
The Relationships between Self-Reported Motor Functioning and Autistic Traits: The Italian Version of the Adult Developmental Coordination Disorders/Dyspraxia Checklist (ADC)

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Materials
2.3. Statistical Analysis
2.3.1. Aim 1: Psychometric Properties of the Italian ADC
2.3.2. Aim 2: Relationships between ADC and Autistic Traits
3. Results
3.1. Aim 1: Psychometric Properties of the Italian ADC
3.1.1. Confirmatory Factor Analysis
3.1.2. Reliability
3.1.3. Concurrent Validity
3.1.4. Sex Differences
3.2. Aim 2: Relationships between ADC and Autistic Traits
3.2.1. Correlation Analysis
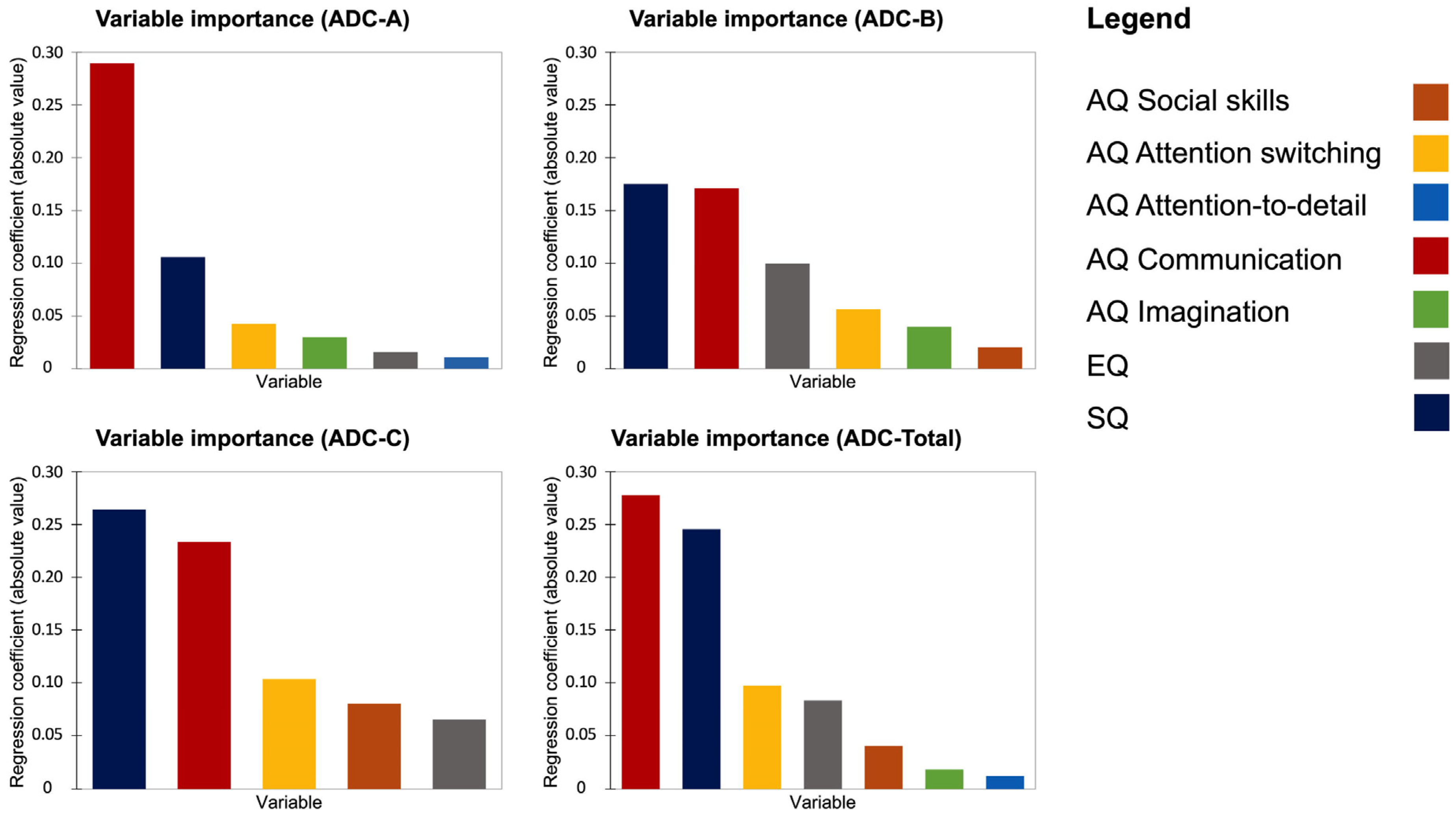
3.2.2. LASSO Regression Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Items (Both in Italian and English) of the Italian Version of the ADC
| Item | |
| Sottoscala A: Da bambino: [Subscale A: As a child, did you:] | |
| Avevi difficoltà con attività quotidiane come allacciare i lacci delle scarpe, chiudere bottoni e cerniere? | A1 |
| [Have difficulties with self-care tasks, such as tying shoelaces, fastening buttons and zips?] | |
| Avevi difficoltà a mangiare senza sporcarti? | A2 |
| [Have difficulty eating without getting dirty?] | |
| Avevi difficoltà ad imparare a portare la biciletta rispetto ai tuoi coetanei? | A3 |
| [Have difficulty learning to ride a bike compared to your peers?] | |
| Avevi difficoltà nei giochi di squadra, come il calcio, la pallavolo, oppure nel ricevere e lanciare la palla con precisione? | A4 |
| [Have difficulties with playing team games, such as football, volleyball, catching or throwing balls accurately?] | |
| Avevi difficoltà a scrivere in modo ordinato (in modo che gli altri potessero leggerlo)? | A5 |
| [Have difficulty writing neatly (so others could read it)?] | |
| Avevi difficoltà a scrivere con la stessa velocità dei tuoi coetanei? | A6 |
| [Have difficulty writing as fast as your peers?] | |
| Urtavi oggetti o persone, inciampavi sulle cose più degli altri? | A7 |
| [Bump into objects or people, trip over things more than others?] | |
| Avevi difficoltà a suonare uno strumento musicale (es. violino, flauto)? | A8 |
| [Have difficulty playing a musical instrument (e.g., violin, recorder)?] | |
| Avevi difficoltà nell’organizzare/trovare cose nella tua stanza? | A9 |
| [Have difficulties with organising/finding your things in your room?] | |
| Gli altri ti facevano notare la tua mancanza di coordinazione o ti definivano maldestro? | A10 |
| [Have others comment about your lack of co-ordination or call yourself clumsy?] | |
| Sottoscala B: Attualmente: Hai difficoltà con le seguenti azioni? [Subscale B: Currently: Do you have difficulties currently with the following 10 items:] | |
| Cura personale come radersi o truccarsi? | B1 |
| [Self-care tasks, such as shaving or make-up?] | |
| Mangiare con coltello e forchetta/cucchiaio? | B2 |
| [Eating with knife and fork/spoon?] | |
| Hobbies che richiedono una buona coordinazione? | B3 |
| [Hobbies that require good co-ordination?] | |
| Scrivere in maniera ordinata quando devi farlo velocemente? | B4 |
| [Writing neatly when having to write fast?] | |
| Scrivere con la stessa velocità dei tuoi coetanei? | B5 |
| [Writing as fast as your peers?] | |
| Leggere la tua scrittura? | B6 |
| [Reading your own writing?] | |
| Copiare qualcosa senza fare errori? | B7 |
| [Copying things down without mistakes?] | |
| Organizzare/trovare qualcosa nella tua stanza? | B8 |
| [Organising/finding your things in your room?] | |
| Trovare la strada nei pressi di un nuovo edificio o luogo? | B9 |
| [Finding your way around new buildings or places?] | |
| Altre persone ti definiscono disorganizzato? | B10 |
| [Have others called you disorganised?] | |
| Sottoscala C: Attualmente: [Subscale C: Please mark the suitable option and describe on the attached paper. Currently.] | |
| Hai difficoltà a stare seduto fermo e sembri irrequieto? | C1 |
| [Do you have difficulties with sitting still or appearing fidgety?] | |
| Perdi o dimentichi i tuoi effetti personali? | C2 |
| [Do you lose or leave behind possessions?] | |
| Puoi dire che urti le cose, rovesci o rompi oggetti? | C3 |
| [Would you say that you bump into things, spill or break things?] | |
| Sei più lento degli altri nello svegliarti al mattino e andare al lavoro o all’Università? | C4 |
| [Are you slower than others getting up in the morning and getting to work or college?] | |
| Hai impiegato più tempo nell’imparare a guidare rispetto agli altri? (se non guidi indica di fianco perché hai scelto di non guidare) | C5 |
| [Did it take you longer than others to learn to drive? (If you do not drive, please indicate so on the attached paper and describe why you chose not to drive.)] | |
| Le persone trovano difficile leggere ciò che scrivi? | C6 |
| [Do others find it difficult to read your writing?] | |
| Eviti gli hobbies che richiedono una buona coordinazione? | C7 |
| [Do you avoid hobbies that require good co-ordination?] | |
| Scegli di trascorrere il tuo tempo libero da solo piuttosto che con gli altri? | C8 |
| [Do you choose to spend leisure time more on your own than with others?] | |
| Eviti giochi o sport di squadra? | C9 |
| [Do you avoid team games/sports?] | |
| Se pratichi uno sport è più probabile che tu lo faccia da solo (es. andare in palestra) oppure con gli altri? | C10 |
| [If you do a sport, is it more likely to be on your own, e.g., going to a gym, than with others?] | |
| Durante la tua adolescenza hai evitato o attualmente eviti di andare in qualche locale a ballare? | C11 |
| [Did you tend in your teens/twenties or currently to avoid going to clubs/dancing?] | |
| Se guidi, hai difficoltà a parcheggiare l’automobile? | C12 |
| [If you are a driver, do you have difficulty parking a car?] | |
| Hai difficoltà a preparare un pasto dall’inizio? | C13 |
| [Do you have difficulty preparing a meal from scratch?] | |
| Hai difficoltà a preparare la valigia per partire? | C14 |
| [Do you have difficulty packing a suitcase to go away?] | |
| Hai difficoltà a piegare i vestiti per metterli via in modo ordinato? | C15 |
| [Do you have difficulty folding clothes to put them away neatly?] | |
| Hai difficolta a gestire i soldi? | C16 |
| [Do you have difficulty managing money?] | |
| Hai difficoltà a fare due cose contemporaneamente (es. guidare e ascoltare o ricevere un messaggio telefonico)? | C17 |
| [Do you have difficulties with performing two things at the same time (e.g., driving and listening)?] | |
| Hai difficoltà a stimare le distanze (es. per parcheggiare, per muoversi tra gli oggetti)? | C18 |
| [Do you have difficulties with distance estimation (e.g., with regard to parking, passing through objects)?] | |
| Hai difficoltà a pianificare il futuro? | C19 |
| [Do you have difficulty planning ahead?] | |
| Ti accorgi che ti stai distraendo in certe situazioni? | C20 |
| [Do you feel you are losing attention in certain situations?] |
References
- Zwicker, J.; Missiuna, C.; Harris, S.; Boyd, L. Developmetnal corodination disorder: A review and update. Eur. J. Paediatr. Neurol. 2012, 16, 573–581. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association [APA] (Ed.) Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Engel-Yeger, B. The role of poor motor coordination in predicting adults’ health related quality of life. Res. Dev. Disabil. 2020, 103, 103686. [Google Scholar] [CrossRef] [PubMed]
- Kirby, A.; Edwards, L.; Sugden, D. Emerging adulthood in developmental co-ordination disorder: Parent and young adult perspectives. Res. Dev. Disabil. 2011, 32, 1351–1360. [Google Scholar] [CrossRef] [PubMed]
- Tal-Saban, M.; Kirby, A. Empathy, social relationship and co-occurrence in young adults with DCD. Hum. Mov. Sci. 2019, 63, 62–72. [Google Scholar] [CrossRef]
- Tal-Saban, M.; Zarka, S.; Grotto, I.; Ornoy, A.; Parush, S. The functional profile of young adults with suspected Developmental Coordination Disorder (DCD). Res. Dev. Disabil. 2012, 33, 2193–2202. [Google Scholar] [CrossRef]
- Kirby, A.; Sugden, D.; Beveridge, S.; Edwards, L.; Edwards, R. Dyslexia and developmental co-ordination disorder in further and higher education—similarities and differences. Does the ‘label’ influence the support given? Dyslexia 2008, 14, 197–213. [Google Scholar] [CrossRef]
- Wilson, P.H.; Smits-Engelsman, B.; Caeyenberghs, K.; Steenbergen, B.; Sugden, D.; Clark, J.; Mumford, N.; Blank, R. Cognitive and neuroimaging findings in developmental coordination disorder: New insights from a systematic review of recent research. Dev. Med. Child. Neurol. 2017, 59, 1117–1129. [Google Scholar] [CrossRef]
- Kirby, A.; Williams, N.; Thomas, M.; Hill, E.L. Self-reported mood, general health, wellbeing and employment status in adults with suspected DCD. Res. Dev. Disabil. 2013, 34, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- Tal-Saban, M.; Ornoy, A.; Parush, S. Young adults with developmental coordination disorder: A longitudinal study. Am. J. Occup. Ther. 2014, 68, 307–316. [Google Scholar] [CrossRef]
- Lino, F.; Chieffo, D.P.R. Developmental Coordination Disorder and most prevalent comorbidities: A narrative review. Children 2022, 9, 1095. [Google Scholar] [CrossRef]
- Cassidy, S.; Hannant, P.; Tavassoli, T.; Allison, C.; Smith, P.; Baron-Cohen, S. Dyspraxia and autistic traits in adults with and without autism spectrum conditions. Mol. Autism. 2016, 7, 48. [Google Scholar] [CrossRef] [PubMed]
- Kirby, A.; Edwards, L.; Sugden, D.; Rosenblum, S. The development and standardization of the Adult Developmental Co-ordination Disorders/Dyspraxia Checklist (ADC). Res. Dev. Disabil. 2010, 31, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Meachon, E.J.; Beitz, C.; Zemp, M.; Wilmut, K.; Alpers, G.W. The adult developmental coordination disorders/dyspraxia checklist—German: Adapted factor structure for the differentiation of DCD and ADHD. Res. Dev. Disabil. 2022, 126, 104254. [Google Scholar] [CrossRef] [PubMed]
- Caravale, B.; Baldi, S.; Capone, L.; Presaghi, F.; Balottin, U.; Zoppello, M. Psychometric properties of the Italian version of the Developmental Coordination Disorder Questionnaire (DCDQ-Italian). Res. Dev. Disabil. 2015, 36C, 543–550. [Google Scholar] [CrossRef]
- Giofrè, D.; Barbato, L.; Cornoldi, C.; Schoemaker, M.M. Il MOQ-T: Un questionario per gli insegnanti di facile utilizzo per la rilevazione dei sintomi del disturbo della coordinazione motoria. Psicol. Clin. Dello Svilupp. 2015, XIX, 495–505. [Google Scholar]
- Cleaton, M.A.M.; Tal-Saban, M.; Hill, E.L.; Kirby, A. Gender and age differences in the presentation of at-risk or probable Developmental Coordination Disorder in adults. Res. Dev. Disabil. 2021, 115, 104010. [Google Scholar] [CrossRef]
- Engel-Yeger, B.; Nagauker-Yanuv, L.; Rosenblum, S. Handwriting performance: The relationships between process and product measures, children’s self- reports, and perceived self-efficacy. Am. J. Occup. Ther. 2009, 63, 182–192. [Google Scholar] [CrossRef]
- Dunford, C.; Street, E.; O’Connell, H.; Kelly, J.; Sibert, J.R. Are referrals to occupational therapy for developmental coordination disorder appropriate? Arch. Dis. Child. 2004, 89, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.T.; Missiuna, C.A.; Macnab, J.J.; Malloy-Miller, T.; Polatajko, H.J. Clinical description of children with developmental coordination disorder. Can. J. Occup. Ther. 2001, 68, 5–15. [Google Scholar] [CrossRef]
- Cornoldi, C.; Candela, M. Prove di Lettura e Scrittura MT.T-16-19. Batteria per la Verifica degli Apprendimenti e la Diagnosi di Dislessia e Disortografia—Classi terza, Quarta, Quinta della Scuola Secondaria di Secondo Grado; Erickson: Trento, Italy, 2015. [Google Scholar]
- Baron-Cohen, S.; Wheelwright, S.; Skinner, R.; Martin, J.; Clubley, E. The autism-spectrum quotient (AQ): Evidence from Asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. J. Autism Develop. Disord. 2001, 31, 5–17. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Wheelwright, S. The empathy quotient (EQ). An investigation of adults with Asperger syndrome or high functioning autism, and normal sex differences. J. Autism Develop. Disord. 2004, 34, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, S.; Richler, J.; Bisarya, D.; Gurunathan, N.; Wheelwright, S. The systemising quotient (SQ): An investigation of adults with Asperger syndrome or high functioning autism and normal sex differences. Philos Trans. R Soc. Lond B Biol. Sci. 2003, 358, 361–374. [Google Scholar] [CrossRef]
- Baron-Cohen, S. The extreme male brain theory of autism. Trends Cog. Sci. 2002, 6, 248–254. [Google Scholar] [CrossRef]
- Baron-Cohen, S. The Pattern Seekers: How Autism Drives Human Invention; BasicBooks: New York, NY, USA, 2021. [Google Scholar]
- Tabachnick, B.; Fidell, L. Using Multivariate Statistics; Pearson Education Inc.: Boston, MA, USA, 2013. [Google Scholar]
- Wang, J.; Wang, X. Structural Equation Modeling: Applications Using Mplus; Wiley, Higher Education Press: Hoboken, NJ, USA, 2012. [Google Scholar] [CrossRef]
- Kyriazos, T. Applied Psychometrics: Sample Size and Sample Power Considerations in Factor Analysis (EFA, CFA) and SEM in General. Psychology 2018, 9, 2207–2230. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Ruta, L.; Mazzone, D.; Mazzone, L.; Wheelwright, S.; Baron-Cohen, S. The Autism-Spectrum Quotient-Italian version: A cross-cultural confirmation of the broader autism phenotype. J. Autism Develop. Disord. 2012, 42, 625–633. [Google Scholar] [CrossRef]
- Preti, A.; Vellante, M.; Baron-Cohen, S.; Zucca, G.; Petretto, D.R.; Masala, C. The Empathy Quotient: A cross-cultural comparison of the Italian version. Cogn. Neuropsychiatry 2011, 6, 50–70. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 3rd ed.; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Cheung, G.W.; Rensvold, R.B. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct Equ Model. 2002, 9, 233–255. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudeck, R. Alternative ways of assessing model fit. In Testing Structural Equation Models; Bollen, K., Long, J., Eds.; Sage: Newbury Park, CA, USA, 1993; pp. 136–162. [Google Scholar]
- Jöreskog, K.G.; Sörbom, D. LISREL 8.71 [Computer Software]; Scientific Software International Inc.: Lincolnwood, IL, USA, 2004. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates, Publishers: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Tibshirani, R. Regression Shrinkage and Selection via the LASSO. J. R. Soc. Interface 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Friedman, J.; Hastie, T.; Tibshirani, R. The Elements of Statistical Learning: Data Mining, Inference, and Prediction; Springer Series in Statistics; Springer: Berlin/Heidelberg, Germany, 2008; Volume 2. [Google Scholar]
- XLSTAT Statistical and Data Analysis Solution; Addinsoft: New York, NY, USA, 2022; Available online: https://www.xlstat.com/en (accessed on 20 June 2022).
- Hoekstra, R.A.; Bartels, M.; Cath, D.C.; Boomsma, D.I. Factor structure, reliability and criterion validity of the autism- spectrum quotient (AQ): A study in Dutch population and patient groups. J. Autism Develop. Disord 2008, 38, 1555–1566. [Google Scholar] [CrossRef]
- Granner-Shuman, M.; Dahan, A.; Yozevitch, R.; Gvirts Problovski, H.Z. The association among autistic traits, interactional synchrony and typical pattern of motor planning and execution in neurotypical individuals. Symmetry 2021, 13, 1034. [Google Scholar] [CrossRef]
- Bhat, A.N.; Boulton, A.J.; Tulsky, D.S. A further study of relations between motor impairment and social communication, cognitive, language, functional impairments, and repetitive behavior severity in children with ASD using the SPARK study dataset. Autism Res. 2022, 15, 1156–1178. [Google Scholar] [CrossRef]
- Dziuk, M.A.; Larson, J.C.G.; Apostu, A.; Mahone, E.M.; Denckla, M.B.; Mostofsky, S.H. Dyspraxia in autism: Association with motor, social, and communicative deficits. Dev. Med. Child. Neurol. 2007, 49, 734–739. [Google Scholar] [CrossRef] [PubMed]
- Gowen, E.; Hamilton, A. Motor abilities in autism: A review using a computational context. J. Autism Develop. Disord. 2013, 43, 323–344. [Google Scholar] [CrossRef]
- Kilroy, E.; Ring, P.; Hossain, A.; Nalbach, A.; Butera, C.; Harrison, L.; Jayashankar, A.; Vigen, C.; Aziz-Zadeh, L.; Cermak, S.A. Motor performance, praxis, and social skills in autism spectrum disorder and developmental coordination disorder. Autism Res. 2022, 15, 1649–1664. [Google Scholar] [CrossRef]
- Tal-Saban, M.; Kirby, M.A. Adulthood in Developmental Coordination Disorder (DCD): A Review of Current Literature Based on ICF Perspective. Curr. Dev. Disord. Rep. 2018, 5, 9–17. [Google Scholar] [CrossRef]
- Meachon, E.J.; Zemp, M.; Alpers, G.W. Developmental Coordination Disorder (DCD): Relevance for Clinical Psychologists in Europe. Clin. Psychol. Eur. 2022, 4, e4165. [Google Scholar] [CrossRef]


{kind=link}
| Factors | |||
|---|---|---|---|
| Item | [1] ADC-A | [2] ADC-B | [3] ADC-C |
| A10 | 0.553 *** | - | - |
| A7 | 0.515 *** | - | - |
| A4 | 0.463 *** | - | - |
| A2 | 0.402 *** | - | - |
| A9 | 0.381 *** | - | - |
| A3 | 0.360 *** | - | - |
| A8 | 0.348 *** | - | - |
| A5 | 0.320 *** | - | - |
| A6 | 0.298 *** | - | - |
| A1 | 0.218 *** | - | - |
| B7 | - | 0.501 *** | - |
| B4 | - | 0.494 *** | - |
| B5 | - | 0.478 *** | - |
| B6 | - | 0.473 *** | - |
| B8 | - | 0.428 *** | - |
| B3 | - | 0.381 *** | - |
| B9 | - | 0.374 *** | - |
| B10 | - | 0.339 *** | - |
| B1 | - | 0.247 *** | - |
| B2 | - | 0.232 *** | - |
| C4 | - | - | 0.398 *** |
| C19 | - | - | 0.393 *** |
| C3 | - | - | 0.379 *** |
| C1 | - | - | 0.369 *** |
| C2 | - | - | 0.369 *** |
| C15 | - | - | 0.368 *** |
| C20 | - | - | 0.341 *** |
| C18 | - | - | 0.337 *** |
| C16 | - | - | 0.320 *** |
| C12 | - | - | 0.299 *** |
| C7 | - | - | 0.282 *** |
| C9 | - | - | 0.282 *** |
| C17 | - | - | 0.274 *** |
| C14 | - | - | 0.273 *** |
| C5 | - | - | 0.259 *** |
| C6 | - | - | 0.207 *** |
| C13 | - | - | 0.187 *** |
| C10 | - | - | 0.157 ** |
| C8 | - | - | 0.143 ** |
| C11 | - | - | 0.141 * |
| Factors | |||
|---|---|---|---|
| Total Sample (N = 498) | Males (N = 157) | Females (N = 341) | |
| ADC-A | 16.16 (4.60) [9–33] | 16.51 (5.31) [10–33] | 16.00 (4.24) [9–32] |
| ADC-B | 15.80 (4.52) [10–33] | 15.90 (4.80) [10–32] | 15.74 (4.40) [10–33] |
| ADC-C | 36.06 (7.64) [20–63] | 35.04 (7.94) [20–63] | 36.52 (7.46) [21–57] |
| ADC-Total score | 68.01 (14.56) [41–121] | 67.45 (15.82) [41–121] | 68.27 (13.96) [41–117] |
| Variables | Mean | SD | Min | Max |
|---|---|---|---|---|
| 1. AQ-soc | 1.98 | 1.74 | 0 | 8 |
| 2. AQ-switch | 4.60 | 1.92 | 0 | 10 |
| 3. AQ-detail | 5.50 | 2.22 | 0 | 10 |
| 4. AQ-comm | 2.99 | 1.70 | 0 | 8 |
| 5. AQ-ima | 2.55 | 1.61 | 0 | 8 |
| 6. EQ | 47.18 | 10.39 | 17 | 73 |
| 7. SQ | 31.47 | 11.75 | 4 | 73 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. ADC-A | - | ||||||||||
| 2. ADC-B | 0.55 *** [0.49; 0.60] | - | |||||||||
| 3. ADC-C | 0.66 *** [0.61; 0.70] | 0.60 *** [0.55; 0.64] | - | ||||||||
| 4. ADC-Total | 0.83 *** [0.80; 0.85] | 0.80 *** [0.77; 0.82] | 0.92 *** [0.90; 0.93] | - | |||||||
| 5. AQ-soc | 0.14 ** [0.06; 0.21] | 0.15 ** [0.07; 0.22] | 0.26 *** [0.19; 0.32] | 0.23 *** [0.16; 0.30] | - | ||||||
| 6. AQ-switch | 0.20 *** [0.12; 0.27] | 0.17 *** [0.09; 0.24] | 0.27 *** [0.20; 0.33] | 0.26 *** [0.19; 0.32] | 0.36 *** [0.29; 0.42] | - | |||||
| 7. AQ-detail | 0.02 [−0.05; 0.09] | −0.08 [−0.15; 0] | −0.08 [−0.15; 0] | −0.06 [−0.13; 0.01] | 0.03 [−0.04; 0.10] | 0.03 [−0.04; 0.10] | - | ||||
| 8. AQ-comm | 0.33 *** [0.26; 0.39] | 0.26 *** [0.19; 0.32] | 0.34 *** [0.27; 0.40] | 0.36 *** [0.29; 0.42] | 0.45 *** [0.39; 0.50] | 0.36 *** [0.29; 0.42] | 0.04 [−0.03; 0.11] | - | |||
| 9. AQ-ima | 0.13 ** [0.05; 0.20] | 0.09 * [0.01; 0.16] | 0.05 [−0.02; 0.12] | 0.10 * [0.02; 0.17] | 0.17 *** [0.09; 0.24] | 0.14 ** [0.06; 0.21] | 0.09 * [0.01; 0.16] | 0.22 *** [0.14; 0.29] | - | ||
| 10. SQ | −0.10 * [−0.17; −0.02] | −0.17 *** [−0.24; −0.09] | −0.30 *** [−0.36; −0.23] | −0.24 *** [−0.30;−0.17] | −0.03 [−0.10; 0.04] | −0.09 * [−0.16; −0.01] | 0.39 *** [0.32; 0.45] | −0.01 [−0.08; 0.06] | 0.11 ** [0.03; 0.18] | - | |
| 11. EQ | −0.22 *** [−0.29; −0.14] | −0.22 *** [−0.29; −0.14] | −0.25 *** [−0.31; −0.18] | −0.27 *** [−0.33; −0.20] | −0.28 *** [−0.34; −0.21] | −0.21 *** [−0.28; −0.13] | 0.06 [−0.01; 0.13] | −0.44 *** [−0.49; −0.38] | −0.35 *** [−0.41; −0.28] | 0.06 [−0.01; 0.13] | - |
| Model/Factors | Goodness of Fit | Coefficients | ||||||
|---|---|---|---|---|---|---|---|---|
| Cohen’s f2 | R2 | R2 90% CI | RMSE | MSE | Lambda | Coeff. | Beta Values | |
| 1. ADC-A | 0.183 | 0.155 | [0; 0.598] | 0.92 | 0.86 | 0.03 | ||
| AQ-soc | 0 * | 0 * | ||||||
| AQ-switch | 0.043 | 0.043 | ||||||
| AQ-detail | 0.011 | 0.011 | ||||||
| AQ-comm | 0.290 | 0.296 | ||||||
| AQ-ima | 0.030 | 0.030 | ||||||
| EQ | −0.016 | −0.016 | ||||||
| SQ | −0.106 | −0.104 | ||||||
| 2. ADC-B | 0.162 | 0.140 | [0; 0.583] | 0.92 | 0.84 | 0.01 | ||
| AQ-soc | 0.020 | 0.020 | ||||||
| AQ-switch | 0.057 | 0.057 | ||||||
| AQ-detail | 0 * | 0 * | ||||||
| AQ-comm | 0.171 | 0.175 | ||||||
| AQ-ima | 0.040 | 0.040 | ||||||
| EQ | −0.100 | −0.100 | ||||||
| SQ | −0.175 | −0.175 | ||||||
| 3. ADC-C | 0.356 | 0.263 | [0; 0.683] | 0.87 | 0.76 | 0.02 | ||
| AQ-soc | 0.080 | 0.081 | ||||||
| AQ-switch | 0.103 | 0.104 | ||||||
| AQ-detail | 0 * | 0 * | ||||||
| AQ-comm | 0.234 | 0.239 | ||||||
| AQ-ima | 0 * | 0 * | ||||||
| EQ | −0.065 | −0.065 | ||||||
| SQ | −0.264 | −0.261 | ||||||
| 4. ADC-Total | 0.336 | 0.252 | [0; 0.676] | 0.87 | 0.77 | 0.01 | ||
| AQ-soc | 0.041 | 0.041 | ||||||
| AQ-switch | 0.097 | 0.098 | ||||||
| AQ-detail | 0.012 | 0.012 | ||||||
| AQ-comm | 0.278 | 0.284 | ||||||
| AQ-ima | 0.018 | 0.018 | ||||||
| EQ | −0.083 | −0.083 | ||||||
| SQ | −0.246 | −0.242 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zappullo, I.; Conson, M.; Baiano, C.; Cecere, R.; Raimo, G.; Kirby, A. The Relationships between Self-Reported Motor Functioning and Autistic Traits: The Italian Version of the Adult Developmental Coordination Disorders/Dyspraxia Checklist (ADC). Int. J. Environ. Res. Public Health 2023, 20, 1101. https://doi.org/10.3390/ijerph20021101
Zappullo I, Conson M, Baiano C, Cecere R, Raimo G, Kirby A. The Relationships between Self-Reported Motor Functioning and Autistic Traits: The Italian Version of the Adult Developmental Coordination Disorders/Dyspraxia Checklist (ADC). International Journal of Environmental Research and Public Health. 2023; 20(2):1101. https://doi.org/10.3390/ijerph20021101
Chicago/Turabian StyleZappullo, Isa, Massimiliano Conson, Chiara Baiano, Roberta Cecere, Gennaro Raimo, and Amanda Kirby. 2023. "The Relationships between Self-Reported Motor Functioning and Autistic Traits: The Italian Version of the Adult Developmental Coordination Disorders/Dyspraxia Checklist (ADC)" International Journal of Environmental Research and Public Health 20, no. 2: 1101. https://doi.org/10.3390/ijerph20021101
APA StyleZappullo, I., Conson, M., Baiano, C., Cecere, R., Raimo, G., & Kirby, A. (2023). The Relationships between Self-Reported Motor Functioning and Autistic Traits: The Italian Version of the Adult Developmental Coordination Disorders/Dyspraxia Checklist (ADC). International Journal of Environmental Research and Public Health, 20(2), 1101. https://doi.org/10.3390/ijerph20021101