young adult men. Appl. Physiol. Nutr. Metab. 2019, 44, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Dias, I.; de Salles, B.F.; Novaes, J.; Costa, P.B.; Simão, R. Influence of exercise order on maximum strength in untrained young men. J. Sci. Med. Sport. 2010, 13, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Dib, M.M.; Tomeleri, C.M.; Nunes, J.P.; Cunha, P.M.; Ribeiro, A.S.; Schiavoni, D.; Cavalcante, E.F.; Kunevaliki, G.; Teixeira, D.C.; de Oliveira, A.R.; et al. Effects of three resistance exercise orders on muscular function and body composition in older women. Int. J. Sports Med. 2020, 41, 1024–1031. [Google Scholar] [CrossRef] [PubMed]
- Cunha, P.M.; Nunes, J.P.; Werneck, A.O.; Ribeiro, A.S.; Machado, D.G.S.; Kassiano, W.; Costa, B.D.V.; Cyrino, L.T.; Antunes, M.; Kunevaliki, G.; et al. Effect of resistance exercise orders on health parameters in trained older women: A randomized crossover trial. Med. Sci. Sports Exerc. 2023, 55, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Nunes, J.P.; Marcori, A.J.; Tomeleri, C.M.; Nascimento, M.A.; Mayhew, J.L.; Ribeiro, A.S.; Cyrino, E.S. Starting the resistance-training session with lower-body exercises provides lower session perceived exertion without altering the training volume in older women. Int. J. Exerc. Sci. 2019, 12, 1187–1197. [Google Scholar]
- Longo, A.R.; Silva-Batista, C.; Pedroso, K.; Painelli, V.D.S.; Lasevicius, T.; Schoenfeld, B.J.; Aihara, A.Y.; Peres, B.D.A.; Tricoli, V.; Teixeira, E.L. Volume load rather than resting interval influences muscle hypertrophy during high-intensity resistance training. J. Strength Cond. Res. 2022, 36, 1554–1559. [Google Scholar] [CrossRef]
- Pedersen, B.K. Muscles and their myokines. J. Exp. Biol. 2011, 214 Pt 2, 337–346. [Google Scholar] [CrossRef]
- Witko-Sarsat, V.; Friedlander, M.; Capeillere-Blandin, C.; Nguyen-Khoa, T.; Nguyen, A.T.; Zingraff, J.; Jungers, P.; Descamps-Latscha, B. Advanced ocidation protein products as a novel marker of oxidative stress in uremia. Kidney Int. 1996, 49, 1304–1313. [Google Scholar] [CrossRef]
- Repetto, M.; Reides, C.; Gomez Carretero, M.L.; Costa, M.; Griemberg, G.; Llesuy, S. Oxidative stress in blood of HIV infected patients. Clin. Chim. Acta 1996, 255, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Guevara, I.; Iwanejko, J.; Dembińska-Kieć, A.; Pankiewicz, J.; Wanat, A.; Anna, P.; Gołąbek, I.; Bartuś, S.; Malczewska-Malec, M.; Szczudlik, A. Determination of nitrite/nitrate in human biological material by the simple Griess reaction. Clin. Chim. Acta 1998, 274, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, A.M.; Januario, R.S.; Gerage, A.M.; Mayhew, J.L.; Cheche, P.; Cyrino, E.S. Familiarization and reliability of one repetition maximum strength testing in older women. J. Strength Cond. Res. 2013, 27, 1136–1142. [Google Scholar]
- Cohen, J. A power primer. Psychol Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, A.; Monteiro, N.; Nunes, J.; Cunha, P.; Andrade-Lima, A.; Aguiar, A.; Cyrino, E. Effects of four exercise orders on perceived exertion, feeling, and arousal in older women following 12 weeks of resistance training. Sci. Sports 2020, 36, 176–178. [Google Scholar] [CrossRef]
- Buskard, A.N.L.; Jacobs, K.A.; Eltoukhy, M.M.; Strand, K.L.; Villanueva, L.; Desai, P.P.; Signorile, J.F. Optimal approach to load progressions during strength training in older adults. Med. Sci. Sports Exerc. 2019, 51, 2224–2233. [Google Scholar] [CrossRef] [PubMed]
- Morishita, S.; Tsubaki, A.; Nakamura, M.; Nashimoto, S.; Fu, J.B.; Onishi, H. Rating of perceived exertion on resistance training in elderly subjects. Expert Rev. Cardiovasc. Ther. 2019, 17, 135–142. [Google Scholar] [CrossRef]
- Morton, R.W.; Colenso-Semple, L.; Phillips, S.M. Training for strength and hypertrophy: An evidence-based approach. Curr. Opin. Physiol. 2019, 11, 149–150. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Febbraio, M.A. Muscle as an endocrine organ: Focus on muscle-derived interleukin-6. Physiol. Rev. 2008, 88, 1379–1406. [Google Scholar] [CrossRef]
- Bonaccio, M.; Di Castelnuovo, A.; Pounis, G.; De Curtis, A.; Costanzo, S.; Persichillo, M.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; Iacoviello, L. A score of low-grade inflammation and risk of mortality: Prospective findings from the Moli-sani study. Haematologica 2016, 101, 1434–1441. [Google Scholar] [CrossRef]
- Zamboni, M.; Rossi, A.P.; Fantin, F.; Zamboni, G.; Chirumbolo, S.; Zoico, E.; Mazzali, G. Adipose tissue, diet and aging. Mech. Ageing Dev. 2014, 136–137, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Azizbeigi, K.; Azarbayjani, M.A.; Atashak, S.; Stannard, S.R. Effect of moderate and high resistance training intensity on indices of inflammatory and oxidative stress. Res. Sports Med. 2015, 23, 73–87. [Google Scholar] [CrossRef] [PubMed]
- Cunha, P.M.; Ribeiro, A.S.; Nunes, J.P.; Tomeleri, C.M.; Nascimento, M.A.; Moraes, G.K.; Junior, P.S.; Barbosa, D.S.; Venturini, D.; Cyrino, E.S.; et al. Resistance training performed with single-set is sufficient to reduce cardiovascular risk factors in untrained older women: The randomized clinical trial. Active Aging Longitudinal Study. Arch. Gerontol. Geriatr. 2019, 81, 171–175. [Google Scholar] [CrossRef]
- Tomeleri, C.M.; Ribeiro, A.S.; Souza, M.F.; Schiavoni, D.; Schoenfeld, B.J.; Venturini, D.; Barbosa, D.S.; Landucci, K.; Sardinha, L.B.; Cyrino, E.S. Resistance training improves inflammatory level, lipid and glycemic profiles in obese older women: A randomized controlled trial. Exp. Gerontol. 2016, 84, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Cavalcante, E.F.; Ribeiro, A.S.; Nascimento, M.A.D.; Silva, A.M.; Tomeleri, C.M.; Nabuco, H.C.; Pina, F.L.C.; Mayhew, J.L.; Da Silva-Grigoletto, M.E.; da Silva, D.R.P.; et al. Effects of different resistance training frequencies on fat in overweight/obese older women. Int. J. Sports Med. 2018, 39, 527–534. [Google Scholar] [CrossRef]
- Wang, H.; Eckel, R.H. Lipoprotein lipase: From gene to obesity. Am. J. Physiol. Endocrinol. Metab. 2009, 297, E271–E288. [Google Scholar] [CrossRef]
- Orsatti, F.; Nahas, E.; Maestá, N.; Neto, J.N.; Orsatti, C.; Portari, G.V.; Burini, R.C. Effects of resistance training frequency on body composition and metabolics and inflammatory markers in overweight postmenopausal women. J. Sports Med. Phys. Fit. 2014, 54, 317–325. [Google Scholar]
- Marques, E.; Carvalho, J.; Soares, J.M.; Marques, F.; Mota, J. Effects of resistance and multicomponent exercise on lipid profiles of older women. Maturitas 2009, 63, 84–88. [Google Scholar] [CrossRef]
- Ribeiro, A.S.; Deminice, R.; Schoenfeld, B.J.; Tomeleri, C.M.; Padilha, C.S.; Venturini, D.; Barbosa, D.S.; Sardinha, L.B.; Cyrino, E.S. Effect of resistance training systems on oxidative stress in older women. Int. J. Sport Nutr. Exerc. Metab. 2017, 27, 439–447. [Google Scholar] [CrossRef]
- Padilha, C.S.; Ribeiro, A.S.; Fleck, S.J.; Nascimento, M.A.; Pina, F.L.; Okino, A.M.; Venturini, D.; Barbosa, D.S.; Mayhew, J.L.; Cyrino, E.S. Effect of resistance training with different frequencies and detraining on muscular strength and oxidative stress biomarkers in older women. Age 2015, 37, 104. [Google Scholar] [CrossRef]
- McHugh, M.P.; Connolly, D.A.; Eston, R.G.; Gleim, G.W. Exercise-induced muscle damage and potential mechanisms for the repeated bout effect. Sports Med. 1999, 27, 157–170. [Google Scholar] [CrossRef] [PubMed]
- Lacroix, A.; Hortobágyi, T.; Beurskens, R.; Granacher, U. Effects of supervised vs. unsupervised training programs on balance and muscle strength in older adults: A systematic review and meta-analysis. Sports Med. 2017, 47, 2341–2361. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Campillo, R.; Martínez, C.; de La Fuente, C.I.; Cadore, E.L.; Marques, M.C.; Nakamura, F.Y.; Loturco, I.; Caniuqueo, A.; Cañas, R.; Izquierdo, M. High-speed resistance training in older women: The role of supervision. J. Aging Phys. Act. 2017, 25, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, E.K.; Fung, E.B. Precision of the hologic DXA in the assessment of visceral adipose tissue. J. Clin. Densitom. 2020, 23, 664–672. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Measures | MJ-SJ (n = 15) | SJ-MJ (n = 14) | CON (n = 15) | |||
|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | |
| Dietary intake | ||||||
| Energy (kcal/kg) | 16.1 ± 3.4 | 16.2 ± 3.9 | 16.2 ± 3.9 | 16.7 ± 3.1 | 16.1 ± 3.2 | 16.4 ± 3.5 |
| Carbohydrates (g/kg) | 2.3 ± 0.7 | 2.3 ± 0.6 | 2.6 ± 0.9 | 2.5 ± 0.7 | 2.5 ± 0.7 | 2.3 ± 0.9 |
| Proteins (g/kg) | 0.8 ± 0.3 | 0.8 ± 0.3 | 0.8 ± 0.3 | 0.9 ± 0.2 | 0.8 ± 0.3 | 0.9 ± 0.4 |
| Lipids (g/kg) | 0.5 ± 0.2 | 0.5 ± 0.2 | 0.5 ± 0.2 | 0.5 ± 0.2 | 0.5 ± 0.3 | 0.6 ± 0.3 |
| Total strength (kg) | 114.1 ± 17.0 | 132.9 ± 21.5 § | 118.4 ± 22.1 | 130.9 ± 19.0 § | 111.6 ± 14.2 | 104.4 ± 14.7 |
| Body fat | ||||||
| Fat mass (kg) | 27.3 ± 8.6 | 25.9 ± 9.1 *§ | 25.4 ± 7.2 | 24.0 ± 7.3 *§ | 26.4 ± 8.7 | 26.9 ± 8.6 |
| Relative body fat (%) | 41.8 ± 6.8 | 39.0 ± 7.4 * | 40.0 ± 5.5 | 37.7 ± 5.5 *§ | 41.1 ± 7.4 | 41.7 ± 7.1 |
| Trunk fat (kg) | 13.7 ± 4.2 | 13.1 ± 4.4 *§ | 12.5 ± 3.6 | 11.6 ± 3.4 *§ | 14.9 ± 4.8 | 15.0 ± 4.6 |
| Relative trunk fat (%) | 42.6 ± 6.7 | 39.9 ± 7.6 *§ | 39.9 ± 6.5 | 37.1 ± 5.9 *§ | 42.9 ± 6.1 | 43.2 ± 5.4 |
| Blood biomarkers | ||||||
| Glucose (mg/dL) | 112 ± 19 | 91 ± 16 *§ | 114 ± 17 | 88 ± 12 *§ | 100 ± 11 | 102 ± 10 |
| TC (mg/dL) | 189 ± 26 | 190 ± 16 | 193 ± 38 | 183 ± 32 | 203 ± 20 | 214 ± 21 |
| HDL-c (mg/dL) | 53 ± 10 | 54 ± 12 | 54 ± 14 | 56 ± 15 | 55 ± 12 | 53 ± 11 |
| LDL-c (mg/dL) | 115 ± 23 | 112 ± 18 § | 118 ± 40 | 105 ± 32 *§ | 124 ± 24 | 139 ± 21 * |
| VLDL-c (mg/dL) | 24 ± 10 | 21 ± 9 | 22 ± 10 | 22 ± 8 | 22 ± 7 | 23 ± 9 |
| Triglycerides (mg/dL) | 107 ± 28 | 119 ± 38 | 108 ± 40 | 109 ± 53 | 117 ± 46 | 110 ± 37 |
| IL-6 (pg/mL) | 2.8 ± 0.8 | 2.4 ± 0.3 | 2.7 ± 0.9 | 2.3 ± 0.5 | 2.8 ± 0.6 | 3.1 ± 0.9 |
| IL-10 (pg/mL) | 11.5 ± 8.9 | 18.7 ± 11.1 *§ | 10.1 ± 3.8 | 15.0 ± 4.5 *§ | 13.8 ± 6.5 | 5.6 ± 4.0 * |
| TNF-α (pg/mL) | 3.8 ± 1.7 | 2.9 ± 0.5 *§ | 4.0 ± 2.3 | 2.9 ± 0.6 *§ | 3.2 ± 1.7 | 3.3 ± 1.9 |
| CRP (mL/dL) | 3.1 ± 1.6 | 2.3 ± 1.4 *§ | 3.1 ± 1.2 | 2.2 ± 0.6 *§ | 3.0 ± 2.1 | 4.4 ± 2.1 * |
| TRAPP (µmolTrolox) | 887 ± 187 | 883 ± 154 | 875 ± 134 | 844 ± 199 | 902 ± 163 | 898 ± 89 |
| AOPP (µmol/L) | 93.0 ± 30.4 | 77.5 ± 13.9 *§ | 88.1 ± 13.9 | 75.0 ± 13.5 *§ | 75.9 ± 17.8 | 86.3 ± 19.3 |
| FOX (mmol/L) | 0.45 ± 0.23 | 0.27 ± 0.07 *§ | 0.49 ± 0.29 | 0.30 ± 0.11 *§ | 0.48 ± 0.31 | 0.57 ± 0.34 |
| NOx (µmol/L) | 7.3 ± 2.6 | 7.4 ± 2.8 | 7.4 ± 2.1 | 7.0 ± 2.4 | 7.8 ± 4.1 | 8.3 ± 4.1 |
| MJ-SJ (n = 15) | SJ-MJ (n = 14) | CON (n = 15) | ||||
|---|---|---|---|---|---|---|
| Body composition | ||||||
| Body mass | 0.03 | (Trivial) | −0.06 | (Trivial) | 0.02 | (Trivial) |
| Fat mass | −0.17 | (Trivial) | −0.17 | (Trivial) | 0.06 | (Trivial) |
| Relative fat mass | −0.43 | (Small) | −0.35 | (Small) | 0.09 | (Trivial) |
| Trunk fat | −0.14 | (Trivial) | −0.21 | (Small) | 0.02 | (Trivial) |
| Relative trunk fat | −0.42 | (Small) | −0.44 | (Small) | 0.05 | (Trivial) |
| Blood biomarkers | ||||||
| Glucose | −1.34 | (Large) | −1.66 | (Large) | 0.13 | (Trivial) |
| Total cholesterol | 0.04 | (Trivial) | −0.36 | (Small) | 0.39 | (Small) |
| HDL-c | 0.08 | (Trivial) | 0.17 | (Trivial) | −0.17 | (Trivial) |
| LDL-c | −0.10 | (Trivial) | −0.45 | (Small) | 0.52 | (Moderate) |
| VLDL-c | −0.33 | (Small) | 0.00 | (Trivial) | 0.11 | (Trivial) |
| Triglycerides | 0.32 | (Small) | 0.03 | (Trivial) | −0.18 | (Trivial) |
| IL-6 | −0.52 | (Moderate) | −0.52 | (Moderate) | 0.39 | (small) |
| IL-10 | 1.13 | (Large) | 0.77 | (Moderate) | −1.28 | (Large) |
| TNF-α | −0.47 | (Small) | −0.58 | (Moderate) | 0.05 | (Trivial) |
| CRP | −0.49 | (Small) | −0.55 | (Moderate) | 0.86 | (Large) |
| TRAPP | −0.02 | (Trivial) | −0.19 | (Trivial) | −0.02 | (Trivial) |
| AOPP | −0.75 | (Moderate) | −0.63 | (Moderate) | 0.50 | (Moderate) |
| FOX | −0.65 | (Moderate) | −0.69 | (Moderate) | 0.33 | (Small) |
| NOx | 0.03 | (Trivial) | −0.14 | (Trivial) | 0.17 | (Trivial) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomeleri, C.M.; Cunha, P.M.; Dib, M.M.; Schiavoni, D.; Kassiano, W.; Costa, B.; Teixeira, D.C.; Deminice, R.; Rodrigues, R.J.; Venturini, D.; et al. Effect of Resistance Exercise Order on Cardiovascular Disease Risk Factors in Older Women: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2023, 20, 1165. https://doi.org/10.3390/ijerph20021165
Tomeleri CM, Cunha PM, Dib MM, Schiavoni D, Kassiano W, Costa B, Teixeira DC, Deminice R, Rodrigues RJ, Venturini D, et al. Effect of Resistance Exercise Order on Cardiovascular Disease Risk Factors in Older Women: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2023; 20(2):1165. https://doi.org/10.3390/ijerph20021165
Chicago/Turabian StyleTomeleri, Crisieli M., Paolo M. Cunha, Márcia M. Dib, Durcelina Schiavoni, Witalo Kassiano, Bruna Costa, Denilson C. Teixeira, Rafael Deminice, Ricardo José Rodrigues, Danielle Venturini, and et al. 2023. "Effect of Resistance Exercise Order on Cardiovascular Disease Risk Factors in Older Women: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 20, no. 2: 1165. https://doi.org/10.3390/ijerph20021165
APA StyleTomeleri, C. M., Cunha, P. M., Dib, M. M., Schiavoni, D., Kassiano, W., Costa, B., Teixeira, D. C., Deminice, R., Rodrigues, R. J., Venturini, D., Barbosa, D. S., Cavaglieri, C. R., Sardinha, L. B., & Cyrino, E. S. (2023). Effect of Resistance Exercise Order on Cardiovascular Disease Risk Factors in Older Women: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 20(2), 1165. https://doi.org/10.3390/ijerph20021165