
Assessing the Efficacy of a Brief Universal Family Skills Programme on Violence and Substance-Use Indicators in Youth in Trentino and Parma, Italy: Study Protocol for a Multi-Centre, Non-Blinded, Cluster-Randomised Controlled Trial (cRCT) of Family UNited

 ,
, 
Abstract
1. Introduction
1.1. Background and Rationale
1.2. The Role of the Family in Violence and Substance-Use Prevention
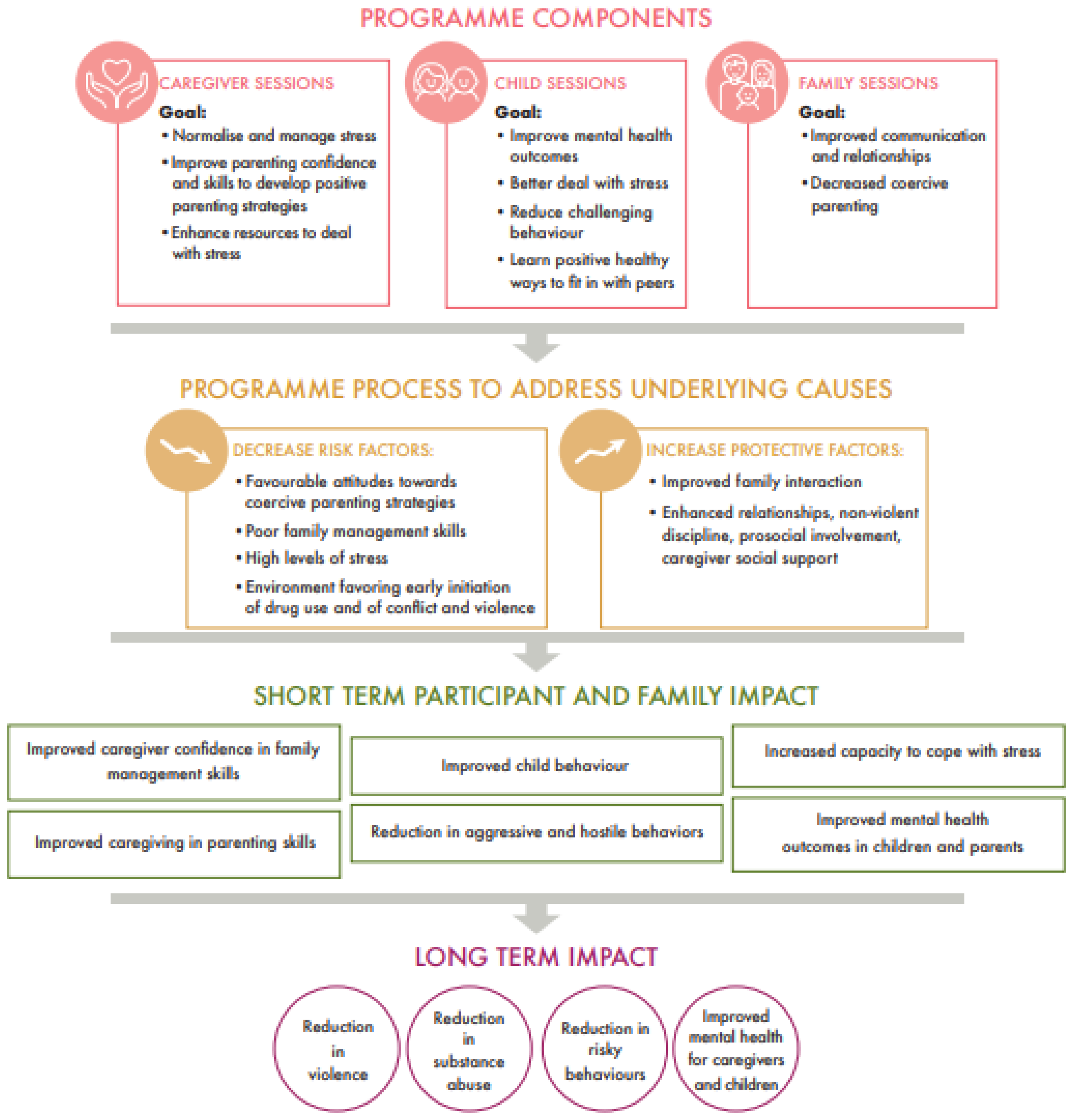
1.3. The Family UNited Programme
1.4. Objectives of This Study
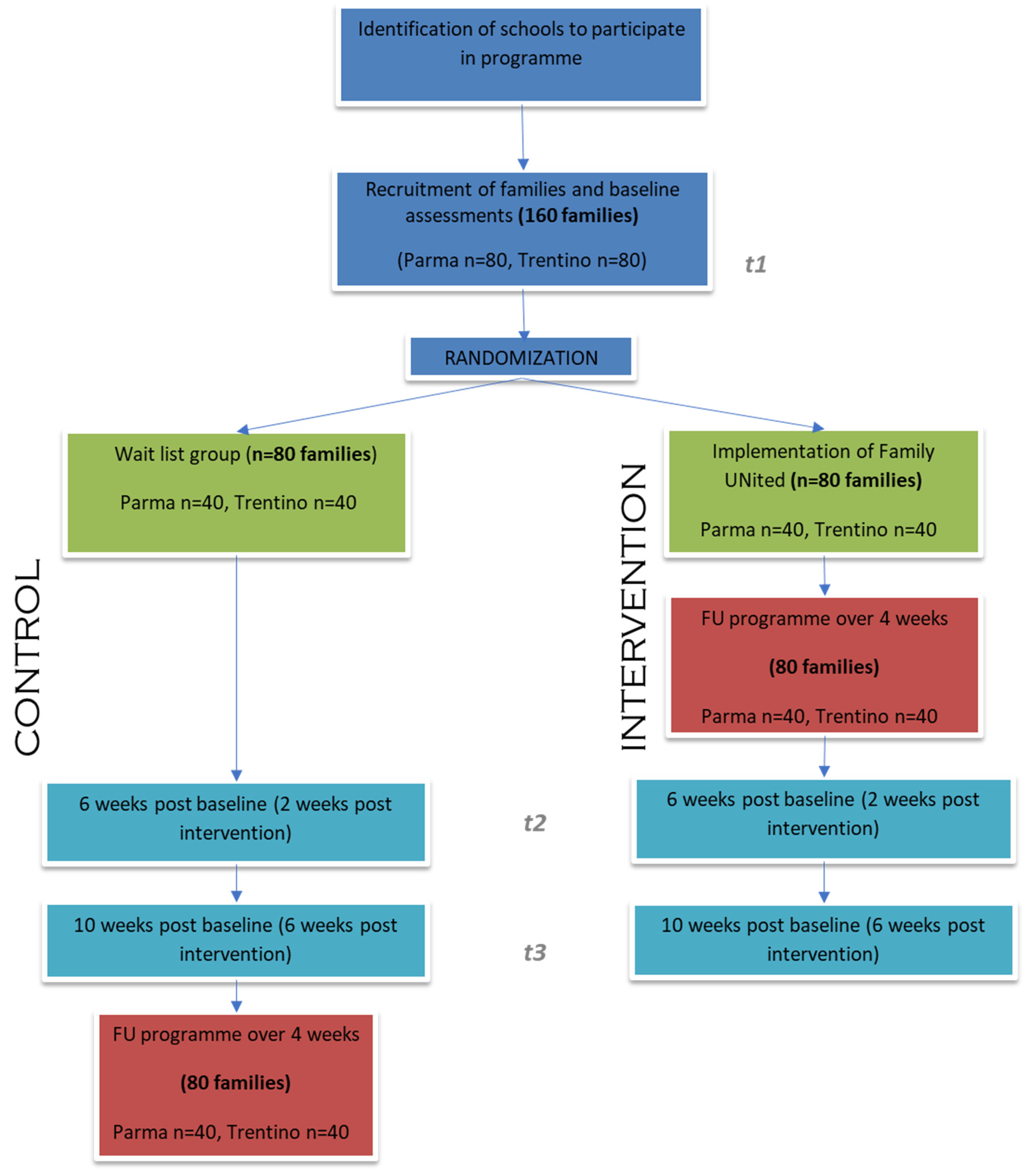
1.5. Trial Design
2. Materials and Methods
2.1. Study Setting
2.2. Eligibility Criteria
2.3. Intervention Condition
2.4. Waitlist/Control Condition
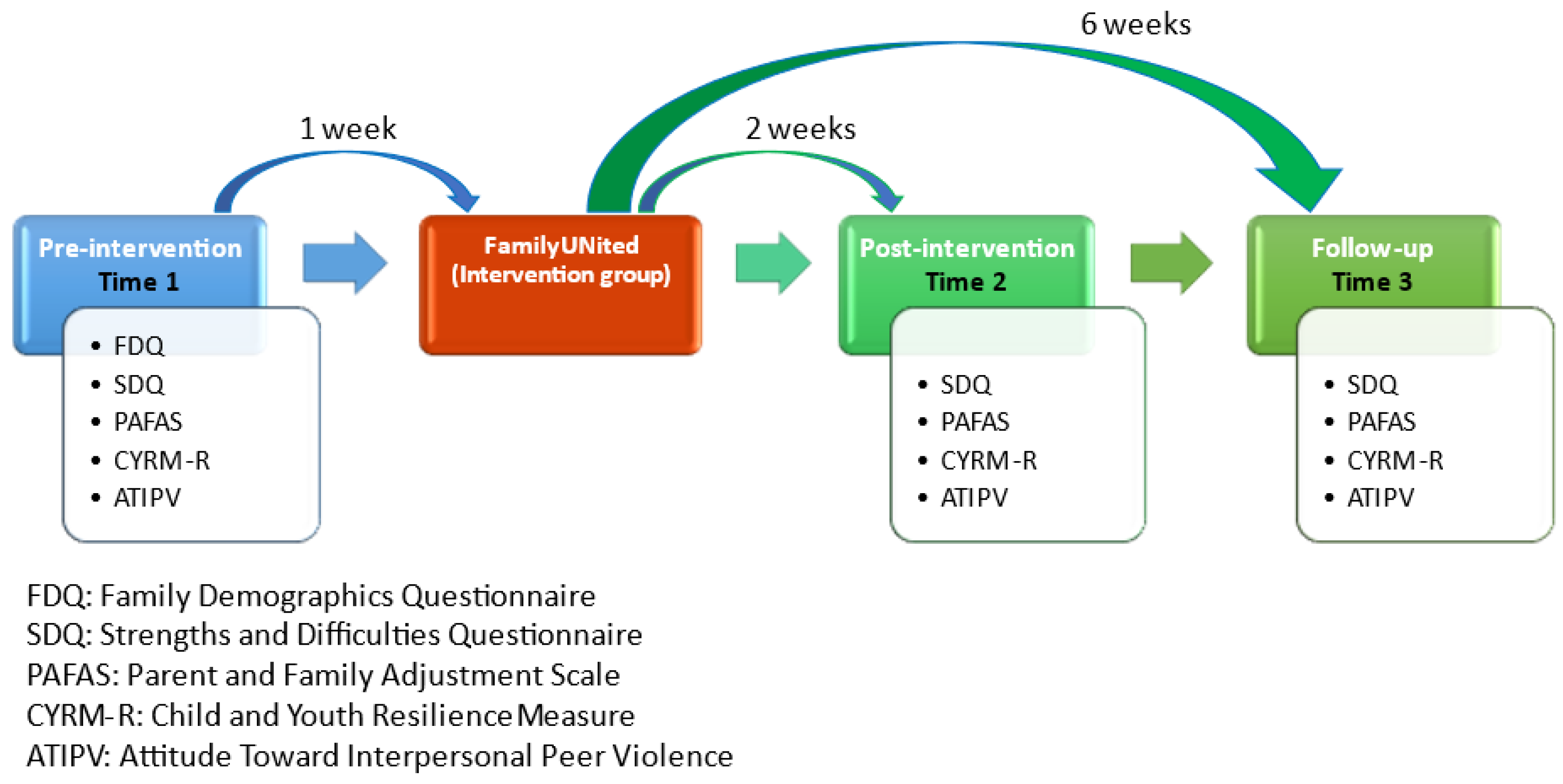
2.5. Outcomes
2.6. Participant Timeline
2.7. Sample Size
2.8. Recruitment of Families
2.9. Allocation
2.10. Data Collection Methods
2.11. Data Management
2.11.1. Data Entry and Data Coding
2.11.2. Data Quality
2.11.3. Quantitative Statistical Methods and Qualitative Data Analysis
2.11.4. Data Monitoring, Quality Assurance and Potential Harms
2.11.5. Auditing
2.12. Ethics and Dissemination
2.12.1. Research Ethics Approval
2.12.2. Protocol Amendments
2.12.3. Consent or Assent
2.12.4. Confidentiality
2.12.5. Declaration of Interests
2.12.6. Access to Data
2.12.7. Ancillary and Post-Trial Care
2.12.8. Dissemination Policy
3. Summary
4. Trial Status
5. Standards of Reporting
6. Protocol Version
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barry, M. Promoting positive mental health: Theoretical frameworks for practice. Int. J. Ment. Health Promot. 2001, 3, 25–34. [Google Scholar]
- Smith, P.; Perrin, S.; Yule, W.; Rabe-Hesketh, S. War Exposure and Maternal Reactions in the Psychological Adjustment of Children from Bosnia-Hercegovina. J. Child Psychol. Psychiatry 2001, 42, 395–404. [Google Scholar] [CrossRef]
- Calam, R.; El-Khani, A.; Maalouf, W. Editorial Perspective: How can we help the children of Ukraine and others affected by military conflict? Child Adolesc. Ment. Health 2022, 27, 294–296. [Google Scholar] [CrossRef]
- Smith, D.E.; Mosby, G. Jamaican child-rearing practices: The role of corporal punishment. Adolescence 2003, 38, 369–381. [Google Scholar]
- Jackson, A. Gang Risk Factors among Urban Jamaican Youth: A Qualitative Analysis. Int. J. Crim. Justice Sci. 2016, 11, 132. [Google Scholar]
- UNODC. Compilation of Evidence-Based Family Skills Training Programmes; United Nations Office on Drugs and Crime: Vienna, Austria, 2010. [Google Scholar]
- Mejia, A.; Calam, R.; Sanders, M.R. A pilot randomized controlled trial of a brief parenting intervention in low-resource settings in Panama. Prev. Sci. 2015, 16, 707–717. [Google Scholar] [CrossRef]
- Haar, K.; El-Khani, A.; Molgaard, V.; Maalouf, W. Strong families: A new family skills training programme for challenged and humanitarian settings: A single-arm intervention tested in Afghanistan. BMC Public Health 2020, 20, 634. [Google Scholar] [CrossRef] [PubMed]
- El-Khani, A.; Haar, K.; Stojanovic, M.; Maalouf, W. Assessing the Feasibility of Providing a Family Skills Intervention, “Strong Families”, for Refugee Families Residing in Reception Centers in Serbia. Int. J. Environ. Res. Public Health 2021, 18, 4530. [Google Scholar] [CrossRef] [PubMed]
- Haar, K.; El-Khani, A.; Mostashari, G.; Hafezi, M.; Malek, A.; Maalouf, W. Impact of a Brief Family Skills Training Programme (“Strong Families”) on Parenting Skills, Child Psychosocial Functioning, and Resilience in Iran: A Multisite Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 11137. [Google Scholar] [CrossRef] [PubMed]
- Kumpfer, K.L.; Trunnell, E.P.; Whiteside, H. The Biopsychosocial Model: Application to the Addictions Field. In Controversies in the Addiction Field; Engs, R.C., Ed.; Kendal-Hunt: Dubuque, IA, USA, 1990. [Google Scholar]
- Richardson, G.E.; Neiger, B.L.; Jensen, S.; Kumpfer, K.L. The Resiliency Model. Health Educ. 1990, 21, 33–39. [Google Scholar] [CrossRef]
- Garmezy, N. Resilience in children’s adaptation to negative life events and stressed environments. Pediatr. Ann. 1991, 20, 459–460, 463–466. [Google Scholar] [CrossRef]
- Masten, A.S. Ordinary magic. Resilience processes in development. Am. Psychol. 2001, 56, 227–238. [Google Scholar] [CrossRef]
- Betancourt, T.S.; Keegan, K.; Farrar, J.; Brennan, R.T. The intergenerational impact of war on mental health and psychosocial wellbeing: Lessons from the longitudinal study of war-affected youth in Sierra Leone. Confl. Health 2020, 14, 62. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A.; Walters, R.H. Social Learning Theory; Prentice Hall: Englewood Cliffs, NJ, USA, 1977; Volume 1. [Google Scholar]
- O’Connor, T.G.; Matias, C.; Futh, A.; Tantam, G.; Scott, S. Social learning theory parenting intervention promotes attachment-based caregiving in young children: Randomized clinical trial. J. Clin. Child Adolesc. Psychol. 2013, 42, 358–370. [Google Scholar] [CrossRef]
- Scott, S.; Gardner, F. Parenting programs. In Rutter’s Child and Adolescent Psychiatry; Wiley: Hoboken, NJ, USA, 2015; pp. 483–495. [Google Scholar]
- UNODC. Family UNited: Universal Family Skills Programme for Prevention of Negative Social Outcomes in Low- and Middle-Income Countries. Available online: https://www.unodc.org/documents/listenfirst/covid19/Family-UNited-leaflet-20200218.pdf (accessed on 28 January 2022).
- Eurostat. Gross Domestic Product (GDP) at Current Market Prices by NUTS 2 Regions. Available online: http://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=nama_10r_2gdp&lang=en (accessed on 19 October 2022).
- Deolmi, M.; Turco, E.C.; Pellegrini, P.; Marchesi, C.; Pisani, F. Psychiatric Emergency in Children and Adolescents: A Retrospective Study in Parma Local Health Unit. Behav. Neurol. 2021, 2021, 8848387. [Google Scholar] [CrossRef] [PubMed]
- Bean, T.M.; Eurelings-Bontekoe, E.; Spinhoven, P. Course and predictors of mental health of unaccompanied refugee minors in the Netherlands: One year follow-up. Soc. Sci. Med. 2007, 64, 1204–1215. [Google Scholar] [CrossRef] [PubMed]
- Linnan, L.; Steckler, A. Process Evaluation for Public Health Interventions and Research: An Overview; Linnan, L., Steckler, A., Eds.; Jossey-Bass: San Francisco, CA, USA, 2002; pp. 1–23. [Google Scholar]
- Segrott, J.; Murphy, S.; Rothwell, H.; Scourfield, J.; Foxcroft, D.; Gillespie, D.; Holliday, J.; Hood, K.; Hurlow, C.; Morgan-Trimmer, S.; et al. An application of Extended Normalisation Process Theory in a randomised controlled trial of a complex social intervention: Process evaluation of the Strengthening Families Programme (10–14) in Wales, UK. SSM Popul. Health 2017, 3, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Dhand, N.; Khatkar, M. Statulator: An Online Statistical Calculator. Sample Size Calculator for Comparing Two Paired Means. Available online: http://statulator.com/SampleSize/ss2PM.html# (accessed on 24 June 2022).
- Riso, D.D.; Salcuni, S.; Chessa, D.; Raudino, A.; Lis, A.; Altoè, G. The Strengths and Difficulties Questionnaire (SDQ). Early evidence of its reliability and validity in a community sample of Italian children. Personal. Individ. Differ. 2010, 49, 570–575. [Google Scholar] [CrossRef]
- Sanders, M.R.; Morawska, A.; Haslam, D.M.; Filus, A.; Fletcher, R. Parenting and Family Adjustment Scales (PAFAS): Validation of a brief parent-report measure for use in assessment of parenting skills and family relationships. Child Psychiatry Hum. Dev. 2014, 45, 255–272. [Google Scholar] [CrossRef]
- Jefferies, P.; McGarrigle, L.; Ungar, M. The CYRM-R: A Rasch-Validated Revision of the Child and Youth Resilience Measure. J. Evid.-Based Soc. Work. 2019, 16, 70–92. [Google Scholar] [CrossRef]
- Dahlberg, L.L.; Toal, S.B.; Swahn, M.H.; Behrens, C.B. Measuring Violence-Related Attitudes, Behaviors, and Influences among Youths: A Compendium of Assessment Tools, 2nd ed.; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2005. [Google Scholar]
- SDQInfo. Downloadable SDQs and Related Items. Available online: https://www.sdqinfo.org/py/sdqinfo/b0.py (accessed on 14 August 2020).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- EU-Dap. EUropean Drug Addiction Prevention Trial. Available online: https://www.eudap.net/ (accessed on 24 October 2022).
- European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). European Drug Prevention Quality Standards (EDPQS) Toolkit 2: Self-Assessment and Reflection. Available online: https://www.emcdda.europa.eu/drugs-library/european-drug-prevention-quality-standards-edpqs-toolkit-2-self-assessment-and-reflection_en (accessed on 24 October 2022).
- European Monitoring Centre for Drugs and Drug Addiction. European Prevention Curriculum: A Handbook for Decision-Makers, Opinion-Makers and Policy-Makers in Science-Based Prevention of Substance Use; European Monitoring Centre for Drugs and Drug Addiction: Luxembourg, 2019. [Google Scholar]
- Chan, A.W.; Tetzlaff, J.M.; Altman, D.G.; Laupacis, A.; Gøtzsche, P.C.; Krleža-Jerić, K.; Hróbjartsson, A.; Mann, H.; Dickersin, K.; Berlin, J.A.; et al. SPIRIT 2013 statement: Defining standard protocol items for clinical trials. Ann. Intern. Med. 2013, 158, 200–207. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Caregiver Session | Child Session | Family Session | |
|---|---|---|---|
| Week 1 | Understanding praising and encouraging children | Building positive qualities | Our family’s positive qualities |
| Week 2 | Changing challenging behaviour | Handling stress | Learning about each other |
| Week 3 | Responding to un-desirable behaviour | Skills to resist peer pressure I | Understanding peer pressure and family connections I |
| Week 4 | Communicating and taking care of yourself | Skills to resist peer pressure II | Understanding peer pressure and family connections II |
| Process Evaluation Component | Data Source | Indicator | Caregiver | Child | Family | Total | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Session 1 | Session 2 | Session 3 | Session 4 | Session 1 | Session 2 | Session 3 | Session 4 | Session 1 | Session 2 | Session 3 | Session 4 | ||||
| Dose delivered | Coordinator | Number of sessions delivered | |||||||||||||
| Fidelity | Observer | Percentage of activities reported as covered | |||||||||||||
| Facilitator | Percentage of activities reported as fully/mostly covered as 3/4 (on a scale of 1 [not/hardly] to 4 [fully]) | ||||||||||||||
| Observer | Percentage of programmes with ≥2 facilitators at every session | ||||||||||||||
| Observer | Percentage of programmes with ≥1 of the same facilitators at every session | ||||||||||||||
| Observer | Percentage of programmes with >4 and <15 families | ||||||||||||||
| Dose received | Facilitator | Percentage of activities reporting interest of young people; and parents/carers as 3/4 (on a scale of 1 [low] to 4 [high]) | |||||||||||||
| Reach | Observer | Percentage of families attending all 4 sessions | |||||||||||||
| Inputs | Observer | Percentage of sheets with a good or very good evaluation of the quality of childcare and travel arrangements | |||||||||||||
| Observer | Percentage of sheets with a positive evaluation of (area of) refreshments | ||||||||||||||
| Observer | Percentage of sheets with a positive evaluation of room/materials/equipment | ||||||||||||||
| Week | Activity |
|---|---|
| PILOT STUDY | |
| Week 1 | Recruitment of 2 Research Assistants and training on measure completion |
| Week 2 | Research Assistants recruit 10 families. |
| Week 2 | Research Assistants conduct baseline measures and consent (Time 1) with all 10 families |
| Week 3–6 | Families take part in weekly sessions of Family UNited for 4 weeks |
| Week 6 | All families’ complete measures again (Time 2) |
| RCT | |
| Week 1–2 | Research Assistants assess families for eligibility and inform them about the planned trial and the programme verbally and in writing |
| Week 3 | Research Assistants recruit 160 families, obtain written assent/consent and conduct baseline measures (Time 1; pre-intervention) with all families After data collection has been completed, families are randomly allocated to intervention or control group |
| Week 4–7 | Intervention group families take part in weekly sessions of Family UNited for 4 weeks Facilitators and observers complete process evaluation tools after each session |
| Week 9 | ALL families complete measures again (Time 2; post-intervention). 10 caregivers from the intervention group are interviewed for acceptability |
| Week 13 | ALL families complete measures again (Time 3; follow-up) |
| Week 14–17 | Control families take part in weekly sessions of Family UNited for 4 weeks |
| Before: Mean ± SD | After: Mean ± SD | Paired Difference in Means ± SD | Sample Size (Power) | ||
|---|---|---|---|---|---|
| PAFAS | 80% | 90% | |||
| Positive encouragement (n = 14) | 5.1 ± 2.3 | 2,1 ± 1.2 | 3.0 * ± 2.7 | 10 | 12 |
| Parental adjustment (n = 14) | 5.9 ± 3.1 | 4.7 ± 2.7 | 1.2 ± 2.7 | 40 | 54 |
| Family relationships (n = 14) | 3.8 ± 2.3 | 2.9 ± 1.7 | 0.9 * ± 1.2 | 17 | 21 |
| SDQ | |||||
| Hyperactivity (n = 14) | 2.8 ± 2.1 | 2.1 ± 1.8 | 0.7 * ± 1.1 | 23 | 30 |
| Conduct problems (n = 14) | 2.6 ± 1.8 | 1.3 ± 1.1 | 1.4 * ± 1.4 | 12 | 15 |
| Total Difficulty Scale (n = 14) | 10.9 ± 5.0 | 8.4 ± 4.4 | 2.6 * ± 3.7 | 20 | 26 |
| CYRM-R | |||||
| Total CYRM (n = 12) | 58.8 ± 19.0 | 60.8 ± 18.2 | 1.9 ± 6.9 | 104 | 138 |
| Personal resilience (n = 12) | 35.8 ± 11.8 | 37.4 ± 11.3 | 1.7 ± 3.9 | 45 | 61 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haar, K.; El-Khani, A.; Lodi, R.; Molin, V.; Pelosi, A.; Yassine, A.; Campello, G.; Maalouf, W. Assessing the Efficacy of a Brief Universal Family Skills Programme on Violence and Substance-Use Indicators in Youth in Trentino and Parma, Italy: Study Protocol for a Multi-Centre, Non-Blinded, Cluster-Randomised Controlled Trial (cRCT) of Family UNited. Int. J. Environ. Res. Public Health 2023, 20, 6548. https://doi.org/10.3390/ijerph20166548
Haar K, El-Khani A, Lodi R, Molin V, Pelosi A, Yassine A, Campello G, Maalouf W. Assessing the Efficacy of a Brief Universal Family Skills Programme on Violence and Substance-Use Indicators in Youth in Trentino and Parma, Italy: Study Protocol for a Multi-Centre, Non-Blinded, Cluster-Randomised Controlled Trial (cRCT) of Family UNited. International Journal of Environmental Research and Public Health. 2023; 20(16):6548. https://doi.org/10.3390/ijerph20166548
Chicago/Turabian StyleHaar, Karin, Aala El-Khani, Riccardo Lodi, Valentina Molin, Annalisa Pelosi, Ali Yassine, Giovanna Campello, and Wadih Maalouf. 2023. "Assessing the Efficacy of a Brief Universal Family Skills Programme on Violence and Substance-Use Indicators in Youth in Trentino and Parma, Italy: Study Protocol for a Multi-Centre, Non-Blinded, Cluster-Randomised Controlled Trial (cRCT) of Family UNited" International Journal of Environmental Research and Public Health 20, no. 16: 6548. https://doi.org/10.3390/ijerph20166548
APA StyleHaar, K., El-Khani, A., Lodi, R., Molin, V., Pelosi, A., Yassine, A., Campello, G., & Maalouf, W. (2023). Assessing the Efficacy of a Brief Universal Family Skills Programme on Violence and Substance-Use Indicators in Youth in Trentino and Parma, Italy: Study Protocol for a Multi-Centre, Non-Blinded, Cluster-Randomised Controlled Trial (cRCT) of Family UNited. International Journal of Environmental Research and Public Health, 20(16), 6548. https://doi.org/10.3390/ijerph20166548