
Complex Sex Differences in Life Expectancy in French Guiana

 ,
,  ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Methods
2.1. Data Sources
2.2. Statistical Methods
3. Results
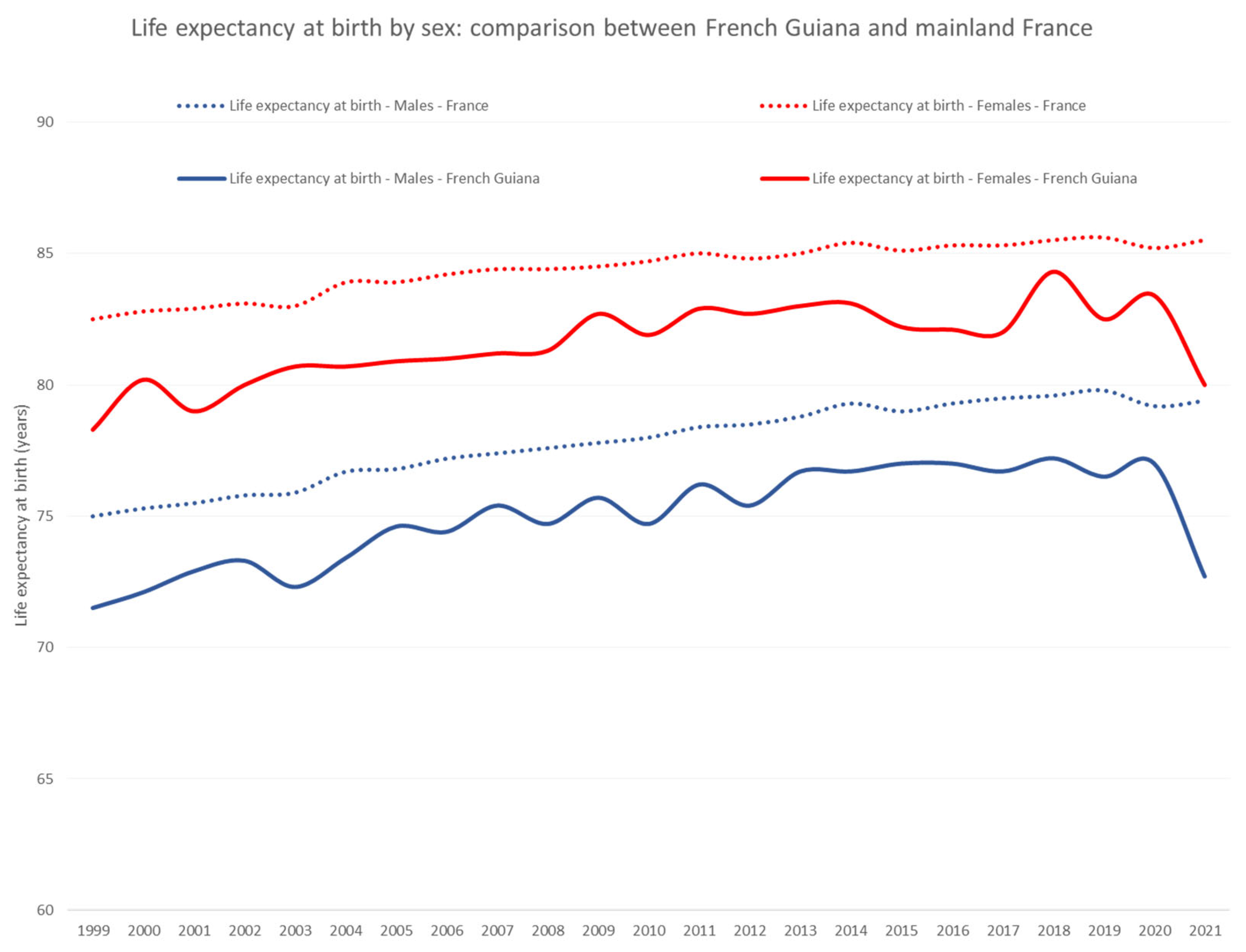
3.1. Life Expectancy at Birth
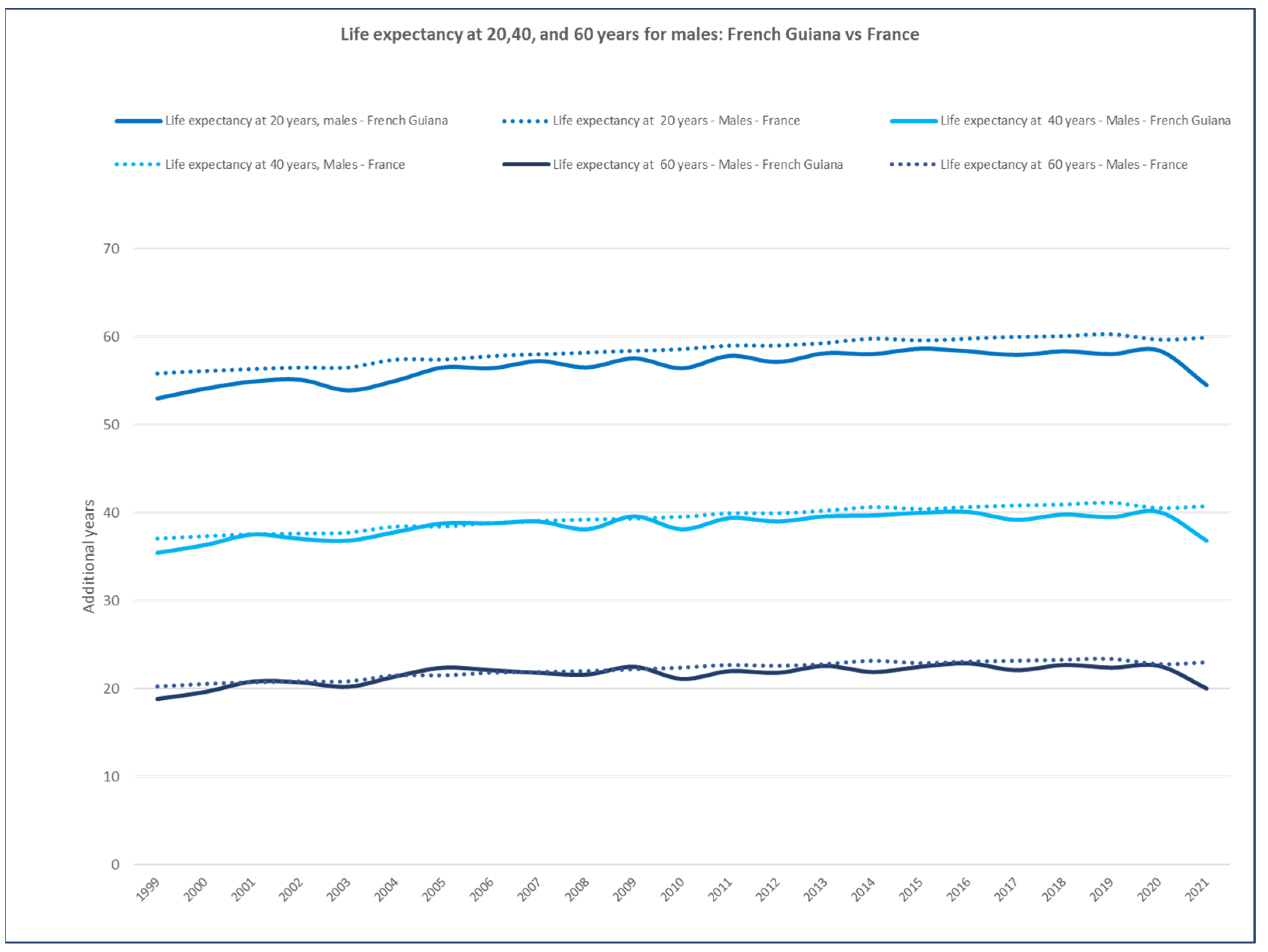
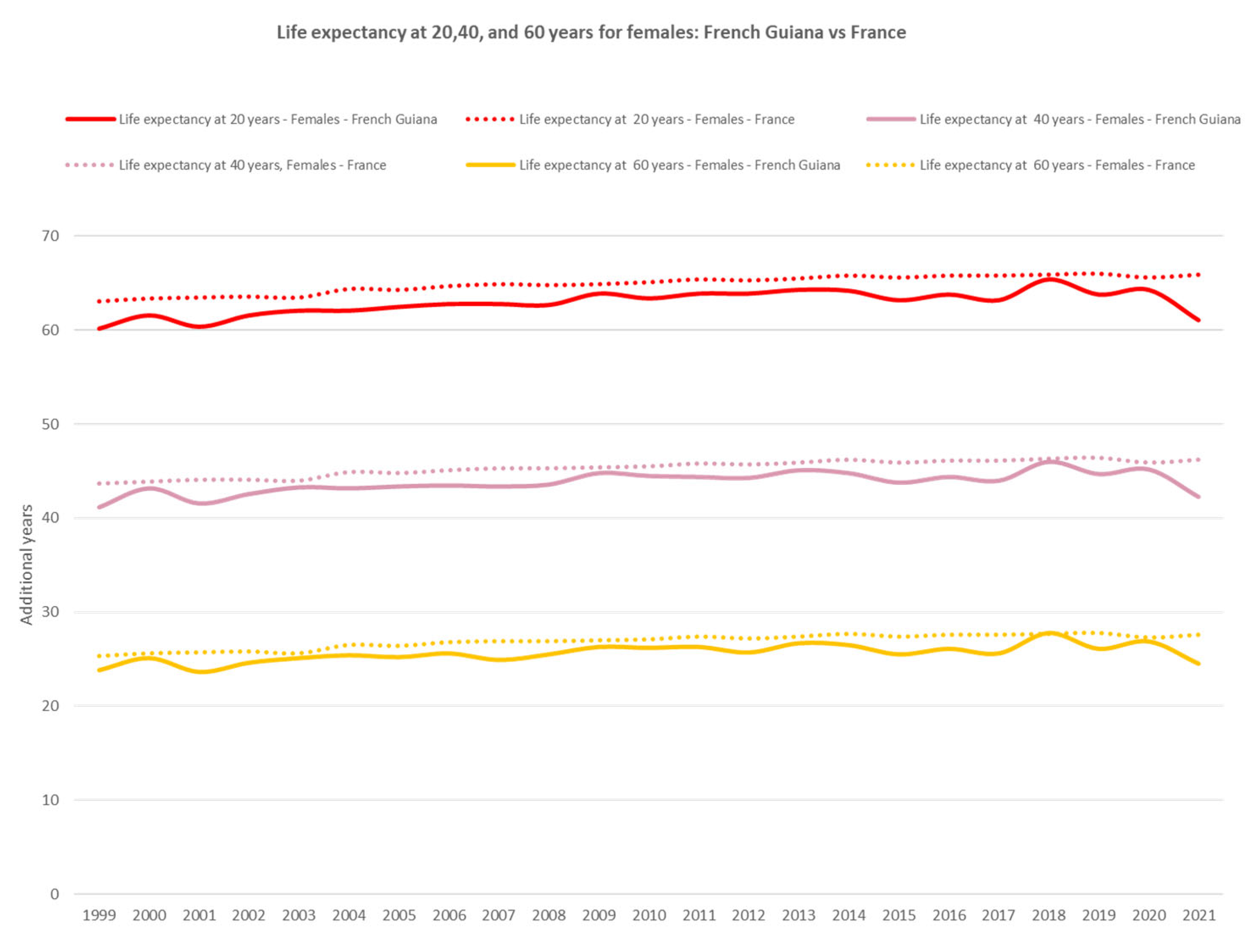
3.2. At 20, 40, and 60 Years
3.3. Poor versus Rich
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Deparcieux, A. Essai Sur Les Probabilités de La Durée de La Vie Humaine: D’où l’on Déduit La Manière de Déterminer Les Rentes Viagères, Tant Simples Qu’en Tontines; Guérin frères: Paris, French, 1746. [Google Scholar]
- Aden, A.S.; Omar, M.M.; Omar, H.M.; Högberg, U.; Persson, L.Å.; Wall, S. Excess Female Mortality in Rural Somalia—Is Inequality in the Household a Risk Factor? Soc. Sci. Med. 1997, 44, 709–715. [Google Scholar] [CrossRef]
- Barford, A.; Dorling, D.; Smith, G.D.; Shaw, M. Life Expectancy: Women Now on Top Everywhere. BMJ 2006, 332, 808. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef] [PubMed]
- Owens, I.P.F. Sex Differences in Mortality Rate. Science 2002, 297, 2008–2009. [Google Scholar] [CrossRef] [PubMed]
- Palmisano, B.T.; Zhu, L.; Eckel, R.H.; Stafford, J.M. Sex differences in lipid and lipoprotein metabolism. Mol. Metab. 2018, 15, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Waldron, I. Sex differences in human mortality: The role of genetic factors. Soc. Sci. Med. 1983, 17, 321–333. [Google Scholar] [CrossRef]
- Luy, M.; Gast, K. Do Women Live Longer or Do Men Die Earlier? Reflections on the Causes of Sex Differences in Life Expectancy. Gerontology 2014, 60, 143–153. [Google Scholar] [CrossRef]
- Lemaire, J. Why Do Females Live Longer than Males? N. Am. Actuar. J. 2002, 6, 21–37. [Google Scholar] [CrossRef]
- Andrade, F.C.D.; Guevara, P.E.; Lebrão, M.L.; Duarte, Y.A.d.O.; Santos, J.L.F. Gender Differences in Life Expectancy and Disability-Free Life Expectancy among Older Adults in São Paulo, Brazil. Women’s Health Issues 2011, 21, 64–70. [Google Scholar] [CrossRef]
- Di Lego, V.; Di Giulio, P.; Luy, M. Gender Differences in Healthy and Unhealthy Life Expectancy. In International Handbook of Health Expectancies; International Handbooks of Population; Jagger, C., Crimmins, E.M., Saito, Y., De Carvalho Yokota, R.T., Van Oyen, H., Robine, J.-M., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 151–172. ISBN 978-3-030-37668-0. [Google Scholar]
- Article—Bulletin Épidémiologique Hebdomadaire. Available online: http://beh.santepubliquefrance.fr/beh/2020/2-3/2020_2-3_1.html (accessed on 16 November 2022).
- Dossier Complet—Département de La Guyane (973)|Insee. Available online: https://www.insee.fr/fr/statistiques/2011101?geo=DEP-973 (accessed on 15 November 2022).
- Rochemont, D.R.; Mimeau, E.; Misslin, C.; Papaix-Puech, M.; De Toffol, B.; Sabbah, N.; Delmas, E.; Bejot, Y.; Fournel, I.; Nacher, M. A Prospective Comparative Study of Health Inequalities and the Epidemiology of Stroke in French Guiana and Dijon, France. Front. Public Health 2022, 10, 849036. [Google Scholar] [CrossRef]
- Van Melle, A.; Cropet, C.; Parriault, M.-C.; Adriouch, L.; Lamaison, H.; Sasson, F.; Duplan, H.; Richard, J.-B.; Nacher, M. Renouncing care in French Guiana: The national health barometer survey. BMC Health Serv. Res. 2019, 19, 99. [Google Scholar] [CrossRef] [PubMed]
- Valmy, L.; Gontier, B.; Parriault, M.C.; Van Melle, A.; Pavlovsky, T.; Basurko, C.; Grenier, C.; Douine, M.; Adenis, A.; Nacher, M. Prevalence and predictive factors for renouncing medical care in poor populations of Cayenne, French Guiana. BMC Health Serv. Res. 2015, 16, 34. [Google Scholar] [CrossRef] [PubMed]
- Linière, S.; Nacher, M.; Drak Alsibai, K.; Mergeayfabre, M.; Hafsi, N.; Charpin, A.; Misslin-Tritsch, C.; Carod, J.-F.; Aurelus, J.M.; De Toffol, B.; et al. Precariousness, Diabetes Control and Complications in French Guiana. Front. Endocrinol. 2022, 13, 937156. [Google Scholar] [CrossRef]
- Massicard, M.; Drak Alsibai, K.; Nacher, M.; Sabbah, N. Nutritional and Socioeconomic Determinants of Overweight and Obesity in the French Amazon: The Health Barometer Study. Front. Endocrinol. 2022, 13, 849718. [Google Scholar] [CrossRef] [PubMed]
- Interroger Les Données de Mortalité|CépiDc. Available online: https://www.cepidc.inserm.fr/causes-medicales-de-deces/interroger-les-donnees-de-mortalite (accessed on 15 November 2022).
- Our World in Data. Available online: https://ourworldindata.org (accessed on 15 November 2022).
- SPF Premiers Résultats du Baromètre Santé DOM 2014—Guyane. Available online: https://www.santepubliquefrance.fr/guyane/premiers-resultats-du-barometre-sante-dom-2014-guyane (accessed on 13 December 2022).
- Guarmit, B.; Brousse, P.; Lucarelli, A.; Donutil, G.; Cropet, C.; Mosnier, E.; Travers, P.; Nacher, M. Descriptive epidemiology of suicide attempts and suicide in the remote villages of French Guiana. Soc. Psychiatry 2018, 53, 1197–1206. [Google Scholar] [CrossRef] [PubMed]
- Pacot, R.; Garmit, B.; Pradem, M.; Nacher, M.; Brousse, P. The problem of suicide among Amerindians in Camopi-Trois Sauts, French Guiana 2008–2015. BMC Psychiatry 2018, 18, 99. [Google Scholar] [CrossRef]
- Shalev, V.; Chodick, G.; Heymann, A.; Kokia, E. Gender differences in healthcare utilization and medical indicators among patients with diabetes. Public Health 2005, 119, 45–49. [Google Scholar] [CrossRef]
- Muennig, P.; Lubetkin, E.; Jia, H.; Franks, P. Gender and the Burden of Disease Attributable to Obesity. Am. J. Public Health 2006, 96, 1662–1668. [Google Scholar] [CrossRef]
- Kautzky-Willer, A.; Harreiter, J. Sex and gender differences in therapy of type 2 diabetes. Diabetes Res. Clin. Pract. 2017, 131, 230–241. [Google Scholar] [CrossRef]
- Pino-Domínguez, L.; Navarro-Gil, P.; González-Vélez, A.E.; Prieto-Flores, M.-E.; Ayala, A.; Rojo-Pérez, F.; Fernández-Mayoralas, G.; Martínez-Martín, P.; Forjaz, M.J. Self-perceived health status, gender, and work status. J. Women Aging 2016, 28, 386–394. [Google Scholar] [CrossRef]
- Duclau, A.; Abad, F.; Adenis, A.; Sabbah, N.; Leneuve, M.; Nacher, M. Prevalence and Risk Factors for Micronutrient Deficiencies during Pregnancy in Cayenne, French Guiana. Food Nutr. Res. 2021, 65, 5268. [Google Scholar] [CrossRef] [PubMed]
- Basurko, C.; Dupart, O.; Savy, M.; Obert-Marby, C.; Mvogo, A.; Gonzalez, A.; Trepont, A.; Cann, L.; Boceno, C.; Osei, L.; et al. Hunger in French Guiana’s Vulnerable Urban Neighborhoods: A Neglected Consequence of COVID-19. Food Nutr. Bull. 2023, 44, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Kobylińska, M.; Antosik, K.; Decyk, A.; Kurowska, K. Malnutrition in Obesity: Is It Possible? Obes. Facts 2021, 15, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Ordovás, J.M.; Smith, C.E. Epigenetics and cardiovascular disease. Nat. Rev. Cardiol. 2010, 7, 510–519. [Google Scholar] [CrossRef]
- Gomez-Verjan, J.C.; Barrera-Vázquez, O.S.; García-Velázquez, L.; Samper-Ternent, R.; Arroyo, P. Epigenetic Variations Due to Nutritional Status in Early-Life and Its Later Impact on Aging and Disease. Clin. Genet. 2020, 98, 313–321. [Google Scholar] [CrossRef]
- Cet Hôpital est un Mouroir. Available online: https://www.guadeloupe.franceantilles.fr/cet-hopital-est-un-mouroir-753184.php (accessed on 16 November 2022).












Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nacher, M.; Basurko, C.; Imounga, L.M.; Wang, Q.; Van Melle, A.; Lucarelli, A.; Adenis, A.; Alsibai, K.D.; Hcini, N.; Sabbah, N. Complex Sex Differences in Life Expectancy in French Guiana. Int. J. Environ. Res. Public Health 2023, 20, 6195. https://doi.org/10.3390/ijerph20136195
Nacher M, Basurko C, Imounga LM, Wang Q, Van Melle A, Lucarelli A, Adenis A, Alsibai KD, Hcini N, Sabbah N. Complex Sex Differences in Life Expectancy in French Guiana. International Journal of Environmental Research and Public Health. 2023; 20(13):6195. https://doi.org/10.3390/ijerph20136195
Chicago/Turabian StyleNacher, Mathieu, Célia Basurko, Laure Manuella Imounga, Qiannan Wang, Astrid Van Melle, Aude Lucarelli, Antoine Adenis, Kinan Drak Alsibai, Najeh Hcini, and Nadia Sabbah. 2023. "Complex Sex Differences in Life Expectancy in French Guiana" International Journal of Environmental Research and Public Health 20, no. 13: 6195. https://doi.org/10.3390/ijerph20136195
APA StyleNacher, M., Basurko, C., Imounga, L. M., Wang, Q., Van Melle, A., Lucarelli, A., Adenis, A., Alsibai, K. D., Hcini, N., & Sabbah, N. (2023). Complex Sex Differences in Life Expectancy in French Guiana. International Journal of Environmental Research and Public Health, 20(13), 6195. https://doi.org/10.3390/ijerph20136195