
The Association between Cervical Length and Successful Labor Induction: A Retrospective Cohort Study



Abstract
1. Introduction
2. Materials and Methods
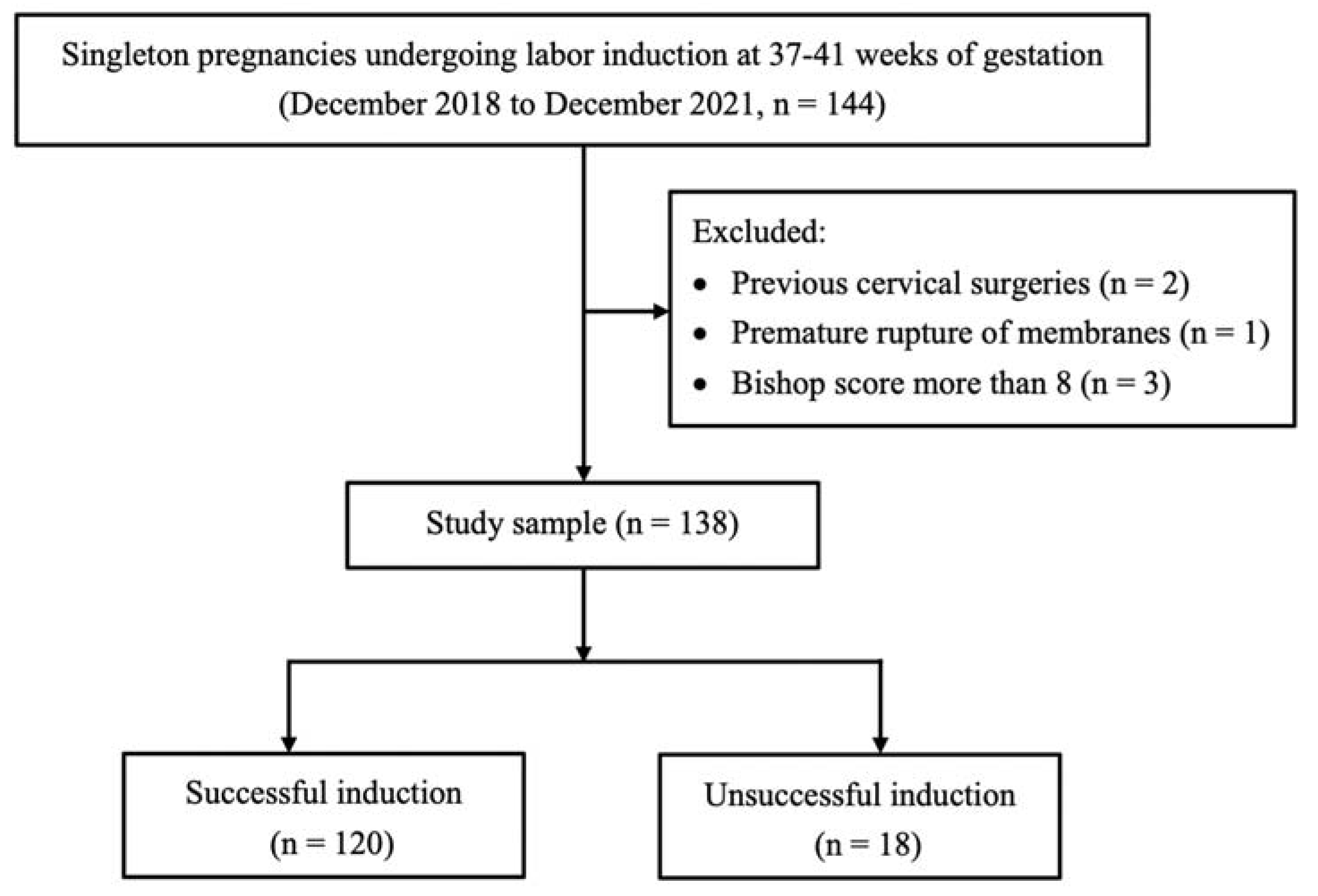
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Induction Protocol
2.4. Outcome Measurement
2.5. Primary Outcome
2.6. Other Characteristics Collected from the Patient
2.7. Statistical Analysis
3. Results
3.1. Demographics
3.2. Factors Associated with Successful Induction
3.3. The Percentage of Successful Labor Induction in Different Cervical Lengths
3.4. Factors Associated with Total Labor Time
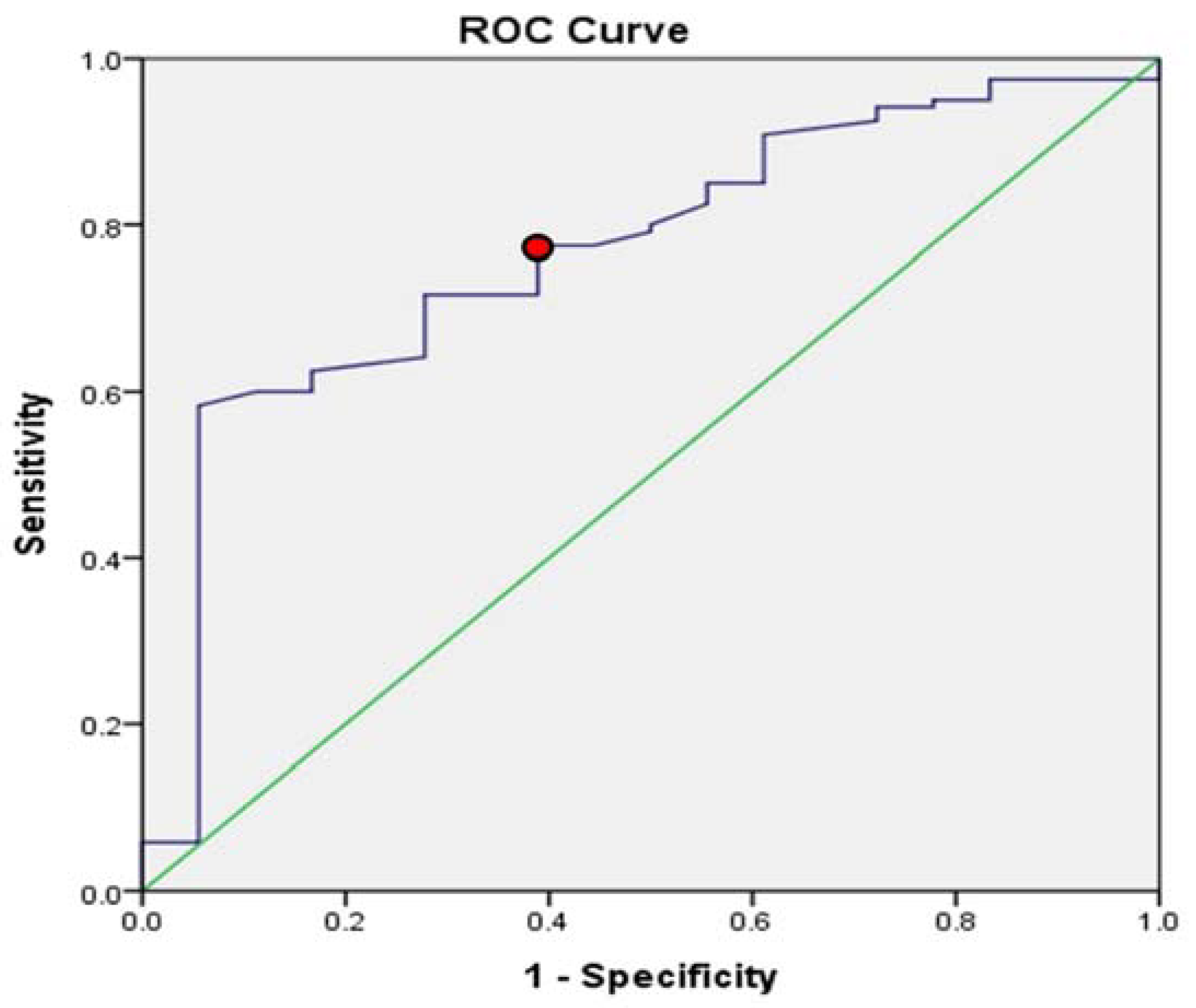
3.5. ROC Curves of Cervical Length and Successful Induction
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Glossary
| Induction of labor | The use of medications or other methods to bring on labor |
| Chi-squared test | Comparison of the distribution of categorial variables in different groups |
| Fisher’s exact test | Analysis of contingency tables |
| ROC (receiver operating characteristic) curve | A graph showing the performance of a classification model at all classification thresholds |
| Independent t-test | An inferential statistical test that determines whether there is a statistically significant difference between the means in two unrelated groups |
| Mann–Whitney U test | A test used to compare the differences between two independent groups that are either ordinal or continuous, but not normally distributed |
| Bishop score | This system evaluates cervical condition including dilation, position of the cervix, effacement, station, and cervical consistence. Scores range from 0 to 3. With a Bishop score equal or more than 8, the chance of successful labor induction is favorable. |
| Term pregnancy | A pregnancy gestation age equal or more than 37 weeks |
| IUGR (intrauterine growth restriction) | Fetal weight is estimated to be below the 10th percentile for its gestational age |
| Oligohydramnios | Amniotic fluid volume less than the minimum expected for gestational age |
| Gestational hypertension/Preeclampsia | These are hypertensive disorders induced by pregnancy. Both disorders resolve postpartum. |
| Polyhydramnios | Pathological increase of amniotic fluid volume in pregnancy |
| Funneling | Ultrasound revealing a protrusion of amniotic membranes into the internal cervical os by greater than 5 mm from the shoulder of the original internal os |
| Nulliparity | Women who have never have given birth to a child or who have never carried a pregnancy |
| Multiparity | Parity ≧ 2 deliveries |
| Cervical length | The linear distance from the internal os to the external os of the cervix measured by ultrasound |
References
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.K.; Driscoll, A.K.; Drake, P. Births: Final Data for 2016. Natl. Vital Stat. Rep. 2018, 67, 1–55. [Google Scholar] [PubMed]
- Zhu, J.; Xue, L.; Shen, H.; Zhang, L.; Lu, D.; Wang, Y.; Zhang, Y.; Zhang, J. Labor Induction in China: A Nationwide Survey. BMC Pregnancy Childbirth 2022, 22, 463. [Google Scholar] [CrossRef] [PubMed]
- Le Ray, C.; Carayol, M.; Bréart, G.; Goffinet, F. PREMODA Study Group Elective Induction of Labor: Failure to Follow Guidelines and Risk of Cesarean Delivery. Acta Obstet. Gynecol. Scand. 2007, 86, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Society of Maternal-Fetal (SMFM) Publications Committee. SMFM Statement on Elective Induction of Labor in Low-Risk Nulliparous Women at Term: The ARRIVE Trial. Am. J. Obstet. Gynecol. 2019, 221, B2–B4. [Google Scholar] [CrossRef] [PubMed]
- Grobman, W. LB01: A Randomized Trial of Elective Induction of Labor at 39 Weeks Compared with Expectant Management of Low-Risk Nulliparous Women. Am. J. Obstet. Gynecol. 2018, 218, S601. [Google Scholar] [CrossRef]
- Grobman, W.A.; Caughey, A.B. Elective Induction of Labor at 39 Weeks Compared with Expectant Management: A Meta-Analysis of Cohort Studies. Am. J. Obstet. Gynecol. 2019, 221, 304–310. [Google Scholar] [CrossRef]
- Kim, H.I.; Choo, S.P.; Han, S.W.; Kim, E.H. Benefits and Risks of Induction of Labor at 39 or More Weeks in Uncomplicated Nulliparous Women: A Retrospective, Observational Study. Obstet. Gynecol. Sci. 2019, 62, 19–26. [Google Scholar] [CrossRef]
- De Los Santos-Garate, A.M.; Villa-Guillen, M.; Villanueva-García, D.; Vallejos-Ruíz, M.L.; Murguía-Peniche, M.T. NEOSANO’s Network Perinatal Morbidity and Mortality in Late-Term and Post-Term Pregnancy. NEOSANO Perinatal Network’s Experience in Mexico. J. Perinatol. 2011, 31, 789–793. [Google Scholar] [CrossRef]
- Penfield, C.A.; Wing, D.A. Labor Induction Techniques: Which Is the Best? Obstet. Gynecol. Clin. N. Am. 2017, 44, 567–582. [Google Scholar] [CrossRef]
- Ting, N.-S.; Ding, D.-C.; Wei, Y.-C. Comparison of the Dinoprostone Vaginal Insert and Dinoprostone Tablet for the Induction of Labor in Primipara: A Retrospective Cohort Study. J. Clin. Med. Res. 2022, 11, 3519. [Google Scholar] [CrossRef]
- Ikeotuonye, A.C.; Anikwe, C.C.; Obuna, J.A.; Okorochukwu, B.C.; Ejikeme, B.N.; Ifemelumma, C.C.; Ekwunife, I.C.; Okoroafor, F.C. Relationship between Bishop Score and Success of Induction of Labour in Federal Teaching Hospital, Abakaliki, Ebonyi State. Open J. Obstet. Gynecol. 2018, 8, 980–992. [Google Scholar] [CrossRef]
- Mohamed El Bishry, G.; Serag Allam, I.; Rasheedy, R.; Mahmoud, A. Accuracy of the Manipal Cervical Scoring System for Predicting Successful Induction of Labour. J. Obstet. Gynaecol. 2019, 39, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Simon, R.; Oros, D.; Gracia-Cólera, D.; Moreno, E.; Paules, C.; Cañizares, S.; Gascón, E.; Fabre, E. Cervix Assessment for the Management of Labor Induction: Reliability of Cervical Length and Bishop Score Determined by Residents. J. Obstet. Gynaecol. Res. 2015, 41, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.Y.; Wie, J.H.; Choi, S.K.; Park, S.; Kim, S.M.; Park, I.Y. The Degree of Cervical Length Shortening as a Predictor of Successful or Failed Labor Induction. Taiwan. J. Obstet. Gynecol. 2021, 60, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Wormer, K.C.; Bauer, A.; Williford, A.E. Bishop Score. In StatPearls; StatPearls Publishing: Tampa, FL, USA, 2022. [Google Scholar]
- Kagan, K.O.; Sonek, J. How to Measure Cervical Length. Ultrasound Obstet. Gynecol. 2015, 45, 358–362. [Google Scholar] [CrossRef]
- Ellis, J.A.; Brown, C.M.; Barger, B.; Carlson, N.S. Influence of Maternal Obesity on Labor Induction: A Systematic Review and Meta-Analysis. J. Midwifery Womens Health 2019, 64, 55–67. [Google Scholar] [CrossRef]
- Lundborg, L.; Liu, X.; Åberg, K.; Sandström, A.; Tilden, E.L.; Stephansson, O.; Ahlberg, M. Association of Body Mass Index and Maternal Age with First Stage Duration of Labour. Sci. Rep. 2021, 11, 13843. [Google Scholar] [CrossRef]
- Palatnik, A.; Kominiarek, M.A. Outcomes of Elective Induction of Labor versus Expectant Management among Obese Women at ≥39 Weeks. Am. J. Perinatol. 2020, 37, 695–707. [Google Scholar] [CrossRef]
- Eberle, A.; Czuzoj-Shulman, N.; Azoulay, L.; Abenhaim, H.A. Induction of Labor at 39 Weeks and Risk of Cesarean Delivery among Obese Women: A Retrospective Propensity Score Matched Study. J. Perinat. Med. 2021, 49, 791–796. [Google Scholar] [CrossRef]
- Al-Adwy, A.M.; Sobh, S.M.; Belal, D.S.; Omran, E.F.; Hassan, A.; Saad, A.H.; Afifi, M.M.; Nada, A.M. Diagnostic Accuracy of Posterior Cervical Angle and Cervical Length in the Prediction of Successful Induction of Labor. Int. J. Gynaecol. Obstet. 2018, 141, 102–107. [Google Scholar] [CrossRef]
- Pierce, S.; Bakker, R.; Myers, D.A.; Edwards, R.K. Clinical Insights for Cervical Ripening and Labor Induction Using Prostaglandins. AJP Rep. 2018, 8, e307–e314. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, Z.H.A.; Chew, K.T.; Velayudham, V.R.V.; Yahaya, Z.; Jamil, A.A.M.; Abu, M.A.; Ghani, N.A.A.; Ismail, N.A.M. Pre-Induction Cervical Assessment Using Transvaginal Ultrasound versus Bishops Cervical Scoring as Predictors of Successful Induction of Labour in Term Pregnancies: A Hospital-Based Comparative Clinical Trial. PLoS ONE 2022, 17, e0262387. [Google Scholar] [CrossRef] [PubMed]
- Khandelwal, R.; Patel, P.; Pitre, D.; Sheth, T.; Maitra, N. Comparison of Cervical Length Measured by Transvaginal Ultrasonography and Bishop Score in Predicting Response to Labor Induction. J. Obstet. Gynaecol. India 2018, 68, 51–57. [Google Scholar] [CrossRef]
- Wang, B.; Zhang, Y.; Chen, S.; Xiang, X.; Wen, J.; Yi, M.; He, B.; Hu, B. Diagnostic Accuracy of Cervical Elastography in Predicting Preterm Delivery: A Systematic Review and Meta-Analysis. Medicine 2019, 98, e16449. [Google Scholar] [CrossRef] [PubMed]
- Grab, D.; Doroftei, B.; Grigore, M.; Nicolaiciuc, O.S.; Anton, S.C.; Simionescu, G.; Maftei, R.; Bolota, M.; Ilea, C.; Costachescu, G.; et al. Fetal Fibronectin and Cervical Length as Predictors of Spontaneous Onset of Labour and Delivery in Term Pregnancies. Healthcare 2022, 10, 1349. [Google Scholar] [CrossRef]
- Witter, F.R.; Rocco, L.E.; Johnson, T.R. A Randomized Trial of Prostaglandin E2 in a Controlled-Release Vaginal Pessary for Cervical Ripening at Term. Am. J. Obstet. Gynecol. 1992, 166, 830–834. [Google Scholar] [CrossRef]
- Daykan, Y.; Biron-Shental, T.; Navve, D.; Miller, N.; Bustan, M.; Sukenik-Halevy, R. Prediction of the Efficacy of Dinoprostone Slow Release Vaginal Insert (Propess) for Cervical Ripening: A Prospective Cohort Study. J. Obstet. Gynaecol. Res. 2018, 44, 1739–1746. [Google Scholar] [CrossRef]
- Abdelaziz, A.; Mahmoud, A.A.; Ellaithy, M.I.; Abees, S.H. Pre-Induction Cervical Ripening Using Two Different Dinoprostone Vaginal Preparations: A Randomized Clinical Trial of Tablets and Slow Release Retrievable Insert. Taiwan. J. Obstet. Gynecol. 2018, 57, 560–566. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Successful Induction | Total | p-Value | ||
|---|---|---|---|---|
| No | Yes | |||
| N (%) | 18 (13.1%) | 120 (86.9%) | 138 | |
| Age (years) | 31.56 ± 5.74 | 29.98 ± 5.48 | 30.19 ± 5.52 | 0.262 |
| Weight (kg) | 77.52 ± 15.05 | 74.20 ± 9.77 | 74.63 ± 10.60 | 0.216 |
| BMI (kg/m2) | 30.92 ± 5.15 | 28.74 ± 3.93 | 29.02 ± 4.16 | 0.037 * |
| GA (weeks) | 38.75 ± 0.73 | 39.05 ± 0.87 | 39.01 ± 0.85 | 0.174 |
| GA group (weeks) | 0.790 | |||
| 37 + 0~37 + 6 | 2 (11.1%) | 8 (6.7%) | 10 (7.2%) | |
| 38 + 0~38 + 6 | 9 (50%) | 49 (40.8%) | 58 (42.0%) | |
| 39 + 0~39 + 6 | 5 (27.8%) | 44 (36.7%) | 49 (35.5%) | |
| 40 + 0~40 + 6 | 2 (11.1%) | 17 (14.2%) | 19 (13.8%) | |
| 41 + 0~41 + 6 | 0 (0%) | 2 (1.7%) | 2 (1.4%) | |
| Hb (g/dL) | 11.27 ± 1.39 | 10.93 ± 1.54 | 10.97 ± 1.52 | 0.370 |
| Parity [n (%)] | - | - | - | 0.004 * |
| Nulliparity | 16 (88.9%) | 63 (52.5%) | 79 (57.2%) | |
| Multiparity | 2 (11.1%) | 57 (47.5%) | 59 (42.8%) | |
| Maternal disease [n (%)] | - | - | - | |
| Normal | 14 (77.8%) | 90 (75.0%) | 104 (75.4%) | 1.000 |
| IDA | 1 (5.6%) | 20 (16.7) | 21 (15.2%) | 0.308 |
| Autoimmune disease | 0 (0.0%) | 3 (2.5%) | 3 (2.2%) | 1.000 |
| Asthma | 1 (5.6%) | 2 (1.7%) | 3 (2.2%) | 0.345 |
| Vitamin D deficiency | 0 (0.0%) | 2 (1.7%) | 2 (1.4%) | 1.000 |
| Thyroid disease | 0 (0.0%) | 2 (1.7%) | 2 (1.4%) | 1.000 |
| Cancer | 0 (0.0%) | 2 (1.7%) | 2 (1.4%) | 1.000 |
| Thalassemia | 2 (11.1%) | 0 (0.0%) | 2 (1.4%) | 0.016 * |
| HBV | 0 (0.0%) | 1 (0.8%) | 1 (0.7%) | 1.000 |
| Sicca syndrome | 0 (0.0%) | 1 (0.8%) | 1 (0.7%) | 1.000 |
| Prenatal problem [n (%)] | - | - | - | 0.055 |
| Normal | 12 (66.7%) | 98 (81.7%) | 110 (79.7%) | |
| GDM | 2 (11.1%) | 11 (9.2%) | 13 (9.4%) | |
| IUGR | 1 (5.6%) | 5 (4.2%) | 6 (4.3%) | |
| Gestational HTN | 0 (0.0%) | 2 (1.7%) | 2 (1.4%) | |
| Polyhydramnios | 1 (5.6%) | 1 (0.8%) | 2 (1.4%) | |
| Preeclampsia | 2 (11.1%) | 0 (0.0%) | 2 (1.4%) | |
| SUA | 0 (0.0%) | 2 (1.7%) | 2 (1.4%) | |
| Fetal arrhythmia | 0 (0.0%) | 1 (0.8%) | 1 (0.7%) | |
| GBS (%) | 4 (22.2%) | 22 (18.3%) | 26 (18.8%) | 0.747 |
| Indication of labor induction [n (%)] | - | - | - | 0.016 * |
| No labor sign | 13 (72.2%) | 110 (91.7%) | 123 (89.1%) | |
| IUGR | 1 (5.6%) | 5 (4.2%) | 6 (4.3%) | |
| Oligohydramnios | 2 (11.1%) | 4 (3.3%) | 6 (4.3%) | |
| Gestational HTN/Polyhydramnios/Preeclampsia | 2 (11.1%) | 1 (0.8%) | 3 (2.2%) | |
| Induction method [n (%)] | - | - | - | 0.155 |
| Prostin | 5 (27.8%) | 54 (45.0%) | 59 (42.8%) | |
| Propess | 4 (22.2%) | 34 (28.3%) | 38 (27.5%) | |
| Propess + Piton | 2 (11.1%) | 13 (10.8%) | 15 (10.9%) | |
| Prostin + Piton | 3 (16.7%) | 9 (7.5%) | 12 (8.7%) | |
| Propess + Prostin | 2 (11.1%) | 3 (2.5%) | 5 (3.6%) | |
| Propess + Prostin + Piton | 2 (11.1%) | 7 (5.8%) | 9 (6.5%) | |
| Epidural anesthesia [n (%)] | 11 (61.1%) | 86 (71.7%) | 97 (70.3%) | 0.361 |
| Cervical length (cm) | 3.52 ± 0.65 | 2.84 ± 0.76 | 2.93 ± 0.78 | <0.001 * |
| Cervical length group | <0.001 * | |||
| <3.0 cm | 1 (5.6%) | 70 (58.3%) | 71 (51.4%) | |
| 3.0–3.5 cm | 8 (44.4%) | 26 (21.7%) | 34 (24.6%) | |
| >3.5–4 cm | 5 (27.8%) | 18 (15.0%) | 23 (16.7%) | |
| >4 cm | 4 (22.2%) | 6 (5.0%) | 10 (7.2%) | |
| Funneling [n (%)] | 2 (11.1%) | 29 (24.2%) | 31 (22.5%) | 0.363 |
| Bishop score | 2.00 ± 2.22 | 2.90 ± 2.21 | 2.78 ± 2.23 | 0.110 |
| Position [n (%)] | - | - | - | 0.698 |
| Posterior | 13 (72.2%) | 93 (77.5%) | 106 (76.8%) | |
| Mid | 5 (27.8%) | 24 (20.0%) | 29 (21.0%) | |
| Anterior | 0 (0.0%) | 3 (2.5%) | 3 (2.2%) | |
| Dilation [n (%)] | - | - | - | 0.499 |
| Closed | 14 (77.8%) | 79 (65.8%) | 93 (67.4%) | |
| 1–2 cm | 4 (22.2%) | 40 (33.3%) | 44 (31.9%) | |
| 3–4 cm | 0 (0.0%) | 1 (0.8%) | 1 (0.7%) | |
| Effacement [n (%)] | - | - | - | 1.000 |
| 0–30% | 15 (83.3%) | 93 (77.5%) | 108 (78.3%) | |
| 40–50% | 3 (16.7%) | 23 (19.2%) | 26 (18.8%) | |
| 60–70% | 0 (0.0%) | 4 (3.3%) | 4 (2.9%) | |
| Consistency [n (%)] | - | - | - | 0.127 |
| Firm | 10 (55.6%) | 36 (30.0%) | 46 (33.3%) | |
| Medium | 0 (0.0%) | 1 (0.8%) | 1 (0.7%) | |
| Soft | 8 (44.4%) | 83 (69.2%) | 91 (65.9%) | |
| Station [n (%)] | - | - | - | 0.683 |
| −3 | 9 (50.0%) | 47 (39.2%) | 56(40.6%) | |
| −2 | 8 (44.4%) | 65 (54.2%) | 73(52.9%) | |
| −1, 0 | 1 (5.6%) | 8 (6.7%) | 9(6.5%) | |
| Induction time (min) | 5194.50 ± 446.18 | 1132.23 ± 800.95 | 1198.82 ± 949.13 | <0.001 * |
| Stages of labor (min) | - | - | - | |
| 1st stage | 1150.50 ± 1448.86 | 325.17 ± 404.26 | 338.70 ± 434.91 | 0.007 * |
| 2nd stage | 54.50 ± 21.92 | 78.35 ± 112.95 | 77.96 ± 112.07 | 0.767 |
| 3rd stage | 9.00 ± 2.83 | 4.71 ± 5.43 | 4.78 ± 5.42 | 0.268 |
| Delivery mode [n (%)] | - | - | - | <0.001 * |
| NSD | 1 (5.6%) | 85 (70.8%) | 86 (62.3%) | |
| VED | 1 (5.6%) | 35 (29.2%) | 36 (26.1%) | |
| C/S | 16 (88.9%) | 0 (0.0%) | 16 (11.6%) | |
| Birth weight (g) | 3115.61 ± 348.53 | 3130.88 ± 327.08 | 3128.88 ± 328.67 | 0.855 |
| Sex of fetus [n (%)] | - | - | - | 0.643 |
| Female | 9 (50.0%) | 67 (55.8%) | 76 (55.1%) | |
| Male | 9 (50.0%) | 53 (44.2%) | 62 (44.9%) | |
| Crude | Adjusted | |||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p-Value | Odds Ratio (95% CI) | p-Value | |
| Age (years) | 0.95 (0.86, 1.04) | 0.262 | 0.94 (0.84, 1.06) | 0.320 |
| BMI (kg/m2) | 0.89 (0.79, 0.99) | 0.042 * | 0.87 (0.75, 0.99) | 0.044 * |
| GA (weeks) | 1.53 (0.83, 2.83) | 0.174 | 2.13 (0.95, 4.78) | 0.066 |
| Bishop score | 1.22 (0.95, 1.56) | 0.114 | 0.92 (0.69, 1.23) | 0.878 |
| Cervical length | - | - | - | - |
| >3.415 cm | Reference (1.0) | Reference (1.0) | ||
| ≤3.415 cm | 5.41 (1.91, 15.31) | 0.001 * | 6.22 (1.75, 22.15) | 0.005 * |
| Parity | - | - | - | - |
| Nulliparity | References | References | ||
| Multiparity | 7.24 (1.59, 32.86) | 0.010 * | 17.69 (2.94, 106.51) | 0.002 * |
| Fetal birth weight (kg) | 1.15 (0.26, 5.15) | 0.854 | 0.63 (0.10, 4.03) | 0.629 |
| N | Successful Induction | p-Value | ||
|---|---|---|---|---|
| No | Yes | |||
| Cervical length group | <0.001 * | |||
| <3.0 cm | 71 | 1 (1.4%) | 70 (98.6%) | |
| 3.0–3.5 cm | 34 | 8 (23.5%) | 26 (76.5%) | |
| >3.5–4.0 cm | 23 | 5 (21.7%) | 18 (78.3%) | |
| >4 cm | 10 | 4 (40.0%) | 6 (60.0%) | |
| Total | 138 | 18 (13.0%) | 120 (87.0%) | |
| Crude | Adjusted | |||||
|---|---|---|---|---|---|---|
| Regression Coefficient | 95% CI | p-Value | Regression Coefficient | 95% CI | p-Value | |
| Age (years) | 10.92 | (−20.52, 42.36) | 0.493 | 8.68 | (−18.98, 36.35) | 0.535 |
| BMI (kg/m2) | 6.50 | (−36.81, 49.80) | 0.767 | 21.61 | (−15.31, 58.53) | 0.249 |
| GA (weeks) | 41.18 | (−158.52, 240.89) | 0.684 | −26.55 | (−210.92, 157.83) | 0.776 |
| Bishop score | −114.41 | (−189.13, −39.69) | 0.003 * | −50.10 | (−121.74, 21.55) | 0.169 |
| Cervical length (cm) | 300.82 | (84.26, 517.38) | 0.007 * | 301.87 | (92.82, 510.92) | 0.005 * |
| Parity | - | - | - | - | - | - |
| Nulliparity | Reference | Reference | NA | Reference | Reference | NA |
| Multiparity | −873.95 | (−1177.76, −570.13) | <0.001 * | −947.74 | (−1256.94, −638.53) | <0.001 * |
| Fetal birth weight (kg) | 47.26 | (-479.98, 574.50) | 0.859 | 231.55 | (−220.45, 683.54) | 0.312 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, P.-C.; Tsui, W.L.; Ding, D.-C. The Association between Cervical Length and Successful Labor Induction: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2023, 20, 1138. https://doi.org/10.3390/ijerph20021138
Li P-C, Tsui WL, Ding D-C. The Association between Cervical Length and Successful Labor Induction: A Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2023; 20(2):1138. https://doi.org/10.3390/ijerph20021138
Chicago/Turabian StyleLi, Pei-Chen, Wing Lam Tsui, and Dah-Ching Ding. 2023. "The Association between Cervical Length and Successful Labor Induction: A Retrospective Cohort Study" International Journal of Environmental Research and Public Health 20, no. 2: 1138. https://doi.org/10.3390/ijerph20021138
APA StyleLi, P.-C., Tsui, W. L., & Ding, D.-C. (2023). The Association between Cervical Length and Successful Labor Induction: A Retrospective Cohort Study. International Journal of Environmental Research and Public Health, 20(2), 1138. https://doi.org/10.3390/ijerph20021138