Abstract
Background: Physical exercise can slow down the decline of the cognitive function of the older adults, yet the review evidence is not conclusive. The purpose of this study was to compare the effects of aerobic and resistance training on cognitive ability. Methods: A computerized literature search was carried out using PubMed, Cochrane Library, Embase SCOPUS, Web of Science, CNKI (China National Knowledge Infrastructure), Wanfang, and VIP database to identify relevant articles from inception through to 1 October 2022. Based on a preliminary search of the database and the references cited, 10,338 records were identified. For the measured values of the research results, the standardized mean difference (SMD) and 95% confidence interval (CI) were used to synthesize the effect size. Results: Finally, 10 studies were included in this meta-analysis. Since the outcome indicators of each literature are different in evaluating the old cognitive ability, a subgroup analysis was performed on the included literature. The study of results suggests that aerobic or resistance training interventions significantly improved cognitive ability in older adults compared with control interventions with the Mini-Mental State Examination (MD 2.76; 95% CI 2.52 to 3.00), the Montreal Cognitive Assessment (MD 2.64; 95% CI 2.33 to 2.94), the Wechsler Adult Intelligence Scale (MD 2.86; 95% CI 2.25 to 3.47), the Wechsler Memory Scale (MD 9.33; 95% CI 7.12 to 11.54), the Wisconsin Card Sorting Test (MD 5.31; 95% CI 1.20 to 9.43), the Trail Making Tests (MD −8.94; 95% CI −9.81 to −8.07), and the Stroop Color and Word Test (MD −5.20; 95% CI −7.89 to −2.51). Conclusion: Physical exercise improved the cognitive function of the older adults in all mental states. To improve cognitive ability, this meta-analysis recommended that patients perform at least moderate-intensity aerobic exercise and resistance exercise on as many days as possible in the week to comply with current exercise guidelines while providing evidence for clinicians.
1. Introduction
The ageing of the population is an issue of widespread concern worldwide. The Report on World Population Trends (now referred to as the Report) issued at the 51st session of the United Nations Commission on Population and Development pointed out that the global population would reach 9.8 billion by 2050. The number of older adults over 65 will exceed 1.5 billion, accounting for 16% of the total population. Normal ageing is typically associated with both physical and cognitive decline. Cognitive functioning changes as people grow older. Cognitive function includes memory, language, visual space, execution, calculation, understanding, and judgment [1]. Most of the older adults also experience a cognitive decline to varying degrees, which will not only reduce the quality of life but also affect the basic activities of daily living ability, reduce the remaining life expectancy, and increase the risk of death [2]. Therefore, determining the biological mechanism of cognitive ageing and seeking preventive measures to offset its harmful effects are the current priorities in clinical and public health.
It is hypothesized that the neural and vascular adaptations to physical exercise improve cognitive function through promotion of neurogenesis, angiogenesis, synaptic plasticity, decreased proinflammatory processes, and reduced cellular damage due to oxidative stress. In non-medical therapy, as a low-cost, low-risk, and ready-made intervention, physical exercise has been widely accepted by the public and medical rehabilitation workers [3]. Regular physical exercise was a critical factor in preventing and managing non-communicable diseases. Physical exercise is also conducive to mental health, preventing cognitive decline, depression, and anxiety symptoms, and helps maintain body mass and overall well-being. Many experiments and clinical studies have shown that physical exercise can improve the cognitive function of the older adults [4,5,6]. Regular and active physical activities of the older adults can promote the maintenance, improvement, or rehabilitation of biological processes and slow down the decline of age-related cognitive functions. However, although some experiments have proposed the beneficial effect of physical activity on healthy older adults, there was no specific conclusion at present [7,8].
The Mini-Mental State Examination (MMSE) is a global clinical psychological, neuropsychological indicator usually used to screen and evaluate the cognitive status of patients. It can comprehensively, accurately, and quickly reflect the intellectual quality and cognitive impairment of the subjects [9]. However, there are many scales to evaluate cognitive ability. By incorporating different screening methods, we can more comprehensively assess the cognitive function of the older adults. In the past few decades, many scientific research teams have studied the effect of exercise on the cognitive function of the older adults in randomized controlled trials [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30]. However, there were contradictions between the results of these studies, and there was no clear conclusion. This systematic review and meta-analysis intends to explore the following questions: (i) the effects of exercise interventions of aerobic and resistance training modes on cognitive ability in the older adults; and (ii) the effects of exercise on different cognitive task results in the older adults.
2. Materials and Methods
2.1. Data Sources and Searches
This article was followed by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guideline [31]. A literature search used PubMed, Cochrane Library, Embase SCOPUS, Web of Science, CNKI (China National Knowledge Infrastructure), Wanfang and VIP database to identify relevant articles from inception through to 1 October 2022. This paper searched three classes of keywords: “cognitive”, “older adults”, and “exercise”. The first keywords were “cognition”, “executive function”, “cognitive ability”, “cognitive decline”, and “memory”. The second keywords were “older adults”, “aged”, “old people”, and “elderly people”. The exercise keywords were “exercise”, “physical exercise”, “aerobic exercise”, “strength training”, and “intervention”. The search strategy for PubMed is presented in Table 1.

Table 1.
Database search of PubMed.
2.2. Inclusion and Exclusion Criteria
Literature inclusion was based on evidence-based medicine PICOS framework, mainly considering five factors: participants, intervention measures, control group, research results, and research design [32]. Inclusion criteria were as follows: (i) participants were over the aged of 50 years or older; (ii) the treatment groups were intervention consisting of physical exercise or physical activity; (iii) the control group included routine home care, health education, or lifestyle maintenance; (iv) the outcomes include the use of any standardized neuropsychological instrument to measure cognitive ability, and the statistics include: sample size, mean, and standard deviation; and (v) the studies’ design was strictly limited to randomized controlled trials (RCTs).
Trials were excluded if they met one of the following exclusion criteria: (i) studies that do not meet the inclusion criteria; (ii) studies without available data for statistics; (iii) conference abstract, observational study, dissertation, or letter; and (iv) exclude articles other than English or Chinese.
2.3. Study Selection and Data Extraction
The retrieved literature was screened by three researchers (L.X., H.G., and X.C.) in an independent double-blind way according to the inclusion and exclusion criteria. The first step was to exclude articles that did not meet the inclusion criteria by reading the title and abstract of the literature. The second part was to read and screen the remaining documents in full and determine the final documents to be included. The two researchers (L.X. and H.G.) independently extracted the literature that met the criteria, including the following information: author name; publication year of the article; participants’ characteristics (e.g., age and gender); the number of participants in each group; intervention content; intervention time; intervention frequency; intervention cycle; and reported outcomes. The number of participants, average value, and standard deviation (SD) in each group before and after the intervention training were extracted from the articles included in the analysis.
2.4. Quality Assessment
The two authors (L.X. and H.G.) evaluated the methodological quality of the included literature, using the Cochrane Collaboration risk bias assessment tools to assess from the following seven areas [33]: selection bias, performance bias, detection bias, attrition bias, reporting bias, and any other preferences. Each indicator was judged by low bias risk, uncertainty, or high bias risk. Any differences arising from the evaluation process shall be settled by the third arbitrator (X.H.).
2.5. Statistical Analysis
Statistical analyses were undertaken using Review Manager 5.4 (Cochrane Collaboration) and Stata version 12.0 (Stata Corp). Since the measurement scores of the exercise group and the control group from baseline to the endpoint are continuous variables, Standardized mean difference (SMD) and 95% confidence intervals (CIs) were calculated according to the mean, standard deviation and sample number of outcomes indicators of the intervention group and the control group. The heterogeneity across the studies was evaluated using the I2 statistic. I2 represents the heterogeneity of the study; when I2 ≤ 25%, it indicated insignificant heterogeneity. The moderate heterogeneity was assessed when I2 ≤ 50% and I2 > 25%. When I2 ≤ 75% and I2 > 50%, it indicated high heterogeneity [33]. I2 represents the heterogeneity of the study; if I2 < 50% or p ≥ 0.05, the fixed effect model is used to combine the effects; If I2 ≥ 50% and p < 0.05, the random effect model is used for analysis.
If there is heterogeneity, a subgroup analysis of regulatory variables is performed. Visual analysis of funnel plot symmetry was used to test publication bias [34]. We conducted subgroup analysis according to the gender and age of the participants, the type of intervention, and the duration of the intervention to further explore the source of heterogeneity. All tests were two-tailed, with inspection level α = 0.05; when the bilateral test p < 0.05, it is considered that the difference is statistically significant.
3. Results
3.1. Search Results
Through searching Chinese and foreign databases, 10,336 articles were preliminarily obtained. Two articles were retrieved manually from other resources. Two independent researchers screened 9185 titles and abstracts after eliminating duplicate published articles. After screening the title and abstract, 9135 research articles were excluded. After filtering titles and abstracts, 9135 articles were excluded. The remaining 50 articles were read in totality, and 21 were included in the final analysis, meeting the requirements of systematic evaluation and meta-analysis. The third reviewer will discuss and decide on any differences in the literature screening process. The search procedure is presented in Figure 1.
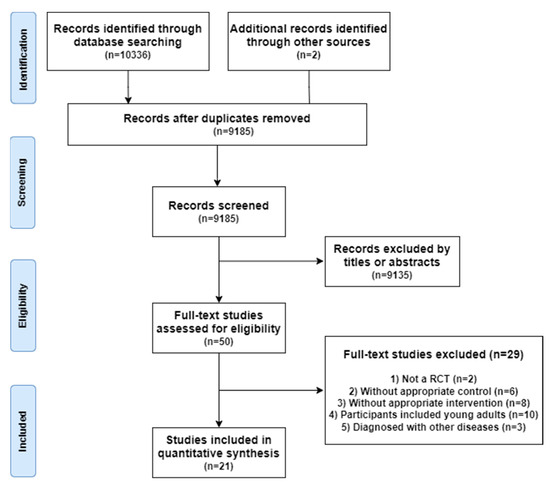
Figure 1.
Flowchart representing the selection progress.
3.2. Studies Characteristics
A total of 21 RCT research articles were included in the mate-analysis [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30]. All included studies were published between 2000 and 2022, including 1414 participants. The subjects in most studies were mixed-gender groups. The topics in five studies were only women [13,18,20,27,28], and only male participants were included in three studies [22,23,29]. For exercise types, 12 trials performed physical exercise [10,11,12,13,14,15,16,17,18,19,20,21], and 9 tests performed mind–body exercise [22,23,24,25,26,27,28,29,30]. The duration of exercise intervention varies from 8 to 52 weeks, and each study has its own time and frequency of intervention. Details of study characteristics are presented in Table 2.
Table 2.
Characteristics of the included trials and participants.
3.3. Quality Evaluation
A summary of the bias risks of all included studies in the meta-analysis is shown in Figure 2A. Figure 2B shows the deviation risk of bias for self-reported and physiological measurement of each included study according to the Cochrane risk of bias tool [33]. These 21 studies have relatively high quality, 12 trials reported the generation process of random sequences, and 5 trials reported the methods used to allocate hiding. Because the subjects have to carry out exercise intervention and cannot be blinded, the performance bias assessment in the study was high risk.
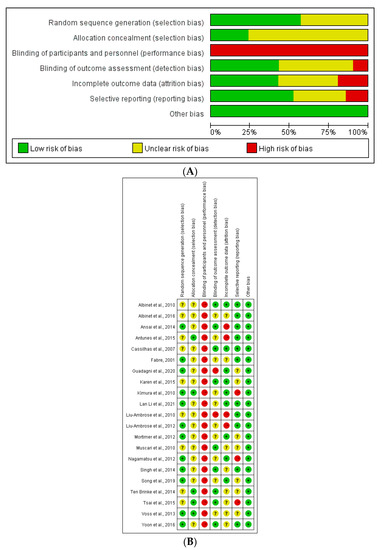
Figure 2.
(A). Risk of bias summary; (B) risk of bias assessments [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30].
3.4. Effects of Exercise on Cognitive Functions
This meta-analysis synthesizes the outcome data of the included studies using the same outcome indicators. Overall, the meta-analysis included the following cognitive abilities outcome indicators: the Mini-Mental State Examination (MMSE), the Montreal Cognitive Assessment (MoCA), the Wechsler Adult Intelligence Scale (WAIS), the Wechsler memory scale (WMS), the Wisconsin card sorting test (WCST), the Trail Making Tests (TMT), and the Stroop Color and Word Test (SCWT). The study found that the exercise intervention methods for the cognitive function of the older adults were mainly divided into two categories: aerobic and resistance exercise.
Twelve studies reported the outcomes of the MMSE scale. Figure 3 shows that the MMSE score of the exercise group was higher than that of the control group (MD 2.76; 95% CI 2.52 to 3.00; p < 0.00001; I2 = 18%), and the heterogeneity between studies was low. Six articles reported the evaluation outcomes of the MoCA scale. The MoCA scores of the exercise group were higher than that of the control group (MD 2.64; 95% CI 2.33 to 2.9; p < 0.00001; I2 = 0%). There was no heterogeneity between studies (Figure 4). Four studies reported the outcomes of WAIS. Compared with the control group, the WAIS score of the exercise group increased significantly (MD 2.86; 95% CI 2.25 to 3.47; p < 0.00001; I2 = 39%), and the heterogeneity between studies was low (Figure 5). Three studies provided the evaluating outcomes of the WMS scale. Figure 6 shows that the exercise group’s WMS score significantly increased compared with the control group (MD 9.33; 95% CI 7.12 to 11.54; p < 0.00001; I2 = 28%), and the heterogeneity between studies was low. Two studies provided the evaluating outcomes of the WCST scale. Figure 7 shows that the WCST score of the exercise group was higher than that of the control group (MD 5.31; 95% CI 1.20 to 9.43; p = 0.01; I2 = 0%). There was no heterogeneity between studies. Three studies provided the evaluating outcomes of the TMT scale. As shown in Figure 8, the analysis indicates, compared with the control group, a significant decrease in TMT scores in the exercise group (MD −8.94; 95% CI −9.81 to −8.07; p < 0.00001; I2 = 30%). Three studies provided the evaluating outcomes of the SCWT scale. The SCWT scores of the exercise group were lower than that of the control group (MD −5.20; 95% CI −7.89 to −2.51; p = 0.0002; I2 = 0%). There was no heterogeneity between studies (Figure 9).
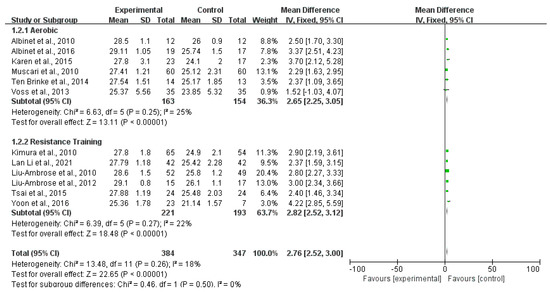
Figure 3.
Forest plots of MMSE scale outcomes in overall analysis [10,11,13,17,20,21,25,26,27,28,29,30].
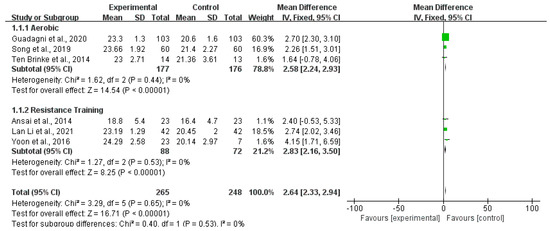
Figure 4.
Forest plots of MoCA scale outcomes in overall analysis [15,19,20,22,26,30].
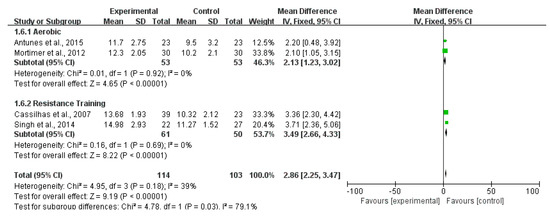
Figure 5.
Forest plots of WAIS scale outcomes in overall analysis [12,16,23,24].

Figure 6.
Forest plots of WMS scale outcomes in overall analysis [14,23,24].

Figure 7.
Forest plots of WCST scale outcomes in overall analysis [11,13].

Figure 8.
Forest plots of TMT scale outcomes in overall analysis [16,18,27].

Figure 9.
Forest plots of SCWT scale outcomes in overall analysis [11,13].
3.5. Publication Bias
A visual inspection of the funnel plots for seven different outcomes (Figure 10) indicated no publication bias for the cognitive ability of the older adults.
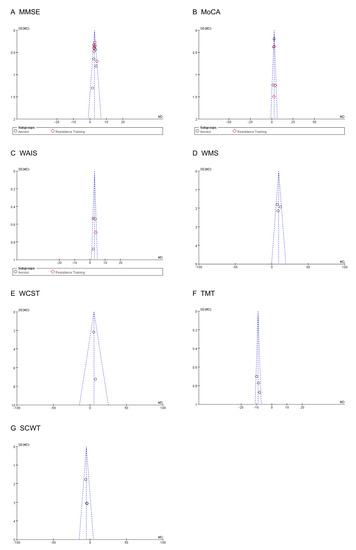
Figure 10.
Funnel plot assessing the publication bias.
4. Discussion
This study explored the intervention effect of exercise on the cognitive function of the older adults from the perspective of evidence-based medicine. The results showed that exercise could effectively delay the decline of the cognitive function of the older adults. According to 21 eligible trials, we extracted and analyzed cognitive ability (MMSE, MoCA, WAIS, WMS, WCST, TMT, SCWT scales) outcomes to evaluate the cognitive function change after exercise interventions. The key finding from this study is that physical exercise interventions effectively improve cognitive function in the elder, regardless of mental status.
The overall analyses suggest evident improvements in exercise on cognitive ability in the elder. The study found that the scores of the cognitive ability assessment scale (MMSE, MoCA, WAIS, WMS, and WCST) were significantly increased in the low heterogeneity and non-heterogeneity intervention groups. Specifically, exercise positively affected cognitive ability by reducing scores on TMT and SCWT scales.
Studies that included aerobic or resistance training in traditional exercise patterns showed similar results. Some studies [35] have found that changes in carotid artery elasticity and imbalance of vasoconstriction and relaxation function can aggravate the degree of cognitive ability damage. These changes will significantly affect the body’s ability to supply blood and oxygen to brain tissue, causing a large amount of oxygen free radicals to accumulate and damage brain tissue. Therefore, exercise can improve cardiovascular function, increase cerebral blood flow and oxygen supply capacity, give brain tissue cells more nutrition, help maintain brain function, and, thus, delay or reverse the neurodegenerative process and disease tracking.
Our study suggests that aerobic exercise benefits older adults’ cognitive functioning. Studies have investigated the effects of two short-term exercise intervention plans on various outcome parameters and executive ability of heart rate variability (HRV) in the older adults by Albinet et al. [11]. The results emphasize that aerobic exercise intervention played an essential role in cardio cerebral vascular protection and show a direct relationship between exercise, HRV, and cognition in the older adults. In addition, some studies have also concluded that specific aerobic intervention can improve the cognitive function of the older adults to varying degrees [10,12,13,14,15,16,17,18,19,20,21].
This study suggests that resistance training may be essential in improving cognitive function in older adults [36]. Resistance exercise can increase the operation of muscle pumps by squeezing peripheral blood vessels, which can increase the cardiac output per stroke, thus increasing cerebral perfusion. Liu-Ambrose et al. compared the effects of different resistance training models on the cognitive function of the older adults [27]. The results showed that resistance training benefited the older women’s selective attention and the executive effect of cognitive ability. This indicates that the intervention of resistance movement has a particularly significant impact on the cognitive function of these older people [22,23,24,25,26,28,29,30].
Previous studies believed that exercise positively impacts the cognitive ability of the older adults, improving memory and inhibition control functions. Exercise is an effective means to treat and intervene in cognitive impairment in the older adults, consistent with the previous review [35,37]. Some studies showed that exercise intervention could improve the cognitive function of the older adults, providing strong evidence for exercise as an effective non-drug intervention. Still, the method of exercise needs to be designed according to the differences between different individuals, which was the main reason for the differences in many research results. In addition, most of the studies were aimed at patients’ physical indicators and cognitive ability, and there were few studies on the mechanism of brain action.
This paper summarizes the intervention of different intervention methods, different from other studies that outline a single sports event. The utility of different periodic and types of sports was more straightforward, which provided a reference for future research and practical application. This paper summarizes the beneficial evidence of aerobic exercise and resistance exercise in improving the cognitive ability of the older adults points out the positive effect of aerobic exercise and resistance movement on improving mild cognitive impairment and emphasizes that we must follow the scientific and safe principles, adopt reasonable exercise methods, improve the cognitive ability of the older adults through regular scientific exercise, improve the body ability and cardiopulmonary function, and provide conditions for the older adults to maintain continuous training.
This study was carried out following the PRISMA statement list, but there were still some shortcomings and limitations. First, the search scope for the literature does not include unpublished literature, and some literature is not included due to incomplete outcome index data, which may affect the comprehensiveness of the data to some extent. Meanwhile, the sample size of the meta-analysis fit in the study is small, which may also reduce the reliability of the analysis results. Finally, although two researchers used an independent double-blind method to evaluate the quality of the included literature, they only used the “Cochrane Risk Bias Tool” for evaluation. Due to subjective judgment errors, specific evaluation errors may be caused. Therefore, it is recommended to add other judgment criteria to minimize personal evaluation error.
5. Conclusions
This systematic review and meta-analysis demonstrate that regular exercise benefits older adults’ cognitive function. Exercise could be used as a supplementary therapy to treat the cognitive decline of the older adults.
Author Contributions
Designed the study and wrote the protocol, L.X., H.G., X.C., X.H. and Y.Z.; Independent screening and data extraction, L.X., H.G. and X.C.; Quality scoring, J.Y. and T.S.; Statistical analysis and wrote the first draft, L.X. and H.G.; Revised the manuscript, X.H. and Y.Z. All the authors made significant contributions to the final manuscript and approved its publication. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by “the National Key Research and Development Program of China” (2020YFC2006701).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are openly available in the studies referenced in the figures. The individual data in each can be seen in the original manuscripts.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Colcombe, S.J.; Erickson, K.I.; Raz, N.; Webb, A.G.; Cohen, N.J.; McAuley, E.; Kramer, A.F. Aerobic fitness reduces brain tissue loss in aging humans. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2003, 58, 176–180. [Google Scholar] [CrossRef]
- Van Dam, P.S.; Aleman, A. Insulin-like growth factor-I, cognition and brain aging. Eur. J. Pharmacol. 2004, 490, 87–95. [Google Scholar] [CrossRef]
- Angevaren, M.; Aufdemkampe, G.; Verhaar, H.J.; Aleman, A.; Vanhees, L. Physical activity and enhanced fitness to improve cognitive function in older people without known cognitive impairment. Cochrane Database Syst. Rev. 2008, 3, 538–541. [Google Scholar]
- Kronenberg, G.; Bick-Sander, A.; Bunk, E.; Wolf, C.; Ehninger, D.; Kempermann, G. Physical exercise prevents age-related decline in precursor cell activity in the mouse dentate gyrus. Neurobiol. Aging 2006, 27, 1505–1513. [Google Scholar] [CrossRef] [PubMed]
- Van Uffelen, J.G.; Chin, A.P.M.J.; Hopman-Rock, M.; Van Mechelen, W. The effects of exercise on cognition in older adults with and without cognitive decline: A systematic review. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2008, 18, 486–500. [Google Scholar] [CrossRef] [PubMed]
- Pedroli, E.; Greci, L.; Colombo, D.; Serino, S.; Cipresso, P.; Arlati, S.; Mondellini, M.; Boilini, L.; Giussani, V.; Goulene, K.; et al. Characteristics, Usability, and Users Experience of a System Combining Cognitive and Physical Therapy in a Virtual Environment: Positive Bike. Sensors 2018, 18, 2343. [Google Scholar] [CrossRef]
- Kramer, A.F.; Hahn, S.; Cohen, N.J.; Banich, M.T.; McAuley, E.; Harrison, C.R.; Chason, J.; Vakil, E.; Bardell, L.; Boileau, R.A. Ageing, fitness and neurocognitive function. Nature 1999, 400, 418–429. [Google Scholar] [CrossRef]
- Colcombe, S.; Kramer, A.F. Fitness effects on the cognitive function of older adults: A meta-analytic study. Psychol. Sci. 2003, 14, 125–130. [Google Scholar] [CrossRef]
- Mitrushina, M.; Satz, P. Reliability and validity of the Mini-Mental State Exam in neurologically intact elderly. J. Clin. Psychol. 1991, 47, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Albinet, C.T.; Abou-Dest, A.; André, N.; Audiffren, M. Executive functions improvement following a 5-month aquaerobics program in older adults: Role of cardiac vagal control in inhibition performance. Biol. Psychol. 2016, 115, 69–77. [Google Scholar] [CrossRef]
- Albinet, C.T.; Boucard, G.; Bouquet, C.A.; Audiffren, M. Increased heart rate variability and executive performance after aerobic training in the elderly. Eur. J. Appl. Physiol. 2010, 109, 617–624. [Google Scholar] [CrossRef] [PubMed]
- Antunes, H.K.; De Mello, M.T.; Santos-Galduróz, R.F.; Galduróz, J.C.; Lemos, V.A.; Tufik, S.; Bueno, O.F. Effects of a physical fitness program on memory and blood viscosity in sedentary elderly men. Braz. J. Med. Biol. Res. Rev. Bras. Pesqui. Med. Biol. 2015, 48, 805–812. [Google Scholar] [CrossRef]
- Antunes, H.K.; Santos-Galduroz, R.F.; De Aquino Lemos, V.; Bueno, O.F.; Rzezak, P.; De Santana, M.G.; De Mello, M.T. The influence of physical exercise and leisure activity on neuropsychological functioning in older adults. Age 2015, 37, 981–995. [Google Scholar] [CrossRef] [PubMed]
- Fabre, C.; Chamari, K.; Mucci, P.; Massé-Biron, J.; Préfaut, C. Improvement of cognitive function by mental and/or individualized aerobic training in healthy elderly subjects. Int. J. Sport. Med. 2002, 23, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Guadagni, V.; Drogos, L.L.; Tyndall, A.V.; Davenport, M.H.; Anderson, T.J.; Eskes, G.A.; Longman, R.S.; Hill, M.D.; Hogan, D.B.; Poulin, M.J. Aerobic exercise improves cognition and cerebrovascular regulation in older adults. Neurology 2020, 94, 2245–2257. [Google Scholar] [CrossRef]
- Mortimer, J.A.; Ding, D.; Borenstein, A.R.; DeCarli, C.; Guo, Q.; Wu, Y.; Zhao, Q.; Chu, S. Changes in brain volume and cognition in a randomized trial of exercise and social interaction in a community-based sample of non-demented Chinese elders. J. Alzheimer’s Dis. JAD 2012, 30, 757–766. [Google Scholar] [CrossRef]
- Muscari, A.; Giannoni, C.; Pierpaoli, L.; Berzigotti, A.; Maietta, P.; Foschi, E.; Ravaioli, C.; Poggiopollini, G.; Bianchi, G.; Magalotti, D. Chronic endurance exercise training prevents aging-related cognitive decline in healthy older adults: A randomized controlled trial. Int. J. Geriatr. Psychiatry 2010, 25, 1055–1064. [Google Scholar] [CrossRef]
- Nagamatsu, L.S.; Handy, T.C.; Hsu, C.L.; Voss, M.; Liu-Ambrose, T. Resistance training promotes cognitive and functional brain plasticity in seniors with probable mild cognitive impairment. Arch. Intern. Med. 2012, 172, 666–678. [Google Scholar] [CrossRef]
- Song, D.; Yu, D.S.F. Effects of a moderate-intensity aerobic exercise programme on the cognitive function and quality of life of community-dwelling elderly people with mild cognitive impairment: A randomised controlled trial. Int. J. Nurs. Stud. 2019, 93, 97–105. [Google Scholar] [CrossRef]
- Ten Brinke, L.F.; Bolandzadeh, N.; Nagamatsu, L.S.; Hsu, C.L.; Davis, J.C.; Miran-Khan, K.; Liu-Ambrose, T. Aerobic exercise increases hippocampal volume in older women with probable mild cognitive impairment: A 6-month randomised controlled trial. Br. J. Sport. Med. 2015, 49, 248–254. [Google Scholar] [CrossRef]
- Voss, M.W.; Heo, S.; Prakash, R.S.; Erickson, K.I.; Alves, H.; Chaddock, L.; Szabo, A.N.; Mailey, E.L.; Wójcicki, T.R.; White, S.M. The influence of aerobic fitness on cerebral white matter integrity and cognitive function in older adults: Results of a one-year exercise intervention. Hum. Brain Mapp. 2013, 34, 2972–2985. [Google Scholar] [CrossRef]
- Ansai, J.H.; Rebelatto, J.R. Effect of two physical exercise protocols on cognition and depressive symptoms in oldest-old people: A randomized controlled trial. Geriatr. Gerontol. Int. 2015, 15, 1127–1134. [Google Scholar] [CrossRef]
- Cassilhas, R.C.; Viana, V.A.; Grassmann, V.; Santos, R.T.; Santos, R.F.; Tufik, S.; Mello, M.T. The impact of resistance exercise on the cognitive function of the elderly. Med. Sci. Sport. Exerc. 2007, 39, 1401–1407. [Google Scholar] [CrossRef] [PubMed]
- Fiatarone Singh, M.A.; Gates, N.; Saigal, N.; Wilson, G.C.; Meiklejohn, J.; Brodaty, H.; Wen, W.; Singh, N.; Baune, B.T.; Suo, C. The Study of Mental and Resistance Training (SMART) study—Resistance training and/or cognitive training in mild cognitive impairment: A randomized, double-blind, double-sham controlled trial. J. Am. Med. Dir. Assoc. 2014, 15, 873–880. [Google Scholar] [CrossRef]
- Kimura, K.; Obuchi, S.; Arai, T.; Nagasawa, H.; Shiba, Y.; Watanabe, S.; Kojima, M. The influence of short-term strength training on health-related quality of life and executive cognitive function. J. Physiol. Anthropol. 2010, 29, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Liu, M.; Zeng, H.; Pan, L. Multi-component exercise training improves the physical and cognitive function of the elderly with mild cognitive impairment: A six-month randomized controlled trial. Ann. Palliat. Med. 2021, 10, 8919–8929. [Google Scholar] [CrossRef] [PubMed]
- Liu-Ambrose, T.; Nagamatsu, L.S.; Graf, P.; Beattie, B.L.; Ashe, M.C.; Handy, T.C. Resistance training and executive functions: A 12-month randomized controlled trial. Arch. Intern. Med. 2010, 170, 170–178. [Google Scholar] [CrossRef]
- Liu-Ambrose, T.; Nagamatsu, L.S.; Voss, M.W.; Khan, K.M.; Handy, T.C. Resistance training and functional plasticity of the aging brain: A 12-month randomized controlled trial. Neurobiol. Aging 2012, 33, 1690–1698. [Google Scholar] [CrossRef]
- Tsai, C.L.; Wang, C.H.; Pan, C.Y.; Chen, F.C. The effects of long-term resistance exercise on the relationship between neurocognitive performance and GH, IGF-1, and homocysteine levels in the elderly. Front. Behav. Neurosci. 2015, 9, 23–33. [Google Scholar] [CrossRef]
- Yoon, D.H.; Kang, D.; Kim, H.J.; Kim, J.S.; Song, H.S.; Song, W. Effect of elastic band-based high-speed power training on cognitive function, physical performance and muscle strength in older women with mild cognitive impairment. Geriatr. Gerontol. Int. 2017, 17, 765–772. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71–80. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, 5928–5936. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Northey, J.M.; Cherbuin, N.; Pumpa, K.L.; Smee, D.J.; Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br. J. Sport. Med. 2018, 52, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Gates, N.; Fiatarone Singh, M.A.; Sachdev, P.S.; Valenzuela, M. The effect of exercise training on cognitive function in older adults with mild cognitive impairment: A meta-analysis of randomized controlled trials. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2013, 21, 1086–1097. [Google Scholar] [CrossRef]
- Liu, L.; Jia, L.; Jian, P.; Zhou, Y.; Zhou, J.; Wu, F.; Tang, Y. The Effects of Benzodiazepine Use and Abuse on Cognition in the Elders: A Systematic Review and Meta-Analysis of Comparative Studies. Front. Psychiatry 2020, 11, 755–768. [Google Scholar] [CrossRef]










Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).