
The Effectiveness of Nursing Rehabilitation Interventions on Self-Care for Older Adults with Respiratory Disorders: A Systematic Review with Meta-Analysis


 ,
,  , and
, and
Abstract
1. Introduction
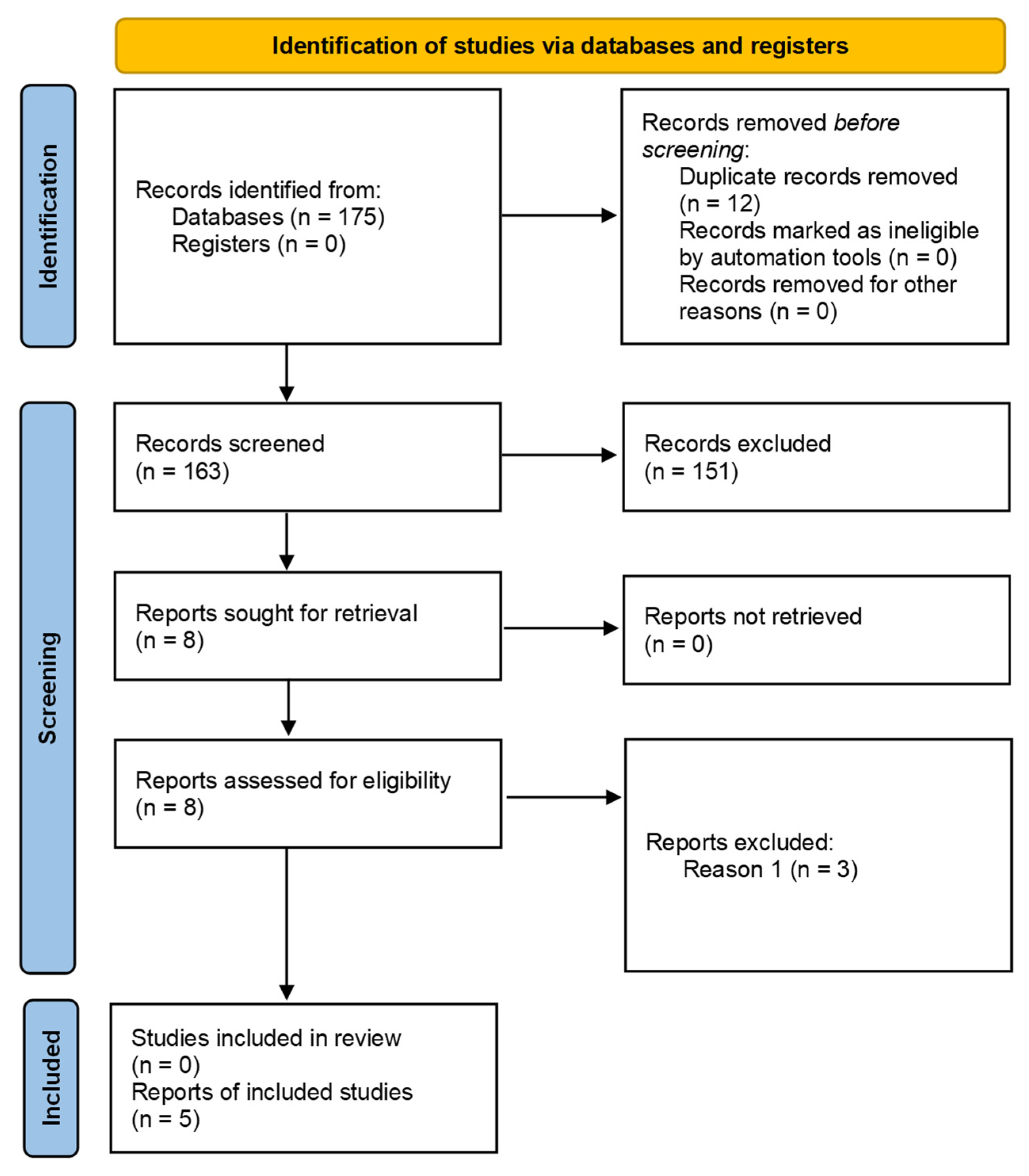
2. Materials and Methods
(self-care promotion OR education) AND (older adults) AND
(respiratory disorders).
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Domains | Rehabilitation Nursing Interventions |
|---|---|
| Functional status |
|
| Symptom control | |
| Self-care capacity | |
| Health-related quality of life | |
| Health promotion activities | |
| Healthcare utilization |
|
| Patient satisfaction |
|
References
- Sharma, G.; Goodwin, J. Effect of aging on respiratory system physiology and immunology. Clin. Interv. Aging 2006, 1, 253–260. [Google Scholar] [CrossRef]
- Ketata, W.; Rekik, W.K.; Ayadi, H.; Kammoun, S. Aging of the respiratory system: Anatomical changes and physiological consequences. Rev. Pneumol. Clin. 2012, 68, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Bentayeb, M.; Simoni, M.; Norback, D.; Baldacci, S.; Maio, S.; Viegi, G.; Annesi-Maesano, I. Indoor air pollution and respiratory health in the elderly. J. Environ. Sci. Health Part A 2013, 48, 1783–1789. [Google Scholar] [CrossRef]
- Andrade, A.; D’Oliveira, A.; De Souza, L.C.; Bastos, A.C.R.d.F.; Dominski, F.H.; Stabile, L.; Buonanno, G. Effects of Air Pollution on the Health of Older Adults during Physical Activities: Mapping Review. Int. J. Environ. Res. Public Health 2023, 20, 3506. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Soriano, J.B.; Kendrick, P.J.; Paulson, K.R.; Gupta, V.; Abrams, E.M.; Adedoyin, R.A.; Adhikari, T.B.; Advani, S.M.; Agrawal, A.; Ahmadian, E.; et al. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2020, 8, 585–596. [Google Scholar] [CrossRef]
- World Health Organization. Chronic Respiratory Diseases. Available online: https://www.who.int/health-topics/chronic-respiratory-diseases#tab=tab_2 (accessed on 9 July 2023).
- Chung, Y.; Huang, T.-Y.; Liao, Y.-H.; Kuo, Y.-C. 12-Week Inspiratory Muscle Training Improves Respiratory Muscle Strength in Adult Patients with Stable Asthma: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 3267. [Google Scholar] [CrossRef]
- Wang, L.H.; Zhao, Y.; Chen, L.Y.; Zhang, L.; Zhang, Y.M. The effect of a nurse-led self-management program on outcomes of patients with chronic obstructive pulmonary disease. Clin. Respir. J. 2019, 14, 148–157. [Google Scholar] [CrossRef]
- World Health Organization. Respiratory Infections: Deaths by Sex and Age Group for a Selected Country or Area and Year. Available online: https://platform.who.int/mortality/themes/theme-details/topics/topic-details/MDB/respiratory-infections (accessed on 9 July 2023).
- Belli, S.; Prince, I.; Savio, G.; Paracchini, E.; Cattaneo, D.; Bianchi, M.; Masocco, F.; Bellanti, M.T.; Balbi, B. Airway Clearance Techniques: The Right Choice for the Right Patient. Front. Med. 2021, 8, 544826. [Google Scholar] [CrossRef]
- O’Neill, K.; O’Donnell, A.E.; Bradley, J.M. Airway clearance, mucoactive therapies and pulmonary rehabilitation in bronchiectasis. Respirology 2019, 24, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Martin-Sanchez, C.; Barbero-Iglesias, F.J.; Amor-Esteban, V.; Martin-Nogueras, A.M. Comparison between Two Inspiratory Muscle Training Protocols, Low Loads versus High Loads, in Institutionalized Elderly Women: A Double-Blind Randomized Controlled Trial. Gerontology 2021, 67, 1–8. [Google Scholar] [CrossRef]
- Tsang, E.W.; Kwok, H.; Chan, A.K.Y.; Choo, K.L.; Chan, K.S.; Lau, K.S.; Chan, C.C.H. Outcomes of community-based and home-based pulmonary rehabilitation for pneumoconiosis patients: A retrospective study. BMC Pulm. Med. 2018, 18, 133. [Google Scholar] [CrossRef]
- Moorhead, S.; Swanson, E.; Johnson, M. Nursing Outcomes Classification (NOC): Measurement of Health Outcomes; Elsevier: Amsterdam, The Netherlands, 2022. [Google Scholar]
- Flynn, M.; Mercer, D.; Flynn, M.; Mercer, D. Respiratory conditions. In Oxford Handbook of Adult Nursing; Oxford University Press: Oxford, UK, 2018; pp. 165–194. [Google Scholar]
- Liu, Q.; Li, W. The Way of Severe Nursing of Respiratory System Failure. J. Healthc. Eng. 2021, 2021, 1667458. [Google Scholar] [CrossRef] [PubMed]
- López-Liria, R.; Vega-Ramírez, F.A.; Aguilar-Parra, J.M.; Padilla-Góngora, D.; Trigueros-Ramos, R.; Rocamora-Pérez, P. Evaluation of the Effectiveness of a Nursing/Physiotherapy Program in Chronic Patients. Int. J. Environ. Res. Public Health 2019, 16, 2236. [Google Scholar] [CrossRef] [PubMed]
- Frosch, D.L.; Rincon, D.; Ochoa, S.; Mangione, C.M. Activating Seniors to Improve Chronic Disease Care: Results from a Pilot Intervention Study. J. Am. Geriatr. Soc. 2010, 58, 1496–1503. [Google Scholar] [CrossRef]
- Steinsbekk, A.; Rygg, L.; Lisulo, M.; Rise, M.B.; Fretheim, A. Group based diabetes self-management education compared to routine treatment for people with type 2 diabetes mellitus. A systematic review with meta-analysis. BMC Health Serv. Res. 2012, 12, 213. [Google Scholar] [CrossRef]
- World Health Organization. Classification of Self-Care Interventions for Health: A Shared Language to Describe the Uses of Self-Care Interventions. Available online: https://www.who.int/publications/i/item/9789240039469 (accessed on 21 May 2023).
- Grady, P.A.; Gough, L.L. Self-Management: A Comprehensive Approach to Management of Chronic Conditions. Am. J. Public Health 2014, 104, e25–e31. [Google Scholar] [CrossRef]
- Nabais, A.; Sá, M.d.C. The patient with chronic obstructive pulmonary disease: How rehabilitation nurses promote self-care. Millenium J. Educ. Technol. Health 2019, 2, 81–89. [Google Scholar] [CrossRef]
- Metting, E.; Dassen, L.; Aardoom, J.; Versluis, A.; Chavannes, N. Effectiveness of Telemonitoring for Respiratory and Systemic Symptoms of Asthma and COPD: A Narrative Review. Life 2021, 11, 1215. [Google Scholar] [CrossRef] [PubMed]
- Gordon, C.S.; Waller, J.W.; Cook, R.M.; Cavalera, S.L.; Lim, W.T.; Osadnik, C.R. Effect of Pulmonary Rehabilitation on Symptoms of Anxiety and Depression in COPD. Chest 2019, 156, 80–91. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Zhong, Y.; Qin, Z.; Li, X.; Wang, W. Effect of muscle training on dyspnea in patients with chronic obstructive pulmonary disease. Medicine 2021, 100, e24930. [Google Scholar] [CrossRef] [PubMed]
- Lopes, A.J.; Guimarães, F.S.; Ferreira, A.S.; Almeida, V.P.; Lima, T.R.L. Handgrip Strength and Pulmonary Disease in the Elderly: What is the Link? Aging Dis. 2019, 10, 1109–1129. [Google Scholar] [CrossRef]
- Gutenbrunner, C.; Stievano, A.; Stewart, D.; Catton, H.; Nugraha, B. Role of nursing in rehabilitation. J. Rehabil. Med. Clin. Commun. 2021, 4, jrmcc00063. [Google Scholar] [CrossRef]
- Sun, X.; Shen, Y.; Shen, J. Respiration-related guidance and nursing can improve the respiratory function and living ability of elderly patients with chronic obstructive pulmonary disease. Am. J. Transl. Res. 2021, 13, 4686–4695. [Google Scholar]
- Mętel, S.; Kostrzon, M.; Adamiak, J. Dynamic Balance and Chest Mobility of Older Adults after Speleotherapy Combined with Pulmonary Rehabilitation, Endurance and Strength Training—A Prospective Study in Chronic Respiratory Diseases. Int. J. Environ. Res. Public Health 2022, 19, 11760. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Pu, Y.; Meng, A.; Zhi, X.; Xu, G. Effectiveness of pulmonary rehabilitation in elderly patients with COPD: A systematic review and meta-analysis of randomized controlled trials. Int. J. Nurs. Pract. 2019, 25, e12745. [Google Scholar] [CrossRef] [PubMed]
- Centre for Reviews and Dissemination University of York. International Prospective Register of Systematic Reviews (PROSPERO). Available online: https://www.crd.york.ac.uk/prospero/ (accessed on 18 May 2023).
- Boren, S.A.; Moxley, D. Systematically reviewing the literature: Building the evidence for health care quality. Mo. Med. 2015, 112, 58–62. [Google Scholar]
- PRISMA. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Available online: http://www.prisma-statement.org/ (accessed on 18 May 2023).
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Introduction to Meta-Analysis, 2nd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2021. [Google Scholar]
- Biostat Inc. Comprehensive Meta-Analysis. Available online: https://www.meta-analysis.com/ (accessed on 18 May 2023).
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Methods 2010, 1, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Lin, J.; Demner-Fushman, D. Evaluation of PICO as a knowledge representation for clinical questions. AMIA Annu. Symp. Proc. 2006, 2006, 359–363. [Google Scholar]
- BIREME; PAHO; WHO. Descritores em Ciências da Saúde (Health Science Descriptors). 2017. Available online: https://decs.bvsalud.org/en/ (accessed on 18 May 2023).
- National Library of Medicine. Medical Subject Headings. Available online: https://www.nlm.nih.gov/mesh/meshhome.html (accessed on 18 May 2023).
- Joanna Briggs Institute. Evidence Based Practice—Database Guide. Available online: https://ospguides.ovid.com/OSPguides/jbidb.htm (accessed on 18 May 2023).
- Joanna Briggs Institute (JBI). Critical Appraisal Tools. Available online: https://jbi.global/critical-appraisal-tools (accessed on 18 May 2023).
- Collins, E.G.; Jelinek, C.; O’Connell, S.; Butler, J.; Reda, D.; Laghi, F. The Effect of Breathing Retraining Using Metronome-Based Acoustic Feedback on Exercise Endurance in COPD: A Randomized Trial. Lung 2019, 197, 181–188. [Google Scholar] [CrossRef]
- Doran, D.; Pringle, D. Patient Outcomes as an Accountability. In Nursing Outcomes: State of the Science, 2nd ed.; Doran, D., Ed.; Jones & Bartlett Learning: Burlington, MA, USA, 2011. [Google Scholar]
- Ordem dos Enfermeiros. Core de Indicadores por Categoria de Enunciados Descritivos dos Padrões de Qualidade dos Cuidados de Enfermagem de Reabilitação. Available online: https://www.ordemenfermeiros.pt/arquivo/colegios/Documents/2015/MCEER_Assembleia/Core_Indicadores_por_Categoria_de_Enunciados_Descrit_PQCER.pdf (accessed on 21 May 2023).
- Pinho, L.G.d.; Lopes, M.J.; Correia, T.; Sampaio, F.; Arco, H.R.d.; Mendes, A.; Marques, M.d.C.; Fonseca, C. Patient-Centered Care for Patients with Depression or Anxiety Disorder: An Integrative Review. J. Personal. Med. 2021, 11, 776. [Google Scholar] [CrossRef]
- Nascimento, V.; Fonseca, C.; Pinho, L.G.; Lopes, M.J. Person-Centered Health Intervention Programs, Provided at Home to Older Adults with Multimorbidity and Their Caregivers: Protocol for a Systematic Review. J. Personal. Med. 2022, 13, 27. [Google Scholar] [CrossRef]
- Fonseca, C.; Ramos, A.; Pinho, L.G.; Morgado, B.; Oliveira, H.; Lopes, M. Functional Profile of Older Adults Hospitalized in Rehabilitation Units of the National Network of Integrated Continuous Care of Portugal: A Longitudinal Study. J. Personal. Med. 2022, 12, 1937. [Google Scholar] [CrossRef] [PubMed]
- Ramos, A.; Fonseca, C.; Pinho, L.; Lopes, M.; Brites, R.; Henriques, A. Assessment of Functioning in Older Adults Hospitalized in Long-Term Care in Portugal: Analysis of a Big Data. Front. Med. 2022, 9, 780364. [Google Scholar] [CrossRef] [PubMed]
- Rojo, J.; de Pinho, L.G.; Fonseca, C.; Lopes, M.J.; Helal, S.; Hernández, J.; Garcia-Alonso, J.; Murillo, J.M. Analyzing the Performance of Feature Selection on Regression Problems: A Case Study on Older Adults’ Functional Profile. IEEE Trans. Emerg. Top. Comput. 2023, 11, 137–152. [Google Scholar] [CrossRef]
- Uslu, A.; Canbolat, O. Nursing Care of The Chronic Obstructive Pulmonary Disease Patient According to Orem’s Theory of Self-Care Deficiency: A Case Report. J. Educ. Res. Nurs. 2022, 19, 269–274. [Google Scholar] [CrossRef]
- Goes, M.; Lopes, M.J.; Oliveira, H.; Fonseca, C.; Marôco, J. A Nursing Care Intervention Model for Elderly People to Ascertain General Profiles of Functionality and Self Care Needs. Sci. Rep. 2020, 10, 1770. [Google Scholar] [CrossRef]
- Goes, M.; Oliveira, H.; Lopes, M.; Fonseca, C.; Pinho, L.; Marques, M. A nursing care-sensitive patient satisfaction measure in older patients. Sci. Rep. 2023, 13, 7607. [Google Scholar] [CrossRef]
- Goes, M.; Lopes, M.; Oliveira, H.; Marôco, J.; Fonseca, C.; Santos, M.; Caeiro, J. Psychometric Qualities of a Core Set to Ascertain the Functional Profile of Portuguese Elderly Citizens. In Gerontechnology; Communications in Computer and Information Science; Springer: Cham, Switzerland, 2020; pp. 314–329. [Google Scholar]
- Goes, M.; Lopes, M.; Oliveira, H.; Marôco, J.; Fonseca, C.; Santos, M.; Caeiro, J. A Nursing Care Intervention Model for Elderly People Adopting Self-care as a Central Concept. In Gerontechnology; Communications in Computer and Information Science; Springer: Cham, Switzerland, 2020; pp. 359–372. [Google Scholar]
- World Health Organization. WHO Guideline on Self-Care Interventions for Health and Well-Being, 2022 Revision. Available online: https://www.who.int/publications/i/item/9789240052192 (accessed on 20 June 2023).
- Goes, M.; Oliveira, H.; Lopes, M.; Fonseca, C.; Pinho, L. Satisfaction: A Concept Based on Functionality and Quality of Life to Be Integrated in a Nursing Care Performance System. In Gerontechnology IV; Lecture Notes in Bioengineering; Springer: Cham, Switzerland, 2022; pp. 84–93. [Google Scholar]
- Lee, J.J.; Sundar, K.M. Evaluation and Management of Adults with Obstructive Sleep Apnea Syndrome. Lung 2021, 199, 87–101. [Google Scholar] [CrossRef]
- López-López, L.; Torres-Sánchez, I.; Cabrera-Martos, I.; Ortíz-Rubio, A.; Granados-Santiago, M.; Valenza, M.C. Nursing Interventions Improve Continuous Positive Airway Pressure Adherence in Obstructive Sleep Apnea with Excessive Daytime Sleepiness: A Systematic Review. Rehabil. Nurs. 2020, 45, 140–146. [Google Scholar] [CrossRef]
- Makic, M.B.F.; Martinez-Kratz, M.R. Ackley and Ladwig’s Nursing Diagnosis Handbook, 13th ed.; Elsevier: Amsterdam, The Netherlands, 2023. [Google Scholar]


| Authors (Year), Reference, and Title | Objectives | Participants | Interventions/Phenomena of Interest | Results and Conclusions |
|---|---|---|---|---|
| Authors: Chung, Y.; Huang, T.-Y.; Liao, Y.-H.; Kuo, Y.-C. (2021) [8] Title: 12-Week Inspiratory Muscle Training Improves Respiratory Muscle Strength in Adult Patients with Stable Asthma: A Randomized Controlled Trial | To investigate and compare the effects of a 12-week intervention using breathing exercises or inspiratory muscle training on lung function, respiratory function, muscle strength, and asthma control (primary outcomes) as well as functional capacity and physical activity (secondary outcomes) in older people with asthma. | Sixty patients with asthma were randomly assigned to the following groups:
| The BET group took part in sessions twice a week for 25 min, performing diaphragmatic and nasal breathing, increasing their expiratory time, decreasing their respiratory flow, and regulating their breathing rhythms. They performed exercises to increase the resistance of the rib cage and abdominal and diaphragmatic strength in association with diaphragmatic breathing techniques and semi-closed lips. The IMT group performed 30 dynamic inspiratory exercises twice a day. The intensity of each inspiration was 50–60% of the maximum inspiratory pressure. Patients initiated inspiration from residual volume to maximal lung pressure for at least 1 s. | Both IMT and BET demonstrated comparable beneficial outcomes in enhancing functional capacity and physical activity. IMT effectively improved respiratory muscle strength (RMS), as evidenced by increased maximal inspiratory pressure. The observed maximal inspiratory pressure ranged from 72% to 82%, indicating the need to improve RMS in the target population of older adults. The impact of IMT on asthma demonstrated an improvement in inspiratory muscle strength and endurance, which supports the effectiveness of IMT as an asthma control strategy, reducing disease severity, as a non-drug therapy. In both groups, maximal expiratory pressure increased, as did RMS and functional capacity. BET and IMT induced increases in the 6-min walking test (6MWT), increasing exercise tolerance. The IMT group tended to show a more significant increase in physical activity time than the BET group, thus leading to the conclusion that implementing health education programs and professional guidance to improve RMS improves ventilatory control, which may be associated with confidence in performing physical activity. |
| Authors: Martin-Sanchez, C.; Barbero-Iglesias, Fausto J.; Amor-Esteban, V.; Martin-Nogueras, Ana M. (2021) [13] Title: Comparison between Two Inspiratory Muscle Training Protocols, Low Loads versus High Loads, in Institutionalized Elderly Women: A Double-Blind Randomized Controlled Trial | To evaluate and compare the effectiveness of 2 protocols with inspiratory muscle training (IMT), one with low intensity and the other with high intensity, to improve respiratory strength, functional capacity, and dyspnea in institutionalized elderly women over 65 years. | Institutionalized elderly women aged 75–95 years with a Barthel Index score of 60 or more, who were able to walk unaided and who understood the purpose and interventions of the study. The participants were randomly distributed into two groups:
| A pressure transducer assessed muscle strength by measuring maximal inspiratory and expiratory pressure. The 6-min walking test (6MWT) was used to assess functional capacity. Dyspnea was assessed using the Modified Medical Research Council scale. The inspiratory muscle training intervention protocol took place over 8 weeks, using the threshold, with a frequency of 1 session per day, 5 days a week. The participants performed 15 series of 1 min with 1 min of rest between them. The training intensity differed in both groups: 40% of the maximum inspiratory pressure in the IMT HIGH group and 20% in the IMT LOW group. | Respiratory muscle strength (RMS): A significant improvement in maximal inspiratory pressure occurred in the high-intensity group after the intervention compared to the low-intensity group. Maximal expiratory pressure increased significantly after the intervention in both groups, and the improvement achieved was similar between them. Functional Capacity: The distance walked on the 6MWT by both groups increased significantly after the intervention. Dyspnea: Dyspnea significantly improved in the low-intensity group after the intervention. In summary: This study showed that an 8-week protocol with inspiratory muscle training improves respiratory muscle strength and functional capacity in older women. Training with high loads was most effective for improving inspiratory muscle strength, and training with low loads was best for reducing dyspnea. A minimum load of 20% of the maximal inspiratory pressure was sufficient to improve dyspnea, inspiratory strength, expiratory strength, and functional capacity in older women. |
| Authors: Wang, L.H.; Zhao, Y.; Chen, L.Y.; Zhang, L.; Zhang, Y.M. (2019) [9] Title: The effect of a nurse-led self-management program on outcomes of patients with chronic obstructive pulmonary disease. | To examine the effectiveness of a nurse-led self-management program on outcomes in patients with chronic obstructive pulmonary disease (COPD) | A total of 154 patients were admitted to the Hospital of Zunyi Medical University in Guizhou with COPD, of whom 77 belonged to the control group and the remaining 77 to the intervention group. The participants were randomly assigned to the groups. | A self-management program was divided into 2 phases. In the first (6–7 days before discharge), the needs and fears of each participant were assessed (social support, barriers to self-management, enjoyment of physical activities) and, according to individual needs, 5 to 6 educational sessions were given by specialist nurses, each lasting 45 min. In each session, topics such as what COPD is and its impact, training the respiratory muscles, half-closed lips and diaphragmatic breathing, medication, inhaler use technique, coughing techniques, non-pharmacological strategies for symptom relief, types of physical exercises adapted to COPD, smoking cessation, and long-term oxygen therapy were addressed. The second phase comprised: (i) phone calls every week for 3 months (checking compliance with the self-management program, providing encouragement and positive reinforcement, checking for complications, and assessing exercise for duration and intensity); (ii) 3 home visits (assessing environmental risk factors, encouraging modification of health behaviors, reinforcing knowledge and self-management, providing understanding and emotional support). | The intervention group used the emergency room less often at 6 and 12 months of intervention than the control group, perhaps because patients were empowered to self-manage their disease and received appropriate interventions simultaneously, thus contributing to a reduction in disease exacerbation. Exercise capacity and tolerance levels increased after 3 and 6 months of intervention in the intervention group compared to the control group. Health-related quality of life increased in the intervention group, while its deterioration occurred in the control group. At 6 and 12 months of intervention, the intervention group was more satisfied with the program, service, and education provided than the control group. The findings of this study showcased that introducing a self-management program led by nurses, which focuses on fostering the skills and capabilities required for effectively managing therapy, symptoms, and psychological impacts in patients with COPD, resulted in decreased visits to the emergency department due to disease exacerbation. Additionally, the program demonstrated enhancements in exercise capacity, functional capacity, health-related quality of life, and overall satisfaction with the provided care. |
| Authors: Collins, E.G.; Jelinek, C.; O’Connell, S.; Butler, J.; Reda, D.; Laghi, F. (2019) [43] Title: The Effect of Breathing Retraining Using Metronome-Based Acoustic Feedback on Exercise Endurance in COPD: A Randomized Trial. | The primary objective of this study was to explore the impact of exercise training with respiratory re-education through acoustic feedback, using a metronome, during exercise in patients with chronic obstructive pulmonary disease (COPD). The secondary objective was to evaluate the impact of respiratory re-education on dynamic hyperinflation and patients’ health-related quality of life. | A total of 119 COPD patients were randomly selected from a population of 205, with 58 in the intervention group and 61 in the control group. | There were 36 training sessions, 3 times a week, in the laboratory. Both groups started by training for 25 min on a treadmill and progressed, according to tolerance, to 45 min. The intervention group was previously instructed to inhale through their noses and exhale with their lips half-closed in time with the metronome sound. The patients in the control group were free to choose how to control their breathing. | Although changes in breathing pattern were obtained in the intervention group, the exercise duration and hyperinflation results were equivalent in both groups. After 12 weeks of the program, the intervention group showed a 9% increase in expiratory time, a 9% decrease in respiratory rate, and 3% dynamic hyperinflation. However, this improvement was minor and insufficient to associate exercise training with respiratory re-education using acoustic feedback with a metronome to increase exercise tolerance compared to exercise training alone. The conclusion of the training program was that both groups witnessed enhancements in dyspnea, fatigue, mental functions, and patient perception of disease control, alongside an increase in health-related quality of life. In both groups, patients reported a significant decrease in dyspnea when performing their activities of daily living, suggesting that changes in breathing patterns in the acoustic feedback training group had no impact on this symptom. |
| Authors: Tsang, E.W.; Kwok, H.; Chan, A.K.Y.; Choo, K.L.; Chan, K.S.; Lau, K.S.; Chan, C.C.H. (2018) [14] Title: Outcomes of community-based and home-based pulmonary rehabilitation for pneumoconiosis patients: a retrospective study. | To analyze the clinical benefits of pulmonary rehabilitation programs in the community and at home in patients with pneumoconiosis. | From a population of 685 patients with pneumoconiosis enrolled in community pulmonary rehabilitation (CPR) or home pulmonary rehabilitation programs (HPRP) offered by three hospitals in Hong Kong, 155 patients in CPR and 26 patients in HPRP were selected as the study sample. The mean age of the participants in CPR was 70.74 and that of the participants in HPRP was 74.54 years. | Data were grouped into 2 categories according to the following: (i) the demographic characteristics of the patients, specific information about the disease, and the program in which they participated (age, sex, degree of disability, body mass index, forced expiratory volume, and smoking history); (ii) the outcomes used to measure the benefits of pulmonary rehabilitation programs, through various scales, were the Chronic Respiratory Questionnaire (CRQ), Hospital Anxiety and Depression Scale (HADS)], Physical (PCS) and Mental (MCS) Health Scales Short Form-12 (SF-12), knowledge (included as an additional file to the article), and the 6-Min Walk Test (6MWT). | The findings of this study indicate that CPR had a beneficial impact on the patients’ overall well-being, leading to a decrease in psychological issues like anxiety and depression. Moreover, the assistance provided by healthcare practitioners, along with home visits and educational sessions for families, were factors linked to a reduction in depressive symptoms. Additionally, a strong correlation was observed between family involvement in these sessions and the improvement of patients’ understanding of the disease. As a result of participating in the program, patients experienced enhanced mobility and increased exercise capacity. Both pulmonary rehabilitation programs involved physical and respiratory training, increasing the patients’ levels of exercise tolerance. The effectiveness of the training period was found to be greater when it was extended, leading to improved physical capacity. During the hygiene education sessions, patients were educated on respiratory hygiene techniques, inhaler usage, and energy conservation methods. The outcomes indicated that patients enhanced their ability to manage their health and achieved higher levels of exercise tolerance. |
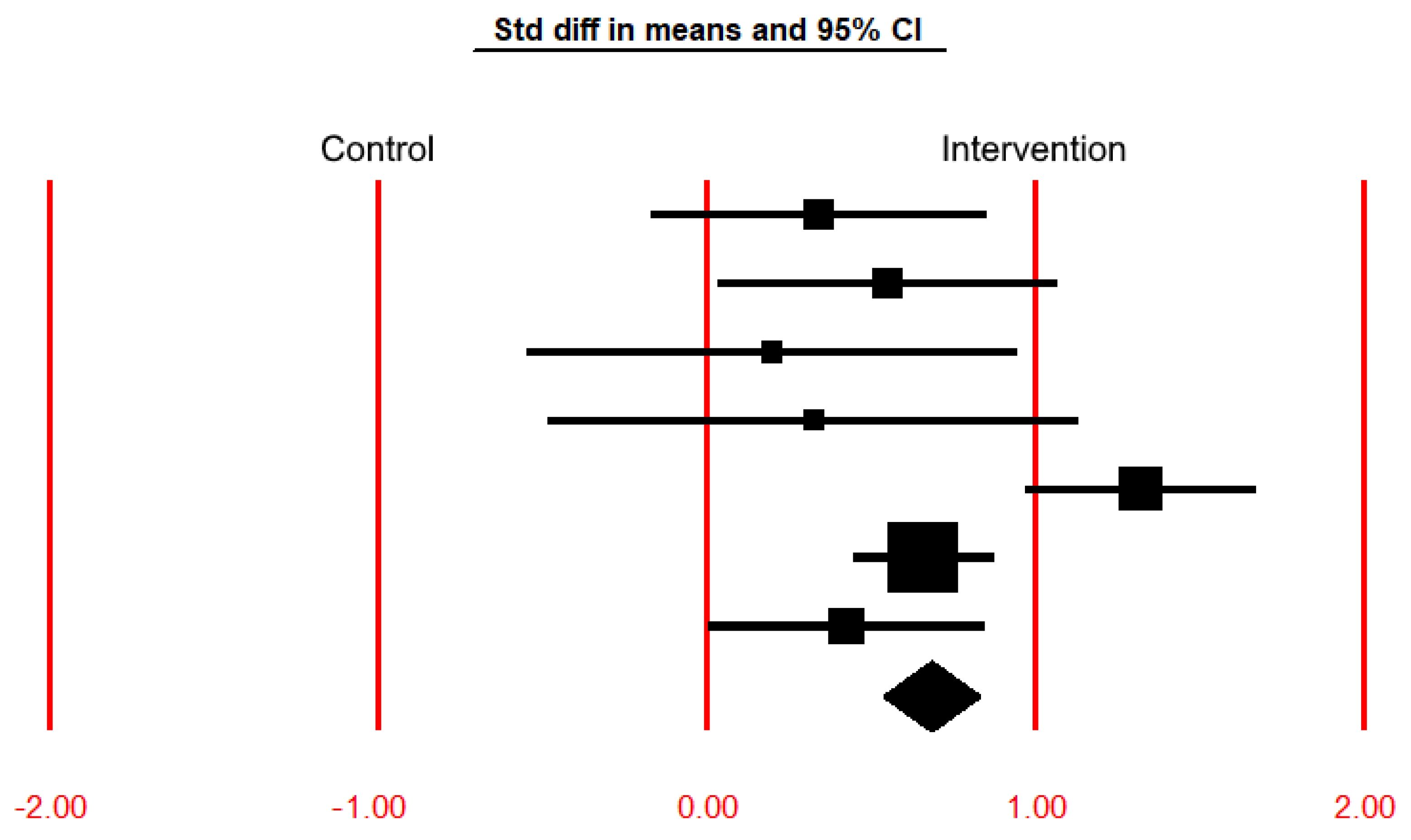
| Study Name | Std Diff in Means 1 | Standard Error | Variance | Lower Limit 2 | Upper Limit 3 | Z-Value | p-Value |
|---|---|---|---|---|---|---|---|
| Chung et al. [8]—BTE | 0.339 | 0.260 | 0.068 | −0.170 | 0.849 | 1.305 | 0.192 |
| Chung et al. [8]—IMT | 0.548 | 0.263 | 0.069 | 0.033 | 1.064 | 2.085 | 0.037 |
| Martin-Sanchez et al. [13]—IMT High | 0.199 | 0.379 | 0.144 | −0.544 | 0.941 | 0.525 | 0.600 |
| Martin-Sanchez et al. [13]—IMT Low | 0.324 | 0.411 | 0.169 | −0.482 | 1.129 | 0.787 | 0.431 |
| Wang et al. [9] | 1.321 | 0.178 | 0.032 | 0.972 | 1.669 | 7.425 | <0.001 |
| Tsang et al. [14]—CBRP | 0.658 | 0.108 | 0.012 | 0.447 | 0.870 | 6.097 | <0.001 |
| Tsang et al. [14]—HBRP | 0.423 | 0.213 | 0.045 | 0.005 | 0.840 | 1.983 | 0.047 |
| Fixed-effect model | 0.682 | 0.074 | 0.006 | 0.536 | 0.827 | 9.186 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ribeiro, R.; Oliveira, H.; Goes, M.; Gonçalves, C.; Dias, A.; Fonseca, C. The Effectiveness of Nursing Rehabilitation Interventions on Self-Care for Older Adults with Respiratory Disorders: A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 6422. https://doi.org/10.3390/ijerph20146422
Ribeiro R, Oliveira H, Goes M, Gonçalves C, Dias A, Fonseca C. The Effectiveness of Nursing Rehabilitation Interventions on Self-Care for Older Adults with Respiratory Disorders: A Systematic Review with Meta-Analysis. International Journal of Environmental Research and Public Health. 2023; 20(14):6422. https://doi.org/10.3390/ijerph20146422
Chicago/Turabian StyleRibeiro, Rita, Henrique Oliveira, Margarida Goes, Cátia Gonçalves, Ana Dias, and César Fonseca. 2023. "The Effectiveness of Nursing Rehabilitation Interventions on Self-Care for Older Adults with Respiratory Disorders: A Systematic Review with Meta-Analysis" International Journal of Environmental Research and Public Health 20, no. 14: 6422. https://doi.org/10.3390/ijerph20146422
APA StyleRibeiro, R., Oliveira, H., Goes, M., Gonçalves, C., Dias, A., & Fonseca, C. (2023). The Effectiveness of Nursing Rehabilitation Interventions on Self-Care for Older Adults with Respiratory Disorders: A Systematic Review with Meta-Analysis. International Journal of Environmental Research and Public Health, 20(14), 6422. https://doi.org/10.3390/ijerph20146422