
Residential Greenspace Is Associated with Lower Levels of Depressive and Burnout Symptoms, and Higher Levels of Life Satisfaction: A Nationwide Population-Based Study in Sweden

 , ,
, ,
Abstract
:1. Introduction
2. Methods
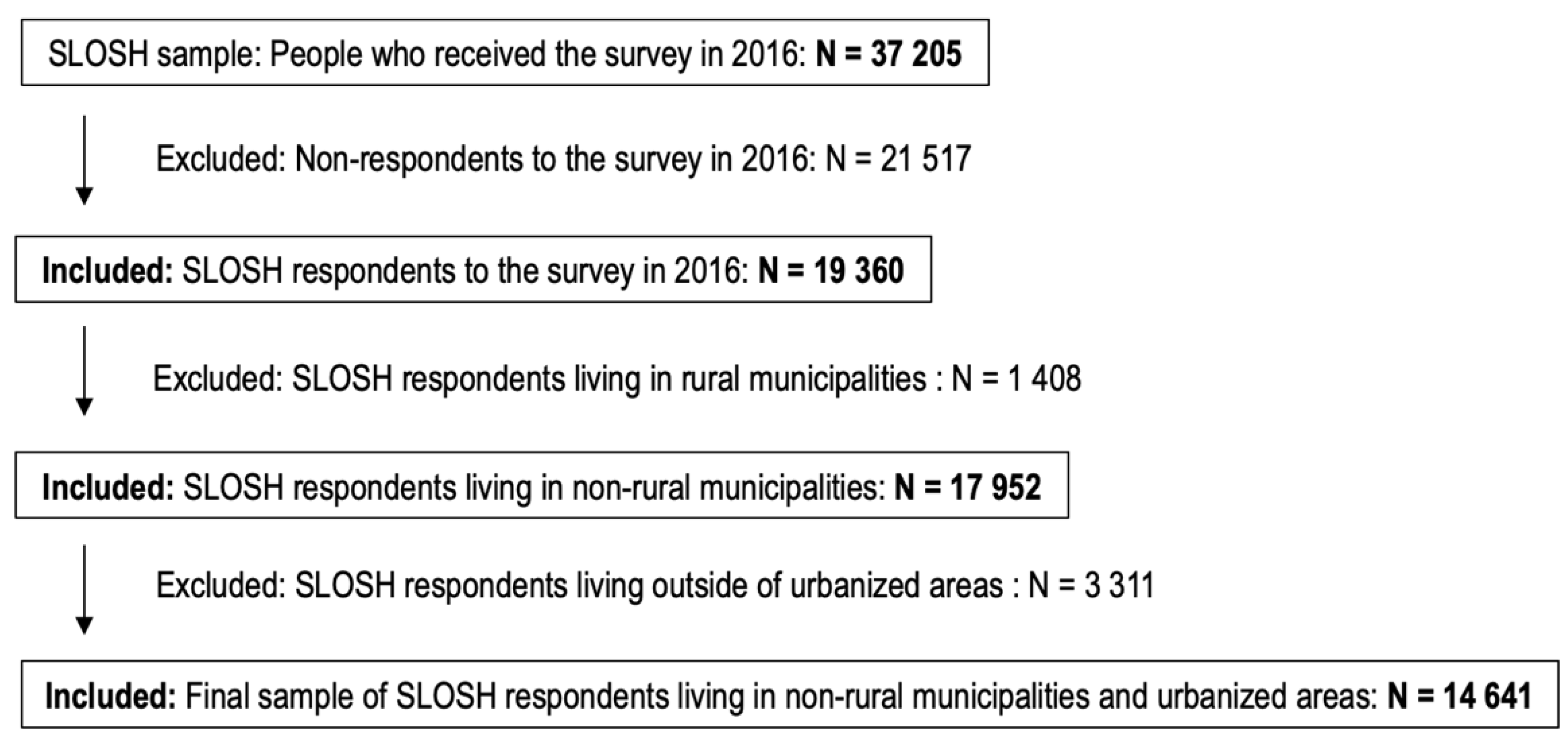
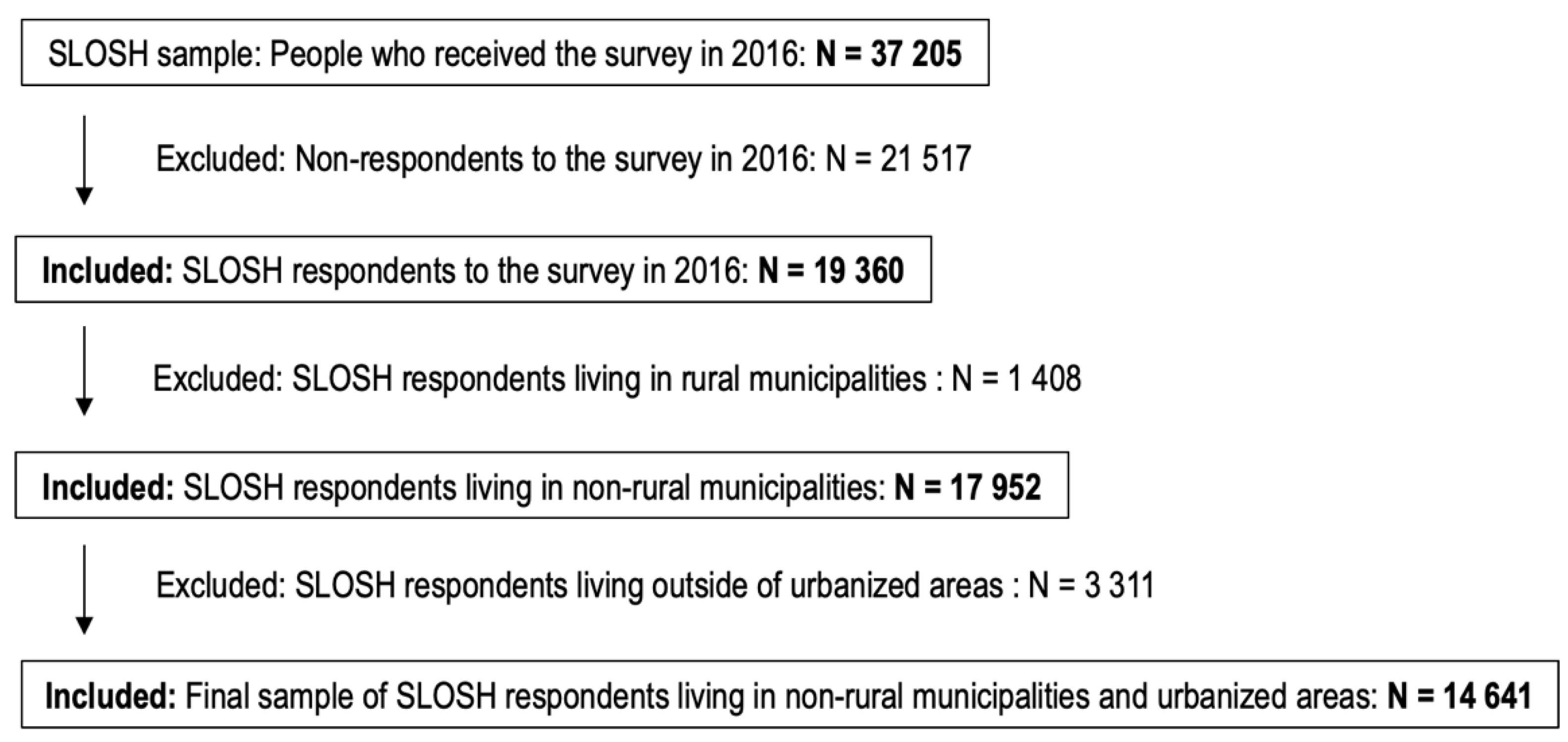
2.1. Study Population and Design
2.2. Variables
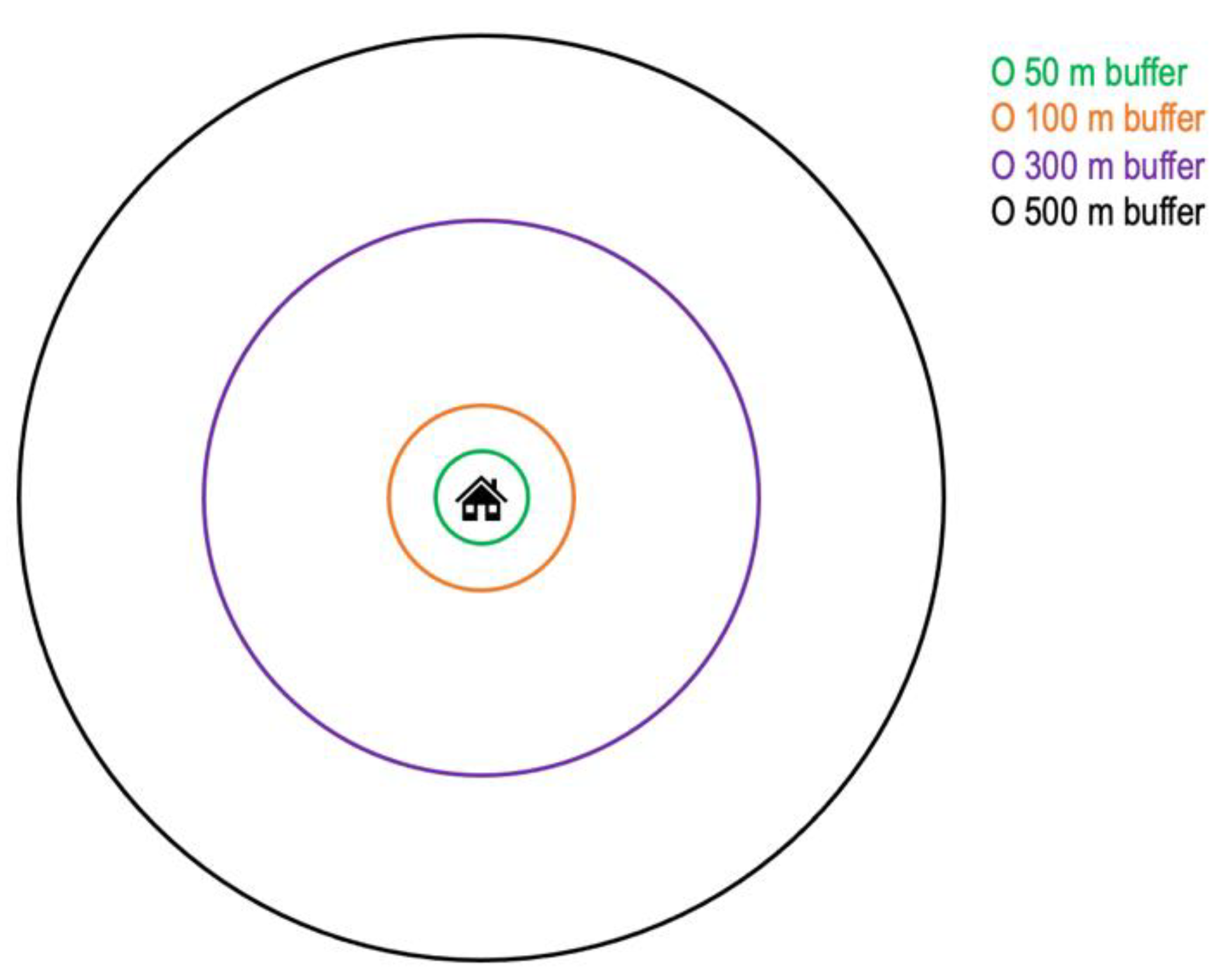
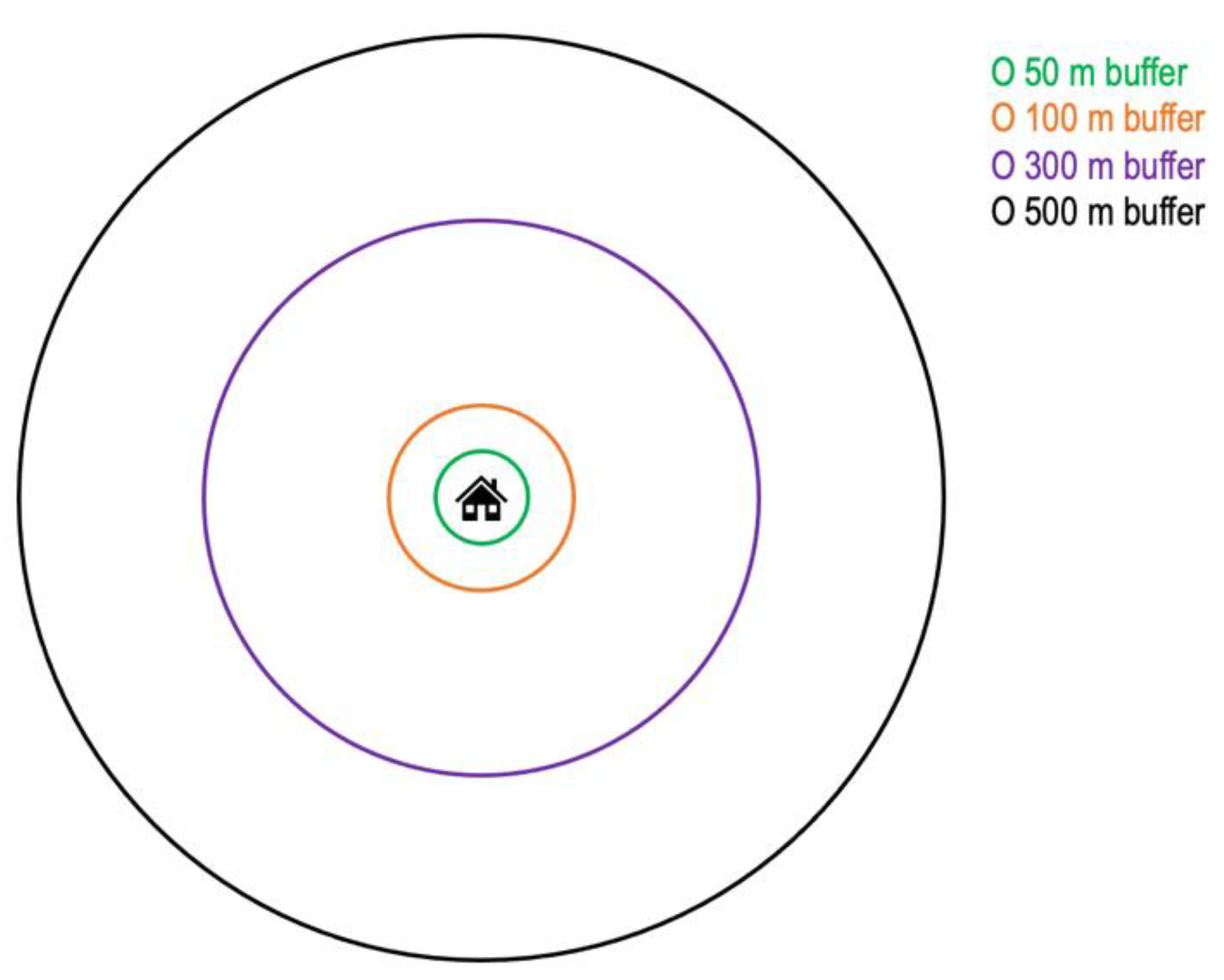
2.2.1. Residential Greenspace and Green–Blue-Space Exposure Assessment
2.2.2. Mental Health Outcomes
2.2.3. Control Variables
2.3. Statistical Analysis
3. Results
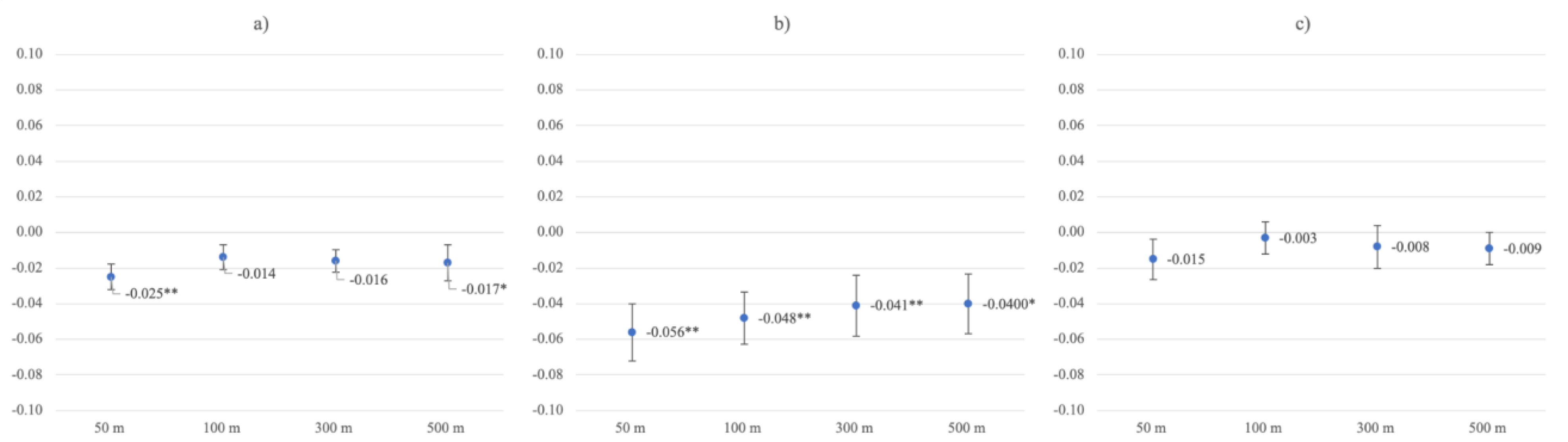
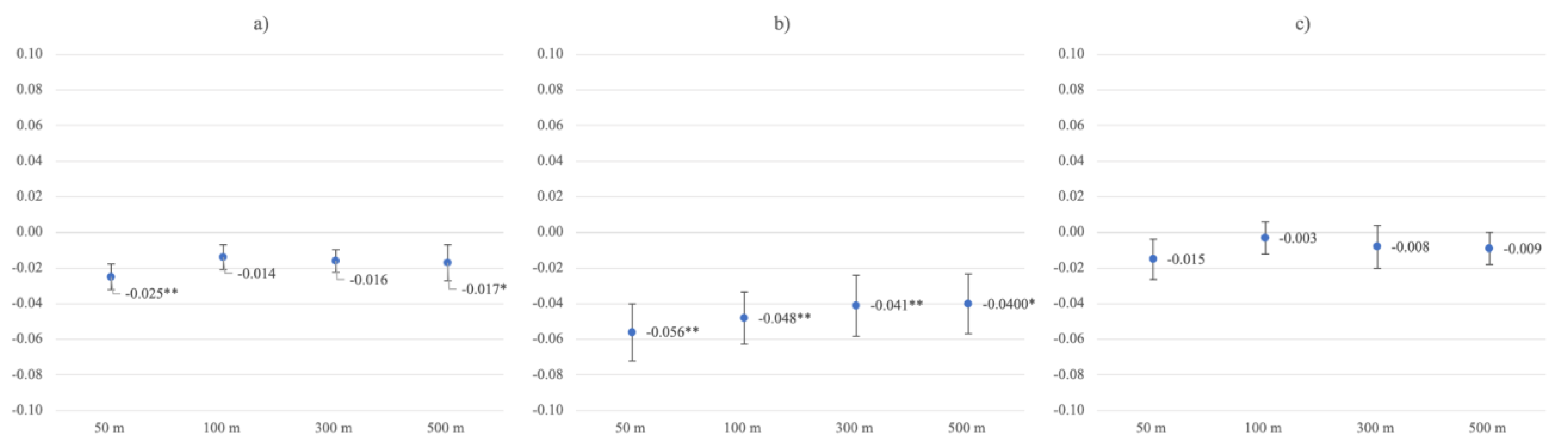
3.1. Residential Greenspace and Depressive Symptoms
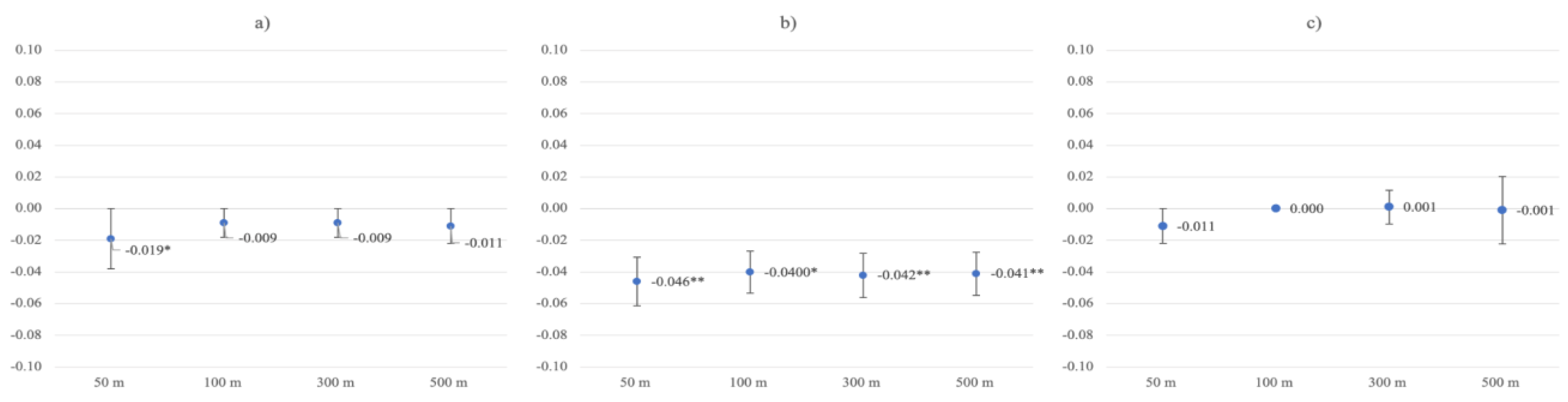
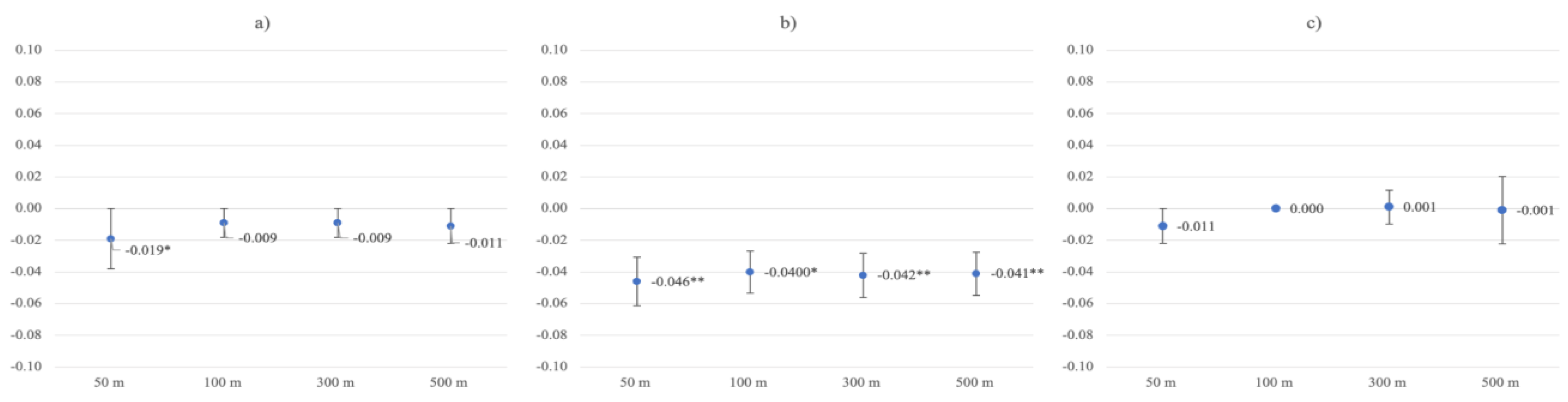
3.2. Residential Greenspace and Burnout Symptoms
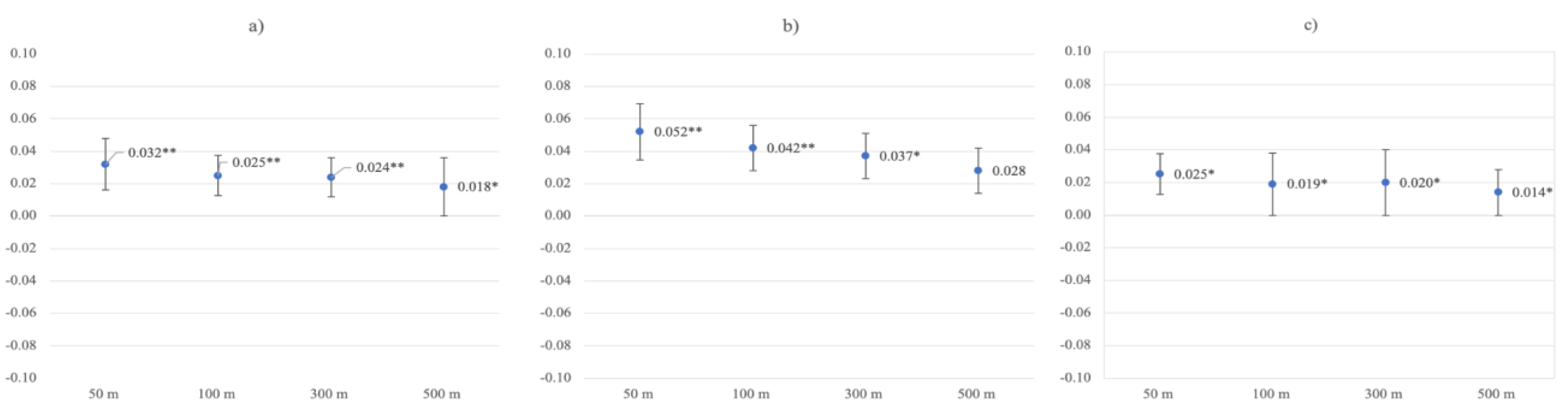
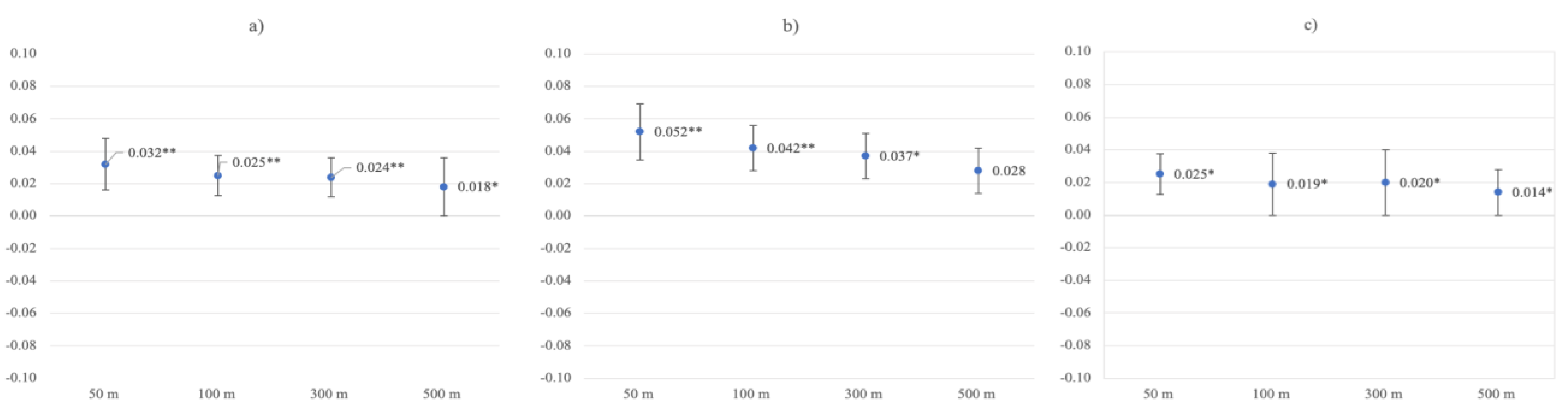
3.3. Residential Greenspace and Life Satisfaction
4. Discussion
4.1. General Discussion
4.2. Residential-Surrounding Greenspace
4.3. Context and Implications
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Rehm, J.; Shield, K.D. Global Burden of Disease and the Impact of Mental and Addictive Disorders. Curr. Psychiatry Rep. 2019, 21, 10. [Google Scholar] [CrossRef] [PubMed]
- Försäkringskassan [Swedish Social Insurance Agency]. Social Insurance in Figures. 2017. ISSN 2000-1703, ISBN 978-91-7500-400-6. Available online: www.forsakringskassan.se (accessed on 30 March 2022).
- Beddington, J.; Cooper, C.; Field, J.; Goswami, U.; Huppert, F.; Jenkins, R.; Jones, H.S.; Kirkwood, T.B.L.; Sahakian, B.; Thomas, S.M. The mental wealth of nations. Nature 2008, 455, 1057–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mills, C. From ‘Invisible Problem’ to Global Priority: The Inclusion of Mental Health in the Sustainable Development Goals. Dev. Chang. 2018, 49, 843–866. [Google Scholar] [CrossRef] [Green Version]
- Seymour, V. The Human–Nature Relationship and Its Impact on Health: A Critical Review. Front. Public Health 2016, 4, 260. [Google Scholar] [CrossRef] [Green Version]
- Roberts, M.; Irvine, K.N.; McVittie, A. Associations between greenspace and mental health prescription rates in urban areas. Urban For. Urban Green. 2021, 64, 127301. [Google Scholar] [CrossRef]
- Stenfors, C.U.D.; van Hedger, S.C.; Schertz, K.E.; Meyer, F.A.C.; Smith, K.E.L.; Norman, G.J.; Bourrier, S.C.; Enns, J.T.; Kardan, O.; Jonides, J.; et al. Positive Effects of Nature on Cognitive Performance Across Multiple Experiments: Test Order but Not Affect Modulates the Cognitive Effects. Front. Psychol. 2019, 10, 1413. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, R. The Nature of the View from Home. Environ. Behav. 2001, 33, 507–542. [Google Scholar] [CrossRef]
- Bratman, G.N.; Daily, G.C.; Levy, B.J.; Gross, J.J. The benefits of nature experience: Improved affect and cognition. Landsc. Urban Plan. 2015, 138, 41–50. [Google Scholar] [CrossRef]
- Mcmahan, E.A.; Estes, D. The effect of contact with natural environments on positive and negative affect: A meta-analysis. J. Posit. Psychol. 2015, 10, 507–519. [Google Scholar] [CrossRef]
- Wilson, E.O. Biophilia; Harvard University Press: Cambridge, MA, USA, 1984. [Google Scholar]
- Ulrich, R.S. View through a window may influence recovery from surgery. Science 1984, 224, 420–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press: Cambridge, UK, 1989. [Google Scholar]
- White, M.P.; Alcock, I.; Wheeler, B.W.; Depledge, M.H. Would You Be Happier Living in a Greener Urban Area? A Fixed-Effects Analysis of Panel Data. Psychol. Sci. 2013, 24, 920–928. [Google Scholar] [CrossRef] [PubMed]
- Beyer, K.M.M.; Kaltenbach, A.; Szabo, A.; Bogar, S.; Nieto, F.J.; Malecki, K.M. Exposure to Neighborhood Green Space and Mental Health: Evidence from the Survey of the Health of Wisconsin. Int. J. Environ. Res. Public Health 2014, 11, 3453–3472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarkar, C.; Webster, C.; Gallacher, J. Residential greenness and prevalence of major depressive disorders: A cross-sectional, observational, associational study of 94 879 adult UK Biobank participants. Lancet Planet. Health 2018, 2, e162–e173. [Google Scholar] [CrossRef]
- Egorov, A.I.; Griffin, S.M.; Converse, R.R.; Styles, J.N.; Sams, E.A.; Wilson, A.; Jackson, L.E.; Wade, T.J. Vegetated land cover near residence is associated with reduced allostatic load and improved biomarkers of neuroendocrine, metabolic and immune functions. Environ. Res. 2017, 158, 508–521. [Google Scholar] [CrossRef] [PubMed]
- Roe, J.J.; Thompson, C.W.; Aspinall, P.A.; Brewer, M.J.; Duff, E.I.; Miller, D.; Mitchell, R.; Clow, A. Green Space and Stress: Evidence from Cortisol Measures in Deprived Urban Communities. Int. J. Environ. Res. Public Health 2013, 10, 4086–4103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Vries, S.; Verheij, R.A.; Groenewegen, P.P.; Spreeuwenberg, P. Natural Environments—Healthy Environments? An Exploratory Analysis of the Relationship between Greenspace and Health. Environ. Plan. A 2003, 35, 1717–1731. [Google Scholar] [CrossRef] [Green Version]
- Maas, R.A.J.; Verheij, P.P.; Groenewegen, S.; de Vries, J.M.; Spreeuwenberg, P. Green space, urbanity, and health: How strong is the relation? J. Epidemiol. Community Health 2006, 60, 587–592. [Google Scholar] [CrossRef] [Green Version]
- White, M.P.; Pahl, S.; Wheeler, B.; Depledge, M.H.; Fleming, L.E. Natural environments and subjective wellbeing: Different types of exposure are associated with different aspects of wellbeing. Health Place 2017, 45, 77–84. [Google Scholar] [CrossRef]
- Astell-Burt, T.; Navakatikyan, M.; Eckermann, S.; Hackett, M.; Feng, X. Is urban green space associated with lower mental healthcare expenditure? Soc. Sci. Med. 2022, 292, 114503. [Google Scholar] [CrossRef]
- Labib, S.M.; Lindley, S.; Huck, J.J. Spatial dimensions of the influence of urban green-blue spaces on human health: A systematic review. Environ. Res. 2020, 180, 108869. [Google Scholar] [CrossRef] [PubMed]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; de Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J.; et al. Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef] [PubMed]
- Georgiou, M.; Morison, G.; Smith, N.; Tieges, Z.; Chastin, S. Mechanisms of Impact of Blue Spaces on Human Health: A Systematic Literature Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 2486. [Google Scholar] [CrossRef] [PubMed]
- Amoly, E.; Dadvand, P.; Forns, J.; López-Vicente, M.; Basagaña, X.; Julvez, J.; Alvarez-Pedrerol, M.; Nieuwenhuijsen, M.J.; Sunyer, J. Green and Blue Spaces and Behavioral Development in Barcelona Schoolchildren: The BREATHE Project. Environ. Health Perspect. 2014, 122, 1351–1358. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, B.W.; White, M.; Stahl-Timmins, W.; Depledge, M.H. Does living by the coast improve health and wellbeing? Health Place 2012, 18, 1198–1201. [Google Scholar] [CrossRef] [Green Version]
- White, M.P.; Alcock, I.; Wheeler, B.; Depledge, M.H. Coastal proximity, health and well-being: Results from a longitudinal panel survey. Health Place 2013, 23, 97–103. [Google Scholar] [CrossRef] [Green Version]
- Hanson, L.L.M.; Leineweber, C.; Persson, V.; Hyde, M.; Theorell, T.; Westerlund, H. Cohort Profile: The Swedish Longitudinal Occupational Survey of Health (SLOSH). Int. J. Epidemiol. 2018, 47, 691–692i. [Google Scholar] [CrossRef] [Green Version]
- The Swedish Association of Local Authorities and Regions. 2016. Available online: https://skr.se/download/18.5627773817e39e979ef5e9f5/1642509656973/5519.pdf (accessed on 23 March 2022).
- DeSO—Demografiska Statistikområden, (n.d.). Available online: https://www.scb.se/hitta-statistik/regional-statistik-och-kartor/regionala-indelningar/deso---demografiska-statistikomraden/ (accessed on 30 January 2022).
- SCB—Statistics Sweden, Grönytor och Grönområden i Tätorter 2015. 2019. Available online: https://www.scb.se/contentassets/e2ef67822f8043549f1554b4f7759bb7/mi0805_2015a01_br_miftbr1901.pdf (accessed on 13 January 2022).
- Hanson, L.L.M.; Westerlund, H.; Leineweber, C.; Rugulies, R.; Osika, W.; Theorell, T.; Bech, P. The Symptom Checklist-core depression (SCL-CD6) scale: Psychometric properties of a brief six item scale for the assessment of depression. Scand. J. Public Health 2014, 42, 82–88. [Google Scholar] [CrossRef]
- Grossi, G.; Perski, A.; Ekstedt, M.; Johansson, T.; Lindström, M.; Holm, K. The morning salivary cortisol response in burnout. J. Psychosom. Res. 2005, 59, 103–111. [Google Scholar] [CrossRef]
- Melamed, S.; Kushnir, T.; Shirom, A. Burnout and Risk Factors for Cardiovascular Diseases. Behav. Med. 1992, 18, 53–60. [Google Scholar] [CrossRef]
- Shirom, A.; Westman, M.; Shamai, O.; Carel, R.S. Effects of work overload and burnout on cholesterol and triglycerides levels: The moderating efffects of emotional reactivity among male and female employees. J. Occup. Health Psychol. 1997, 2, 275–288. [Google Scholar] [CrossRef] [PubMed]
- Melamed, S.; Ugarten, U.; Shirom, A.; Kahana, L.; Lerman, Y.; Froom, P. Chronic burnout, somatic arousal and elevated salivary cortisol levels. J. Psychosom. Res. 1999, 46, 591–598. [Google Scholar] [CrossRef]
- Singh-Manoux, A.; Adler, N.E.; Marmot, M. Subjective social status: Its determinants and its association with measures of ill-health in the Whitehall II study. Soc. Sci. Med. 2002, 56, 1321–1333. [Google Scholar] [CrossRef]
- Cheung, F.; Lucas, R. Assessing the validity of single-item life satisfaction measures: Results from three large samples. Qual. Life Res. 2014, 23, 2809–2818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annual Average Exchange Rates (Aggregate)|Sveriges Riksbank, (n.d.). Available online: https://www.riksbank.se/en-gb/statistics/search-interest--exchange-rates/annual-average-exchange-rates/?y=2015&m=12&s=Comma&f=y (accessed on 23 March 2022).
- Longitudinal integrated database for health insurance and labour market studies, LISA. 2019. Available online: https://www.scb.se/en/services/ordering-data-and-statistics/ordering-microdata/vilka-mikrodata-finns/longitudinella-register/longitudinal-integrated-database-for-health-insurance-and-labour-market-studies-lisa/ (accessed on 30 March 2022).
- Alegría, M.; NeMoyer, A.; Bagué, I.F.; Wang, Y.; Alvarez, K. Social Determinants of Mental Health: Where We Are and Where We Need to Go. Curr. Psychiatry Rep. 2018, 20, 95. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.; Loureiro, A.; Cardoso, G. Social determinants of mental health: A review of the evidence. Eur. J. Psychiatry 2016, 30, 259–292. Available online: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0213-61632016000400004&lng=es&nrm=iso&tlng=en (accessed on 11 February 2022).
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 5th ed.; Pearson International Edition: Boston, MA, USA, 2007. [Google Scholar]
- Taylor, L.; Hahs, A.K.; Hochuli, D.F. Wellbeing and urban living: Nurtured by nature. Urban Ecosyst. 2018, 21, 197–208. [Google Scholar] [CrossRef]
- Van Dillen, S.M.E.; de Vries, S.; Groenewegen, P.P.; Spreeuwenberg, P. Greenspace in urban neighbourhoods and residents’ health: Adding quality to quantity. J. Epidemiol. Commun. Health 2012, 66, e8. [Google Scholar] [CrossRef] [Green Version]
- Alvarsson, J.J.; Wiens, S.; Nilsson, M.E. Stress Recovery during Exposure to Nature Sound and Environmental Noise. Int. J. Environ. Res. Public Health 2010, 7, 1036–1046. [Google Scholar] [CrossRef]
- Hedblom, M.; Gunnarsson, B.; Iravani, B.; Knez, I.; Schaefer, M.; Thorsson, P.; Lundström, J. Reduction of physiological stress by urban green space in a multisensory virtual experiment. Sci. Rep. 2019, 9, 10113. [Google Scholar] [CrossRef] [Green Version]
- Bratman, G.N.; Hamilton, J.P.; Hahn, K.S.; Daily, G.C.; Gross, J.J. Nature experience reduces rumination and subgenual prefrontal cortex activation. Proc. Natl. Acad. Sci. USA 2015, 112, 8567–8572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevenson, M.P.; Schilhab, T.; Bentsen, P. Attention Restoration Theory II: A systematic review to clarify attention processes affected by exposure to natural environments. J. Toxicol. Environ. Health Part B 2018, 21, 227–268. [Google Scholar] [CrossRef] [PubMed]
- Mayer, F.S.; Frantz, C.M.; Bruehlman-Senecal, E.; Dolliver, K.; Bielagus, E.; Doohan, C.; Friedman, M.; Kaplan, S.; Keeler-Wolf, E.; Luce, Z.; et al. Why Is Nature Beneficial? The Role of Connectedness to Nature. Environ. Behav. 2008, 41, 607–643. [Google Scholar] [CrossRef]
- Pritchard, A.; Richardson, M.; Sheffield, D.; McEwan, K. The Relationship Between Nature Connectedness and Eudaimonic Well-Being: A Meta-analysis. J. Happiness Stud. 2020, 21, 1145–1167. [Google Scholar] [CrossRef] [Green Version]
- Statistics Sweden. The Labour Market during the COVID-19 Pandemic, 2021; SCB Statistics Sweden: Stockholm, Sweden, 2021. [Google Scholar]
- Kananen, L.; Enroth, L.; Raitanen, J.; Jylhävä, J.; Bürkle, A.; Moreno-Villanueva, M.; Bernhardt, J.; Toussaint, O.; Grubeck-Loebenstein, B.; Malavolta, M.; et al. Self-rated health in individuals with and without disease is associated with multiple biomarkers representing multiple biological domains. Sci. Rep. 2021, 11, 6139. [Google Scholar] [CrossRef]
- Jordan, P.J.; Troth, A.C. Common method bias in applied settings: The dilemma of researching in organizations. Aust. J. Manag. 2020, 45, 3–14. [Google Scholar] [CrossRef]
- Fisher, G.G.; Matthews, R.A.; Gibbons, A.M. Developing and investigating the use of single-item measures in organizational research. J. Occup. Health Psychol. 2016, 21, 3–23. [Google Scholar] [CrossRef]
- Diener, E.; Inglehart, R.; Tay, L. Theory and Validity of Life Satisfaction Scales. Soc. Indic. Res. 2013, 112, 497–527. [Google Scholar] [CrossRef]
- Allen, M.S.; Iliescu, D.; Greiff, S. Single Item Measures in Psychological Science: A Call to Action. Eur. J. Psychol. Assess. 2022, 38, 1–5. [Google Scholar] [CrossRef]
- Song, Y.; Huang, B.; Cai, J.; Chen, B. Dynamic assessments of population exposure to urban greenspace using multi-source big data. Sci. Total Environ. 2018, 634, 1315–1325. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total Sample (n = 14,641) | Working (n = 10,365) | Non-Working (n = 4276) |
|---|---|---|---|
| Mean depressive symptoms score (SD) | 4.91 (5.03) | 5.21 (5.06) | 4.20 (4.89) |
| Mean burnout score (SD) | 2.43 (1.25) | 2.54 (1.24) | 2.15 (1.23) |
| Mean life satisfaction score (SD) | 5.82 (1.24) | 5.77 (1.23) | 5.92 (1.25) |
| Mean RGS in percent | |||
| 50 m buffer zone (SD) 100 m buffer zone (SD) 300 m buffer zone (SD) 500 m buffer zone (SD) | 54.08 (19.40) 56.01 (18.43) 56.82 (17.00) 56.13 (16.40) | 54.24 (19.40) 56.14 (18.53) 56.93 (17.09) 56.22 (16.47) | 53.70 (19.39) 55.69 (18.23) 56.54 (16.79) 55.92 (16.22) |
| Mean GBS in percent | |||
| 50 m buffer zone (SD) 100 m buffer zone (SD) 300 m buffer zone (SD) 500 m buffer zone (SD) | 54.31 (19.25) 56.68 (18.12) 59.20 (16.30) 60.05 (15.50) | 54.43 (19.27) 56.75 (18.21) 59.23 (16.39) 60.08 (15.58) | 54.00 (19.20) 56.52 (17.89) 59.11 (16.07) 59.98 (15.29) |
| Count (%) Mean average neighborhood income in SEK | |||
| Low income, <= 2205 Lower medium income, 2206–2495 Higher medium income, 2496–2908 High income, 2909+ | 2760 (18.9) 3517 (24.0) 3975 (27.1) 4390 (30.0) | 1837 (17.7) 2440 (23.5) 2833 (27.3) 3255 (31.4) | 923 (21.6) 1077 (25.2) 1141 (26.7) 1135 (26.5) |
| Count (%) Mean individual income in 100’s SEK | |||
| Low income, <= 2175 Lower medium income, 2176–2818 Higher medium income, 2819–3617 High income, 3618 + | 3116 (21.3) 3341 (22.8) 3757 (25.7) 4427 (30.2) | 1022 (9.9) 2505 (24.2) 3103 (29.9) 3735 (36.0) | 2094 (49.0) 836 (19.6) 654 (15.3) 692 (16.2) |
| Mean age | 55.40 (11.70) | 51.43 (9.76) | 65.04 (10.35) |
| Count women (%) | 8303 (56.7) | 5 921 (57.1) | 2382 (55.7) |
| Count men (%) | 6338 (43.3) | 4444 (42.9) | 1894 (44.3) |
| Count married or cohabiting (%) | 11,207 (76.5) | 8025 (77.4) | 3182 (74.4) |
| Count Single (%) | 3232 (22.1) | 2238 (21.6) | 994 (23.2) |
| 50 m Buffer | 100 m Buffer | 300 m Buffer | 500 m Buffer | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model, N = 14,290 | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p |
| 1 | −0.025 | −0.007 | −0.011, −0.002 | 0.002 | −0.014 | −0.004 | −0.008, 0.001 | 0.084 | −0.016 | −0.005 | −0.010, 0.000 | 0.056 | −0.017 | −0.005 | −0.010, 0.000 | 0.045 |
| 2 | −0.016 | −0.004 | −0.008, 0.000 | 0.045 | −0.008 | −0.002 | −0.006, 0.002 | 0.353 | −0.012 | −0.004 | −0.008, 0.001 | 0.132 | −0.013 | −0.004 | −0.009, 0.001 | 0.104 |
| 3 | −0.018 | −0.005 | −0.009, −0.000 | 0.032 | −0.008 | −0.002 | −0.007, −0.002 | 0.317 | −0.013 | −0.004 | −0.008, −0.001 | 0.126 | −0.014 | −0.004 | −0.009, 0.001 | 0.089 |
| 4 | −0.017 | −0.004 | −0.009, 0.000 | 0.037 | −0.008 | −0.002 | −0.007, 0.002 | 0.314 | −0.014 | −0.004 | −0.009, 0.001 | 0.096 | −0.015 | −0.005 | −0.010, 0.000 | 0.058 |
| 5 | 0.000 | 0.000 | −0.004, 0.004 | 0.959 | 0.009 | 0.002 | −0.002, 0.007 | 0.274 | 0.001 | 0.000 | −0.005, 0.005 | 0.920 | −0.003 | −0.001 | −0.006, 0.004 | 0.718 |
| 50 m Buffer | 100 m Buffer | 300 m Buffer | 500 m Buffer | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model, N = 4120 | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p |
| 1 | −0.056 | −0.014 | −0.022, −0.006 | 0.000 | −0.048 | −0.013 | −0.021, −0.005 | 0.002 | −0.041 | −0.012 | −0.021, −0.003 | 0.008 | −0.040 | −0.012 | −0.021, −0.003 | 0.011 |
| 2 | −0.038 | −0.010 | −0.017, −0.002 | 0.013 | −0.032 | −0.009 | −0.017, −0.001 | 0.033 | −0.029 | −0.009 | −0.017, 0.000 | 0.054 | −0.028 | −0.008 | −0.017, 0.001 | 0.070 |
| 3 | −0.040 | −0.010 | −0.018, −0.003 | 0.008 | −0.034 | −0.009 | −0.017, −0.001 | 0.025 | −0.030 | −0.009 | −0.017, 0.000 | 0.045 | −0.030 | −0.009 | −0.018, 0.000 | 0.048 |
| 4 | −0.042 | −0.011 | −0.018, −0.003 | 0.006 | −0.037 | −0.010 | −0.018, −0.002 | 0.014 | −0.036 | −0.010 | −0.019, −0.002 | 0.019 | −0.036 | −0.011 | −0.020, −0.002 | 0.018 |
| 5 | −0.024 | −0.006 | −0.014, 0.001 | 0.113 | −0.019 | −0.005 | −0.013, 0.003 | 0.220 | −0.020 | −0.006 | −0.014, 0.003 | 0.183 | −0.023 | −0.007 | 0.016, 0.002 | 0.135 |
| 50 m Buffer | 100 m Buffer | 300 m Buffer | 500 m Buffer | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model, N = 14,303 | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p |
| 1 | −0.019 | −0.001 | −0.002, 0.000 | 0.023 | −0.009 | −0.001 | −0.002, 0.001 | 0.285 | −0.009 | −0.001 | −0.002, 0.001 | 0.270 | −0.011 | −0.001 | −0.002, 0.000 | 0.206 |
| 2 | −0.008 | −0.001 | −0.002, 0.000 | 0.306 | −0.001 | 0.000 | −0.001, 0.001 | 0.917 | −0.005 | 0.000 | −0.002, 0.001 | 0.537 | −0.007 | −0.001 | −0.002, 0.001 | 0.415 |
| 3 | −0.010 | −0.001 | −0.002, 0.000 | 0.205 | −0.002 | 0.000 | −0.001, 0.001 | 0.822 | −0.005 | 0.000 | −0.002, 0.001 | 0.515 | −0.008 | −0.001 | −0.002, 0.001 | 0.345 |
| 4 | −0.010 | −0.001 | −0.002, 0.000 | 0.235 | −0.002 | 0.000 | −0.001, 0.001 | 0.824 | −0.006 | 0.000 | −0.002, 0.001 | 0.430 | −0.009 | −0.001 | −0.002, 0.001 | 0.255 |
| 5 | 0.003 | 0.000 | −0.001, 0.001 | 0.727 | 0.011 | 0.001 | 0.000, 0.002 | 0.174 | 0.004 | 0.000 | −0.001, 0.002 | 0.589 | 0.000 | 0.000 | −0.001, 0.001 | 0.991 |
| 50 m Buffer | 100 m Buffer | 300 m Buffer | 500 m Buffer | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model, N = 4116 | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p |
| 1 | −0.046 | −0.003 | −0.005, 0.001 | 0.003 | −0.040 | −0.003 | −0.005, 0.001 | 0.011 | −0.042 | −0.003 | −0.005, 0.001 | 0.006 | −0.041 | −0.003 | −0.005, 0.001 | 0.008 |
| 2 | −0.023 | −0.001 | −0.003, 0.000 | 0.118 | −0.019 | −0.001 | −0.003, 0.001 | 0.198 | −0.027 | −0.002 | −0.004, 0.000 | 0.067 | −0.026 | −0.002 | −0.004, 0.000 | 0.084 |
| 3 | −0.025 | −0.002 | −0.003, 0.000 | 0.089 | −0.020 | −0.001 | −0.003, 0.001 | 0.168 | −0.028 | −0.002 | −0.004, 0.000 | 0.057 | −0.028 | −0.002 | −0.004, 0.000 | 0.061 |
| 4 | −0.026 | −0.002 | −0.003, 0.000 | 0.077 | −0.023 | −0.002 | −0.003, 0.000 | 0.127 | −0.032 | −0.002 | −0.004, 0.000 | 0.032 | −0.032 | −0.002 | −0.005, 0.000 | 0.032 |
| 5 | −0.016 | −0.001 | −0.003, 0.001 | 0.282 | −0.012 | −0.001 | −0.003, 0.001 | 0.416 | −0.023 | −0.002 | −0.004, 0.000 | 0.120 | −0.024 | −0.002 | −0.004, 0.000 | 0.100 |
| 50 m Buffer | 100 m Buffer | 300 m Buffer | 500 m Buffer | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model, N = 14,279 | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p |
| 1 | 0.032 | 0.002 | 0.001, 0.003 | 0.000 | 0.025 | 0.002 | 0.001, 0.003 | 0.003 | 0.024 | 0.002 | 0.001, 0.003 | 0.004 | 0.018 | 0.001 | 0.000, 0.003 | 0.034 |
| 2 | 0.029 | 0.002 | 0.001, 0.003 | 0.000 | 0.023 | 0.002 | 0.000, 0.003 | 0.005 | 0.024 | 0.002 | 0.001, 0.003 | 0.004 | 0.018 | 0.001 | 0.000, 0.003 | 0.035 |
| 3 | 0.032 | 0.002 | 0.001, 0.003 | 0.000 | 0.025 | 0.002 | 0.001, 0.003 | 0.003 | 0.024 | 0.002 | 0.001, 0.003 | 0.003 | 0.019 | 0.001 | 0.000, 0.003 | 0.022 |
| 4 | 0.032 | 0.002 | 0.001, 0.003 | 0.000 | 0.025 | 0.002 | 0.001, 0.003 | 0.003 | 0.026 | 0.002 | 0.001, 0.003 | 0.002 | 0.021 | 0.002 | 0.000, 0.003 | 0.011 |
| 5 | −0.003 | 0.000 | −0.001, 0.001 | 0.748 | −0.010 | −0.001 | −0.002, 0.000 | 0.206 | −0.004 | 0.000 | −0.001, 0.001 | 0.650 | −0.005 | 0.000 | −0.002, 0.001 | 0.563 |
| 50 m Buffer | 100 m Buffer | 300 m Buffer | 500 m Buffer | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model, N = 4102 | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p |
| 1 | 0.052 | 0.003 | 0.001, 0.005 | 0.001 | 0.042 | 0.003 | 0.001, 0.005 | 0.007 | 0.037 | 0.003 | 0.000, 0.005 | 0.018 | 0.028 | 0.002 | 0.000, 0.005 | 0.072 |
| 2 | 0.046 | 0.003 | 0.001, 0.005 | 0.003 | 0.037 | 0.003 | 0.001, 0.005 | 0.018 | 0.034 | 0.003 | 0.000, 0.005 | 0.027 | 0.025 | 0.002 | 0.000, 0.004 | 0.103 |
| 3 | 0.049 | 0.003 | 0.001, 0.005 | 0.001 | 0.039 | 0.003 | 0.001, 0.005 | 0.012 | 0.036 | 0.003 | 0.000, 0.005 | 0.020 | 0.029 | 0.002 | 0.000, 0.005 | 0.063 |
| 4 | 0.051 | 0.003 | 0.001, 0.005 | 0.001 | 0.042 | 0.003 | 0.001, 0.005 | 0.006 | 0.041 | 0.003 | 0.001, 0.005 | 0.008 | 0.034 | 0.003 | 0.000, 0.005 | 0.026 |
| 5 | 0.021 | 0.001 | −0.001, 0.003 | 0.162 | 0.012 | 0.001 | −0.001, 0.003 | 0.447 | 0.016 | 0.001 | −0.001, 0.003 | 0.306 | 0.013 | 0.001 | −0.001, 0.003 | 0.405 |
| 50 m Buffer | 100 m Buffer | 300 m Buffer | 500 m Buffer | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model, N = 10,177 | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p | β | B | Lower, upper (95% CI of B) | p |
| 1 | 0.025 | 0.002 | 0.000, 0.003 | 0.012 | 0.019 | 0.001 | 0.000, 0.003 | 0.053 | 0.020 | 0.001 | 0.000, 0.003 | 0.043 | 0.014 | 0.001 | 0.000, 0.003 | 0.149 |
| 2 | 0.023 | 0.001 | 0.000, 0.003 | 0.019 | 0.018 | 0.001 | 0.000, 0.002 | 0.068 | 0.020 | 0.001 | 0.000, 0.003 | 0.044 | 0.014 | 0.001 | 0.000, 0.003 | 0.149 |
| 3 | 0.026 | 0.002 | 0.000, 0.003 | 0.008 | 0.019 | 0.001 | 0.000, 0.003 | 0.050 | 0.020 | 0.001 | 0.000, 0.003 | 0.042 | 0.015 | 0.001 | 0.000, 0.003 | 0.122 |
| 4 | 0.026 | 0.002 | 0.000, 0.003 | 0.008 | 0.019 | 0.001 | 0.000, 0.003 | 0.047 | 0.021 | 0.002 | 0.000, 0.003 | 0.032 | 0.017 | 0.001 | 0.000, 0.003 | 0.085 |
| 5 | −0.010 | −0.001 | −0.002, 0.001 | 0.298 | −0.018 | −0.001 | −0.002, 0.000 | 0.072 | −0.010 | −0.001 | −0.002, 0.001 | 0.299 | −0.010 | −0.001 | −0.002, 0.001 | 0.283 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klein, Y.; Lindfors, P.; Osika, W.; Magnusson Hanson, L.L.; Stenfors, C.U.D. Residential Greenspace Is Associated with Lower Levels of Depressive and Burnout Symptoms, and Higher Levels of Life Satisfaction: A Nationwide Population-Based Study in Sweden. Int. J. Environ. Res. Public Health 2022, 19, 5668. https://doi.org/10.3390/ijerph19095668
Klein Y, Lindfors P, Osika W, Magnusson Hanson LL, Stenfors CUD. Residential Greenspace Is Associated with Lower Levels of Depressive and Burnout Symptoms, and Higher Levels of Life Satisfaction: A Nationwide Population-Based Study in Sweden. International Journal of Environmental Research and Public Health. 2022; 19(9):5668. https://doi.org/10.3390/ijerph19095668
Chicago/Turabian StyleKlein, Yannick, Petra Lindfors, Walter Osika, Linda L. Magnusson Hanson, and Cecilia U. D. Stenfors. 2022. "Residential Greenspace Is Associated with Lower Levels of Depressive and Burnout Symptoms, and Higher Levels of Life Satisfaction: A Nationwide Population-Based Study in Sweden" International Journal of Environmental Research and Public Health 19, no. 9: 5668. https://doi.org/10.3390/ijerph19095668
APA StyleKlein, Y., Lindfors, P., Osika, W., Magnusson Hanson, L. L., & Stenfors, C. U. D. (2022). Residential Greenspace Is Associated with Lower Levels of Depressive and Burnout Symptoms, and Higher Levels of Life Satisfaction: A Nationwide Population-Based Study in Sweden. International Journal of Environmental Research and Public Health, 19(9), 5668. https://doi.org/10.3390/ijerph19095668