
Situation Analysis of a New Effort of Community-Based Health Planning and Services (CHPS) for Maternal Health in Upper West Region in Rural Ghana

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Study Design
2.3. Sample Size
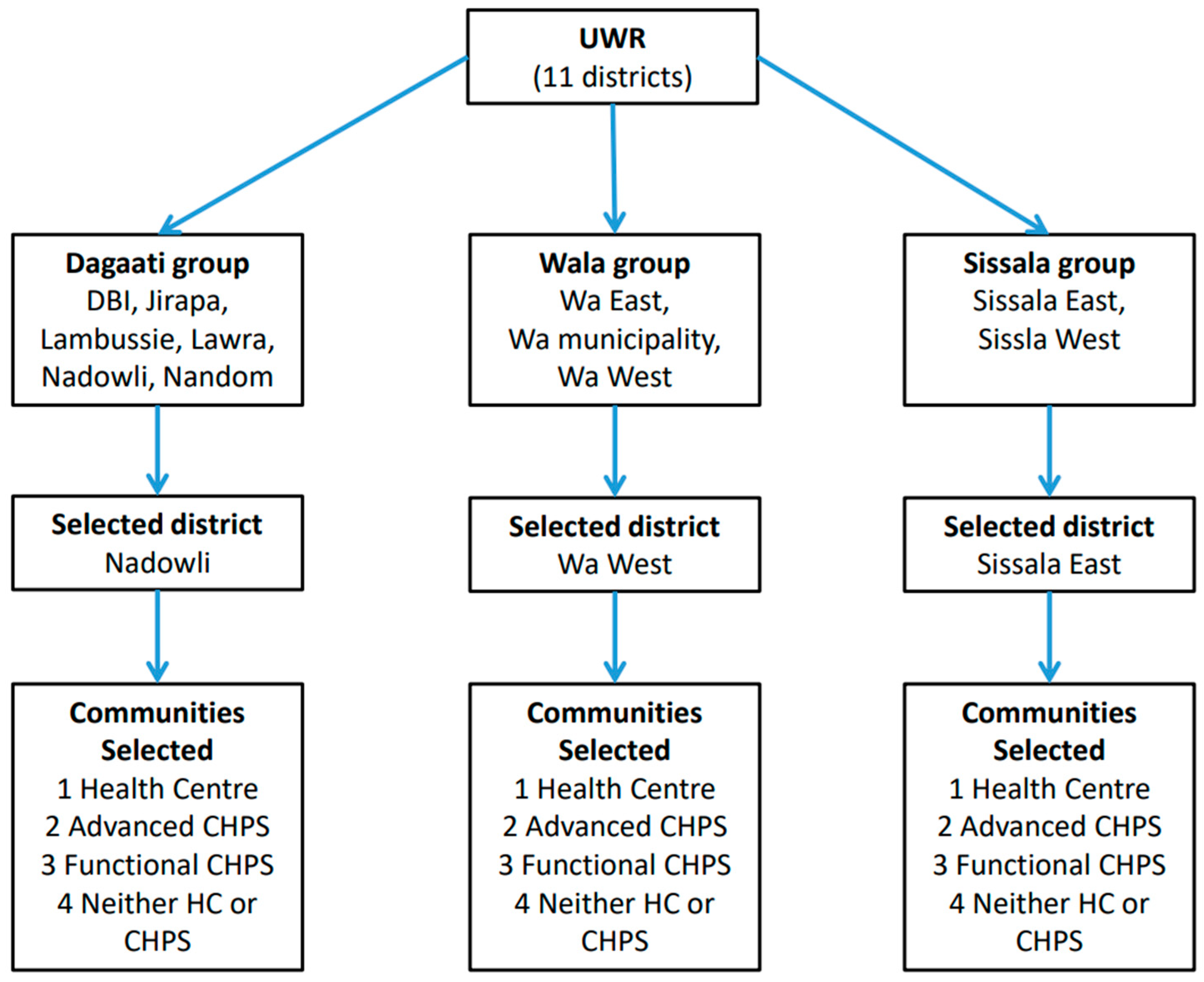
2.4. Sampling and Data Collection
2.5. Data Processing and Analysis
2.6. Ethical Consideration
3. Results
3.1. Background Characteristics of Respondents
3.2. Choice of Place of Childbirth
3.3. Cost of Childbirth
3.4. Catastrophic Payment
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization; UNICEF. United Nations Population Fund and The World Bank, Trends in Maternal Mortality: 2000 to 2020; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- WHO. Maternal Mortality. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/maternal-mortality (accessed on 15 August 2023).
- Azaare, J.; Akweongo, P.; Aryeetey, G.C.; Dwomoh, D. Impact of free maternal health care policy on maternal health care utilization and perinatal mortality in Ghana: Protocol design for historical cohort study. Reprod. Health 2020, 17, 169. [Google Scholar] [CrossRef] [PubMed]
- Meda, I.B.; Baguiya, A.; Ridde, V.; Ouédraogo, H.G.; Dumont, A.; Kouanda, S. Out-of-pocket payments in the context of a free maternal health care policy in Burkina Faso: A national cross-sectional survey. Health Econ. Rev. 2019, 9, 11. [Google Scholar] [CrossRef] [PubMed]
- Twum, P.; Qi, J.; Aurelie, K.K.; Xu, L. Effectiveness of a free maternal healthcare programme under the National Health Insurance Scheme on skilled care: Evidence from a cross-sectional study in two districts in Ghana. BMJ Open 2018, 8, e022614. [Google Scholar] [CrossRef] [PubMed]
- Dalaba, M.A.; Welaga, P.; Immurana, M.; Ayanore, M.; Ane, J.; Danchaka, L.L.; Matsubara, C. Cost of childbirth in Upper West Region of Ghana: A cross-sectional study. BMC Pregnancy Childbirth 2022, 22, 613. [Google Scholar] [CrossRef] [PubMed]
- WHO; UNICEF; UNFPA; World Bank Group; United Nations Population Division. Trends in Maternal Mortality: 2000 to 2017; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Ghana Statistical Service (GSS); Ghana Health Service (GHS); ICF. Ghana Maternal Health Survey 2017; GSS: Accra, Ghana; GHS: Accra, Ghana; ICF: Rockville, MD, USA, 2018. [Google Scholar]
- Ghana Health Service, Community-Based Health Planning and Services (CHPS) the Operational Policy, Ghana Health Service Policy Document No.20, Accra. 2005. Available online: https://www.moh.gov.gh/wp-content/uploads/2016/02/CHPS-Operational-Policy-2005.pdf (accessed on 15 August 2023).
- Awoonor-Williams, J.K.; Sory, E.K.; Nyonator, F.K.; Phillips, J.F.; Wang, C.; Schmitt, M.L. Lessons learned from scaling up a community-based health program in the Upper East Region of northern Ghana. Glob. Health Sci. Pract. 2013, 1, 117–133. [Google Scholar] [CrossRef] [PubMed]
- Kweku, M.; Amu, H.; Awolu, A.; Adjuik, M.; Ayanore, M.A.; Manu, E.; Tarkang, E.E.; Komesuor, J.; Asalu, G.A.; Aku, F.Y.; et al. Community-Based Health Planning and Services Plus programme in Ghana: A qualitative study with stakeholders in two Systems Learning Districts on improving the implementation of primary health care. PLoS ONE 2020, 15, e0226808. [Google Scholar] [CrossRef] [PubMed]
- CHW Central. Ghana Community Health Officers and Community Health Volunteers. Available online: https://chwcentral.org/ghanas-community-health-officers-and-community-health-volunteers/ (accessed on 15 August 2023).
- Dalaba, M.A.; Akweongo, P.; Savadogo, G.; Saronga, H.; Williams, J.; Sauerborn, R.; Dong, H.; Loukanova, S. Cost of maternal health services in selected primary care centres in Ghana: A step down allocation approach. BMC Health Serv. Res. 2013, 13, 287. [Google Scholar] [CrossRef] [PubMed]
- Dalaba, M.A.; Welaga, P.; Oduro, A.; Danchaka, L.L.; Matsubara, C. Cost of malaria treatment and health seeking behaviour of children under-five years in the Upper West Region of Ghana. PLoS ONE 2018, 13, e0195533. [Google Scholar] [CrossRef] [PubMed]
- Dalinjong, P.A.; Wang, A.Y.; Homer, C.S.E. The implementation of the free maternal health policy in rural Northern Ghana: Synthesised results and lessons learnt. BMC Res. Notes 2018, 11, 341. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Food and Agriculture, Ghana, Upper West Region. Accra. 2023. Available online: https://mofa.gov.gh/site/directorates/regional-directorates/upper-west-region#:~:text=The%20southern%20part%20of%20the,annual%20evaporation%20exceeding%20annual%20precipitation (accessed on 15 August 2023).
- Ghana Statistical Service (GSS); Ghana Health Service (GHS); ICF International. Ghana Demographic and Health Survey 2014; GSS: Accra, Ghana; GHS: Accra, Ghana; ICF International: Rockville, MD, USA, 2015. [Google Scholar]
- Dalaba, M.A.; Akweongo, P.; Aborigo, R.A.; Saronga, H.P.; Williams, J.; Aninanya, G.A.; Sauerborn, R.; Loukanova, S. Cost to households in treating maternal complications in northern Ghana: A cross sectional study. BMC Health Serv. Res. 2015, 15, 34. [Google Scholar] [CrossRef] [PubMed]
- Kpodotsi, A.; Baku, E.A.; Adams, J.H.; Alaba, O. Socioeconomic inequalities in access and use of skilled birth attendants during childbirth in Ghana: A decomposition analysis. BMC Pregnancy Childbirth 2021, 21, 850. [Google Scholar] [CrossRef] [PubMed]
- Sumankuuro, J.; Crockett, J.; Wang, S. Maternal Health Care Initiatives: Causes of Morbidities and Mortalities in Two Rural Districts of Upper West Region, Ghana. PLoS ONE 2017, 12, e0183644. [Google Scholar] [CrossRef] [PubMed]
- Dalinjong, P.A.; Wang, A.Y.; Homer, C.S.E. Has the free maternal health policy eliminated out of pocket payments for maternal health services? Views of women, health providers and insurance managers in Northern Ghana. PLoS ONE 2018, 13, e0184830. [Google Scholar] [CrossRef] [PubMed]
- Amiri, M.M.; Teymourzadeh, E.; Ravangard, R.; Bahadori, M. Health Informal Payments and Their Main Determinants: The Case of Iran. Proc. Singap. Healthc. 2019, 0, 2010105818822594. [Google Scholar] [CrossRef]
- Akazili, J.; McIntyre, D.; Kanmiki, E.W.; Gyapong, J.; Oduro, A.; Sankoh, O.; Ataguba, J.E. Assessing the catastrophic effects of out-of-pocket healthcare payments prior to the uptake of a nationwide health insurance scheme in Ghana. Glob. Health Action 2017, 10, 1289735. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Ahmed, M.W.; Hasan, Z.; Mehdi, G.G.; Islam, Z.; Rehnberg, C.; Niessen, L.W.; Khan, J.A.M. Assessing the incidence of catastrophic health expenditure and impoverishment from out-of-pocket payments and their determinants in Bangladesh: Evidence from the nationwide Household Income and Expenditure Survey 2016. Int. Health 2022, 14, 84–96. [Google Scholar] [CrossRef] [PubMed]
- Bank of Ghana. Ghanaian Cedi (GHS) to United States Dollar (USD) on 5 October 2018 Exchange Rates—FX Exchange Rate; Bank of Ghana: Accra, Ghana, 2018. [Google Scholar]
- Kweku, M.; Amu, H.; Adjuik, M.; Aku, F.Y.; Manu, E.; Tarkang, E.E.; Komesuor, J.; Asalu, G.A.; Amuna, N.N.; Boateng, L.A.; et al. Community utilisation and satisfaction with the community-based health planning and services initiative in Ghana: A comparative study in two system learning districts of the CHPS+ project. BMC Health Serv. Res. 2020, 20, 845. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Number | % |
|---|---|---|
| Age Group | ||
| 15–19 | 18 | 3.4 |
| 20–34 | 416 | 77.9 |
| 35+ | 100 | 18.7 |
| Ethnicity | ||
| Wala | 96 | 18.0 |
| Sissala | 170 | 31.8 |
| Dagaati | 242 | 45.3 |
| Other | 26 | 4.9 |
| Education | ||
| Never been to school | 324 | 60.8 |
| Primary school | 104 | 19.5 |
| Junior high | 74 | 13.9 |
| Senior high | 28 | 5.3 |
| University/College | 3 | 0.6 |
| Occupation | ||
| Farmer | 427 | 80.0 |
| Industrial worker | 2 | 0.4 |
| Home industry | 52 | 9.7 |
| Market vender | 25 | 4.7 |
| NGO/Private employee | 2 | 0.4 |
| Shop/Restaurant | 4 | 0.8 |
| Civil servant | 2 | 0.4 |
| No income | 16 | 3.0 |
| Student | 4 | 0.8 |
| NHIS status of respondents | ||
| Yes | 449 | 85.2 |
| No | 78 | 14.8 |
| Household annual income | ||
| Median (IQR) | GHS 1176 | (350–3168) |
| Frequency | % | ||
|---|---|---|---|
| Near Health Centre (n = 160) | Home (No visit) | 28 | 17.5 |
| CHPS | 16 | 10.0 | |
| Health Centre | 99 | 61.9 | |
| District Hospital | 7 | 4.4 | |
| Others | 10 | 6.3 | |
| Near Advanced CHPS (n = 131) | Home (No visit) | 26 | 19.9 |
| CHPS | 64 | 48.9 | |
| Health Centre | 12 | 9.2 | |
| District Hospital | 19 | 14.5 | |
| Others | 10 | 7.6 | |
| Near Functional CHPS (n = 104) | Home (No visit) | 15 | 14.4 |
| CHPS | 44 | 42.3 | |
| Health Centre | 30 | 28.9 | |
| District Hospital | 10 | 9.6 | |
| Others | 5 | 4.8 | |
| Neither Health Center Nor CHPS (n = 139) | Home (No visit) | 21 | 15.1 |
| CHPS | 16 | 11.5 | |
| Health Centre | 52 | 37.4 | |
| District Hospital | 38 | 27.3 | |
| Others | 2 | 1.4 | |
| CHPS: Community-based Health Planning and Services | |||
| Proper place | |||
| Crossing | |||
| Unproper place | |||
| Number That Paid (%) | Average Cost (SD) | Minimum Cost (GHS) | Maximum Cost (GHS) | ||
|---|---|---|---|---|---|
| Near Health Centre (n = 160) | Medical cost | 68 (42.5) | 15.3 (17.8) | 1 | 85 |
| Non-medical cost | 89 (55.6) | 20.8 (53.3) | 1 | 500 | |
| Total | 114 (71.3) | 25.4 (48.6) | 1 | 502 | |
| Near Advanced CHPS (n = 131) | Medical cost | 39 (29.8) | 28.8 (38.8) | 2 | 220 |
| Non-medical cost | 63 (48.1) | 21.2 (27.9) | 2 | 150 | |
| Total | 76 (58.0) | 32.3 (39.9) | 2 | 230 | |
| Near Functional CHPS (n = 104) | Medical cost | 28 (26.9) | 25.2 (25.5) | 1 | 100 |
| Non-medical cost | 68 (48.1) | 22.2 (18.2) | 2 | 73 | |
| Total | 72 (69.2) | 30.8 (18.2) | 1 | 140 | |
| Neither Health Center Nor CHPS (n = 139) | Medical cost | 51 (36.7) | 20.9 (27.9) | 1 | 120 |
| Non-medical cost | 100 (71.9) | 21.2 (33.7) | 2 | 224 | |
| Total | 105 (75.5) | 30.3 (41.7) | 3 | 254 |
| Residential Area | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Health Centre | Advanced CHPS | Functional CHPS | Neither Health Centre or CHPS | ||||||
| Freq. | % | Freq. | % | Freq. | % | Freq. | % | ||
| Catastrophic payment | Yes | 20 | 14.0 | 6 | 5.0 | 16 | 18.8 | 22 | 19.1 |
| No | 123 | 6.0 | 115 | 95.0 | 69 | 81.2 | 93 | 80.9 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsubara, C.; Dalaba, M.A.; Danchaka, L.L.; Welaga, P. Situation Analysis of a New Effort of Community-Based Health Planning and Services (CHPS) for Maternal Health in Upper West Region in Rural Ghana. Int. J. Environ. Res. Public Health 2023, 20, 6595. https://doi.org/10.3390/ijerph20166595
Matsubara C, Dalaba MA, Danchaka LL, Welaga P. Situation Analysis of a New Effort of Community-Based Health Planning and Services (CHPS) for Maternal Health in Upper West Region in Rural Ghana. International Journal of Environmental Research and Public Health. 2023; 20(16):6595. https://doi.org/10.3390/ijerph20166595
Chicago/Turabian StyleMatsubara, Chieko, Maxwell Ayindenaba Dalaba, Laata Latif Danchaka, and Paul Welaga. 2023. "Situation Analysis of a New Effort of Community-Based Health Planning and Services (CHPS) for Maternal Health in Upper West Region in Rural Ghana" International Journal of Environmental Research and Public Health 20, no. 16: 6595. https://doi.org/10.3390/ijerph20166595
APA StyleMatsubara, C., Dalaba, M. A., Danchaka, L. L., & Welaga, P. (2023). Situation Analysis of a New Effort of Community-Based Health Planning and Services (CHPS) for Maternal Health in Upper West Region in Rural Ghana. International Journal of Environmental Research and Public Health, 20(16), 6595. https://doi.org/10.3390/ijerph20166595