
Decision Support Frameworks in Public Health Emergencies: A Systematic Review of Dynamic Models in Complex Contexts

 ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
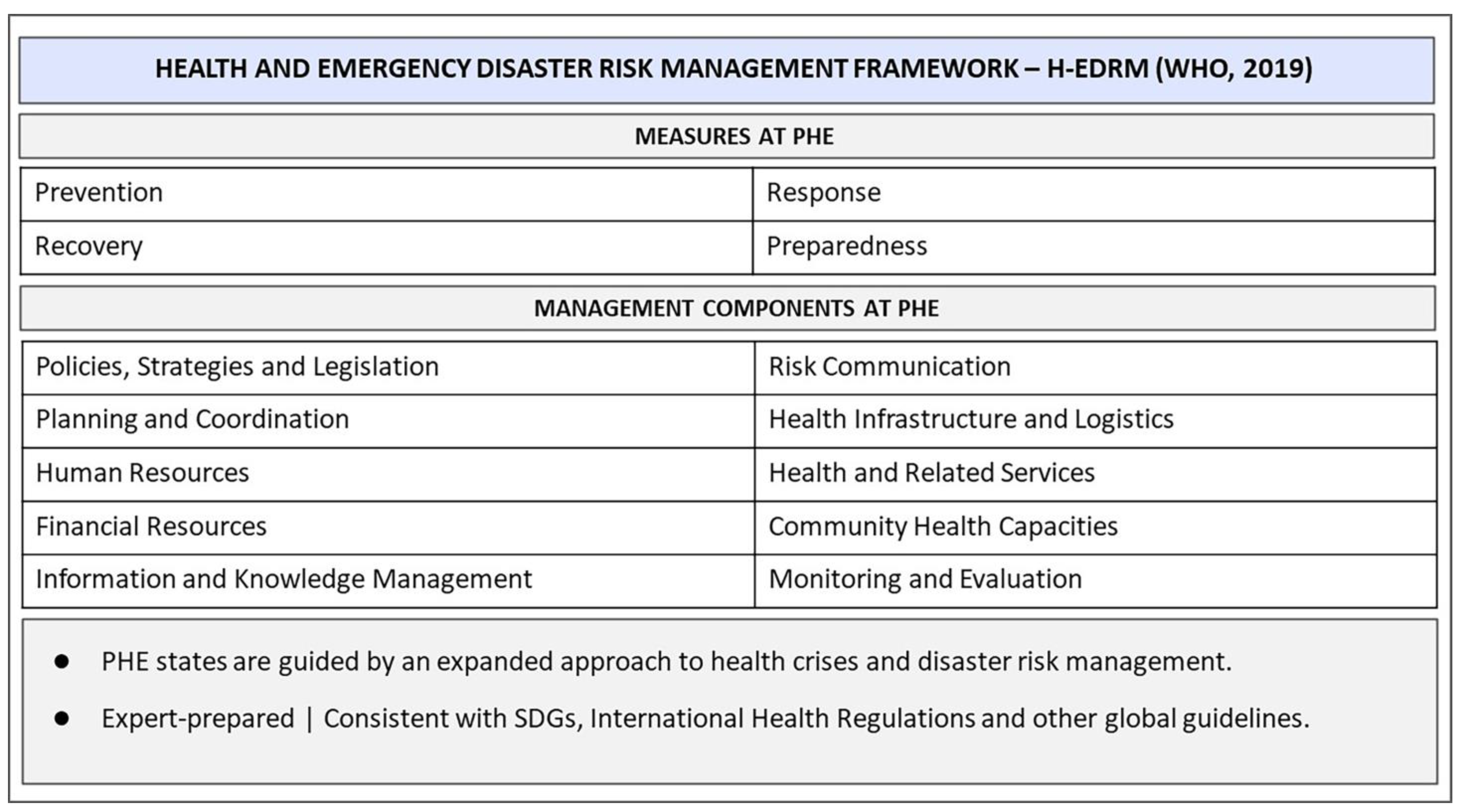
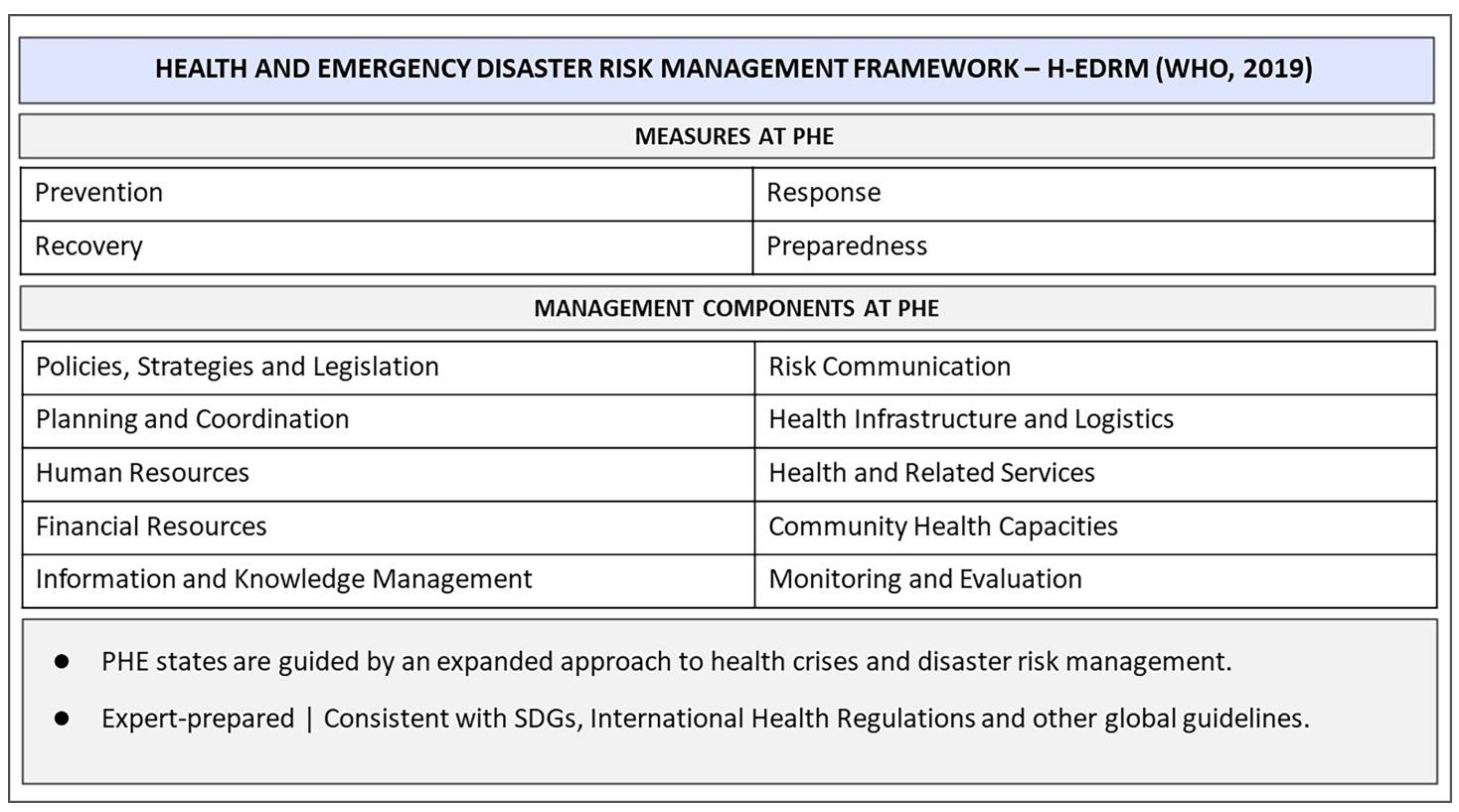
2. Decision Support Frameworks in Public Health Emergencies: Concepts, Complexities, and Managerial Intervention Capacity
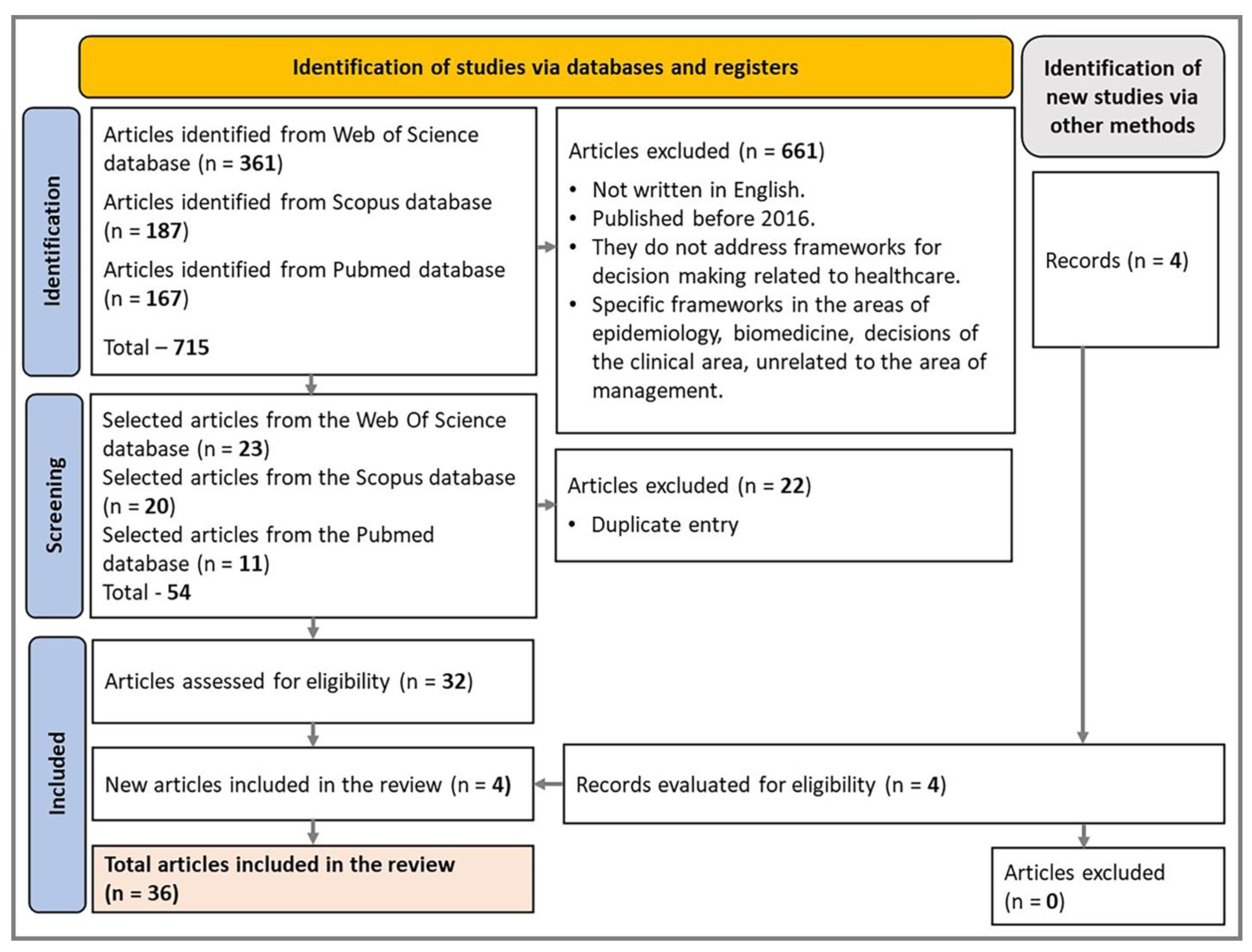
3. Materials and Methods
3.1. Planning
3.2. Defining the Scope
3.3. Bibliographic Research
3.4. Database Evaluation
- E1: Exclude studies that do not address frameworks for health-related decision making.
- E2: Exclude specialized framework studies irrelevant to management from the fields of epidemiology, biomedicine, and clinical area decisions.
- E3: Exclude non-English-written studies, due to the impossibility of evaluating titles in all languages and English being the predominant language in the knowledge bases searched.
- E4: Exclude research published before 2016.
3.5. Synthesis and Analysis
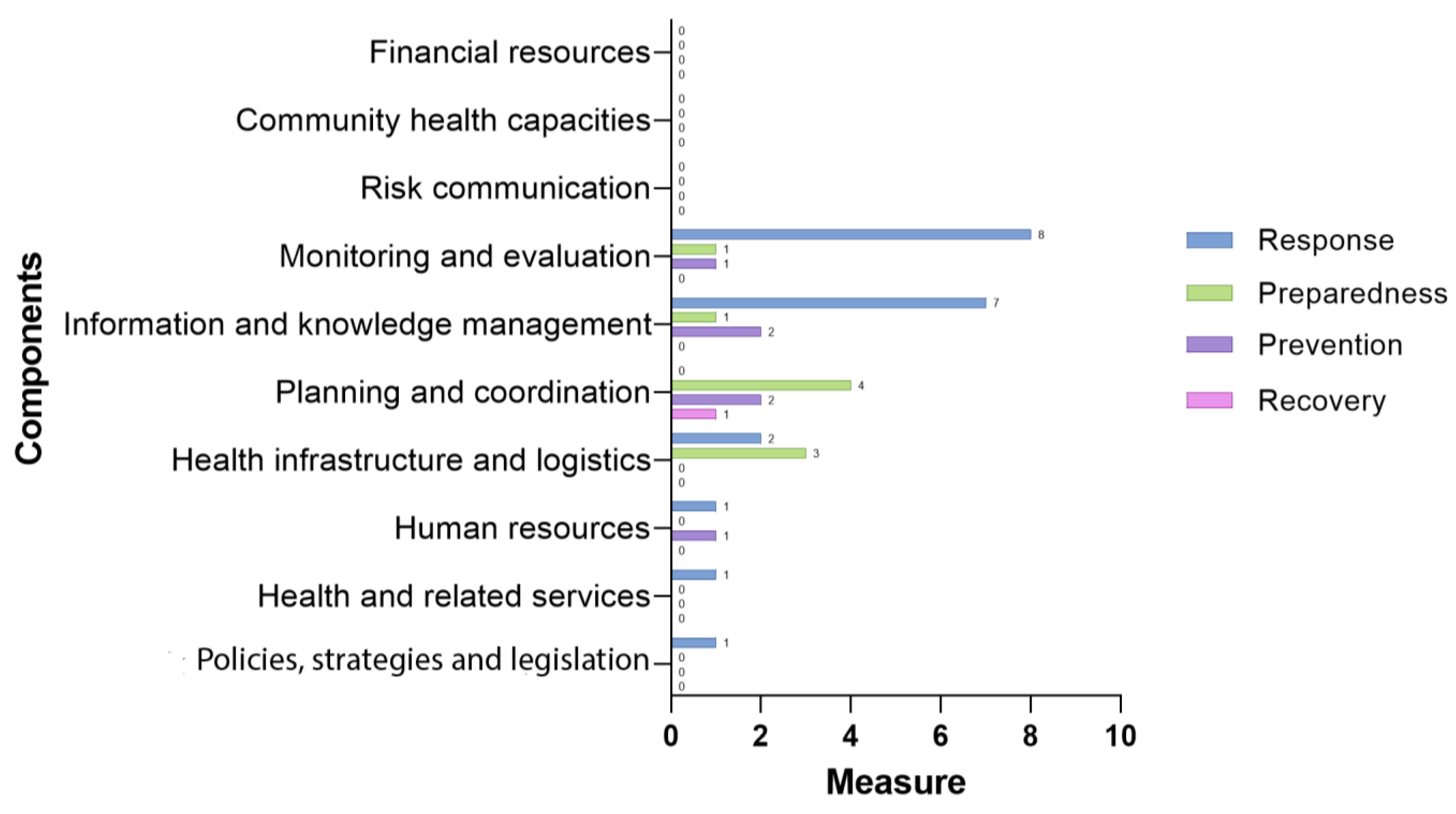
4. Results
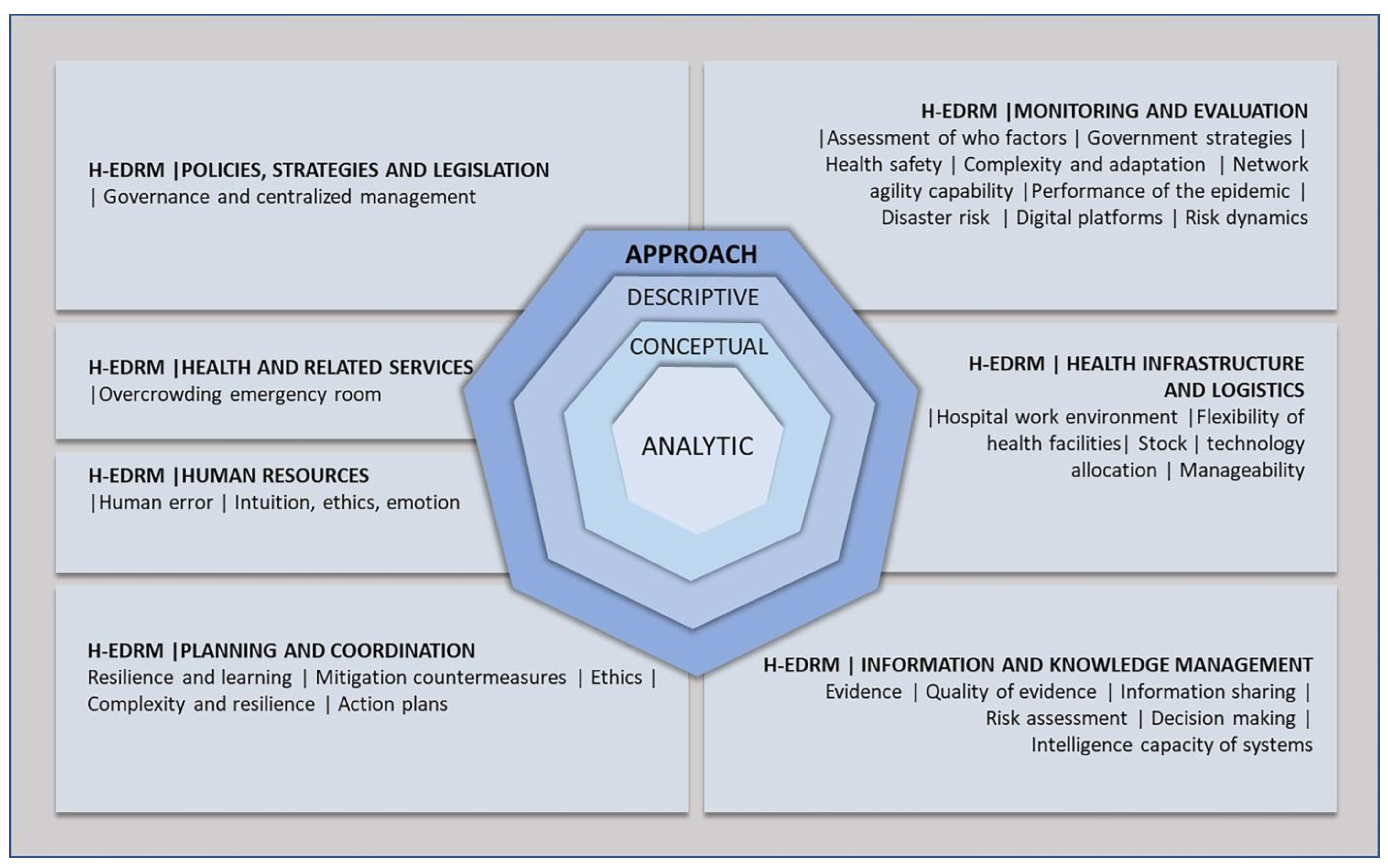
4.1. Frameworks Dynamics: Scope, Intervention, and Gaps
4.1.1. Policies, Strategies, and Legislation | H-EDRM-PSL
4.1.2. Planning and Coordination | H-EDRM-P&C
4.1.3. Human Resources | H-EDRM-HR
4.1.4. Monitoring and Evaluation | H-EDRM-M&E
4.1.5. Information and Knowledge Management | H-EDRM-I&KM
4.1.6. Health Infrastructure and Logistics | H-EDRM-HI&L
4.1.7. Health and Related Services | H-EDRM-H&RS
5. Conclusions
- Adapt the development of frameworks to the country’s governance model, according to its organizational forms, vulnerabilities, and capacities, to mitigate the introduction of models that are disconnected from reality.
- Prioritize ethical aspects in the planning of PHEs in all actions (preparedness, response, prevention, and recovery), with special attention to the most vulnerable populations, incorporating historical data to know the behavior of society in previous events and strengthen the resilience capacity for future emergencies.
- Strengthen policies, strategies, and legislation to prepare the states, prioritizing planning and scenario projection as a conditioning step for response time, improving the effectiveness of interventions and the recovery of health systems.
- Integrate the expectations and hesitations of decision makers at all levels, individual and collective, with frameworks that best interface heuristics and bias and the rationale of context in the face of variables of uncertainty.
- Develop within the framework functions that incorporate community capacity into PHE decision making to produce appropriate responses at all levels and increase the social resilience through collective action to strengthen the capacity of the society to deal with the effects of positive entropy in complex and dynamic PHE contexts.
- Apply methods capable of incorporating the linguistic expressions of the agents, feedback relations, and interdependence among criteria in framework development, making hypotheses and behaviors explicit in the context analysis, due to the uncertainties that compromise the accuracy of predictions.
- Improve evidence sharing and analysis frameworks, with quality analysis and guidance on levels of certainty, to define local strategies aligned to global challenges in PHEs. In this regard, the interoperability of information systems needs to be strengthened.
- Forecast complexity scenarios in all phases of a PHE, continuously confronting the behavior of the health event and the limits of the health services and the supply chain, production, and logistics to develop strategies for allocating strategic inputs to health, including human, cognitive, financial, and technological resources.
- Expand the capacity of the communication frameworks with society, as a strategic action to avoid misinformation and to strengthen sensemaking in society about the interventions.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Health Emergency and Disaster Risk Management Framework. 2019. Available online: https://apps.who.int/iris/handle/10665/326106 (accessed on 17 June 2022).
- Horton, R. Offline: COVID-19 is not a pandemic. Lancet 2020, 396, 10255. [Google Scholar] [CrossRef] [PubMed]
- Kayman, H.; Logar, T. A Framework for Training Public Health Practitioners in Crisis Decision-Making. Disaster Med. Public Health Prep. 2016, 10, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Koonin, L.M.; Pillai, S.; Kahn, E.B.; Moulia, D.; Patel, A. Strategies to Inform Allocation of Stockpiled Ventilators to Healthcare Facilities During a Pandemic. Health Secur. 2020, 18, 69–74. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Hub for Pandemic and Epidemic Intelligence. 2021. Available online: https://cdn.who.int/media/docs/default-source/2021-dha-docs/who_hub.pdf?sfvrsn=8dc28ab6_5 (accessed on 5 May 2022).
- Sterman, J. Business Dynamics: Systems Thinking and Modeling for a Complex World; McGraw-Hill: New York, NY, USA, 2000; Available online: http://www.worldcat.org/title/business-dynamics-systems-thinking-and-modeling-for-a-complex-world/oclc/751006828 (accessed on 17 September 2022).
- Project Management Institute, Inc. Navigating Complexity: A Practice Guide/Project Management Institute; Project Management Institute, Inc.: Newtown, PA, USA, 2014; ISBN 9781628250367. [Google Scholar]
- Neville, K.; O’riordan, S.; Pope, A.; Rauner, M.; Rochford, M.; Madden, M.; Sweeney, J.; Nussbaumer, A.; McCarthy, N.; O’brien, C. Towards the development of a decision support system for multi-agency decision-making during cross-border emergencies. J. Decis. Syst. 2016, 25, 381–396. [Google Scholar] [CrossRef]
- Warsame, A.; Blanchet, K.; Checchi, F. Towards systematic evaluation of epidemic responses during humanitarian crises: A scoping review of existing public health evaluation frameworks. BMJ Glob. Health 2020, 5, e002109. [Google Scholar] [CrossRef] [PubMed]
- Keim, M. Assessing Disaster-Related Health Risk: Appraisal for Prevention. Prehosp. Disaster Med. 2018, 33, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Funk, S.; Camacho, A.; Kucharski, A.J.; Lowe, R.; Eggo, R.M.; Edmunds, W.J. Assessing the performance of real-time epidemic forecasts: A case study of Ebola in the Western Area region of Sierra Leone, 2014–2015. PLoS Comput. Biol. 2019, 15, 2. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Huang, L.; Li, K.; Wang, X.H.; Liu, H.C. An Extended Multi-Attributive Border Approximation Area Comparison Method for Emergency Decision Making with Complex Linguistic Information. Mathematics 2022, 10, 3437. [Google Scholar] [CrossRef]
- Lv, J.; Mao, Q.; Li, Q.; Yu, R. A Group Emergency Decision-Making Method for Epidemic Prevention and Control Based on Probabilistic Hesitant Fuzzy Prospect Set Considering Quality of Information. Int. J. Comput. Intell. Syst. 2022, 15, 33. [Google Scholar] [CrossRef]
- Groot, G.; Baer, S.; Badea, A.; Dalidowicz, M.; Yasinian, M.; Ali, A.; Carr, T.; Reeder, B.; COVID-19 Evidence Support Team (CEST); Azizian, A.R.; et al. Developing a rapid evidence response to COVID-19: The collaborative approach of Saskatchewan, Canada. Learn Health Syst. 2021, 6, e10280. [Google Scholar] [CrossRef]
- Schünemann, H.J.; Santesso, N.; Vist, G.E.; Cuello, C.; Lotfi, T.; Flottorp, S.; Davoli, M.; Mustafa, R.; Meerpohl, J.J.; Alonso-Coello, P.; et al. Using GRADE in situations of emergencies and urgencies: Certainty in evidence and recommendations matters during the COVID-19 pandemic, now more than ever and no matter what. J. Clin. Epidemiol. 2020, 127, 202–207. [Google Scholar] [CrossRef]
- Miglietta, A.; de Waure, C.; Chronaki, C.; Wild, C.; Favaretti, C.; Timen, A.; Edelstein, M.; Petelos, E. Health technology assessment applied to emergency preparedness: A new perspective. Int. J. Technol. Assess. Heal. Care 2021, 37, e77. [Google Scholar] [CrossRef] [PubMed]
- Kapiriri, L.; Essue, B.M.; Bwire, G.; Nouvet, E.; Kiwanuka, S.; Sengooba, F.; Reeleder, D. A framework to support the integration of priority setting in the preparedness, alert, control and evaluation stages of a disease pandemic. Glob. Public Heal. 2021, 17, 1479–1491. [Google Scholar] [CrossRef] [PubMed]
- Jing, Y. Seeking opportunities from crisis? China’s governance responses to the COVID-19 pandemic. Int. Rev. Adm. Sci. 2021, 87, 631–650. [Google Scholar] [CrossRef]
- McDonald, F.; Horwell, C.J.; Wecker, R.; Dominelli, L.; Loh, M.; Kamanyire, R.; Ugarte, C. Facemask use for community protection from air pollution disasters: An ethical overview and framework to guide agency decision making. Int. J. Disaster Risk Reduct. 2020, 43, 101376. [Google Scholar] [CrossRef]
- Khan, Y.; O’sullivan, T.; Brown, A.; Tracey, S.; Gibson, J.; Généreux, M.; Henry, B.; Schwartz, B. Public health emergency preparedness: A framework to promote resilience. BMC Public Health 2018, 18, 1344. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6280369/pdf/12889_2018_Article_6250.pdf (accessed on 6 August 2021). [CrossRef]
- WHO. Environmental Health in Emergencies and Disasters: A Practical Guide. 2002. Available online: https://apps.who.int/iris/bitstream/handle/10665/42561/9241545410_eng.pdf?sequence=1&isAllowed=y (accessed on 7 July 2022).
- Freitas, C.M.; Silva, I.V.D.M.; Alpino, T.D.M. Guia—Preparação Para Resposta à Emergência em Saúde Pública por Inundações Graduais. In Fiocruz, 23rd ed.; ENSP—Fiocruz: Rio de Janeiro, Brazil, 2021; Volume CDD, Available online: https://informe.ensp.fiocruz.br/secoes/noticia/45057/52402 (accessed on 9 July 2023).
- Goode, E.-J.; Thomas, E.; Landeg, O.; Duarte-Davidson, R.; Hall, L.; Roelofs, J.; Schulpen, S.; De Bruin, A.; Wigenstam, E.; Liljedahl, B.; et al. Development of a Rapid Risk and Impact Assessment Tool to Enhance Response to Environmental Emergencies in the Early Stages of a Disaster: A Tool Developed by the European Multiple Environmental Threats Emergency NETwork (EMETNET) Project. Int. J. Disaster Risk Sci. 2021, 12, 528–539. [Google Scholar] [CrossRef]
- DeCS—Descritores em Ciências da Saúde. Available online: https://decs.bvsalud.org/ (accessed on 4 February 2023).
- Winck, G.R.; Raimundo, R.L.G.; Fernandes-Ferreira, H.; Bueno, M.G.; D’andrea, P.S.; Rocha, F.L.; Cruz, G.L.T.; Vilar, E.M.; Brandão, M.; Cordeiro, J.L.P.; et al. Socioecological vulnerability and the risk of zoonotic disease emergence in Brazil. Sci. Adv. 2022, 8, 5774. Available online: https://www.science.org/doi/10.1126/sciadv.abo5774 (accessed on 10 October 2022). [CrossRef]
- Brasil, M.S. Portaria GM/MS no 28, de 20 de Janeiro de 2023. 2023. Available online: https://www.gov.br/saude/pt-br/composicao/svsa/resposta-a-emergencias/coes/coe-yanomami/publicacoes-tecnicas/decretos-e-portarias/portaria-gm-ms-no-28-de-20-de-janeiro-de-2023/view (accessed on 4 February 2023).
- OPAS/OMS. Histórico da Pandemia de COVID-19—OPAS/OMS. Available online: https://www.paho.org/pt/covid19/historico-da-pandemia-covid-19 (accessed on 4 February 2023).
- Legislação Informatizada—DECRETO Nº 10.212, DE 30 DE JANEIRO DE 2020—Publicação Original. Available online: https://www2.camara.leg.br/legin/fed/decret/2020/decreto-10212-30-janeiro-2020-789706-publicacaooriginal-159895-pe.html (accessed on 6 August 2021).
- Ansell, C.; Sørensen, E.; Torfing, J. The COVID-19 pandemic as a game changer for public administration and leadership? The need for robust governance responses to turbulent problems. Public Manag. Rev. 2021, 23, 949–960. [Google Scholar] [CrossRef]
- Spiegel, T.; Caulliraux, H.M. A tomada de decisão diante da racionalidade limitada: Revisão da literatura. Ciências Cognição 2013, 18, 186–207. Available online: http://www.cienciasecognicao.org/revista/index.php/cec/article/view/844 (accessed on 6 August 2021).
- Dresch, A.; Lacerda, D.P.; Antunes, J.A.V., Jr. Design Science Research; Bookman: Porto Alegre, Brasil, 2015; ISBN 9788582605530. [Google Scholar]
- Angeli, F.; Montefusco, A. Sensemaking and learning during the COVID-19 pandemic: A complex adaptive systems perspective on policy decision-making. World Dev. 2020, 136, 105106. [Google Scholar] [CrossRef]
- Creswell, J.D.; Creswell, J.W. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches; Sage Publications: Los Angeles, CA, USA, 2018; ISBN 9781506386706. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Booth, A.; Sutton, A.; Clowes, M.; James, M.M.-S. Systematic Approaches to a Successful Literature Review.; Sage Publications: Thousand Oaks, CA, USA, 2021. [Google Scholar]
- Hou, L.X.; Mao, L.X.; Liu, H.C.; Zhang, L. Decades on emergency decision-making: A bibliometric analysis and literature review. Complex Intell. Syst. 2021, 7, 2819–2832. [Google Scholar] [CrossRef] [PubMed]
- Akabane, G.K. Gestão Estratégica das Tecnologias Cognitivas: Conceitos, Metodologias e Aplicações; Érica: São Paulo, Brasil, 2018; ISBN 9788536527925. [Google Scholar]
- Content—How Scopus Works—Scopus—|Elsevier Solutions. Scopus. 2021. Available online: https://www.elsevier.com/solutions/scopus/how-scopus-works/content (accessed on 1 May 2023).
- Matthews, T. LibGuides: Resources for Librarians: Web of Science Coverage Details. Available online: https://clarivate.libguides.com/librarianresources/coverage (accessed on 1 May 2023).
- Pubmed PubMed. Pubmed. 2021. Available online: https://pubmed.ncbi.nlm.nih.gov/ (accessed on 1 May 2023).
- Carmo, E.H. Emergências de saúde pública: Breve histórico, conceitos e aplicações. Saúde Debate 2020, 44, 9–19. [Google Scholar] [CrossRef]
- Clarivate. Introducing the Journal Citation Indicator. A new Approach to Measure the Citation Impact of Journals in the Web of Science Core Colletion. White Paper. 2021. Available online: https://clarivate.com/wp-content/uploads/dlm_uploads/2021/05/Journal-Citation-Indicator-discussion-paper.pdf (accessed on 27 July 2022).
- Alkan, N.; Kahraman, C. Evaluation of government strategies against COVID-19 pandemic using q-rung orthopair fuzzy TOPSIS method. Appl. Soft Comput. 2021, 110, 107653. [Google Scholar] [CrossRef]
- Dashtpeyma, M.; Ghodsi, R. Humanitarian relief chain agility: Identification and evaluation of enabling factors. Int. J. Emerg. Serv. 2021, 11. [Google Scholar] [CrossRef]
- Hezer, S.; Gelmez, E.; Ozceylan, E.; Özceylan, E. Comparative analysis of TOPSIS, VIKOR and COPRAS methods for the COVID-19 Regional Safety Assessment. J. Infect. Public Health 2021, 14, 775–786. [Google Scholar] [CrossRef]
- Huang, L.; Mao, L.X.; Chen, Y.; Liu, H.C. New method for emergency decision making with an integrated regret theory-EDAS method in 2-tuple spherical linguistic environment. Appl. Intell. 2022, 52, 13296–13309. [Google Scholar] [CrossRef]
- Labib, A. Towards a new approach for managing pandemics: Hybrid resilience and bowtie modelling. Saf. Sci. 2021, 139, 105274. [Google Scholar] [CrossRef]
- Moheimani, A.; Sheikh, R.; Hosseini, S.M.H.; Sana, S.S. Assessing the agility of hospitals in disaster management: Application of interval type-2 fuzzy Flowsort inference system. Soft Comput. 2021, 25, 3955–3974. [Google Scholar] [CrossRef]
- Onar, S.C.; Kahraman, C.; Oztaysi, B. Multi-criteria spherical fuzzy regret based evaluation of healthcare equipment stocks. J. Intell. Fuzzy Syst. 2020, 39, 5987–5997. [Google Scholar] [CrossRef]
- Pegoraro, F.; Santos, E.A.P.; Loures, E.D.F.R.; Laus, F.W. A hybrid model to support decision making in emergency department management. Knowl.-Based Syst. 2020, 203, 106148. [Google Scholar] [CrossRef]
- Rathore, B.; Gupta, R. A fuzzy based hybrid decision-making framework to examine the safety risk factors of healthcare workers during COVID-19 outbreak. J. Decis. Syst. 2020, 31, 68–101. [Google Scholar] [CrossRef]
- Raveendran, A.; Renjith, V.R.; Madhu, G. A comprehensive review on dynamic risk analysis methodologies. J. Loss Prev. Process. Ind. 2022, 76, 104734. [Google Scholar] [CrossRef]
- Strong, P.; Shenvi, A.; Yu, X.; Papamichail, K.N.; Wynn, H.P.; Smith, J.Q. Building a Bayesian decision support system for evaluating COVID-19 countermeasure strategies. J. Oper. Res. Soc. 2021, 74, 476–488. [Google Scholar] [CrossRef]
- Yang, Y.; Guo, Z. Evaluation of Emergency Intelligence Capability of Major Public. Comput. Intell. Neurosci. 2022, 2022, 1302598. [Google Scholar]
- Deng, Q.; Xiao, X.; Zhu, L.; Cao, X.; Liu, K.; Zhang, H.; Huang, L.; Yu, F.; Jiang, H.; Liu, Y. A national risk analysis model (NRAM) for the assessment of COVID-19 epidemic. Risk Anal. 2023; online ahead of print. [Google Scholar] [CrossRef]
- Pan, L.; Su, Y.; Yan, H.; Zhang, R. Assessment Model for Rapid Suppression of SARS-CoV-2 Transmission under Government Control. Trop. Med. Infect. Dis. 2022, 7, 399. [Google Scholar] [CrossRef]
- Wang, H. Grey Multiattribute Emergency Decision-Making Method for Public Health Emergencies Based on Cumulative Prospect Theory. Math Probl. Eng. 2022, 2022, 3240483. [Google Scholar] [CrossRef]
- Asadi, S.; Nilashi, M.; Abumalloh, R.A.; Samad, S.; Ahani, A.; Ghabban, F.; Yusuf, S.Y.M.; Supriyanto, E. Evaluation of Factors to Respond to the COVID-19 Pandemic Using DEMATEL and Fuzzy Rule-Based Techniques. Int. J. Fuzzy Syst. 2022, 24, 27–43. [Google Scholar] [CrossRef]
- Gossip, K.; Gouda, H.; Lee, Y.Y.; Firth, S.; Bermejo, R., III; Zeck, W.; Soto, E.J. Monitoring and evaluation of disaster response efforts undertaken by local health departments: A rapid realist review. BMC Health Serv. Res. 2017, 17, 450. [Google Scholar] [CrossRef] [PubMed]
- Bickley, S.J.; Torgler, B. A systematic approach to public health—Novel application of the human factors analysis and classification system to public health and COVID-19. Saf. Sci. 2021, 140, 105312. [Google Scholar] [CrossRef] [PubMed]
- Gomes, L.F.A.M.; Simões, C.F.; Gomes, P. Princípios e Métodos para Tomada de Decisão Enfoque Multicritério, 6th ed.; Editora Atlas Ltda: São Paulo, Brazil, 2019; ISBN 9788597021585. [Google Scholar]
- Brambilla, A.; Sun, T.-Z.; Elshazly, W.; Ghazy, A.; Barach, P.; Lindahl, G.; Capolongo, S. Flexibility during the COVID-19 Pandemic Response: Healthcare Facility Assessment Tools for Resilient Evaluation. Int. J. Env. Res. Public Health 2021, 18, 11478. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Year | JCI | Selected Studies—Title | H-EDRM | PPRR Mode | Subject |
|---|---|---|---|---|---|---|
| (Shi et al., 2022) | 2022 | 2.15 | An extended multi-attributive border approximation area comparison method for emergency decision making with complex linguistic information | H-EDRM-I&KM | Response | Decision-making method |
| (Schünemann et al., 2020) | 2020 | 1.69 | Using GRADE in situations of emergencies and urgencies: certainty in evidence and recommendations matters during the COVID-19 pandemic, now more than ever and no matter what | H-EDRM-I&KM | Response | Quality of evidence |
| (Warsame et al., 2020) | 2020 | 1.58 | Towards systematic evaluation of epidemic responses during humanitarian crises: a scoping review of existing public health evaluation frameworks | H-EDRM-M&E | Response | Adaptive approach to epidemic intervention cycle |
| (Alkan & Kahraman, 2021) | 2021 | 1.57 | Evaluation of government strategies against COVID-19 pandemic using q-rung orthopair fuzzy TOPSIS method | H-EDRM-M&E | Response | Government strategies |
| (Pegoraro et al., 2020) | 2020 | 1.56 | A hybrid model to support decision making in emergency department management | H-EDRM-H&RS | Response | Reduction of overcrowding |
| (Hezer et al., 2021) | 2021 | 1.3 | Comparative analysis of TOPSIS, VIKOR and COPRAS methods for the COVID-19 Regional Safety Assessment | H-EDRM-M&E | Response | Assessing health security |
| (Deng et al., 2023) | 2023 | 1.29 | A national risk analysis model (NRAM) for the assessment of COVID-19 epidemic | H-EDRM-I&KM | Prevention | Risk analysis |
| (Bickley & Torgler, 2021) | 2021 | 1.16 | A systematic approach to public health-Novel application of the human factors analysis and classification system to public health and COVID-19 | H-EDRM-HR | Prevention | Human error |
| (Labib, 2021) | 2021 | 1.16 | Towards a new approach for managing pandemics: Hybrid resilience and bowtie modelling | H-EDRM-P&C | Recovery | Resilience |
| (McDonald et al., 2020) | 2020 | 1.11 | Facemask use for community protection from air pollution disasters: An ethical overview and framework to guide agency decision making | H-EDRM-P&C | Prevention | Ethical values |
| (Funk et al., 2019) | 2019 | 1.11 | Assessing the performance of real-time epidemic forecasts: A case study of Ebola in the Western Area region of Sierra Leone, 2014–2015 | H-EDRM-M&E | Response | Evaluating performance of an epidemic |
| (Jing, 2021) | 2021 | 1.05 | Seeking opportunities from crisis? China’s governance responses to the COVID-19 pandemic | H-EDRM-PSL | Response | Government strategies |
| (Khan et al., 2018) | 2018 | 1.02 | Public health emergency preparedness: a framework to promote resilience | H-EDRM-P&C | Preparedness | Resilience |
| (Asadi et al., 2022) | 2022 | 1.01 | Evaluation of Factors to Respond to the COVID-19 Pandemic Using DEMATEL and Fuzzy Rule-Based Techniques | H-EDRM-M&E | Response | Assessment of the WHO guiding factors |
| (Goode et al., 2021) | 2021 | 1 | Development of a Rapid Risk and Impact Assessment Tool to Enhance Response to Environmental Emergencies in the Early Stages of a Disaster: A Tool Developed by the European Multiple Environmental Threats Emergency NETwork (EMETNET) Project | H-EDRM-I&KM | Response | Risk assessing |
| (Huang et al., 2022) | 2022 | 0.93 | New method for emergency decision making with an integrated regret theory-EDAS method in 2-tuple spherical linguistic environment | H-EDRM-I&KM | Response | Decision-making method |
| (Brambilla et al., 2021) | 2021 | 0.93 | Flexibility during the COVID-19 Pandemic Response: Healthcare Facility Assessment Tools for Resilient Evaluation | H-EDRM-HI&L | Preparedness | Health facilities—hospitals |
| (Keim, 2018) | 2018 | 0.89 | Assessing Disaster-Related Health Risk: Appraisal for Prevention | H-EDRM-M&E | Prevention | Assessing disaster-related health risk |
| (Groot et al., 2021) | 2021 | 0.88 | Developing a rapid evidence response to COVID-19: The collaborative approach of Saskatchewan, Canada | H-EDRM-I&KM | Response | Producing evidence |
| (Gossip et al., 2017) | 2017 | 0.83 | Monitoring and evaluation of disaster response efforts undertaken by local health departments: a rapid realist review | H-EDRM-M&E | Response | Monitoring and evaluating the disaster cycle |
| (Kapiriri et al., 2021) | 2021 | 0.82 | A framework to support the integration of priority setting in the preparedness, alert, control and evaluation stages of a disease pandemic | H-EDRM-P&C | Preparedness | Action Plan |
| (Kayman & Logar, 2016) | 2016 | 0.81 | A Framework for Training Public Health Practitioners in Crisis Decision-Making | H-EDRM-HR | Response | Learning for decision making |
| (Moheimani et al., 2021) | 2021 | 0.8 | Assessing the agility of hospitals in disaster management: application of interval type-2 fuzzy Flowsort inference system | H-EDRM-HI&L | Preparedness | Classifying hospitals by level of agility |
| (Yang & Guo, 2022) | 2022 | 0.73 | Evaluation of Emergency Intelligence Capability of Major Public Health Events in Probabilistic Uncertain Language Environment | H-EDRM-I&KM | Preparedness | Emergency intelligence systems |
| (Pan et al., 2022) | 2022 | 0.67 | Assessment model for rapid suppression of SARS-CoV-2 transmission under government control | H-EDRM-M&E | Response | Government strategies |
| (Strong et al., 2021) | 2021 | 0.67 | Building a Bayesian decision support system for evaluating COVID-19 countermeasure strategies | H-EDRM-P&C | Prevention | Countermeasure strategies |
| (Koonin et al., 2020) | 2020 | 0.66 | Strategies to Inform Allocation of Stockpiled Ventilators to Healthcare Facilities During a Pandemic | H-EDRM-HI&L | Response | Allocation of technology |
| (Raveendran et al., 2022) | 2022 | 0.59 | A comprehensive review on dynamic risk analysis methodologies | H-EDRM-M&E | Preparedness | Dynamic risk analysis |
| (Miglietta et al., 2021) | 2021 | 0.48 | Health technology assessment applied to emergency preparedness: a new perspective | H-EDRM-P&C | Preparedness | Action Plan |
| (Lv et al., 2022) | 2022 | 0.43 | A group emergency decision-making method for epidemic prevention and control based on probabilistic hesitant fuzzy prospect set considering quality of information | H-EDRM-I&KM | Prevention | Group decision-making method |
| (Wang, 2022) | 2022 | 0.42 | Grey multiattribute emergency decision-making method for public health emergencies based on cumulative prospect theory | H-EDRM-I&KM | Response | Decision-making method |
| (Dashtpeyma & Ghodsi, 2021) | 2021 | 0.42 | Humanitarian relief chain agility: identification and evaluation of enabling factors | H-EDRM-M&E | Response | Agility capacity of humanitarian aid network |
| (Onar et al., 2020) | 2020 | 0.32 | Multi-criteria spherical fuzzy regret-based evaluation of healthcare equipment stocks | H-EDRM-HI&L | Preparedness | Stock levels of health systems in emergency |
| (Rathore & Gupta, 2022) | 2022 | 0.3 | A fuzzy based hybrid decision-making framework to examine the safety risk factors of healthcare workers during COVID-19 outbreak | H-EDRM-HI&L | Response | Safety risk factors in hospital |
| (Neville et al., 2016) | 2016 | 0.29 | Towards the development of a decision support system for multi-agency decision-making during cross-border emergencies | H-EDRM-I&KM | Response | Sharing critical information |
| (WHO, 2019) | 2019 | NI | Health Emergency and Disaster Risk Management Framework | H-EDRM-P&C | Preparedness | WHO strategies |
| Authors | Year | JCI | H-EDRM | PPRR Mode | Multicriteria Method | Application in the Evaluated Study |
|---|---|---|---|---|---|---|
| (Shi et al., 2022) | 2022 | 2.15 | H-EDRM-I&KM | Response | Composition: DHHLTSs, MABAC | Incorporate the decision maker’s uncertain information into the evaluation of alternatives, weighting of choice criteria, and ranking of solutions. |
| (Alkan & Kahraman, 2021) | 2021 | 1.57 | H-EDRM-M&E | Response | TOPSIS q-rung orthopair fuzzy method. | Establish alternatives in extended contexts, with a lack of information, and ambiguities, uncertainties, and dissensions among experts. |
| (Pegoraro et al., 2020) | 2020 | 1.56 | H-EDRM-H&RS | Response | Composition: DEMATEL, PROMETHEE II | Address feedback relationships, interdependence, and influences among criteria. |
| (Hezer et al., 2021) | 2021 | 1.3 | H-EDRM-M&E | Response | Comparison: TOPSIS, VIKOR, COPRAS | Ranking alternatives according to the distances between positive and negative ideal solutions (TOPSIS). Sort and select alternatives with conflicting criteria (VIKOR). Ranking alternatives according to importance and utility (COPRAS). |
| (Deng et al., 2023) | 2023 | 1.29 | H-EDRM-I&KM | Prevention | Composition: Bayesian Network (BN), ISM, K2 algorithm. | Establish networks with expert knowledge and case study data from context. Identify network factors and parameters for scenario production and sensitivity analysis. |
| (Labib, 2021) | 2021 | 1.16 | H-EDRM-P&C | Recovery | Resilience modeling and bowtie modeling. | Analyze the interaction between a temporal and causal axis. |
| (Asadi et al., 2022) | 2022 | 1.01 | H-EDRM-M&E | Response | Composition: DEMATEL, Fuzzy | Identify causal relationships between critical factors and elements that impact virus infection. |
| (Huang et al., 2022) | 2022 | 0.93 | H-EDRM-I&KM | Response | Composition: 2-Tuple spherical linguistic term set, CRITIC, EDAS | Address expressions of uncertainty by decision makers, rank alternatives, and establish criteria weights for an optimal solution. |
| (Moheimani et al., 2021) | 2021 | 0.8 | H-EDRM-HI&L | Preparedness | Composition: Literature review; Flowsort with IT2FSs | Incorporate agility factors and linguistic expressions into the analysis. Establish alternatives based on sorted criteria and categories. |
| (Yang & Guo, 2022) | 2022 | 0.73 | H-EDRM-I&KM | Preparedness | Composition: PULTS, VIKOR | Assess intelligence capability in PHE, uncertain probabilistic language environments. |
| (Strong et al., 2021) | 2021 | 0.67 | H-EDRM-P&C | Revention | Bayesian networks | Address uncertainty in dynamic environments in the transition from short term to long term. |
| (Raveendran et al., 2022) | 2022 | 0.59 | H-EDRM-M&E | Preparedness | Dynamic risk analysis (DRA) | Identify the dynamics of risk. |
| (Lv et al., 2022) | 2022 | 0.43 | H-EDRM-I&KM | Prevention | Fuzzy (PHFS). Cumulative Prospect Theory (CPT) | Analyze probabilities of performance of the decision object, integrating decision makers’ choices in a risk context. |
| (Wang, 2022) | 2022 | 0.42 | H-EDRM-I&KM | Response | Application of the Cumulative Prospect Theory (TCP). | Weighting functions in contexts of uncertainty and risk for decision gains and losses. Establish the possibility of values for a range or set of variables, rather than exact values. |
| (Dashtpeyma & Ghodsi, 2021) | 2021 | 0.42 | H-EDRM-M&E | Response | Composition: DEMATEL, ANP. | Evaluate interactions between elements and establish consistency ratings. |
| (Onar et al., 2020) | 2020 | 0.32 | H-EDRM-HI&L | Preparedness | Multicriteria spherical fuzzy regret. | Represent the level of hesitation or adherence of decision makers to listed alternatives. |
| (Rathore & Gupta, 2022) | 2022 | 0.3 | H-EDRM-HI&L | Response | Composition: Fuzzy FDM, FAHP, FTOPSIS. | Identify risk factors. Calculate and rank weights of categories and factors according to their importance. Classify hospitals. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Príncipe, A.S.; Filho, A.S.N.; Machado, B.A.S.; Barbosa, J.D.V.; Winkler, I.; Ferreira, C.V. Decision Support Frameworks in Public Health Emergencies: A Systematic Review of Dynamic Models in Complex Contexts. Int. J. Environ. Res. Public Health 2023, 20, 6685. https://doi.org/10.3390/ijerph20176685
Príncipe AS, Filho ASN, Machado BAS, Barbosa JDV, Winkler I, Ferreira CV. Decision Support Frameworks in Public Health Emergencies: A Systematic Review of Dynamic Models in Complex Contexts. International Journal of Environmental Research and Public Health. 2023; 20(17):6685. https://doi.org/10.3390/ijerph20176685
Chicago/Turabian StylePríncipe, Alex S., Aloísio S. N. Filho, Bruna A. S. Machado, Josiane D. V. Barbosa, Ingrid Winkler, and Cristiano V. Ferreira. 2023. "Decision Support Frameworks in Public Health Emergencies: A Systematic Review of Dynamic Models in Complex Contexts" International Journal of Environmental Research and Public Health 20, no. 17: 6685. https://doi.org/10.3390/ijerph20176685
APA StylePríncipe, A. S., Filho, A. S. N., Machado, B. A. S., Barbosa, J. D. V., Winkler, I., & Ferreira, C. V. (2023). Decision Support Frameworks in Public Health Emergencies: A Systematic Review of Dynamic Models in Complex Contexts. International Journal of Environmental Research and Public Health, 20(17), 6685. https://doi.org/10.3390/ijerph20176685