
Standardised 25-Step Traditional Thai Massage (TTM) Protocol for Treating Office Syndrome (OS)

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design of the 25-Step Protocol
2.2. Investigation of the Efficacy of the 25-Step Protocol
2.3. Recruitment of Therapists and Patients and Treatment with TTM
2.4. Outcome Measures
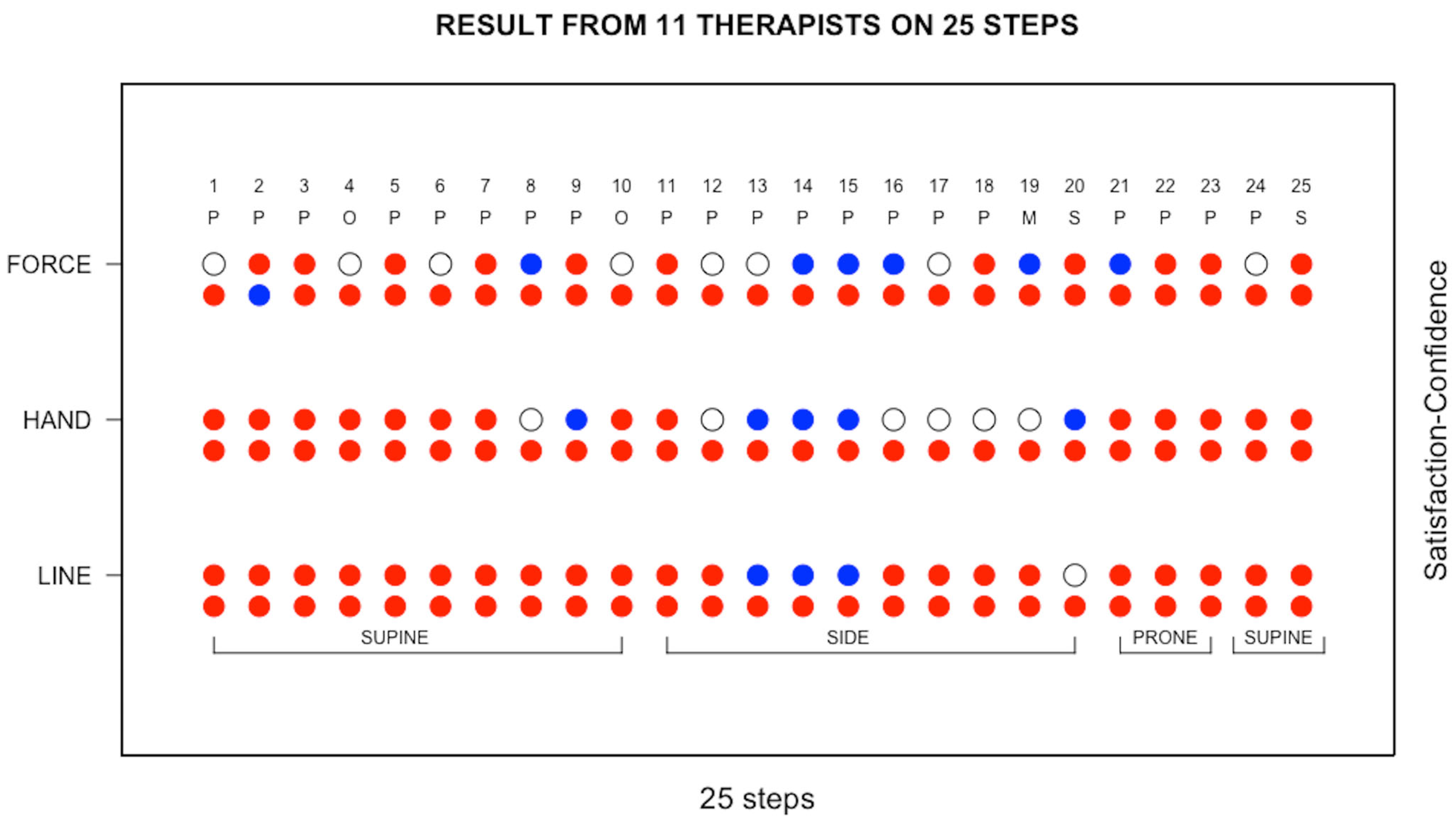
- For each of the 25 steps, each TTM therapist provided responses on a 3-point Likert scale regarding whether they considered that they had learned the specific action to be performed in terms of (a) the Sen Seb line to be followed, (b) the hand and body position to adopt, and (c) the force to apply;
- For each of the 25 steps, each TTM therapist provided responses on a 3-point Likert scale regarding whether they felt confident to be able to deliver the treatment in terms of (a) the Sen Seb line to be followed, (b) the hand and body position to adopt, and (c) the force to apply;
- Each TTM therapist was asked if there were any recommendations that they would like to make;
- Each OS patient provided responses on Likert’s 3-point scale for 9 items regarding whether they were satisfied with the TTM treatment they received;
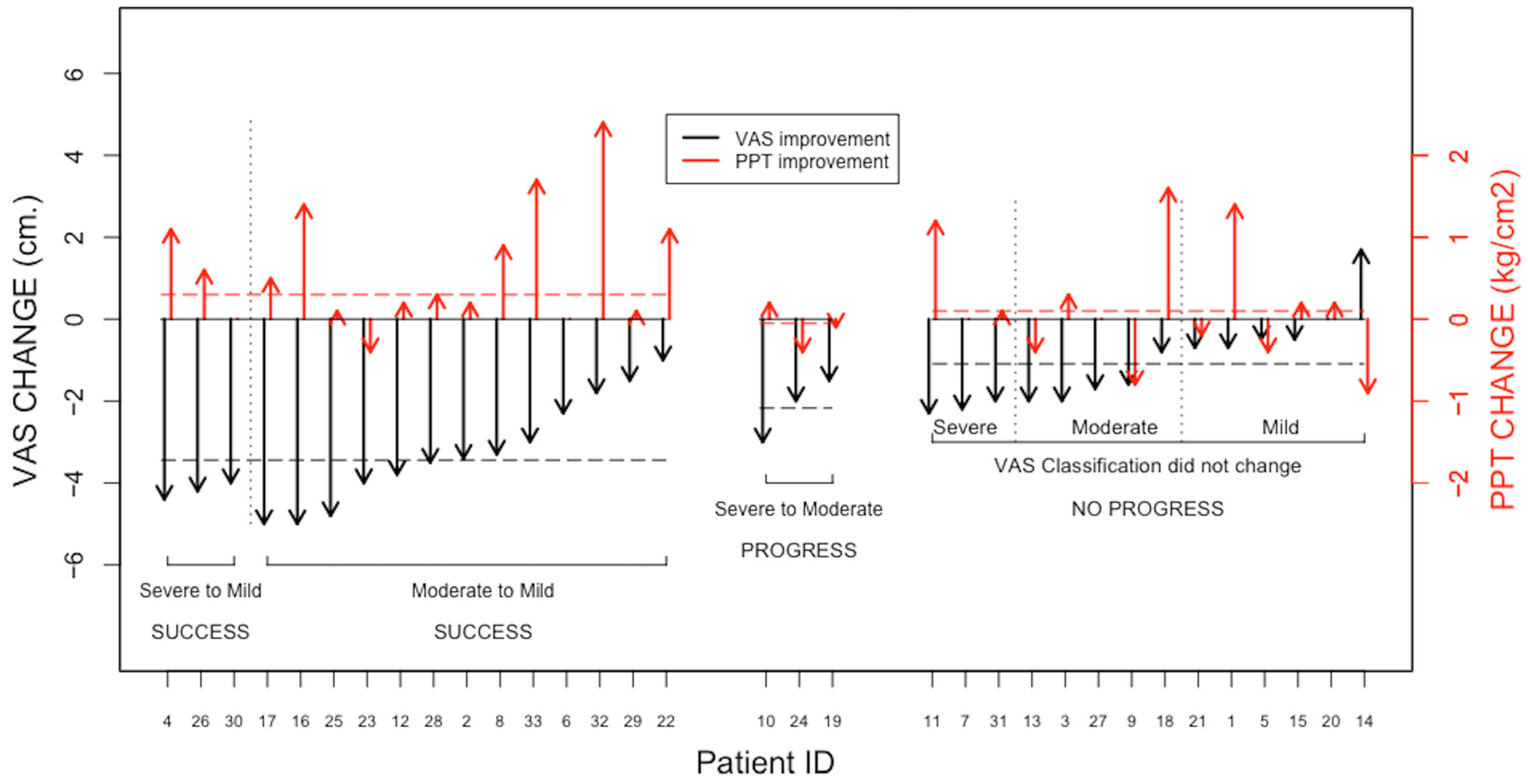
- For each OS patient, prior to treatment and again immediately following treatment several outcome measurements were recorded. These were the intensity of the pain which they were currently experiencing as measured using a numerical VAS scale, ranging from 0 to 10 cm, with 0 corresponding to no pain anywhere and 10 corresponding to the worst pain imaginable, and PPT was measured using a pressure algometry (OE-220, ITO Co., Ltd., Tokyo, Japan) for the central part of upper trapezius muscle on the most painful side. The intra-rater repeatability and inter-rater reproducibility of the PPT measurements were tested in 28 volunteers before recruiting the participants. The results showed that the ICC was 0.94 (p < 0.001) and 0.97 (p < 0.001), respectively;
- Each OS patient was asked to report any side effects, such as slight bruising, mild headache, tiredness, increased discomfort or soreness, that were present immediately after receiving treatment and one day later;
- Each OS patient was asked if there were any recommendations that they would like to make.
2.5. Statistical Analysis
3. Results
3.1. Participants
3.1.1. Therapists
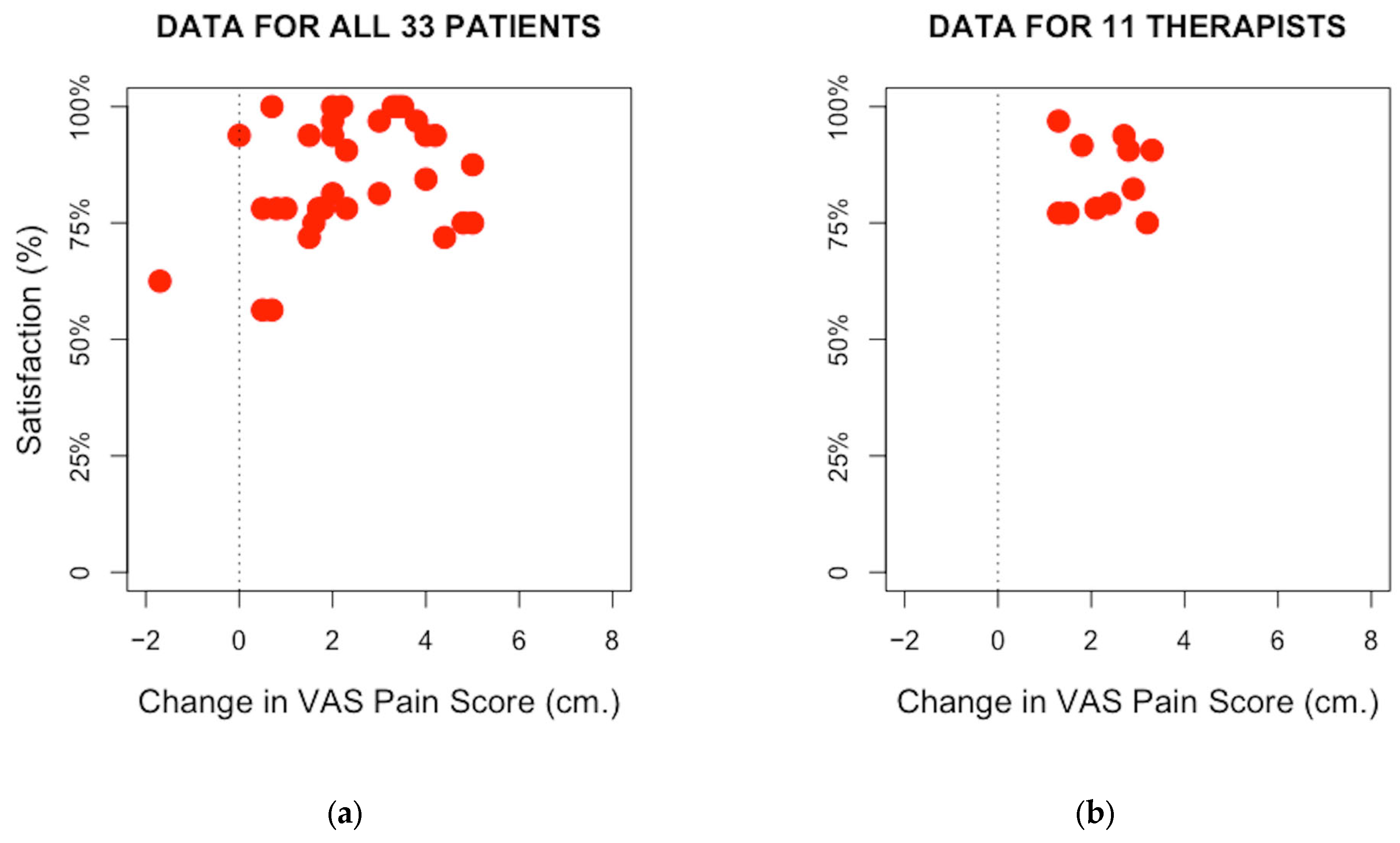
3.1.2. Outcome Measures Recorded for Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bennett, S.; Bennett, M.J.; Chatchawan, U.; Jenjaiwit, P.; Pantumethakul, R.; Kunhasura, S.; Eungpinichpong, W. Acute Effects of Traditional Thai Massage on Cortisol Levels, Arterial Blood Pressure and Stress Perception in Academic Stress Condition: A Single Blind Randomised Controlled Trial. J. Bodyw. Mov. Ther. 2016, 20, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Roylance, D.; David, L.; Salguero, C.P. Thai Massage Workbook: For Basic, Intermediate, and Advanced Courses; Findhorn Press: Scotland, UK, 2011; ISBN 9781844095643. [Google Scholar]
- Sucharit, W.; Eungpinichpong, W.; Hunsawong, T.; Pungsuwan, P.; Bennett, S.; Hojo, E.; Cruz, M.; Roberts, N.; Chatchawan, U. Pre-and Post-Treatment Study of the Application of a Traditional Thai Massage (TTM) Protocol for Treating Office Syndrome. Asia -Pac. J. Sci. Technol. 2023, 28, 1–9. [Google Scholar]
- Yoopat, P.; Maes, C.; Poriau, S.; Vanwonterghem, K. Thai Traditional Massage: Efficiency-Assessment of Three Traditional Massage Methods on Office Workers: An Explorative Study. J. Bodyw. Mov. Ther. 2015, 19, 246–252. [Google Scholar] [CrossRef]
- Chatchawan, U.; Thinkhamrop, B.; Kharmwan, S.; Knowles, J.; Eungpinichpong, W. Effectiveness of Traditional Thai Massage versus Swedish Massage among Patients with Back Pain Associated with Myofascial Trigger Points. J. Bodyw. Mov. Ther. 2005, 9, 298–309. [Google Scholar] [CrossRef]
- Chatchawan, U.; Eungpinichpong, W.; Sooktho, S.; Tiamkao, S.; Yamauchi, J. Effects of Thai Traditional Massage on Pressure Pain Threshold and Headache Intensity in Patients with Chronic Tension-Type and Migraine Headaches. J. Altern. Complement. Med. 2014, 20, 486–492. [Google Scholar] [CrossRef]
- Plakornkul, V.; Vannabhum, M.; Viravud, Y.; Roongruangchai, J.; Mutirangura, P.; Akarasereenont, P.; Laohapand, T. The Effects of the Court-Type Thai Traditional Massage on Anatomical Relations, Blood Flow, and Skin Temperature of the Neck, Shoulder, and Arm. BMC Complement. Altern. Med. 2016, 16, 363. [Google Scholar] [CrossRef]
- Viravud, Y.; Apichartvorakit, A.; Mutirangura, P.; Plakornkul, V.; Roongruangchai, J.; Vannabhum, M.; Laohapand, T.; Akarasereenont, P. The Anatomical Study of the Major Signal Points of the Court-Type Thai Traditional Massage on Legs and Their Effects on Blood Flow and Skin Temperature. J. Integr. Med. 2017, 15, 142–150. [Google Scholar] [CrossRef]
- Buttagat, V.; Eungpinichpong, W.; Kaber, D.; Chatchawan, U.; Arayawichanon, P. Acute Effects of Traditional Thai Massage on Electroencephalogram in Patients with Scapulocostal Syndrome. Complement. Ther. Med. 2012, 20, 167–174. [Google Scholar] [CrossRef]
- Boonrua, J.; Niempoog, S.; Pattaraarchachai, J.; Palanuvej, C.; Ruangrungsi, N. Effectiveness of the Court-Type Traditional Thai Massage versus Topical Diclofenac in Treating Patients with Myofascial Pain Syndrome in the Upper Trapezius. Indian J. Tradit. Knowl. 2016, 15, 30–34. [Google Scholar]
- Damapong, P.; Kanchanakhan, N.; Eungpinichpong, W.; Putthapitak, P.; Damapong, P. A Randomized Controlled Trial on the Effectiveness of Court-Type Traditional Thai Massage versus Amitriptyline in Patients with Chronic Tension-Type Headache. Evid. Based Complement. Altern. Med. 2015, 2015, 930175. [Google Scholar] [CrossRef]
- Sananpanichkul, P.; Sawadhichai, C.; Leaungsomnapa, Y.; Yapanya, P. Possible Role of Court-Type Thai Traditional Massage During Parturition: A Randomized Controlled Trial. Int. J. Ther. Massage Bodyw. 2019, 12, 23–28. [Google Scholar] [CrossRef]
- Srikaew, N.; Kietinun, S.; Sriyakul, K.; Tungsukruthai, P.; Pawa, K.K. Effectiveness of Court-Type Traditional Thai Massage plus Meditation in Patients with Myofascial Pain Syndrome on Upper Trapezius. Adv. Integr. Med. 2021, 9, 63–68. [Google Scholar] [CrossRef]
- Buttagat, V.; Muenpan, K.; Wiriyasakunphan, W.; Pomsuwan, S.; Kluayhomthong, S.; Areeudomwong, P. A Comparative Study of Thai Massage and Muscle Energy Technique for Chronic Neck Pain: A Single-Blinded Randomized Clinical Trial. J. Bodyw. Mov. Ther. 2021, 27, 647–653. [Google Scholar] [CrossRef]
- Buttagat, V.; Eungpinichpong, W.; Chatchawan, U.; Arayawichanon, P. Therapeutic Effects of Traditional Thai Massage on Pain, Muscle Tension and Anxiety in Patients with Scapulocostal Syndrome: A Randomized Single-Blinded Pilot Study. J. Bodyw. Mov. Ther. 2012, 16, 57–63. [Google Scholar] [CrossRef]
- Keeratitanont, K.; Jensen, M.P.; Chatchawan, U.; Auvichayapat, P. The Efficacy of Traditional Thai Massage for the Treatment of Chronic Pain: A Systematic Review. Complement. Ther. Clin. Pract. 2015, 21, 26–32. [Google Scholar] [CrossRef]
- Eungpinichpong, W.; Kongnaka, T. Effects of Femoral Artery Temporarily Occlusion on Skin Blood Flow of Foot. J. Med. Technol. Phys. Ther. 2002, 14, 151–159. [Google Scholar]
- Mohammadipour, F.; Pourranjbar, M.; Naderi, S.; Rafie, F. Work-Related Musculoskeletal Disorders in Iranian Office Workers: Prevalence and Risk Factors. J. Med. Life 2018, 11, 328–333. [Google Scholar] [CrossRef]
- Treaster, D.; Marras, W.S.; Burr, D.; Sheedy, J.E.; Hart, D. Myofascial Trigger Point Development from Visual and Postural Stressors during Computer Work. J. Electromyogr. Kinesiol. 2006, 16, 115–124. [Google Scholar] [CrossRef]
- Simons, D.G.; Travell, J.G. Travell & Simons’ Myofascial Pain and Dysfunction: The Trigger Point Manual, 2nd ed.; Williams & Wilkins: Baltimore, MD, USA, 1999. [Google Scholar]
- Dewitt, S.; Hall, J.; Smith, L.; Buckley, J.P.; Biddle, S.J.; Mansfield, L.; Gardner, B. Office Workers’ Experiences of Attempts to Reduce Sitting-Time: An Exploratory, Mixed-Methods Uncontrolled Intervention Pilot Study. BMC Public Health 2019, 19, 819. [Google Scholar] [CrossRef]
- Simons, D.G. Review of Enigmatic MTrPs as a Common Cause of Enigmatic Musculoskeletal Pain and Dysfunction. J. Electromyogr. Kinesiol. 2004, 14, 95–107. [Google Scholar] [CrossRef]
- Buttagat, V.; Hancharoenkul, B. Therapeutic Effects of Traditional Thai Massage on Cervical Range of Motion, Pain and Anxiety in Patients With Upper Trapezius Myofascial Pain Syndrome: An Assessor-Blind Randomized Controlled Trial. J. Med. Technol. Phys. Ther. 2019, 31, 9–20. [Google Scholar]
- Leesiriwattanagul, S.; Charoenkit, K.; Pibanwong, W. The Effects of a Thai Massage Program on Office Syndrome among Personnel. Nurs. J. Minist. Public Health 2019, 29, 129–141. [Google Scholar]
- Boonruab, J.; Niempoog, S.; Pattaraarchachai, J.; Palanuvej, C.; Ruangrungsi, N. A Comparison of the Quality of Life in Myofascial Pain Syndrome Patients Treated with the Court-Type Traditional Thai Massage and Topical Diclofenac. J. Health Res. 2015, 29, 371–375. [Google Scholar] [CrossRef]
- Wiwanitkit, V. Thai Traditional Massage: Issues Causing Possible Adverse Effects. Anc. Sci. Life 2015, 35, 122. [Google Scholar] [CrossRef]
- Mackawan, S.; Eungpinichpong, W.; Pantumethakul, R.; Chatchawan, U.; Hunsawong, T.; Arayawichanon, P. Effects of Traditional Thai Massage versus Joint Mobilization on Substance P and Pain Perception in Patients with Non-Specific Low Back Pain. J. Bodyw. Mov. Ther. 2007, 11, 9–16. [Google Scholar] [CrossRef]
- Chow, S.C.; Shao, J.; Wang, H.; Lokhnygina, Y. Sample Size Calculations in Clinical Research, 2nd ed.; Hall: Chapman, CA, USA, 2003. [Google Scholar]
- Ngamjarus, C.; Chongsuvivatwong, V.; McNeil, E. N4Studies: Sample Size and Power Calculation for an Epidemiological Study on a Smart Device. Siriraj Med J. 2016, 68, 160–170. [Google Scholar]
- Iglesias-gonzález, J.J.; Rey, U.; Carlos, J.; De, A. Myofascial Trigger Points, Pain, Disability, and Sleep Quality in Patients with Chronic Nonspecific Low Back Pain. Pain Med. 2013, 14, 1964–1970. [Google Scholar] [CrossRef]
- Cerezo-Téllez, E.; Torres-Lacomba, M.; Mayoral-del Moral, O.; Sánchez-Sánchez, B.; Dommerholt, J.; Gutiérrez-Ortega, C. Prevalence of Myofascial Pain Syndrome in Chronic Non-Specific Neck Pain: A Population- Based Cross-Sectional Descriptive Study. Pain Med. 2016, 17, 2369–2377. [Google Scholar] [CrossRef]
- Ribeiro, D.C.; Belgrave, A.; Naden, A.; Fang, H.; Matthews, P.; Parshottam, S. The Prevalence of Myofascial Trigger Points in Neck and Shoulder-Related Disorders: A Systematic Review of the Literature. BMC Musculoskelet. Disord. 2018, 19, 1–13. [Google Scholar] [CrossRef]
- Ginszt, M.; Berger, M.; Gawda, P.; Bożyk, A.; Gawda, J.; Szkutnik, J.; Suwała, M.; Majcher, P.; Kapelan, M. The Immediate Effect of Masseter Trigger Points Compression on Masticatory Muscle Activity. Forum Ortodon. 2017, 13, 78–88. [Google Scholar] [CrossRef]
- Shah, J.P.; Gilliams, E.A. Uncovering the Biochemical Milieu of Myofascial Trigger Points Using in Vivo Microdialysis: An Application of Muscle Pain Concepts to Myofascial Pain Syndrome. J. Bodyw. Mov. Ther. 2008, 12, 371–384. [Google Scholar] [CrossRef]
- Chen, Q.; Basford, J.; An, K.N. Ability of Magnetic Resonance Elastography to Assess Taut Bands. Clin. Biomech. 2008, 23, 623–629. [Google Scholar] [CrossRef]
- Eriksson Crommert, M.; Lacourpaille, L.; Heales, L.J.; Tucker, K.; Hug, F. Massage Induces an Immediate, Albeit Short-Term, Reduction in Muscle Stiffness. Scand. J. Med. Sci. Sport. 2015, 25, e490–e496. [Google Scholar] [CrossRef]
- Kett, A.R.; Sichting, F. Sedentary Behaviour at Work Increases Muscle Stiffness of the Back: Why Roller Massage Has Potential as an Active Break Intervention. Appl. Ergon. 2020, 82, 102497. [Google Scholar] [CrossRef]
- Caliskan, E.; Akkoc, O.; Bayramoglu, Z.; Gozubuyuk, O.B.; Kural, D.; Azamat, S.; Adaletli, I. Effects of Static Stretching Duration on Muscle Stiffness and Blood Flow in the Rectus Femoris in Adolescents. Med. Ultrason. 2019, 21, 136–143. [Google Scholar] [CrossRef]
- Mori, H.; Ohsawa, H.; Tanaka, T.H.; Taniwaki, E.; Leisman, G.; Nishijo, K. Effect of Massage on Blood Flow and Muscle Fatigue Following Isometric Lumbar Exercise. Med. Sci. Monit. 2004, 10, 173–179. [Google Scholar]
- Cambron, J.A.; Dexheimer, J.; Coe, P.; Swenson, R. Side-Effects of Massage Therapy: A Cross-Sectional Study of 100 Clients. J. Altern. Complement. Med. 2007, 13, 793–796. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Step | Original | Revised | Number of Pressing Points | Position of Patient |
|---|---|---|---|---|
| 1 | Press—Dor. Foot | Press—Dor. Foot | 9 |  |
| 2 | Press—Ant. Leg and Thigh | Press—Ant. Leg and Thigh | 9 | |
| 3 | Press—Lat. Thigh | Press—Lat. Thigh | 6 | |
| 4 | Occlusion—Femoral | Occlusion—Femoral | 1 | |
| 5 | Press—Pal. Hand *** | Press—Pal. Hand *** | 2 | |
| 6 | Press—Ant. Arm | Press—Ant. Arm | 9 | |
| 7 | Press—Dor. Hand | Press—Dor. Hand | 6 | |
| 8 | Press—Post. Arm | Press—Post. Arm | 9 | |
| 9 | Press—Ant. Shoulder *** | Press—Ant. Shoulder *** | 1 | |
| 10 | Occlusion—Brachial | Occlusion—Brachial | 1 | |
| 11 | Press—Plant. Foot | Press—Plant. Foot | 9 |  |
| 12 | Press—Med. Leg/Thigh | Press—Med. Leg/Thigh | 9 | |
| 13 | Press—Lat. Leg/Thigh | Press—Lat. Leg/Thigh | 12 | |
| 14 | Press—Gluteus *** | Press—Gluteus *** | 3 | |
| 15 | Press—Lat. Lower/Upper Back | Press—Lat. Lower/Upper Back | 30 | |
| 16 | Press—Scapular | Press—Scapular | 12 | |
| 17 | Press—Post. Shoulder/Neck | Press—Post. Shoulder/Neck | 12 | |
| 18 | Press—Lat. Shoulder/Head | Press—Lat. Shoulder/Head | 12 | |
| 19 | PT Stretch—Upper | Press—Post. Leg | 6 |  |
| 20 | PT Stretch—Lower | Press—Post. Thigh | 6 | |
| 21 | Press—Post. Leg | Press—Post. Lower/Upper Back | 24 | |
| 22 | Press—Post. Thigh | Press—Head/Face | 12 | |
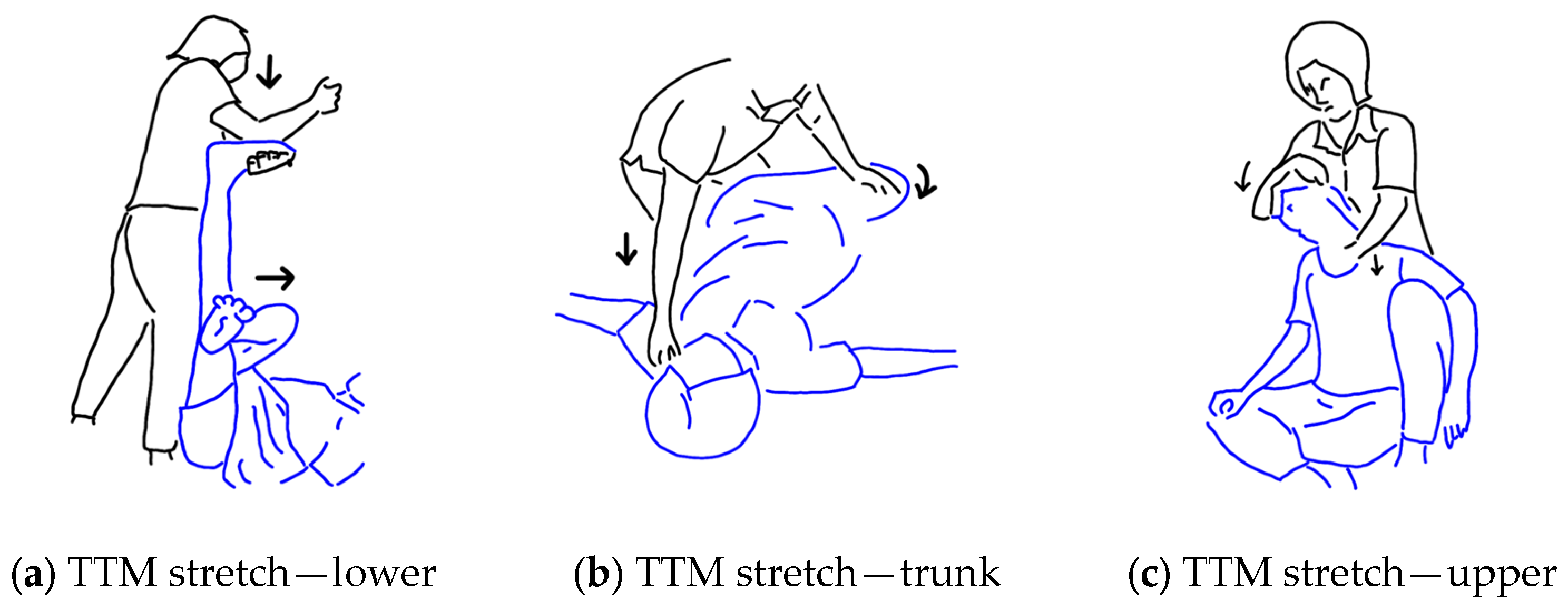
| 23 | Press—Post. Lower/Upper Back | TTM Stretch—Lower | 3 | |
| 24 | Press—Head/Face | TTM Stretch—Trunk | 3 | |
| 25 | TTM Stretch—Trunk | TTM Stretch—Upper | 4 |  |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sucharit, W.; Roberts, N.; Eungpinichpong, W.; Hunsawong, T.; Chatchawan, U. Standardised 25-Step Traditional Thai Massage (TTM) Protocol for Treating Office Syndrome (OS). Int. J. Environ. Res. Public Health 2023, 20, 6159. https://doi.org/10.3390/ijerph20126159
Sucharit W, Roberts N, Eungpinichpong W, Hunsawong T, Chatchawan U. Standardised 25-Step Traditional Thai Massage (TTM) Protocol for Treating Office Syndrome (OS). International Journal of Environmental Research and Public Health. 2023; 20(12):6159. https://doi.org/10.3390/ijerph20126159
Chicago/Turabian StyleSucharit, Wiraphong, Neil Roberts, Wichai Eungpinichpong, Torkamol Hunsawong, and Uraiwan Chatchawan. 2023. "Standardised 25-Step Traditional Thai Massage (TTM) Protocol for Treating Office Syndrome (OS)" International Journal of Environmental Research and Public Health 20, no. 12: 6159. https://doi.org/10.3390/ijerph20126159
APA StyleSucharit, W., Roberts, N., Eungpinichpong, W., Hunsawong, T., & Chatchawan, U. (2023). Standardised 25-Step Traditional Thai Massage (TTM) Protocol for Treating Office Syndrome (OS). International Journal of Environmental Research and Public Health, 20(12), 6159. https://doi.org/10.3390/ijerph20126159