
Particle Exposure Hazards of Visiting Outdoor Smoking Areas for Patients with Asthma or COPD Even in EU Countries with Comprehensive Smokefree Laws
 , , ,
, , ,  ,
,  , , , , and
, , , , and
Abstract
1. Introduction
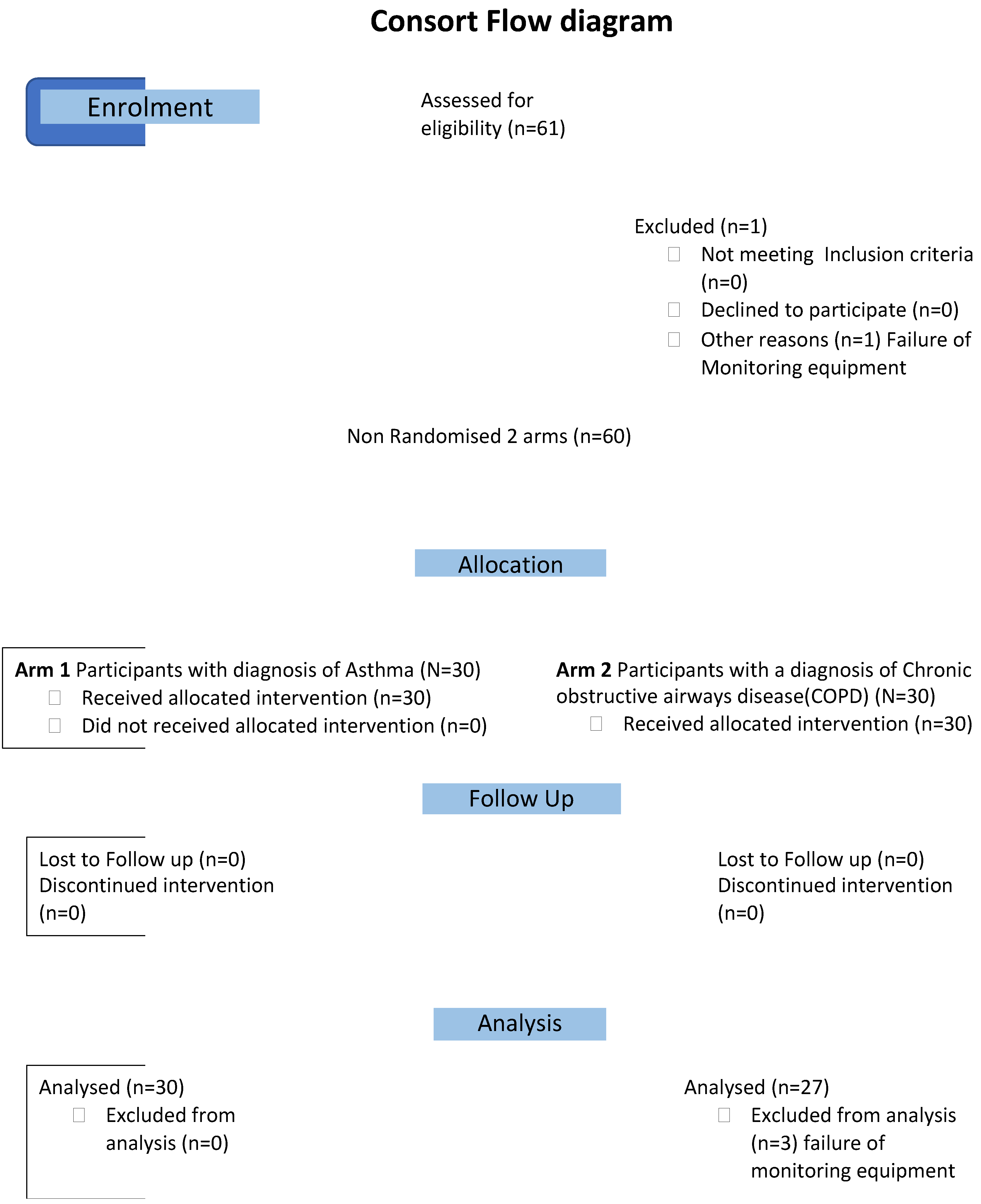
2. Methods
2.1. Ethics
2.2. Recruitment
2.3. Group Assignment
2.4. Details of the Intervention
2.5. Patients, Protocol and Training
2.6. Venues
2.7. Measurements
2.8. Statistical Analysis
3. Results
3.1. Exposure Levels
3.2. Respiratory Responses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wakefield, T.D.; Glantz, S.A. Securing Smokefree Laws Covering Casinos and Bars in Louisiana via Messaging, Continuous Campaigning and Health Coalitions. Int. J. Environ. Res. Public Health 2022, 19, 3936. [Google Scholar] [CrossRef]
- Sendall, M.C.; Fox, L.; Wraith, D. University Staff and Students’ Attitudes towards a Completely Smoke-Free Campus: Shifting Social Norms and Organisational Culture for Health Promotion. Int. J. Environ. Res. Public Health 2021, 18, 7104. [Google Scholar] [CrossRef] [PubMed]
- Campaign for Tobacco-Free Kids. Tobacco Control Laws: Legislation: Campaign for Tobacco-Free Kids, 2021. Available online: https://www.tobaccocontrollaws.org/legislation (accessed on 14 March 2023).
- Hanafin, J.; Clancy, L. History of Tobacco Production and Use. In Tobacco Epidemic, 2nd ed.; Karger International: Basel, Switzerland, 2015; Volume 42, pp. 1–18. [Google Scholar]
- Martínez-Sánchez, J.M.; Fernández, E.; Fu, M.; Gallus, S.; Martínez, C.; Sureda, X.; La Vecchia, C.; Clancy, L. Smoking Behaviour, Involuntary Smoking, Attitudes towards Smoke-Free Legislations, and Tobacco Control Activities in the European Union. PLoS ONE 2010, 5, e13881. [Google Scholar] [CrossRef] [PubMed]
- Sunday, S.; Kabir, Z. Impact of Carers’ Smoking Status on Childhood Obesity in the Growing up in Ireland Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 2759. [Google Scholar] [CrossRef]
- Goodman, P.; Agnew, M.; McCaffrey, M.; Paul, G.; Clancy, L. Effects of the Irish smoking ban on respiratory health of bar workers and air quality in Dublin pubs. Am. J. Respir. Crit. Care Med. 2007, 175, 840–845. [Google Scholar] [CrossRef]
- Frazer, K.; Callinan, J.E.; Mchugh, J.; van Baarsel, S.; Clarke, A.; Doherty, K.; Kelleher, C. Legislative smoking bans for reducing harms from secondhand smoke exposure, smoking prevalence and tobacco consumption. Cochrane Database Syst. Rev. 2016, 2, CD005992. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, S.O.; Fernández, E.; Driezen, P.; Fu, M.; Tigova, O.; Castellano, Y.; Mons, U.; Herbeć, A.; Kyriakos, C.N.; Demjén, T. Secondhand smoke exposure in European countries with different smoke-free legislation: Findings from the EUREST-PLUS ITC Europe surveys. Nicotine Tob. Res. 2022, 24, 85–92. [Google Scholar] [CrossRef]
- Gao, M.; Li, Y.; Wang, F.; Zhang, S.; Qu, Z.; Wan, X.; Wang, X.; Yang, J.; Tian, D.; Zhang, W. The effect of smoke-free legislation on the mortality rate of acute myocardial infarction: A meta-analysis. BMC Public Health 2019, 19, 1269. [Google Scholar] [CrossRef] [PubMed]
- Semple, S.; Creely, K.S.; Naji, A.; Miller, B.G.; Ayres, J.G. Secondhand smoke levels in Scottish pubs: The effect of smoke-free legislation. Tob. Control 2007, 16, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Stallings-Smith, S.; Zeka, A.; Goodman, P.; Kabir, Z.; Clancy, L. Reductions in Cardiovascular, Cerebrovascular, and Respiratory Mortality Following the National Irish Smoking Ban: Interrupted Time-Series Analysis. PLoS ONE 2013, 8, e62063. [Google Scholar] [CrossRef] [PubMed]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans; World Health Organization; International Agency for Research on Cancer. Tobacco Smoke and Involuntary Smoking; IARC: Lyon, French, 2004; Volume 83, ISBN 92-832-1283-5. [Google Scholar]
- CDC [Center for Disease Control]. Smokefree Policies Improve Health. Available online: https://www.cdc.gov/tobacco/secondhand-smoke/protection/improve-health.htm (accessed on 14 March 2023).
- Hawkins, S.S.; Hristakeva, S.; Gottlieb, M.; Baum, C.F. Reduction in emergency department visits for children’s asthma, ear infections, and respiratory infections after the introduction of state smoke-free legislation. Prev. Med. 2016, 89, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Reitsma, M.; Kendrick, P.; Ababneh, E.; Abbafati, C.; Abbasi-Kangevari, M.; Abdoli, A.; Abedi, A.; Abhilash, E.; Abila, D.; Aboyans, V.; et al. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990–2019: A systematic analysis from the Global Burden of Disease Study 2019. Lancet 2021, 397, 2337–2360. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Report on the Global Tobacco Epidemic 2021: Addressing New and Emerging Products; Licence: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Zhai, C.; Hu, D.; Yu, G.; Hu, W.; Zong, Q.; Yan, Z.; Wang, Y.; Wang, L.; Zhang, T.; Sun, H.; et al. Global, regional, and national deaths, disability-adjusted life years, years lived with disability, and years of life lost for the global disease burden attributable to second-hand smoke, 1990–2019: A systematic analysis for the Global Burden of Disease Study. Sci. Total Environ. 2023, 862, 160677. [Google Scholar] [CrossRef] [PubMed]
- Government of Ireland Public Health (Tobacco) Acts 2002 and 2004. Dublin: Stationery Office, 2004. Available online: https://www.irishstatutebook.ie/eli/2004/act/6/enacted/en/html (accessed on 14 March 2023).
- International Agency for Research on Cancer (IARC). Handbooks of Cancer Prevention, Tobacco Control. In Evaluating the Effectiveness of Smoke-Free Policies; IARC: Lyon, French, 2009; Volume 13. [Google Scholar]
- López, M.J.; Fernández, E.; Gorini, G.; Moshammer, H.; Polanska, K.; Clancy, L.; Dautzenberg, B.; Delrieu, A.; Invernizzi, G.; Muñoz, G. Exposure to secondhand smoke in terraces and other outdoor areas of hospitality venues in eight European countries. PLoS ONE 2012, 7, e42130. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Disparities in secondhand smoke exposure—United States, 1988–1994 and 1999–2004. MMWR Morb. Mortal. Wkly. Rep. 2008, 57, 744–747. [Google Scholar]
- Strulovici-Barel, Y.; Omberg, L.; O’Mahony, M.; Gordon, C.; Hollmann, C.; Tilley, A.E.; Salit, J.; Mezey, J.; Harvey, B.G.; Crystal, R.G. Threshold of biologic responses of the small airway epithelium to low levels of tobacco smoke. Am. J. Respir. Crit. Care Med. 2010, 182, 1524–1532. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Li, B. Exposure-response relationship between passive smoking and adult pulmonary function. Am. J. Respir. Crit. Care Med. 1995, 151, 41–46. [Google Scholar] [CrossRef]
- Eisner, M.D.; Wang, Y.; Haight, T.J.; Balmes, J.; Hammond, S.K.; Tager, I.B. Secondhand Smoke Exposure, Pulmonary Function, and Cardiovascular Mortality. Ann. Epidemiol. 2007, 17, 364–373. [Google Scholar] [CrossRef]
- White, J.R.; Froeb, H.F. Small-airways dysfunction in nonsmokers chronically exposed to tobacco smoke. N. Engl. J. Med. 1980, 302, 720–723. [Google Scholar] [CrossRef]
- Masjedi, M.-R.; Kazemi, H.; Johnson, D.C. Effects of passive smoking on the pulmonary function of adults. Thorax 1990, 45, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Kendrick, P.J.; Paulson, K.R.; Gupta, V.; Abrams, E.M.; Adedoyin, R.A.; Adhikari, T.B.; Advani, S.M.; Agrawal, A.; Ahmadian, E.; et al. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2020, 8, 585–596. [Google Scholar] [CrossRef] [PubMed]
- Kabir, Z.; Manning, P.J.; Holohan, J.; Keogan, S.; Goodman, P.G.; Clancy, L. Second-hand smoke exposure in cars and respiratory health effects in children. Eur. Respir. J. 2009, 34, 629–633. [Google Scholar] [CrossRef]
- Öberg, M.; Jaakkola, M.S.; Woodward, A.; Peruga, A.; Prüss-Ustün, A. Worldwide burden of disease from exposure to second-hand smoke: A retrospective analysis of data from 192 countries. Lancet 2011, 377, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Flouris, A.D.; Koutedakis, Y. Immediate and short-term consequences of secondhand smoke exposure on the respiratory system. Curr. Opin. Pulm. Med. 2011, 17, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.T.; Hu, K.R.; Jian, Z.; Ai, F.L.; Shi, Y.L.; Wang, X.W.; Yang, W.Y.; Wang, J.X.; Ai, L.M.; Xia, W. The Association between Exposure to Second-Hand Smoke and Disease in the Chinese Population: A Systematic Review and Meta-Analysis. Biomed. Environ. Sci. 2023, 36, 24–37. [Google Scholar]
- Zhao, B.; Bai, L.; Wan, R.; Wang, Y.; Qin, L.; Xiao, Q.; Pan, P.; Hu, C.; Jiang, J. Exposure to second-hand smoke is an independent risk factor of small airway dysfunction in non-smokers with chronic cough: A retrospective case-control study. Front. Public Health 2022, 2308, 912100. [Google Scholar] [CrossRef]
- Keogan, S.; Alonso, T.; Sunday, S.; Tigova, O.; Fernández, E.; López, M.J.; Gallus, S.; Semple, S.; Tzortzi, A.; Boffi, R. Lung function changes in patients with chronic obstructive pulmonary disease (COPD) and asthma exposed to secondhand smoke in outdoor areas. J. Asthma 2021, 58, 1169–1175. [Google Scholar] [CrossRef]
- Cammalleri, V.; Marotta, D.; Protano, C.; Vitali, M.; Villari, P.; Cattaruzza, M.S. Smoke-free department working group how do combustion and non-combustion products used outdoors affect outdoor and indoor particulate matter levels? A field evaluation near the entrance of an Italian university library. Int. J. Environ. Res. Public Health 2020, 17, 5200. [Google Scholar] [CrossRef]
- Kaplan, B.; Carkoglu, A.; Ergor, G.; Hayran, M.; Sureda, X.; Cohen, J.E.; Navas-Acien, A. Evaluation of Secondhand smoke using PM2.5 and observations in a random stratified sample in hospitality venues from 12 cities. Int. J. Environ. Res. Public Health 2019, 16, 1381. [Google Scholar] [CrossRef]
- Currie, L.M.; Clancy, L. The road to smoke-free legislation in Ireland. Addiction 2011, 106, 15–24. [Google Scholar] [CrossRef]
- Kulhánek, A.; Lukavská, K.; Švancarová, I.; Fidesová, H.; Gabrhelík, R. Changes in tobacco use patterns and motivation to quit related to the new smoke-free legislation in the Czech Republic. J. Public Health 2021, 43, 348–354. [Google Scholar] [CrossRef]
- Fernández, E.; Fu, M.; Pérez-Ríos, M.; Schiaffino, A.; Sureda, X.; López, M.J. Changes in secondhand smoke exposure after smoke-free legislation (Spain, 2006–2011). Nicotine Tob. Res. 2017, 19, 1390–1394. [Google Scholar] [CrossRef] [PubMed]
- Arvind, D.K.; Mann, J.; Bates, A.; Kotsev, K. The AirSpeck Family of Static and Mobile Wireless Air Quality Monitors. In Proceedings of the 19th Euromicro Conference on Digital System Design, Limassol, Cyprus, 31 August–2 September 2016. [Google Scholar]
- Drummond, G.; Bates, A.; Mann, J.; Arvind, D. Validation of a new non-invasive automatic monitor of respiratory rate for postoperative subjects. Br. J. Anaesth. 2011, 107, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Clancy, L.; Keogan, S.; Sunday, S.; Šípková, M.; Sanz, M.T.P.; Soriano, J.B. Changes in breathing during exposure to SHS in outside areas of pubs in patients with asthma and COPD in three EU countries. Tob. Prev. Cessat. 2020, 6, A78. [Google Scholar] [CrossRef]
- Potera, C. Smoking and secondhand smoke. Study finds no level of SHS exposure free of effects. Environ. Health Perspect. 2010, 118, 474. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (US); U.S. Department of Health and Human Services. The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General; Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2006; ISBN 0-16-076152-2. [Google Scholar]
- Eagan, T.M.L.; Hetland, J.; Aarø, L.E. Decline in respiratory symptoms in service workers five months after a public smoking ban. Tob. Control 2006, 15, 242–246. [Google Scholar] [CrossRef]
- Eisner, M.D.; Smith, A.K.; Blanc, P.D. Bartenders’ respiratory health after establishment of smoke-free bars and taverns. J. Am. Med. Assoc. 1998, 280, 1909–1914. [Google Scholar] [CrossRef]
- Stewart, I.C.; Parker, A.; Catterall, J.R.; Douglas, N.J.; Flenley, D.C. Effect of bronchial challenge on breathing patterns and arterial oxygenation in stable asthma. Chest 1989, 95, 65–70. [Google Scholar] [CrossRef]
- Becklake, M.; Kauffmann, F. Gender differences in airway behaviour over the human life span. Thorax 1999, 54, 1119–1138. [Google Scholar] [CrossRef]
- Noble, M.I.M. Abraham Guz memorial: Still unresolved hypotheses: Lung reflexes and perceptions of breathing. Respir. Physiol. Neurobiol. 2015, 217, 46–53. [Google Scholar] [CrossRef]
- Hernandez, L.; Manning, J.; Zhang, S. Voluntary control of breathing affects center of pressure complexity during static standing in healthy older adults. Gait Posture 2019, 68, 488–493. [Google Scholar] [CrossRef] [PubMed]
- Flenley, D.C.; Cooke, N.J.; King, A.J.; Leitch, A.G.; Brash, H.M. The hypoxic drive to breathing during exercise in normal man and in hypoxic patients with chronic bronchitis and emphysema. Bull. Physiopathol. Respir. 1973, 9, 689–693. [Google Scholar] [CrossRef]
- Soleimani, F.; Dobaradaran, S.; De-la-Torre, G.E.; Schmidt, T.C.; Saeedi, R. Content of toxic components of cigarette, cigarette smoke vs cigarette butts: A comprehensive systematic review. Sci. Total Environ. 2022, 813, 152667. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Asthma | COPD | All | ||
|---|---|---|---|---|
| n = 30 | n = 30 | n = 60 | p-Value | |
| Age in years | 46.9 ± 18.7 | 63.3 ± 10.2 | 55.2 ± 17.1 | >0.01 |
| Weight in kg | 75.6 ± 18.1 | 80.3 ± 16.5 | 78 ± 17.3 | 0.33 |
| Sex | ||||
| Male | 11 (36.7%) | 14 (46.7%) | 25 (41.7%) | 0.30 |
| Female | 19 (63.3%) | 16 (53.3%) | 35 (58.3%) | |
| Smoking status | ||||
| Current smoker | 8 (26.7%) | 21 (70%) | 29 (48.3%) | >0.01 |
| Ex-smoker | 6 (20%) | 9 (30%) | 15 (25%) | |
| Never smoked | 16 (53.3%) | 0 (0%) | 16 (26.7%) | |
| Lives with a smoker | ||||
| Yes | 7 (23.3%) | 10 (33.3%) | 17 (28.3%) | |
| No | 23 (76.7%) | 20 (66.7%) | 43 (71.7%) | 0.39 |
| CAT/ACT score | 21.8 ± 3.6 | 12.0 ± 7.4 | 16.88 | >0.01 |
| Number smoking in the outdoor smoking areas during visit | ||||
| 1–5 smokers | 22 (73.3%) | 22 (73.3%) | 44 (73.3%) | |
| More than 5 smokers | 8 (26.7%) | 8 (26.7%) | 16 (26.7%) | 0.77 |
| Number of walls in the outdoor smoking area | ||||
| 1 and 2 | 5 (16.7%) | 6 (20%) | 11 (18.3%) | |
| 3 and 4 | 25 (83.3%) | 24 (80%) | 49 (81.7%) | 0.44 |
| n | µg/m3 | SD/IQR | Range (µg/m3) | |
|---|---|---|---|---|
| Mean PM 2.5 | ||||
| not in SHS area, | 60 | 101.45 | 164.5 | 5.84–987.99 |
| in SHS area, | 57 | 233.59 | 359.81 | 5.81–1933.71 |
| Median PM 2.5 | ||||
| Not in SHS area, | 60 | 68.40 | 42.2 | 4.51–812.59 |
| In SHS area, | 57 | 214.26 | 362.61 | 5.84–1913.3 |
| (a) Overall Population | |||||
|---|---|---|---|---|---|
| n | Mean | SD/IQR | Range Br | ||
| Mean breathing rates | |||||
| Not in SHS area, | 60 | 21.66 | 1.91 | 17.88–28.58 | |
| In SHS area, | 57 * | 21.57 | 2.51 | 16.46–27.56 | |
| Median breathing rates | |||||
| Not in SHS area, | 60 | 21.64 | 2.33 | 17.71–29.47 | |
| In SHS area, | 57 * | 21.58 | 3.17 | 15.98–28.12 | |
| (b) Population Subgroups: Br Increased or Decreased | |||||
| Variable | Before SHS exposure mean (SD) | During SHS exposure mean (SD) | Mean difference (95% C.I) | t (df) | p-value |
| Breathing rates increased (n = 28) | 21.47 (1.74) | 22.82 (2.29) | −1.35 (−1.80, −0.91) | −6.22 (27) | 0.00 |
| Breathing rates decreased (n = 29) | 21.95 (2.43) | 20.38 (2.79) | 1.57 (1.03, 2.12) | 5.93 (28) | 0.00 |
| (a) Breathing Rates/Minute (Br) | |||||
|---|---|---|---|---|---|
| Variable | Br at Rest before Exposure Mean (SD) | Br at Rest during Exposure Mean (SD) | Mean Difference (95% C.I.) | t (df) | p-Value |
| Gender | |||||
| Male (n = 26) | 21.49 (2.04) | 20.94 (2.68) | 0.55 (−0.40, 1.51) | 1.20 (23) | 0.24 |
| Female (n = 34) | 21.88 (2.18) | 22.05 (2.86) | −0.17 (0.76, 0.43) | −0.57 (32) | 0.57 |
| Diagnosis | |||||
| Asthma (n = 30) | 21.00 (1.79) | 20.80 (2.24) | 0.21 (−0.43, 0.;84) | 0.66 (29) | 0.51 |
| COPD (n = 27) | 22.51 (2.190 | 22.45 (3.16) | 0.06 (−0.82, 0.94) | 0.14 (26) | 0.89 |
| Smoking status | |||||
| Current smoker (n = 28) | 22.17 (2.47) | 22.14 (3.03) | 0.03 (−0.70, 0.77) | 0.09 (27) | 0.93 |
| Ex-smoker (n = 16) | 21.30 (1.63) | 20.70 (3.25) | 0.60 (−0.90, 2.10) | 0.87 (12) | 0.40 |
| Non-smoker (n = 16) | 21.27 (1.67) | 21.33 (1.82) | −0.06 (−0.93, 0.82) | −0.14 (15) | 0.89 |
| Duration time of exposure | |||||
| Up to 1 h (n = 21) | 21.60 (2.10) | 21.67 (3.30) | −0.07 (−1.13, 0.98) | −0.15 (18) | 0.88 |
| 1 to 2 h (n = 28) | 21.49 (1.60) | 21.26 (2.43) | 0.23 (−0.60, 1.07) | 0.58 (26) | 0.57 |
| >2 h (n = 11) | 22.48 (3.09) | 22.23 (2.94) | 0.26 (−0.43, 0.95) | 0.83 (10) | 0.43 |
| (b) Increase in Br | |||||
| Variable | Br at rest before exposure Mean (SD) | Br during exposure Mean (SD) | Mean difference (95% C.I) | t (df) | p-value |
| Asthma (n = 17) | 20.83 (1.28) | 21.72 (1.65) | −0.90 (−1.30, −0.49) | −4.71 (16) | 0.00 |
| Male (n = 5) | 20.45 (1.50) | 21.00 (1.83) | −0.53 (−1.21, 0.14) | −2.20 (4) | 0.09 |
| Female (n = 12) | 21.00 (1.21) | 22.04 (1.53) | −1.05 (−1.58, −0.51) | −4.32 (11) | 0.00 |
| COPD (n = 11) | 22.28 (1.94) | 24.52 (2.15) | −2.05 (−2.93, −1.19) | −5.26 (10) | 0.00 |
| Male (n= 4) | 20.84 (1.64) | 23.62 (2.46) | −2.78 (−5.19, −0.38) | −3.70 (3) | 0.03 |
| Female (n = 7) | 23.40 (1.47) | 25.03 (2.00) | −1.64 (−2.62, −0.66) | −4.11 (6) | 0.00 |
| (c) Decrease in Br | |||||
| Variable | Br at rest before exposure Mean (SD) | Br at rest During exposure Mean (SD) | Mean difference (95% C.I) | t (df) | p-value |
| Asthma (n = 13) | 21.23 (2.34) | 19.58 (2.38) | 1.65 (0.74, 2.55) | 3.96 (12) | 0.00 |
| Male (n = 6) | 21.07 (2.60) | 18.63 (2.03) | 2.45 (2.03) | 3.40 (5) | 0.02 |
| Female (n = 7) | 21.37 (2.33) | 20.40 (2.49) | 0.96 (0.19, 1.74) | 3.03 (6) | 0.02 |
| COPD (n = 16) | 22.55 (2.40) | 21.03 (3.00) | 1.51 (0.76, 2.27) | 4.28 (15) | 0.00 |
| Male (n = 9) | 22.64 (1.80) | 21.26 (2.53) | 1.38 (0.28, 2.48) | 2.90 (8) | 0.02 |
| Female (n = 7) | 22.42 (3.18) | 20.74 (3.70) | 1.69 (0.31, 3.10) | 3.00 (6) | 0.02 |
| (a) | ||||
|---|---|---|---|---|
| Population | Change in Br (n = 57) | |||
| Characteristics (n = 57) | Decreased Br | Increased Br | Total/Mean Difference (95% CI) n= 57 | |
| n = 29 (50.88) | n = 28 (49.12) | |||
| Gender | Gender | |||
| Male | 15 (51.72) | Male | ||
| Female | 14 (48.28) | Female | ||
| Mean Age (years) | 56.00 ± 17.05 | Mean Age (years) | ||
| Male | 58.27 ± 17.47 | Male | ||
| Female | 54.64 ± 17.05 | Female | ||
| Smoking Status | Smoking Status | |||
| Current Smoker | 16 (55.17) | Current Smoker | ||
| Ex-Smoker | 7 (24.14) | Ex-Smoker | ||
| Non-Smoker | 6 (20.69) | Non-Smoker | ||
| Mean Weight (kg) | 77.68 ± 16.00 | Mean Weight (kg) | ||
| Male | 86.18 ± 13.76 | Male | ||
| Female | 68.57 ± 13.20 | Female | ||
| Diagnosis | Diagnosis | |||
| COPD | 16 (55.17) | COPD | ||
| Asthma | 13 (44.83) | Asthma | ||
| CAT/ACT Score | CAT/ACT Score | |||
| COPD (CAT) | 10.12 ± 4.72 | COPD (CAT) | ||
| Asthma (ACT) | 21.38 ± 3.42 | Asthma (ACT) | ||
| Duration Time of Exposure | Duration Time of Exposure | |||
| Up to 1 h | 7 (24.14) | Up to 1 h | ||
| 1 to 2 h | 14 (48.28) | 1 to 2 h | ||
| >2 h | 8 (27.59) | > 2 h | ||
| (b) | ||||
| Changes in female asthmatics according to spirometry changes | Breathing Rates (Br) | Total | ||
| Decreased Br | Increased Br | n = 19 | ||
| FEV1 n = 19 | Decrease Increase | 3 (42.86) 4 (51.14) | FEV1 n = 19 | Decrease Increase |
| FVC * n = 18 | Decrease Increase | 2 (28.57) 5 (71.43) | FVC * n = 18 | Decrease Increase |
| PEFR ** n = 18 | Decrease Increase | 3 (42.86) 4 (57.14) | PEFR ** n = 18 | Decrease Increase |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keogan, S.; Alonso, T.; Sunday, S.; Hanafin, J.; Tigova, O.; Fernandez, E.; Lopez, M.J.; Gallus, S.; Semple, S.; Tzortzi, A.; et al. Particle Exposure Hazards of Visiting Outdoor Smoking Areas for Patients with Asthma or COPD Even in EU Countries with Comprehensive Smokefree Laws. Int. J. Environ. Res. Public Health 2023, 20, 5978. https://doi.org/10.3390/ijerph20115978
Keogan S, Alonso T, Sunday S, Hanafin J, Tigova O, Fernandez E, Lopez MJ, Gallus S, Semple S, Tzortzi A, et al. Particle Exposure Hazards of Visiting Outdoor Smoking Areas for Patients with Asthma or COPD Even in EU Countries with Comprehensive Smokefree Laws. International Journal of Environmental Research and Public Health. 2023; 20(11):5978. https://doi.org/10.3390/ijerph20115978
Chicago/Turabian StyleKeogan, Sheila, Tamara Alonso, Salome Sunday, Joan Hanafin, Olena Tigova, Esteve Fernandez, Maria Jose Lopez, Silvano Gallus, Sean Semple, Anna Tzortzi, and et al. 2023. "Particle Exposure Hazards of Visiting Outdoor Smoking Areas for Patients with Asthma or COPD Even in EU Countries with Comprehensive Smokefree Laws" International Journal of Environmental Research and Public Health 20, no. 11: 5978. https://doi.org/10.3390/ijerph20115978
APA StyleKeogan, S., Alonso, T., Sunday, S., Hanafin, J., Tigova, O., Fernandez, E., Lopez, M. J., Gallus, S., Semple, S., Tzortzi, A., Boffi, R., Gorini, G., Lopez-Nicolas, A., Arvind, D. K., Radu-Loghin, C., Soriano, J. B., & Clancy, L. (2023). Particle Exposure Hazards of Visiting Outdoor Smoking Areas for Patients with Asthma or COPD Even in EU Countries with Comprehensive Smokefree Laws. International Journal of Environmental Research and Public Health, 20(11), 5978. https://doi.org/10.3390/ijerph20115978