


“I Don’t Want to Go to Work”: A Mixed-Methods Analysis of Healthcare Worker Experiences from the Front- and Side-Lines of COVID-19
 ,
, 
Abstract
1. Introduction
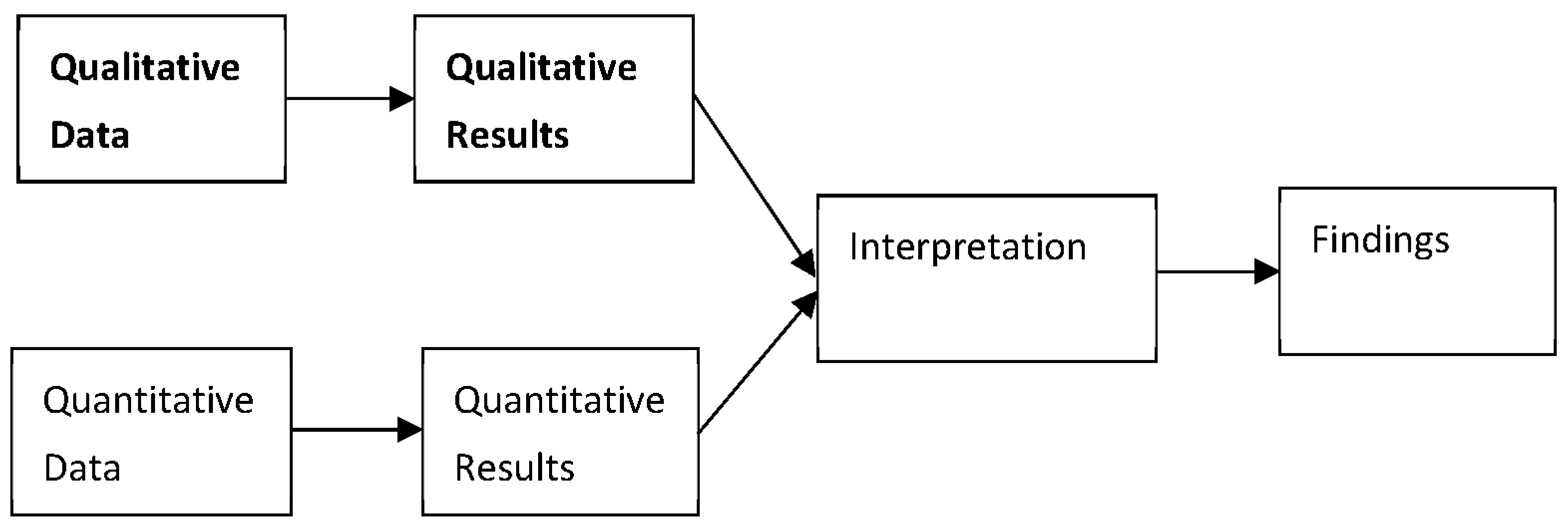
2. Materials and Methods
3. Results
3.1. Theme 1: Professional Identity
I realized I am the one that is in contact every single day that I work with COVID patients, so… I had an epiphany that I will not be able to do massage for a really long time.
3.1.1. Subtheme 1.1: Locked-Out
I don’t know what it’s going to feel like the next time I have my hands on someone. I think it’s going to feel really great, but I also think it’s going to feel really scary.
3.1.2. Subtheme 1.2: Locked-In
I’ve even thought about calling in sick for shifts because I just don’t want to go in and have to deal with all of this stuff… I don’t want to go to work.
Yes, I chose to do training in medicine, and yes I wanted to be there, but I didn’t want to feel like the resources weren’t there or feel like I couldn’t provide the right answers.
3.2. Theme 2: Intrinsic Stressors
3.2.1. Subtheme 2.1: Fear of COVID-19 and Concern about Spread
Unfortunately, because I felt fine on Saturday, I saw three of my massage clients, and so they were all exposed. I was wearing a mask and a face shield… [but] one of the three have tested positive.
There was quite a bit of stress in that having parents above the age of 65 and have comorbidities and then coming to a family’s house and having to deal with potentially spreading the virus to them unknowingly. It’s the unknowing part of COVID that’s the most stressful.
3.2.2. Subtheme 2.2: Allostatic Load
I’m worried that if I make [wearing masks] a mandatory thing, I’m going to lose that client…It’s a very conservative town, and a lot of people don’t like to wear masks.
I have a lot of people that are stressed by the politics and the election…There’s different stress stimulus that wasn’t present a few months ago.
3.3. Theme 3: Extrinsic Factors
Our hospitals have a huge decrease of patients, which means starting next week we start furloughs…which is a very strange feeling, thinking that you’re very important and you’re going to do all this good, [then] you are not needed.
I’d be putting my livelihood, my business, and my professional recognition at stake if I were to justify to myself that medically necessary massage was ok with the mandates that our governor has made.
3.4. Theme 4: Coping Strategies
I am sleeping a lot. I don’t get out of bed very often. I have been looking for something to fill my time, so I’ve taken up some gardening and getting some ideas ready for yard work.
I’ve been coping by eating a lot of comfort food… I’m gaining weight like crazy, like 20 pounds since quarantine started.
I’ve noticed with the downtime the social isolation has gotten to me. Some of my less healthy coping patterns have resurfaced like, um, tobacco smoking and comfort foods, um, and staying up way too late.
We have a quarantine station we set up in the front door… We wipe everything down as soon as we get home, strip our clothes, they go right into the wash, we go right to the shower before we do anything else when we get home.
I feel more vulnerable to COVID… I’ve been paying a lot of attention to the number of people I’ve massaged and their occupation. Once I reached a hundred and fifty since we’ve been reopened, I looked at my data and… 11.3% of those 150 are nurses.
3.5. Moral Distress and Burnout
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Which of the Following Are You Currently Experiencing? | N (%) |
|---|---|
| Shortage of PPE (personal protective equipment) | 49 (25.5) |
| Shortage of supplies needed to treat patients | 20 (10.4) |
| Shortage of medications needed to treat patients | 5 (2.6) |
| Staffing concerns in my department/office (only my department/office is experiencing issues with too few doctors/too few nurses/too few staff) | 60 (31.2) |
| Staffing concerns in the hospital (the entire hospital is experiencing issues with too few doctors/too few nurses/too few staff) | 43 (22.4) |
| Lack of sufficient access to COVID-19 testing for healthcare providers | 41 (21.4) |
| Feeling ill-prepared to manage escalating work demands | 54 (28.1) |
| Difficulty admitting or transferring patients | 23 (12.0) |
| Fear that the risk of COVID-19 exposure is not under my control | 113 (58.9) |
| Total Responses | 192 |
| Which of the Following Are You Currently Concerned about Regarding Your Clinical Work Environment? Check All That Apply. | N (%) |
|---|---|
| Shortage of PPE (personal protective equipment) | 56 (29.2) |
| Shortage of supplies needed to treat patients | 32 (16.7) |
| Shortage of medications needed to treat patients | 13 (6.8) |
| Staffing concerns in my department (only my department/office is experiencing issues with too few doctors/too few nurses/too few staff) | 58 (30.2) |
| Staffing concerns in the hospital (the entire hospital is experiencing issues with too few doctors/too few nurses/too few staff) | 40 (20.8) |
| Lack of sufficient access to COVID-19 testing for healthcare providers | 44 (22.9) |
| Feeling ill-prepared to manage escalating work demands | 60 (31.2) |
| Difficulty admitting or transferring patients | 24 (12.5) |
| Fear that the risk of COVID-19 exposure is not under my control | 109 (56.8) |
| Total Responses | 192 |
| Which of the Following Are You Currently Concerned about Regarding General Work-Related Stressors? Check All That Apply: | Locked-In N (%) | Locked-Out N (%) | Total N (%) | p-Value |
|---|---|---|---|---|
| Too many bureaucratic tasks (e.g., charting, paperwork) | 78 (40.6) | 45 (23.4) | 123 (32.0) | * <0.001 |
| Electronic health record issues | 33 (17.2) | 11 (5.7) | 44 (11.5) | * <0.001 |
| Spending too many hours at work | 40 (20.8) | 38 (19.8) | 78 (20.3) | 0.40 |
| Keeping workspace sanitary | NA | 144 (75.0) | NA | NA |
| Communication problems (e.g., unclear, delayed, conflicting, or too much information) | 94 (49.0) | 95 (49.5) | 189 (49.2) | 0.54 |
| Lack of support from the hospital/organization | 60 (31.2) | 33 (17.2) | 93 (24.2) | * <0.001 |
| Lack of advance planning and resource availability at a local/national level | 88 (45.8) | 95 (49.5) | 183 (47.7) | 0.76 |
| Too many marketing/business-related tasks (e.g., scheduling patients, advertising re-opening) | NA | 45 (24.4) | NA | NA |
| Frustration with societal misperceptions and/or misinformation that impede my ability to care for patients quickly and effectively | 98 (51.0) | 102 (53.1) | 200 (52.1) | 0.66 |
| Increasing conflict between professional responsibilities (e.g., duty to patients and the healthcare system) and personal responsibilities (e.g., keeping my family and friends safe) | 99 (51.6) | 113 (58.8) | 212 (55.2) | 0.92 |
| Total Responses | 192 | 192 | 384 |
Appendix B
| Which of the Following Have You Found Helpful in the Past Week? Check All That Apply: | Locked-In N(%) | Locked-Out N (%) | Total N (%) | Χ2 | p-Value |
|---|---|---|---|---|---|
| Regular social interaction/check-ins with friends and family | 147 (76.5) | 145 (75.5) | 292 (76.0) | 0.06 | 0.45 |
| Regular social interaction/check-ins with work colleagues | 76 (39.6) | 78 (40.6) | 154 (40.1) | 0.04 | 0.46 |
| One-on-one counseling | 19 (9.9) | 24 (2.5) | 43 (11.2) | 0.65 | 0.26 |
| Support groups/group counseling | 6 (3.1) | 13 (6.8) | 19 (5.0) | 2.72 | 0.08 |
| Fully disconnecting from work | 79 (41.1) | 64 (33.3) | 143 (37.2) | 2.51 | 0.07 |
| Prayer/religion, meditation, practicing gratitude, etc. | 87 (45.3) | 96 (50.0) | 183 (45.2) | 0.84 | 0.21 |
| Maintaining a daily routine | 75 (39.1) | 87 (45.3) | 162 (42.2) | 1.54 | 0.13 |
| Exercising | 108 (56.2) | 124 (64.6) | 232 (60.4) | 2.79 | 0.06 |
| Alcohol use | 32 (16.7) | 41 (21.4) | 73 (19.0) | 1.37 | 0.15 |
| Sleeping pill use | 14 (7.3) | 8 (4.2) | 22 (5.7) | 1.74 | 0.14 |
| Prescription medications | 20 (10.4) | 19 (9.9) | 39 (10.2) | 0.03 | 0.50 |
| Illicit substance use | 14 (7.3) | 15 (7.8) | 29 (7.6) | 0.04 | 0.50 |
| Tobacco use | 9 (4.7) | 5 (2.6) | 14 (3.6) | 1.19 | 0.21 |
| Support from coworkers | 60 (31.2) | 29 (15.1) | 89 (23.2) | 14.06 | * <0.001 |
| Support from my supervisor | 29 (15.1) | 11 (5.7) | 40 (10.4) | 9.04 | * 0.002 |
| Feeling that my work is meaningful | 125 (65.1) | 61 (31.8) | 186 (48.4) | 42.71 | * <0.001 |
| Knowing I am helping to address the COVID-19 pandemic | 46 (24.0) | 59 (30.7) | 105 (25.9) | 2.22 | 0.08 |
| Having a positive impact on patients | 134 (69.8) | 27 (14.1) | 161 (41.9) | 122.45 | * <0.001 |
| Getting positive feedback from the family members of patients | 51 (26.6) | 17 (8.8) | 65 (17.7) | 20.66 | * <0.001 |
| Receiving assistance/resources to help manage non-work needs | 22 (11.5) | 22 (11.5) | 44 (11.5) | 0.00 | 0.56 |
| Maladaptive Coping Strategies (composite of alcohol, tobacco, illicit substances, sleeping pills) | 52 (27.1) | 59 (30.7) | 111 (28.9) | 0.62 | 0.25 |
| Total Responses | 192 | 192 | 384 |
References
- Maunder, R.; Hunter, J.; Vincent, L.; Bennett, J.; Peladeau, N.; Leszcz, M.; Sadavoy, J.; Verhaeghe, L.M.; Steinberg, R.; Mazzulli, T. The immediate psychological and occupational impact of the 2003 SARS outbreak in a teaching hospital. Can. Med. Assoc. J. 2003, 168, 1245–1251. [Google Scholar]
- Lancee, W.J.; Maunder, R.G.; Goldbloom, D.S. Prevalence of psychiatric disorders among Toronto hospital workers one to two years after the SARS outbreak. Psychiatr. Serv. 2008, 59, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Chew, N.W.S.; Lee, G.K.H.; Tan, B.Y.Q.; Jing, M.; Goh, Y.; Ngiam, N.J.H.; Yeo, L.L.L.; Ahmad, A.; Ahmed Khan, F.; Napolean Shanmugam, G.N.; et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav. Immun. 2020, 88, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wang, H.; Jin, X.R.; Li, X.; Pender, M.; Song, C.P.; Tang, S.-L.; Cao, J.; Wu, H.; Wang, Y.-G. Experiences and challenges in the health protection of medical teams in the Chinese Ebola treatment center, Liberia: A qualitative study. Infect. Dis. Poverty 2018, 7, 92. [Google Scholar] [CrossRef] [PubMed]
- Bodenheimer, T.; Sinsky, C. From triple to Quadruple Aim: Care of the patient requires care of the provider. Ann. Fam. Med. 2014, 12, 573–576. [Google Scholar] [CrossRef] [PubMed]
- Soto-Añari, M.; Rivera-Fernández, C.; Ramos-Vargas, L.; Denegri-Solis, L.; Herrera-Pino, J.; Camargo, L.; Camargo, L.; Castillo, E.; Díaz, M.; Gaitán-Quintero, G.; et al. Prevalence and factors associated with subjective cognitive complaints in Latin American health workers during the COVID-19 pandemic. Rev. Colomb. Psiquiatr. 2022; Epub ahead of print. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Savage, A.; Young, S.; Titley, H.K.; Thorne, T.E.; Spiers, J.; Estabrooks, C.A. This Was My Crimean War: COVID-19 Experiences of Nursing Home Leaders. J. Am. Med. Dir. Assoc. 2022, 23, 1827–1832. [Google Scholar] [CrossRef]
- Demmin, D.L.; Silverstein, S.M.; Shors, T.J. Mental and physical training with meditation and aerobic exercise improved mental health and well-being in teachers during the COVID-19 pandemic. Front. Hum. Neurosci. 2022, 16, 847301. [Google Scholar] [CrossRef]
- Chandler, A.B.; Wank, A.A.; Vanuk, J.R.; O’Connor, M.F.; Dreifuss, B.A.; Dreifuss, H.M.; Ellingson, K.D.; Khan, S.M.; Friedman, S.E.; Athey, A. Implementing Psychological First Aid for Healthcare Workers during the COVID-19 Pandemic: A Feasibility Study of the ICARE Model. J. Clin. Psychol. Med. Settings 2022. [Google Scholar] [CrossRef]
- Kwiatkowska-Ciotucha, D.; Zaluska, U.; Ślazyk-Sobol, M.; Lehesvuori, M.; Polak, A. Occupational burnout in health care—Analysis of systemic and organisational risks as well as possible preventive actions. Econometrics 2019, 23, 43–62. [Google Scholar] [CrossRef]
- Unjai, S.; Forster, E.M.; Mitchell, A.E.; Creedy, D.K. Compassion satisfaction, resilience and passion for work among nurses and physicians working in intensive care units: A mixed method systematic review. Intensive Crit. Care Nurs. 2022, 71, 103248. [Google Scholar] [CrossRef] [PubMed]
- Załuska, U.; Ślazyk-Sobol, M.; Kwiatkowska-Ciotucha, D. Burnout and Its Correlates—An Empirical Study Conducted among Education, Higher Education and Health Care Professionals. Econometrics 2018, 22, 26–38. [Google Scholar] [CrossRef]
- Ratzon, A.; Farhi, M.; Ratzon, N.; Adini, B. Resilience at Work, Burnout, Secondary Trauma, and Compassion Satisfaction of Social Workers Amidst the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 5500. [Google Scholar] [CrossRef] [PubMed]
- Lluch, C.; Galiana, L.; Doménech, P.; Sansó, N. The Impact of the COVID-19 Pandemic on Burnout, Compassion Fatigue, and Compassion Satisfaction in Healthcare Personnel: A Systematic Review of the Literature Published during the First Year of the Pandemic. Healthcare 2022, 10, 364. [Google Scholar] [CrossRef] [PubMed]
- Rathert, C.; May, D.R.; Chung, H.S. Nurse moral distress: A survey identifying predictors and potential interventions. Int. J. Nurs. Stud. 2016, 53, 39–49. [Google Scholar] [CrossRef]
- Dyrbye, L.N.; Satele, D.; Sloan, J.; Shanafelt, T.D. Utility of a Brief Screening Tool to Identify Physicians in Distress. J. Gen. Intern. Med. 2013, 28, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Dolan, E.D.; Mohr, D.; Lempa, M.; Joos, S.; Fihn, S.D.; Nelson, K.M.; Helfrich, C.D. Using a Single Item to Measure Burnout in Primary Care Staff: A Psychometric Evaluation. J. Gen. Intern. Med. 2015, 30, 582–587. [Google Scholar] [CrossRef]
- Tam, C.W.C.; Pang, E.P.F.; Lam, L.C.W.; Chiu, H.F.K. Severe acute respiratory syndrome (SARS) in Hongkong in 2003: Stress and psychological impact among frontline healthcare workers. Psychol. Med. 2004, 34, 1197–1204. [Google Scholar] [CrossRef]
- Ross, A.; Bevans, M.; Brooks, A.T.; Gibbons, S.; Wallen, G.R. Nurses and Health-Promoting Behaviors: Knowledge May Not Translate Into Self-Care. AORN J. 2017, 105, 267–275. [Google Scholar] [CrossRef]
- Dort, J.; Romanelli, J.; Choudhury, N.; Flink, B.J.; Lak, K.; Levy, S.; Needleman, B.J.; Paget, C.J.; Telem, D.; Schwarz, E.; et al. SAGES primer for taking care of yourself during and after the COVID-19 crisis. Surg. Endosc. 2020, 34, 2856–2862. [Google Scholar] [CrossRef]
- Trudel-Fitzgerald, C.; Chen, Y.; Singh, A.; Okereke, O.I.; Kubzansky, L.D. Psychiatric, Psychological, and Social Determinants of Health in the Nurses’ Health Study Cohorts. Am. J. Public Health 2016, 106, 1644–1649. [Google Scholar] [CrossRef] [PubMed]
- Linzer, M.; Poplau, S.; Grossman, E.; Varkey, A.; Yale, S.; Williams, E.; Hicks, L.; Brown, R.L.; Wallock, J.; Kohnhorst, D.; et al. A Cluster Randomized Trial of Interventions to Improve Work Conditions and Clinician Burnout in Primary Care: Results from the Healthy Work Place (HWP) Study. J. Gen. Intern. Med. 2015, 30, 1105–1111. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W.; Clark, V.L.P. Designing and Conducting Mixed Methods Research, 3rd ed.; SAGE Publications: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Shorten, A.; Smith, J. Mixed methods research: Expanding the evidence base. Evid. Based Nurs. 2017, 20, 74–75. [Google Scholar] [CrossRef] [PubMed]
- O’Cathain, A.; Murphy, E.; Nicholl, J. Three techniques for integrating data in mixed methods studies. BMJ 2010, 341, c4587. Available online: https://www.bmj.com/content/341/bmj.c4587 (accessed on 13 October 2021). [CrossRef]
- Neal, J.W.; Neal, Z.P.; Van Dyke, E.; Kornbluh, M. Expediting the Analysis of Qualitative Data in Evaluation: A Procedure for the Rapid Identification of Themes from Audio Recordings (RITA). Am. J. Eval. 2015, 36, 118–132. [Google Scholar] [CrossRef]
- Luann, D.; Fortune, M.L.M.T.; Elena Gillespie, M. The Influence of Practice Standards on Massage Therapists’ Work Experience: A Phenomenological Pilot Study. Int. J. Ther. Massage Bodyw. Res. Educ. Pract. 2010, 3, 5–11. [Google Scholar]

| Variable | Baseline Survey N = 1299 (%) | Enrolled in Prospective 1 | Weekly Responses 2 |
|---|---|---|---|
| Race | |||
| White, Non-Hispanic/Latinx | 1073 (82.6) | 762 (71.0) | 2402 (84.1) |
| Other races and ethnicities | 226 (17.4) | 156 (69.0) | 453 (15.9) |
| Gender | |||
| Women | 1118 (86.1) | 798 (71.4) | 2402 (84.1) |
| Other Identities | 181 (13.9) | 120 (66.3) | 453 (15.9) |
| Profession | |||
| Allied Health | 54 (4.2) | 37 (68.5) | 94 (3.9) |
| Massage Therapy | 592 (45.6) | 469 (79.2) | 1559 (64.5) |
| Medicine | 171 (13.2) | 96 (56.1) | 214 (8.9) |
| Mental Health | 28 (2.2) | 21 (75.0) | 43 (1.8) |
| Nursing | 273 (21.0) | 178 (65.2) | 242 (10.0) |
| Dual profession | 81 (6.2) | 56 (69.1) | 124 (5.1) |
| Other | 100 (7.7) | 61 (61.0) | 135 (5.6) |
| Which of the Following Are You Currently Concerned about Regarding Yourself? Check All That Apply: | Locked-In N (%) | Locked-Out N (%) | Total N (%) | Χ2 | p-Value |
|---|---|---|---|---|---|
| Concern that my colleagues will get sick | 77 (40.1) | 61 (31.8) | 138 (35.9) | 2.90 | 0.06 |
| Fear of getting sick and/or dying myself | 105 (54.7) | 95 (49.5) | 200 (52.1) | 1.04 | 0.18 |
| Fear of my loved ones getting sick and/or dying | 140 (72.9) | 134 (69.8) | 274 (71.4) | 0.46 | 0.29 |
| Feeling socially isolated/lonely | 100 (52.1) | 72 (37.5) | 172 (44.8) | 8.26 | 0.002 |
| Feeling like I can’t share my concerns/feelings safely with others | 73 (38.0) | 63 (32.8) | 136 (35.4) | 1.14 | 0.17 |
| Difficulty sleeping due to increased stress from the pandemic | 67 (34.9) | 73 (38.0) | 140 (36.5) | 0.40 | 0.30 |
| Difficulty making arrangements for dependent care (e.g., children, elderly relatives) | 32 (16.7) | 19 (9.9) | 51 (13.3) | 3.82 | 0.04 |
| Uncertainty about how long the pandemic will continue | 165 (85.9) | 169 (88.0) | 334 (87.0) | 0.37 | 0.32 |
| Fears of societal instability | 133 (69.3) | 124 (64.6) | 257 (66.9) | 0.95 | 0.19 |
| Personal resource worries (e.g., financial concerns, not having a will/advance directive in place, not having adequate supplies at home) | 83 (43.2) | 114 (59.4) | 197 (51.3) | 10.02 | 0.001 |
| Total Responses | 192 | 192 | 384 |
| Professional Category | Increasing Baseline Moral Distress | High Baseline Moral Distress | ||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% Confidence Interval | p-Value | Odds Ratio | 95% Confidence Interval | p-Value | |
| Allied Health | 0.26 | 0.03, 2.63 | <0.001 | 0.64 | 0.03, 8.25 | 0.98 |
| Massage Therapy | 1.51 | 0.78, 2.93 | 0.54 | 1.04 | 0.47, 2.32 | 0.22 |
| Medicine | 0.31 | 0.10, 0.96 | <0.001 | 0.14 | 0.02, | 0.23 |
| Mental Health | 1.76 | 0.26, 11.81 | 0.52 | 0.74 | 0.07, 7.42 | 0.98 |
| Nursing | 1.31 | 0.64, 2.71 | <0.001 | 1.17 | 0.51, 2.71 | 0.39 |
| Dual Profession | 1.03 | 0.44, 2.40 | <0.001 | 0.91 | 0.33, 2.50 | 0.59 |
| Other | 0.78 | 0.41, 1.49 | 0.01 | 0.81 | 0.31, 2.09 | 0.50 |
| All Professions | 0.72 | 0.52, 0.98 | 0.37 | 0.81 | 0.06, 1.05 | 0.04 |
| Scale | Outcomes | OR | 95% CI | p-Value |
|---|---|---|---|---|
| Ordinal | Moral Distress | 0.55 | 0.38, 0.81 | 0.30 |
| WBI | 1.19 | 0.82, 1.72 | 0.22 | |
| Mini-Z | 1.57 | 1.06, 2.33 | 0.20 | |
| High Scores | Moral Distress | 0.46 | 0.28, 0.73 | 0.02 |
| WBI | 1.34 | 0.81, 2.22 | 0.19 | |
| Mini-Z | 1.38 | 0.68, 2.92 | 0.16 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heavner, S.F.; Stuenkel, M.; Russ Sellers, R.; McCallus, R.; Dean, K.D.; Wilson, C.; Shuffler, M.; Britt, T.W.; Stark Taylor, S.; Benedum, M.; et al. “I Don’t Want to Go to Work”: A Mixed-Methods Analysis of Healthcare Worker Experiences from the Front- and Side-Lines of COVID-19. Int. J. Environ. Res. Public Health 2023, 20, 5953. https://doi.org/10.3390/ijerph20115953
Heavner SF, Stuenkel M, Russ Sellers R, McCallus R, Dean KD, Wilson C, Shuffler M, Britt TW, Stark Taylor S, Benedum M, et al. “I Don’t Want to Go to Work”: A Mixed-Methods Analysis of Healthcare Worker Experiences from the Front- and Side-Lines of COVID-19. International Journal of Environmental Research and Public Health. 2023; 20(11):5953. https://doi.org/10.3390/ijerph20115953
Chicago/Turabian StyleHeavner, Smith F., Mackenzie Stuenkel, Rebecca Russ Sellers, Rhiannon McCallus, Kendall D. Dean, Chloe Wilson, Marissa Shuffler, Thomas W. Britt, Shannon Stark Taylor, Molly Benedum, and et al. 2023. "“I Don’t Want to Go to Work”: A Mixed-Methods Analysis of Healthcare Worker Experiences from the Front- and Side-Lines of COVID-19" International Journal of Environmental Research and Public Health 20, no. 11: 5953. https://doi.org/10.3390/ijerph20115953
APA StyleHeavner, S. F., Stuenkel, M., Russ Sellers, R., McCallus, R., Dean, K. D., Wilson, C., Shuffler, M., Britt, T. W., Stark Taylor, S., Benedum, M., Munk, N., Mayo, R., Cartmell, K. B., Griffin, S., & Kennedy, A. B. (2023). “I Don’t Want to Go to Work”: A Mixed-Methods Analysis of Healthcare Worker Experiences from the Front- and Side-Lines of COVID-19. International Journal of Environmental Research and Public Health, 20(11), 5953. https://doi.org/10.3390/ijerph20115953