

Lung and Colorectal Cancer Disparities in Appalachian Kentucky: Spatial Analysis on the Influence of Education and Literacy
 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Cancer Data
2.2. Education Data
2.3. Visualizations
2.4. Statistical Analysis
3. Results
3.1. Colorectal and Lung Cancer Incidence and Mortality between Appalachian and Non-Appalachian Populations in Kentucky
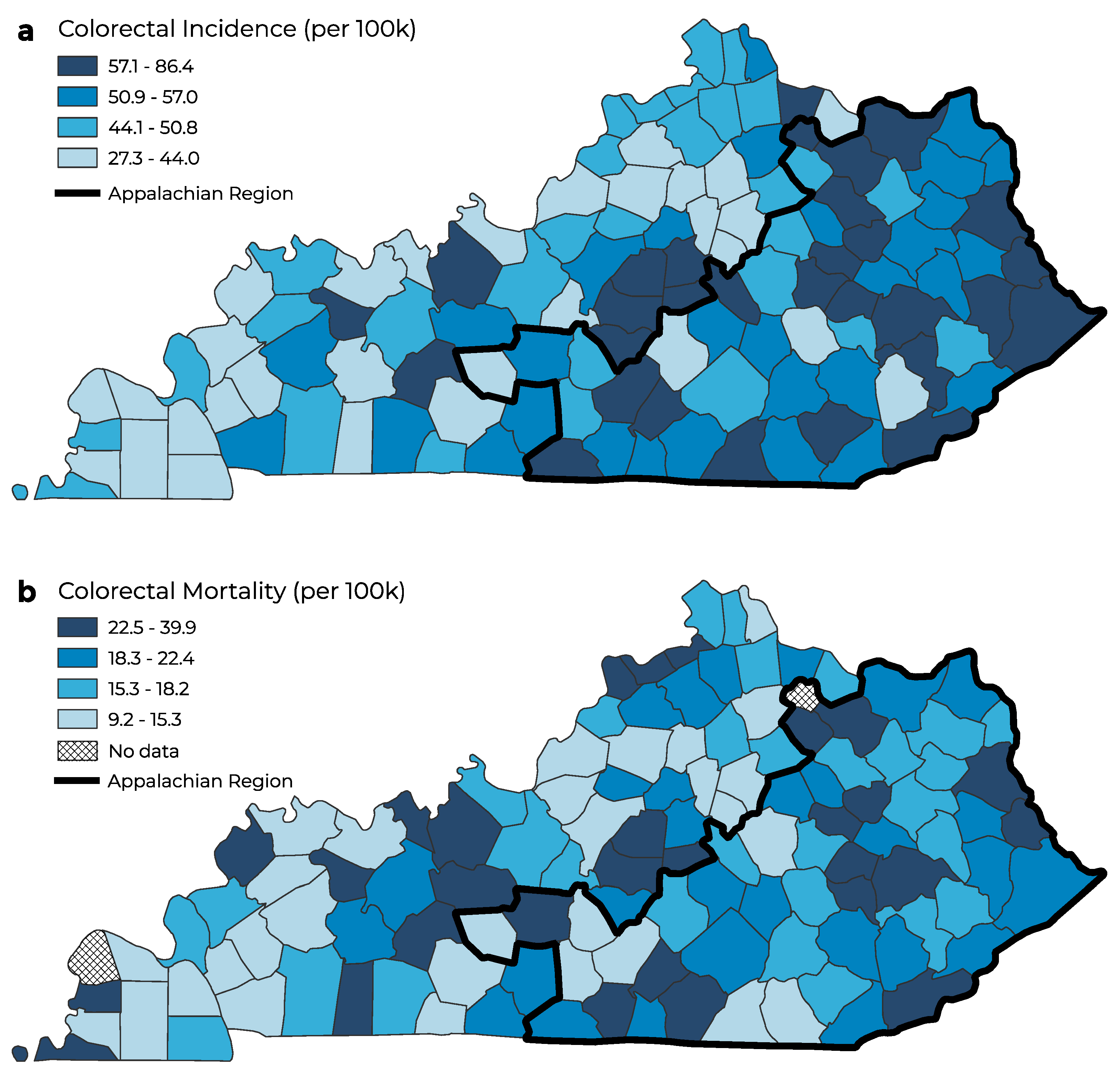
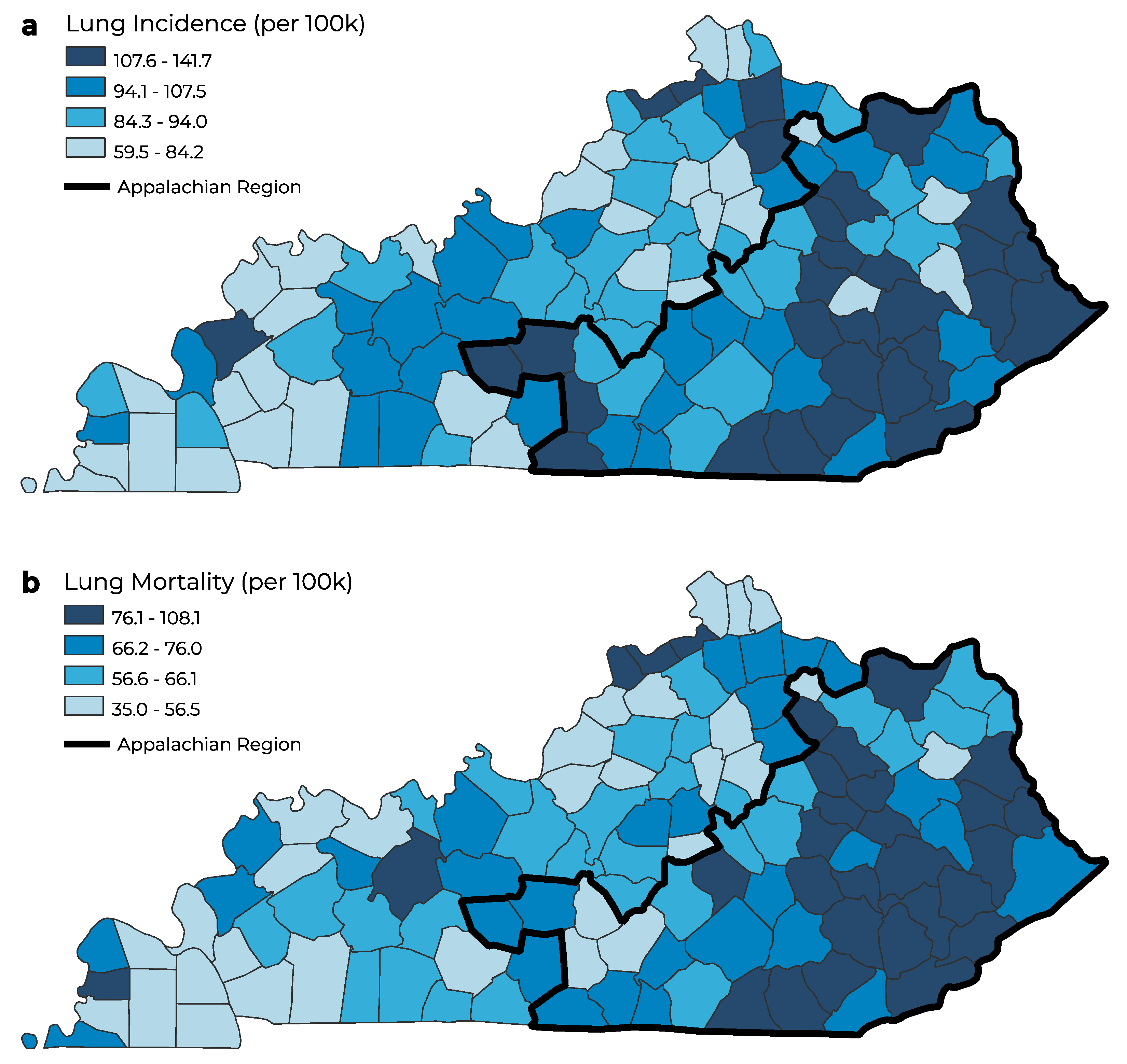
3.2. Colorectal and Lung Cancer Incidence and Mortality by Geographic Distribution
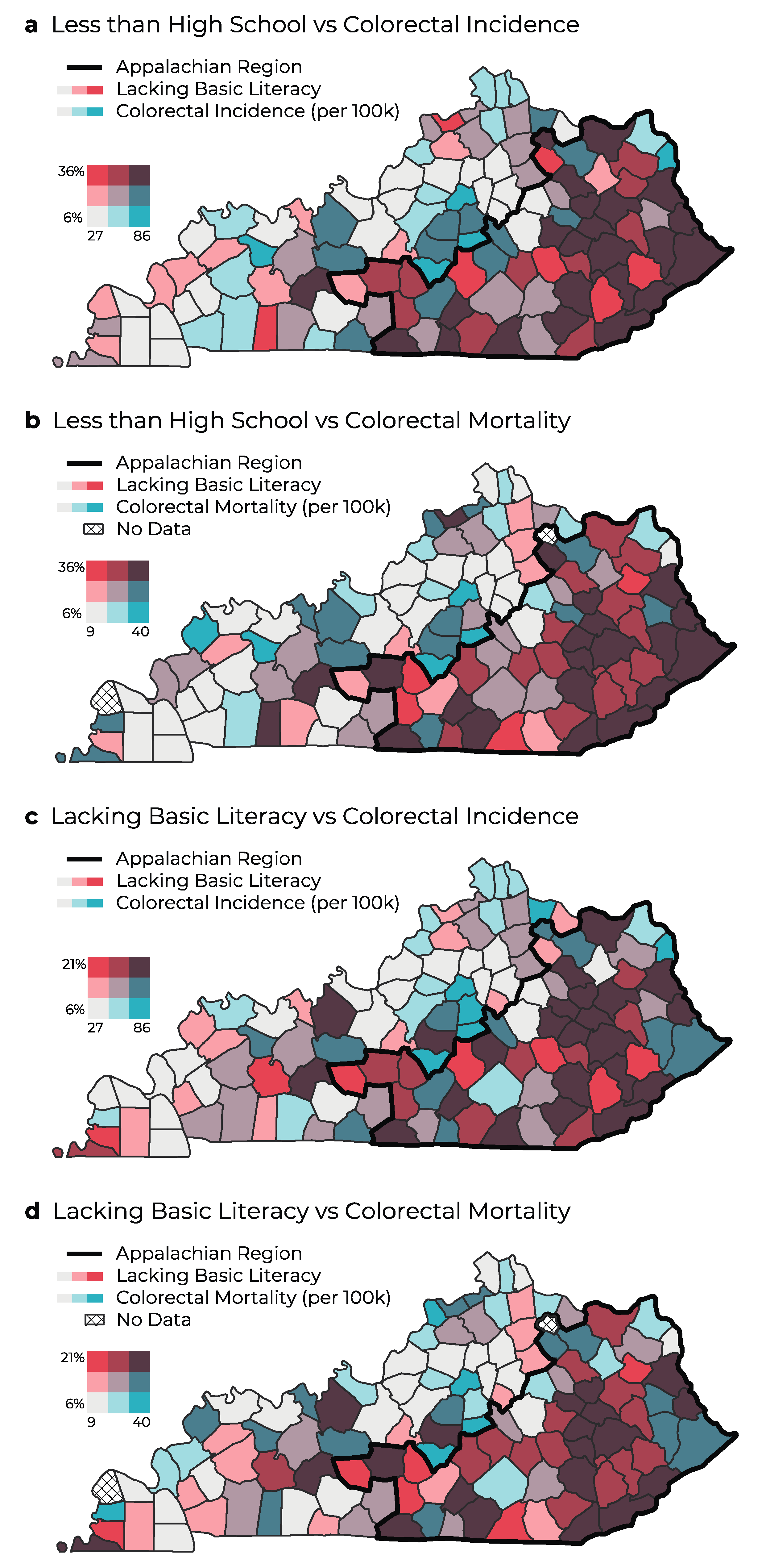
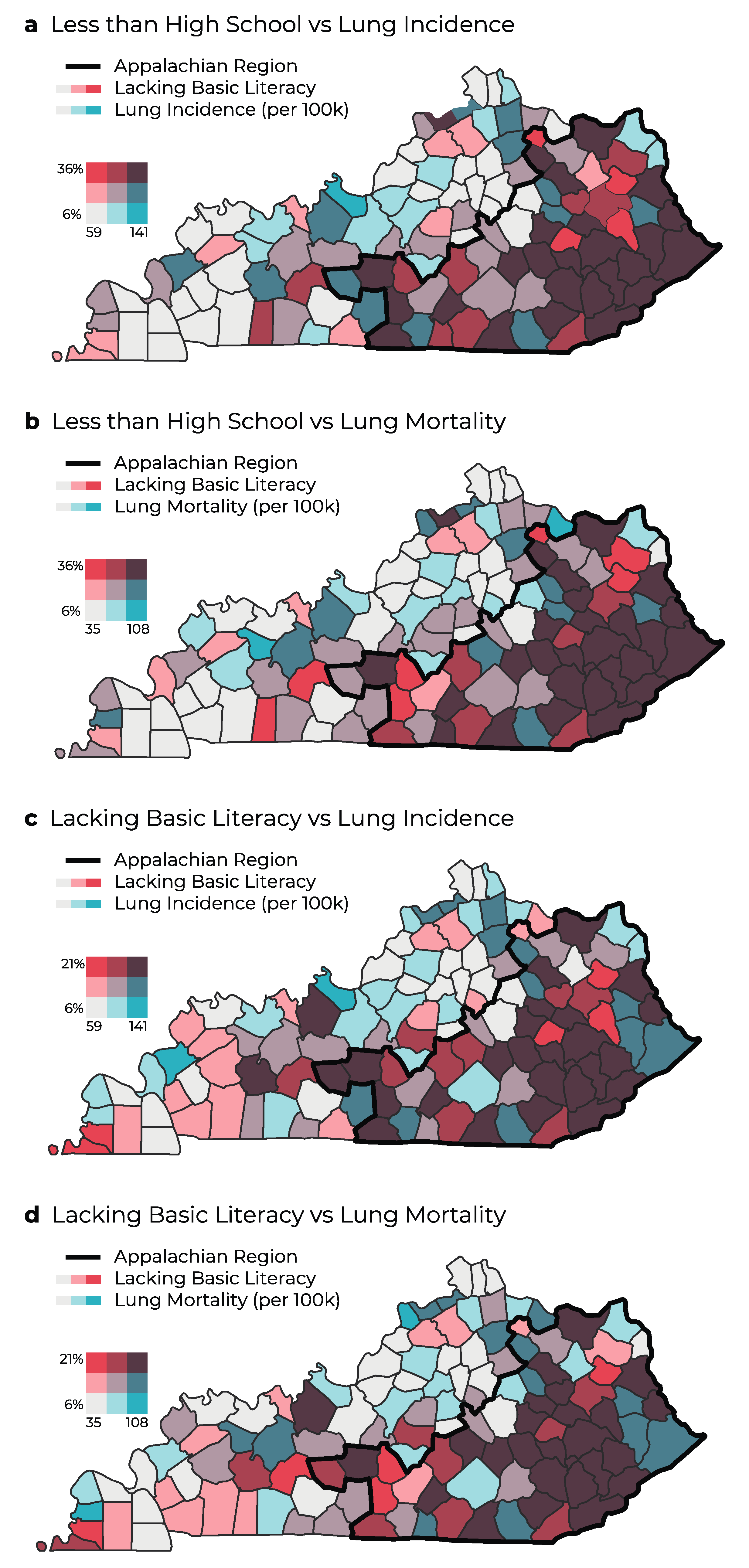
3.3. Cancer Rates and Educational Attainment in Appalachia Compared to Non-Appalachia Regions in Kentucky
3.4. Cancer Rates and Basic Literacy in Appalachia Compared to Non-Appalachia Regions in Kentucky
3.5. Simple Linear Regression Analysis
3.6. Spatial Regression Analysis
4. Discussion
4.1. Existing Research
4.2. Application of Findings
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Appalachian Regional Commission. The Appalachian Region. Available online: https://www.arc.gov/about-the-appalachian-region/ (accessed on 30 April 2022).
- Lengerich, E.J.; Tucker, T.C.; Powell, R.K.; Colsher, P.; Lehman, E.; Ward, A.J.; Siedlecki, J.C.; Wyatt, S.W. Cancer incidence in Kentucky, Pennsylvania, and West Virginia: Disparities in Appalachia. J. Rural Health 2005, 21, 39–47. [Google Scholar] [CrossRef]
- Pollard, K.; Jacobsen, L.A. The Appalachian Region: A Data Overview from the 2016–2020 American Community Survey Chartbook; Appalachian Regional Commission: Washington, DC, USA, 2022.
- Mokdad, A.H.; Dwyer-Lindgren, L.; Fitzmaurice, C.; Stubbs, R.W.; Bertozzi-Villa, A.; Morozoff, C.; Charara, R.; Allen, C.; Naghavi, M.; Murray, C.J. Trends and patterns of disparities in cancer mortality among US counties, 1980–2014. JAMA 2017, 317, 388–406. [Google Scholar] [CrossRef]
- Wilson, R.J.; Ryerson, A.B.; Singh, S.D.; King, J.B. Cancer Incidence in Appalachia, 2004–2011. Cancer Epidemiol. Biomark. Prev. 2016, 25, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Yao, N.; Alcalá, H.E.; Anderson, R.; Balkrishnan, R. Cancer disparities in rural Appalachia: Incidence, early detection, and survivorship. J. Rural Health 2017, 33, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Markey Cancer Center. Cancer Needs Assessment. Available online: https://www.kycancerneeds.org/ (accessed on 31 July 2022).
- Rodriguez, S.D.; Vanderford, N.L.; Huang, B.; Vanderpool, R.C. A social-ecological review of cancer disparities in Kentucky. South. Med. J. 2018, 111, 213–219. [Google Scholar] [CrossRef]
- American Cancer Society. Cancer Statistics Center. Available online: https://cancerstatisticscenter.cancer.org/#!/state/Kentucky (accessed on 30 April 2022).
- Elam, C. Culture, poverty and education in Appalachian Kentucky. Educ. Cult. 2012, 18, 10–13. [Google Scholar]
- Paskett, E.D.; Fisher, J.L.; Lengerich, E.J.; Schoenberg, N.E.; Kennedy, S.K.; Conn, M.E.; Roberto, K.A.; Dwyer, S.K.; Fickle, D.; Dignan, M. Disparities in underserved white populations: The case of cancer-related disparities in Appalachia. Oncologist 2011, 16, 1072–1081. [Google Scholar] [CrossRef] [PubMed]
- Albano, J.D.; Ward, E.; Jemal, A.; Anderson, R.; Cokkinides, V.E.; Murray, T.; Henley, J.; Liff, J.; Thun, M.J. Cancer mortality in the United States by education level and race. J. Natl. Cancer Inst. 2007, 99, 1384–1394. [Google Scholar] [CrossRef] [PubMed]
- McCann, A. Most & Least Educated States in America. Available online: https://wallethub.com/edu/e/most-educated-states/31075 (accessed on 3 May 2022).
- Appalachian Regional Commission. Social Determinants. In Creating Culture of Health in Appalachia; Appalachian Regional Commission: Washington, DC, USA, 2021; pp. 283–314. [Google Scholar]
- Appalachian Regional Commission. Education in Appalachia. Available online: https://www.arc.gov/education-in-appalachia/ (accessed on 30 April 2022).
- McConnell Parsons, J.R.; Hanley, C.; Prichard, C.; Vanderford, N.L. The Appalachian Career Training in Oncology (ACTION) Program: Preparing Appalachian Kentucky high school and undergraduate students for cancer careers. J. STEM Outreach 2021, 4, 1–14. [Google Scholar] [CrossRef]
- Kannapel, P.J.; Flory, M.A. Postsecondary transitions for youth in Appalachia’s Central Subregions: A review of education research, 1995–2015. J. Res. Rural Educ. 2017, 32, 1–17. [Google Scholar]
- Kutner, M.; Greenberg, E.; Ying, J.; Paulsen, C. The Health Literacy of America’s Adults: Results from the 2003 National Assessment of Adult Literacy; U.S. Department of Education; National Center for Education Statistics: Washington, DC, USA, 2006.
- Oldach, B.R.; Katz, M.L. Health literacy and cancer screening: A systematic review. Patient Educ. Couns. 2014, 94, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Samoil, D.; Kim, J.; Fox, C.; Papadakos, J.K. The importance of health literacy on clinical cancer outcomes: A scoping review. Ann. Cancer Epidemiol. 2021, 5, 3. [Google Scholar] [CrossRef]
- Berkman, N.; Dewalt, D.; Pignone, M.; Sheridan, S.; Lohr, K.; Lux, L.; Sutton, S.; Swinson, T.; Bonito, A. AHRQ Evidence Report Summaries; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2004.
- Holden, C.E.; Wheelwright, S.; Harle, A.; Wagland, R. The role of health literacy in cancer care: A mixed studies systematic review. PLoS ONE 2021, 16, e0259815. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Economic Research Service. Rural-Urban Continuum Codes. Available online: https://www.ers.usda.gov/data-products/rural-urban-continuum-codes/ (accessed on 30 April 2022).
- Robertson, N.M.; Hudson, L.; Attia, S.L.; Porterfield, J.Z.; Vanderford, N.L. Assessing the effectiveness of cancer screening interventions targeting Appalachian populations: A systematic review. J. Rural Health 2021, 37, 602–623. [Google Scholar] [CrossRef]
- Fay, M.P.; Tiwari, R.C.; Feuer, E.J.; Zou, Z. Estimating average annual percent change for disease rates without assuming constant change. Biometrics 2006, 62, 847–854. [Google Scholar] [CrossRef]
- Anselin, L.; Rey, S. Properties of Tests for Spatial Dependence in Linear Regression Models. Geogr. Anal. 1991, 23, 112–131. [Google Scholar] [CrossRef]
- National Cancer Institute. SEER*Stat Software Version 8.3.9; National Cancer Institute: Bethesda, MD, USA, 2021.
- Kuo, T.M.; Meyer, A.M.; Baggett, C.D.; Olshan, A.F. Examining determinants of geographic variation in colorectal cancer mortality in North Carolina: A spatial analysis approach. Cancer Epidemiol. 2019, 59, 8–14. [Google Scholar] [CrossRef]
- Rakhshkhorshid, M.; Navaee, M.; Nouri, N.; Safarzaii, F. The association of health literacy with breast cancer knowledge, perception and screening behavior. Eur. J. Breast Health 2018, 14, 144–147. [Google Scholar] [CrossRef]
- Islami, F.; Ward, E.M.; Jacobs, E.J.; Ma, J.; Goding Sauer, A.; Lortet-Tieulent, J.; Jemal, A. Potentially preventable premature lung cancer deaths in the USA if overall population rates were reduced to those of educated whites in lower-risk states. Cancer Causes Control 2015, 26, 409–418. [Google Scholar] [CrossRef]
- Centers for Disease Control & Prevention. Smoking and Tobacco Use. Available online: https://www.cdc.gov/tobacco/stateandcommunity/state-fact-sheets/index.htm (accessed on 3 May 2022).
- Ryan, B.M. Lung cancer health disparities. Carcinogenesis 2018, 39, 741–751. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Fang, Y.J.; Abulimiti, A.; Huang, C.Y.; Liu, K.Y.; Chen, Y.M.; Zhang, C.X. Educational level and colorectal cancer risk: The mediating roles of lifestyle and dietary factors. Eur. J. Cancer Prev. 2022, 31, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Callahan, K.; Sy, F.; Siweya, A.; Pinheiro, P.; Ponce, C. Variation in the association between education and colorectal cancer mortality by race/ethnicity. In Proceedings of the American Public Health Association, Philadelphia, PA, USA, 2–6 November 2019. [Google Scholar]
- Morris, N.S.; Field, T.S.; Wagner, J.L.; Cutrona, S.L.; Roblin, D.W.; Gaglio, B.; Williams, A.E.; Han, P.J.; Costanza, M.E.; Mazor, K.M. The association between health literacy and cancer-related attitudes, behaviors, and knowledge. J. Health Commun. 2013, 18 (Suppl. S1), 223–241. [Google Scholar] [CrossRef]
- Charlton, M.; Schlichting, J.; Chioreso, C.; Ward, M.; Vikas, P. Challenges of rural cancer care in the United States. Oncology 2015, 29, 633–640. [Google Scholar]
- Hudson, L.; Prichard, C.; Weiss, L.T.; Vanderford, N.L. Evidence for cancer literacy knowledge retention among Kentucky middle and high school students after a brief educational intervention. South. Med. J. 2020, 113, 541–548. [Google Scholar] [CrossRef]
- Hudson, L.; Samons, K.M.; Dicken, H.E.; Prichard, C.; Weiss, L.T.; Edward, J.; Vanderpool, R.C.; Vanderford, N.L. A brief educational intervention enhances basic cancer literacy among Kentucky middle and high school students. J. Cancer Educ. 2021, 36, 735–740. [Google Scholar] [CrossRef]
- Hudson, L.; Sharp, K.; Prichard, C.; Ickes, M.; Alameh, S.; Vanderford, N.L. Cancer curriculum for Appalachian Kentucky middle and high schools. J. Appalach. Health 2021, 3, 43–55. [Google Scholar] [CrossRef]
- Idrovo, A.J. Three criteria for ecological fallacy. Environ. Health Perspect. 2011, 119, A332. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measure | Site | Appl KY Rate | Non-Appl KY Rate | Rate Ratio (Ref. Non-Appl KY) | % Higher in Appl KY |
|---|---|---|---|---|---|
| Incidence | All Site | 538.6 | 510.0 | 1.06 *** | 5.60 |
| Colorectal | 54.8 | 45.4 | 1.21 *** | 20.70 | |
| Lung | 105.3 | 82.4 | 1.28 *** | 27.79 | |
| Mortality | All Site | 172.3 | 153.8 | 1.12 *** | 12.02 |
| Colorectal | 15.3 | 13.5 | 1.13 *** | 13.33 | |
| Lung | 48.4 | 37.5 | 1.29 *** | 29.07 |
| Age-Adjusted Cancer Rates per 100,000 People | Cancer Site | Did Not Complete High School | Lacking Basic Literacy | ||||
|---|---|---|---|---|---|---|---|
| Coef | Std Coef | R² | Coef | Std Coef | R² | ||
| Incidence | Colorectal | 0.62 *** | 0.37 *** | 13.9% | 1.35 *** | 0.39 *** | 14.9% |
| Lung | 1.69 *** | 0.61 *** | 37.6% | 3.05 *** | 0.53 *** | 27.7% | |
| Mortality | Colorectal | 0.30 *** | 0.37 *** | 14.0% | 0.58 *** | 0.34 *** | 11.8% |
| Lung | 1.45 *** | 0.64 *** | 40.8% | 2.78 *** | 0.58 *** | 34.1% | |
| Age-Adjusted Cancer Rates per 100,000 People | Cancer Site | Did Not Complete High School | Lacking Basic Literacy | ||||
|---|---|---|---|---|---|---|---|
| Coef | Std Coef | Spatial Parameter | Coef | Std Coef | Spatial Parameter | ||
| Incidence | Colorectal | 0.47 *** | 0.29 *** | 0.30 * | 1.07 *** | 0.31 *** | 0.31 ** |
| Lung | 1.36 *** | 0.50 *** | 0.28 * | 2.23 *** | 0.38 *** | 0.40 *** | |
| Mortality | Colorectal | 0.27 *** | 0.34 *** | 0.16 | 0.51 *** | 0.30 *** | 0.20 |
| Lung | 1.16 *** | 0.51 *** | 0.28 * | 2.09 *** | 0.44 *** | 0.38 *** | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robertson, N.M.; Burus, T.; Hudson, L.; Hull, P.C.; Park, L.; Vanderford, N.L. Lung and Colorectal Cancer Disparities in Appalachian Kentucky: Spatial Analysis on the Influence of Education and Literacy. Int. J. Environ. Res. Public Health 2023, 20, 6363. https://doi.org/10.3390/ijerph20146363
Robertson NM, Burus T, Hudson L, Hull PC, Park L, Vanderford NL. Lung and Colorectal Cancer Disparities in Appalachian Kentucky: Spatial Analysis on the Influence of Education and Literacy. International Journal of Environmental Research and Public Health. 2023; 20(14):6363. https://doi.org/10.3390/ijerph20146363
Chicago/Turabian StyleRobertson, Nicole M., Todd Burus, Lauren Hudson, Pamela C. Hull, Lee Park, and Nathan L. Vanderford. 2023. "Lung and Colorectal Cancer Disparities in Appalachian Kentucky: Spatial Analysis on the Influence of Education and Literacy" International Journal of Environmental Research and Public Health 20, no. 14: 6363. https://doi.org/10.3390/ijerph20146363
APA StyleRobertson, N. M., Burus, T., Hudson, L., Hull, P. C., Park, L., & Vanderford, N. L. (2023). Lung and Colorectal Cancer Disparities in Appalachian Kentucky: Spatial Analysis on the Influence of Education and Literacy. International Journal of Environmental Research and Public Health, 20(14), 6363. https://doi.org/10.3390/ijerph20146363