
In the Shadow of the Casinos: The Relationship between Religion and Health in Macau


Abstract
:1. Introduction
2. Theoretical Background
2.1. Altruism as a Mediating Mechanism for Religion and Health
2.2. Prejudice as a Mediating Mechanism for Religion and Health
2.3. Religion, Life Satisfaction, and Health
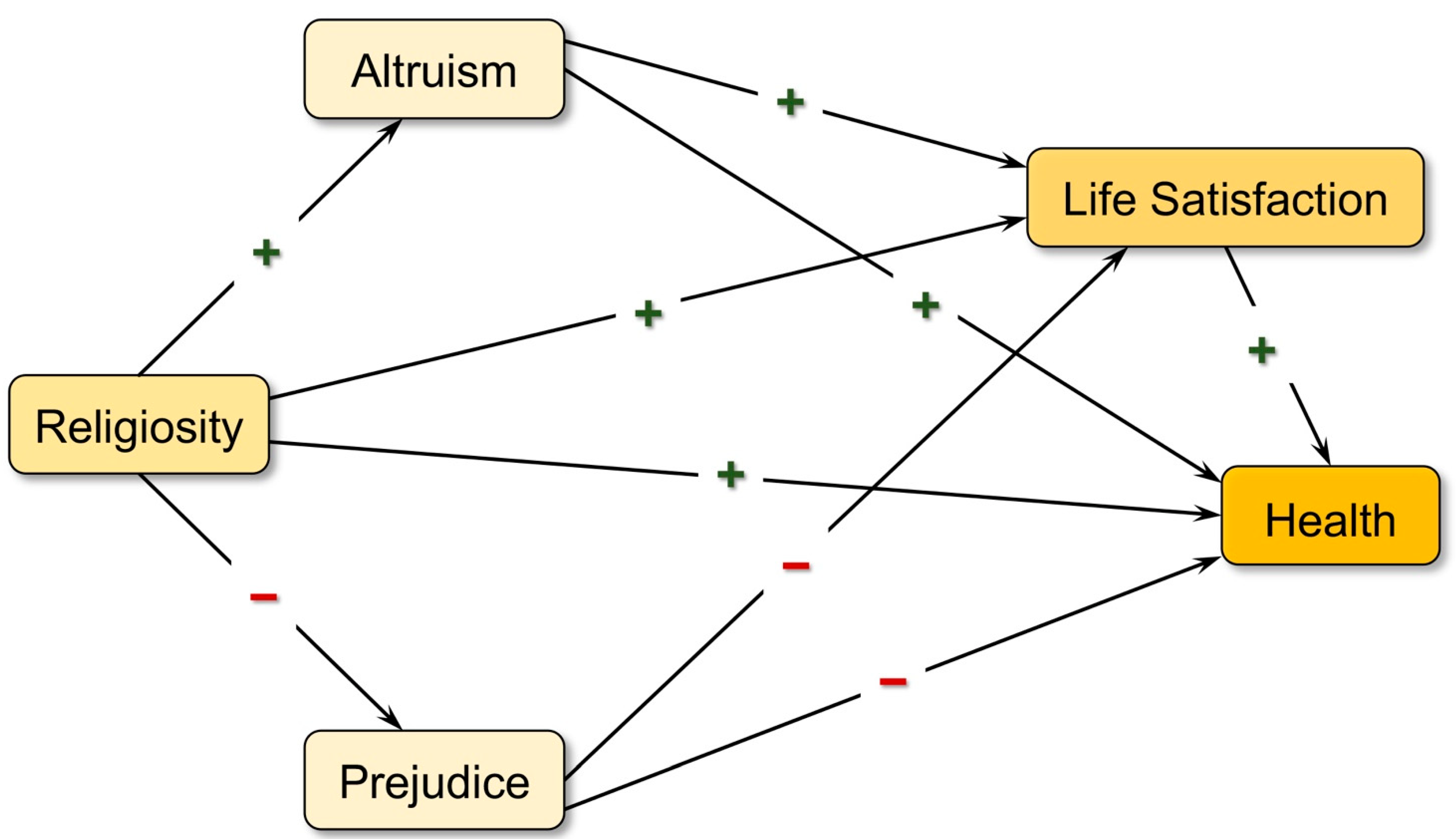
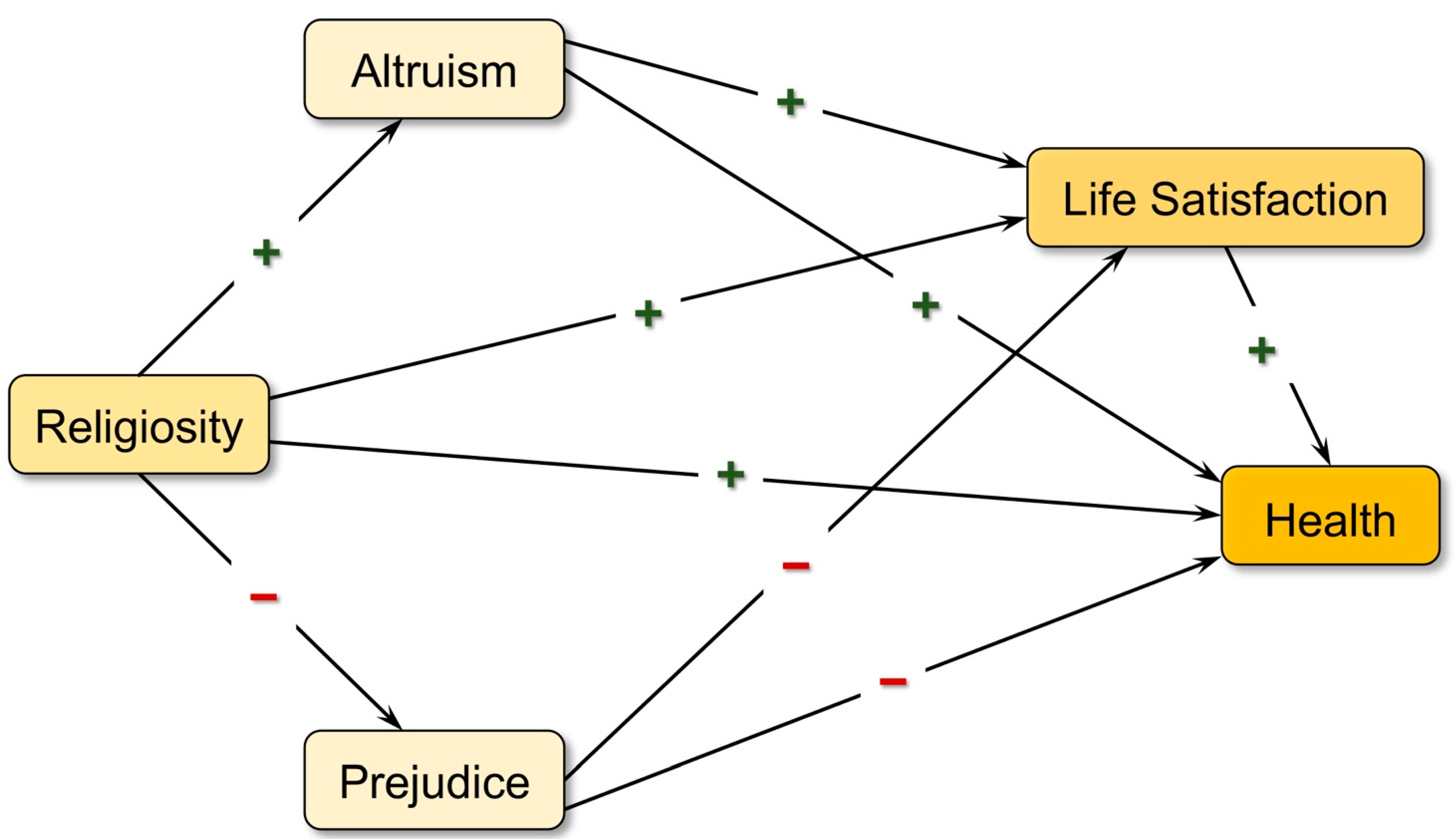
3. Current Study
4. Methods
4.1. Sample and Data
4.2. Variables and Measures
5. Results
5.1. Characteristics of the Sample
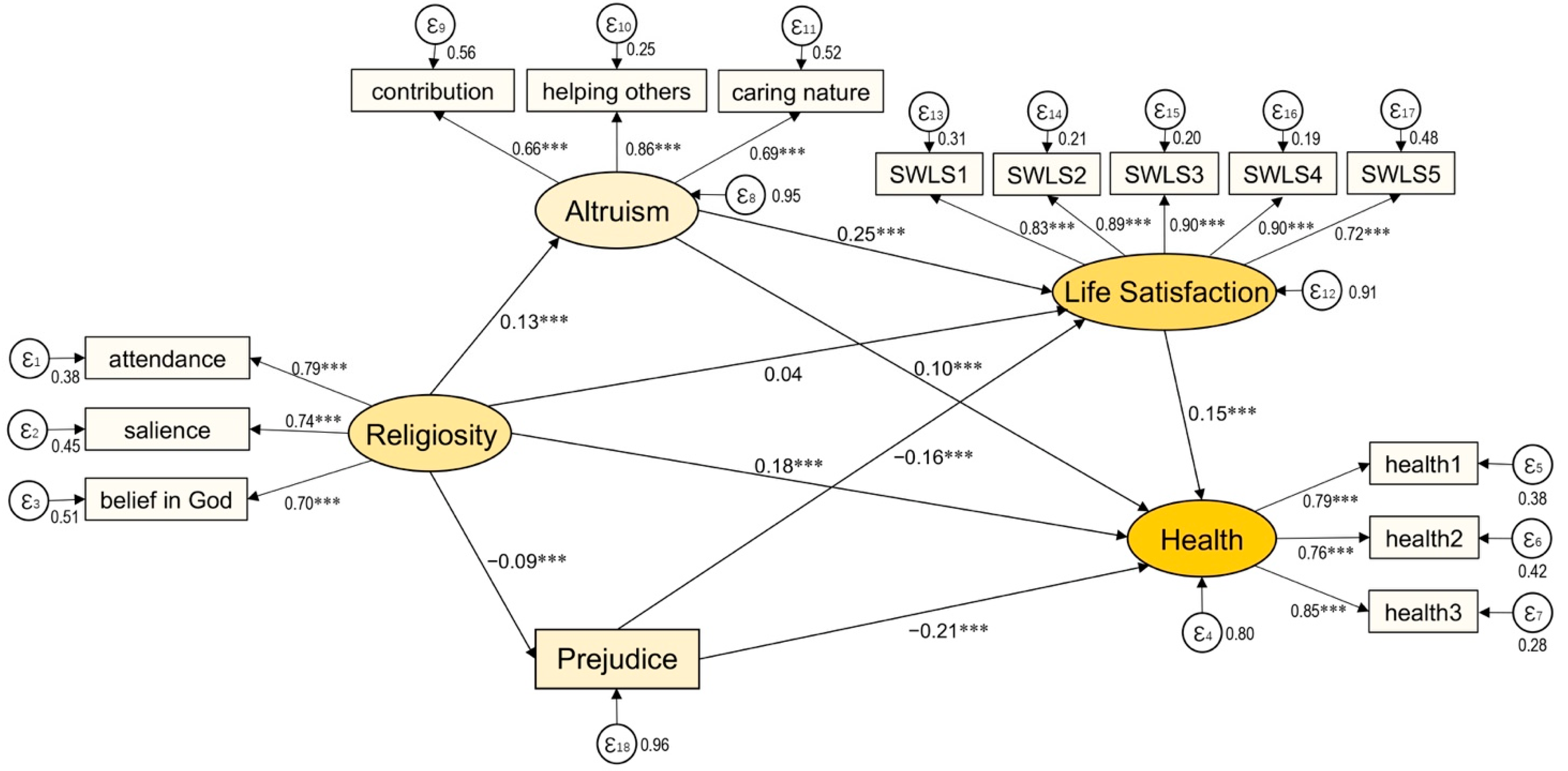
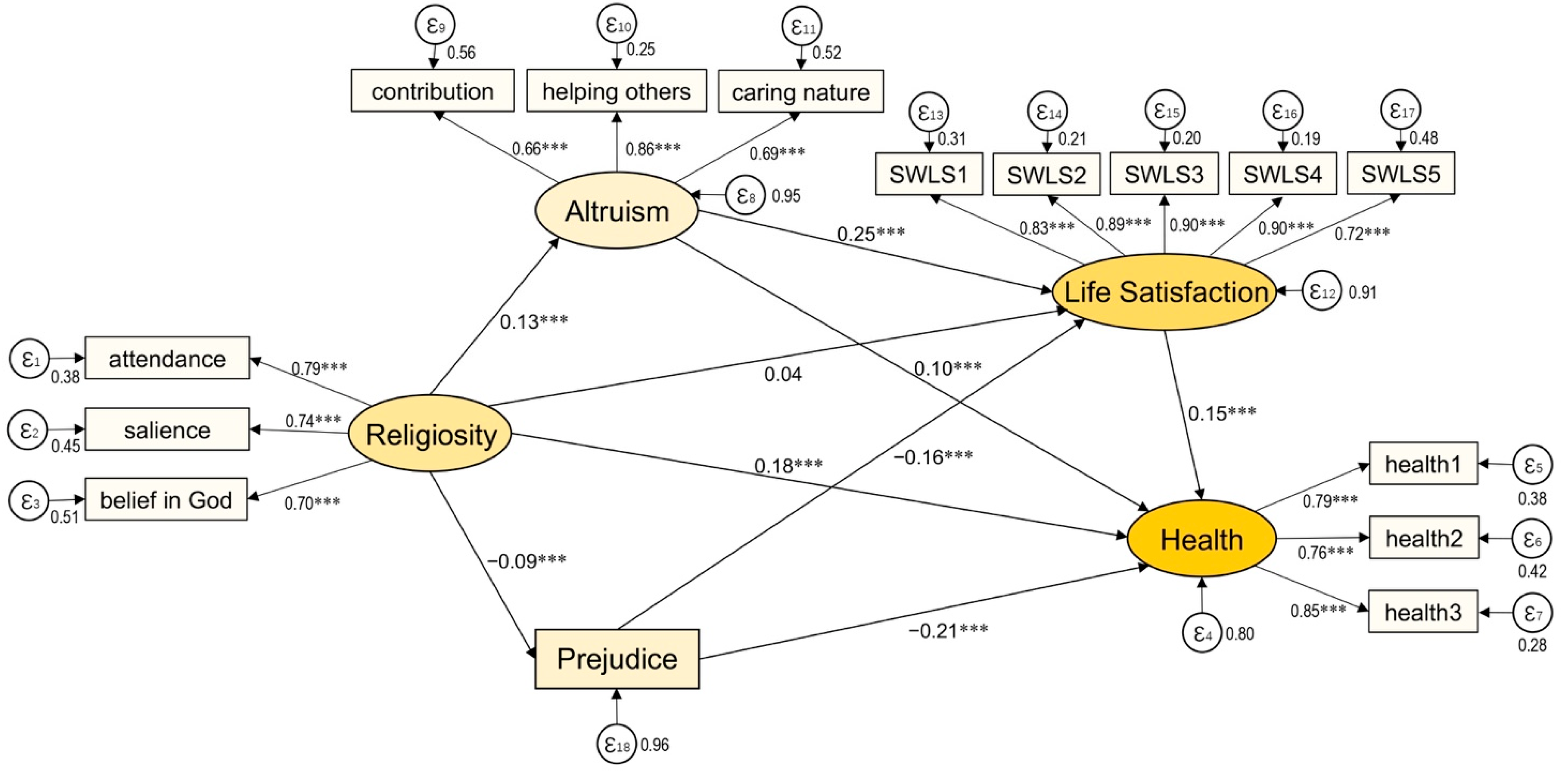
5.2. Results of Structural Equation Models
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Construct | Indicator | Factor Loading |
|---|---|---|
| Religiosity | Religious activity attendance | 0.79 *** |
| Religious salience | 0.74 *** | |
| Belief in God | 0.70 *** | |
| Life Satisfaction | Life is close to ideal | 0.83 *** |
| Conditions are excellent | 0.89 *** | |
| Satisfied with life | 0.90 *** | |
| Have important things | 0.90 *** | |
| Would change almost nothing | 0.72 *** | |
| Altruism | Social contribution | 0.66 *** |
| Helping others | 0.86 *** | |
| Caring for nature | 0.69 *** | |
| Overall Health | Perceived health condition compared to peer | 0.79 *** |
| Perceived health condition compared to last year | 0.76 *** | |
| Perceived overall health | 0.85 *** |
References
- Godlove, T.F. Kant and the Meaning of Religion: The Critical Philosophy and Modern Religious Thought; Bloomsbury Publishing: London, UK, 2014. [Google Scholar]
- Callahan, D. The WHO definition of ‘health’. Hastings Cent. Stud. 1973, 1, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Park, N.S.; Klemmack, D.L.; Roff, L.L.; Parker, M.W.; Koenig, H.G.; Sawyer, P.; Allman, R.M. Religiousness and longitudinal trajectories in elders’ functional status. Res. Aging 2008, 30, 279–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berges, I.-M.; Kuo, Y.-F.; Markides, K.S.; Ottenbacher, K. Attendance at religious services and physical functioning after stroke among older Mexican Americans. Exp. Aging Res. 2007, 33, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Koenig, H.G.; George, L.K.; Titus, P. Religion, spirituality, and health in medically ill hospitalized older patients. J. Am. Geriatr. Soc. 2004, 52, 554–562. [Google Scholar] [CrossRef]
- Reyes-Ortiz, C.A.; Pelaez, M.; Koenig, H.G.; Mulligan, T. Religiosity and self-rated health among Latin American and Caribbean elders. Int. J. Psychiatry Med. 2007, 37, 425–443. [Google Scholar] [CrossRef]
- McCullough, M.E.; Laurenceau, J.-P. Religiousness and the trajectory of self-rated health across adulthood. Personal. Soc. Psychol. Bull. 2005, 31, 560–573. [Google Scholar] [CrossRef] [Green Version]
- Levin, J.S.; Chatters, L.M.; Taylor, R.J. Religious effects on health status and life satisfaction among Black Americans. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 1995, 50, S154–S163. [Google Scholar] [CrossRef]
- Greene, K.V.; Yoon, B.J. Religiosity, economics and life satisfaction. Rev. Soc. Econ. 2004, 62, 245–261. [Google Scholar] [CrossRef]
- Sethi, S.; Seligman, M.E. The hope of fundamentalists. Psychol. Sci. 1994, 5, 58. [Google Scholar] [CrossRef]
- Murphy, P.E.; Ciarrocchi, J.W.; Piedmont, R.L.; Cheston, S.; Peyrot, M.; Fitchett, G. The relation of religious belief and practices, depression, and hopelessness in persons with clinical depression. J. Consult. Clin. Psychol. 2000, 68, 1102. [Google Scholar] [CrossRef]
- Ai, A.L.; Peterson, C.; Bolling, S.F.; Koenig, H. Private prayer and optimism in middle-aged and older patients awaiting cardiac surgery. Gerontologist 2002, 42, 70–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krause, N. Religious doubt and psychological well-being: A longitudinal investigation. Rev. Relig. Res. 2006, 47, 287–302. [Google Scholar]
- Okun, M.A. Predictors of volunteer status in a retirement community. Int. J. Aging Hum. Dev. 1993, 36, 57–74. [Google Scholar] [CrossRef] [PubMed]
- Harris, A.H.; Thoresen, C.E. Volunteering is associated with delayed mortality in older people: Analysis of the longitudinal study of aging. J. Health Psychol. 2005, 10, 739–752. [Google Scholar] [CrossRef] [PubMed]
- Saroglou, V.; Pichon, I.; Trompette, L.; Verschueren, M.; Dernelle, R. Prosocial behavior and religion: New evidence based on projective measures and peer ratings. J. Sci. Study Relig. 2005, 44, 323–348. [Google Scholar] [CrossRef] [Green Version]
- Ecklund, E.H.; Park, J.Z. Religious diversity and community volunteerism among Asian Americans. J. Sci. Study Relig. 2007, 46, 233–244. [Google Scholar] [CrossRef]
- Koenig, H.G.; George, L.K.; Peterson, B.L. Religiosity and remission of depression in medically ill older patients. Am. J. Psychiatry 1998, 155, 536–542. [Google Scholar] [CrossRef] [Green Version]
- Koenig, H.G. Religion and remission of depression in medical inpatients with heart failure/pulmonary disease. J. Nerv. Ment. Dis. 2007, 195, 389–395. [Google Scholar] [CrossRef]
- Krause, N. Religious involvement, gratitude, and change in depressive symptoms over time. Int. J. Psychol. Relig. 2009, 19, 155–172. [Google Scholar] [CrossRef]
- Harold, G.; Linda, K.G. Religion and anxiety disorder: An examination and comparison of associations in young, middle-aged, and elderly adults. J. Anxiety H’mnierr 1993, 7, 321–342. [Google Scholar]
- Azhar, M.Z.; Varma, S.L.; Dharap, A.S. Religious psychotherapy in anxiety disorder patients. Acta Psychiatr. Scand. 1994, 90, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Nisbet, P.A.; Duberstein, P.R.; Conwell, Y.; Seidlitz, L. The effect of participation in religious activities on suicide versus natural death in adults 50 and older. J. Nerv. Ment. Dis. 2000, 188, 543–546. [Google Scholar] [CrossRef]
- Rasic, D.T.; Belik, S.-L.; Elias, B.; Katz, L.Y.; Enns, M.; Sareen, J.; Team, S.C.S.P. Spirituality, religion and suicidal behavior in a nationally representative sample. J. Affect. Disord. 2009, 114, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Steinman, K.J.; Ferketich, A.K.; Sahr, T. The dose-response relationship of adolescent religious activity and substance use: Variation across demographic groups. Health Educ. Behav. 2008, 35, 22–43. [Google Scholar] [CrossRef] [PubMed]
- Harrell, Z.A.; Broman, C.L. Racial/ethnic differences in correlates of prescription drug misuse among young adults. Drug Alcohol Depend. 2009, 104, 268–271. [Google Scholar] [CrossRef]
- Koenig, H.G. Religion, spirituality, and health: The research and clinical implications. Int. Sch. Res. Not. 2012, 2012, 278730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemmati, R.; Bidel, Z.; Nazarzadeh, M.; Valadi, M.; Berenji, S.; Erami, E.; Al Zaben, F.; Koenig, H.G.; Sanjari Moghaddam, A.; Teymoori, F. Religion, spirituality and risk of coronary heart disease: A matched case–control study and meta-analysis. J. Relig. Health 2019, 58, 1203–1216. [Google Scholar] [CrossRef]
- Horne, B.D.; May, H.T.; Anderson, J.L.; Kfoury, A.G.; Bailey, B.M.; McClure, B.S.; Renlund, D.G.; Lappé, D.L.; Carlquist, J.F.; Fisher, P.W. Usefulness of routine periodic fasting to lower risk of coronary artery disease in patients undergoing coronary angiography. Am. J. Cardiol. 2008, 102, 814–819. [Google Scholar] [CrossRef] [Green Version]
- Walsh, A. Religion and hypertension: Testing alternative explanations among immigrants. Behav. Med. 1998, 24, 122–130. [Google Scholar] [CrossRef]
- Gillum, R.F.; Ingram, D.D. Frequency of attendance at religious services, hypertension, and blood pressure: The Third National Health and Nutrition Examination Survey. Psychosom. Med. 2006, 68, 382–385. [Google Scholar] [CrossRef]
- Colantonio, A.; Kasl, S.V.; Ostfeld, A.M. Depressive symptoms and other psychosocial factors as predictors of stroke in the elderly. Am. J. Epidemiol. 1992, 136, 884–894. [Google Scholar] [CrossRef] [PubMed]
- Van Ness, P.H.; Kasl, S.V. Religion and cognitive dysfunction in an elderly cohort. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2003, 58, S21–S29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corsentino, E.A.; Collins, N.; Sachs-Ericsson, N.; Blazer, D.G. Religious attendance reduces cognitive decline among older women with high levels of depressive symptoms. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2009, 64, 1283–1289. [Google Scholar] [CrossRef] [PubMed]
- Jim, H.S.; Pustejovsky, J.E.; Park, C.L.; Danhauer, S.C.; Sherman, A.C.; Fitchett, G.; Merluzzi, T.V.; Munoz, A.R.; George, L.; Snyder, M.A. Religion, spirituality, and physical health in cancer patients: A meta-analysis. Cancer 2015, 121, 3760–3768. [Google Scholar] [CrossRef]
- Reisi, S.; Ahmadi, S.M.; Sadeghi, K.; Reisi, S.; Ahmadi, S.M. The Effect of Religion and Spirituality on Anxiety and Depression in Cancer Patients: A Review Article. Medicine 2021, 6, 75–86. [Google Scholar]
- Gonçalves, J.P.d.B.; Lucchetti, G.; Menezes, P.R.; Vallada, H. Complementary religious and spiritual interventions in physical health and quality of life: A systematic review of randomized controlled clinical trials. PLoS ONE 2017, 12, e0186539. [Google Scholar]
- Blumenthal, J.A.; Babyak, M.A.; Ironson, G.; Thoresen, C.; Powell, L.; Czajkowski, S.; Burg, M.; Keefe, F.J.; Steffen, P.; Catellier, D. Spirituality, religion, and clinical outcomes in patients recovering from an acute myocardial infarction. Psychosom. Med. 2007, 69, 501–508. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Stampfer, M.J.; Williams, D.R.; VanderWeele, T.J. Association of religious service attendance with mortality among women. JAMA Intern. Med. 2016, 176, 777–785. [Google Scholar] [CrossRef]
- Williams, D.R.; Sternthal, M.J. Spirituality, Religion and Health: Evidence and Research Directions. 2007. Available online: https://www.mja.com.au/system/files/issues/186_10_210507/wil11060_fm.pdf (accessed on 10 February 2022).
- Koenig, H.G.; Larson, D.B.; Larson, S.S. Religion and coping with serious medical illness. Ann. Pharmacother. 2001, 35, 352–359. [Google Scholar] [CrossRef]
- Koenig, H.G.; Hays, J.C.; Larson, D.B.; George, L.K.; Cohen, H.J.; McCullough, M.E.; Meador, K.G.; Blazer, D.G. Does religious attendance prolong survival? A six-year follow-up study of 3,968 older adults. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 1999, 54, M370–M376. [Google Scholar]
- VanderWeele, T.J. Religion and health in Europe: Cultures, countries, context. Eur. J. Epidemiol. 2017, 32, 857–861. [Google Scholar] [CrossRef] [PubMed]
- Koenig, H.G. Religion, congestive heart failure, and chronic pulmonary disease. J. Relig. Health 2002, 41, 263–278. [Google Scholar] [CrossRef]
- Powell, L.H.; Shahabi, L.; Thoresen, C.E. Religion and spirituality: Linkages to physical health. Am. Psychol. 2003, 58, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassibba, R.; Papagna, S.; Calabrese, M.T.; Costantino, E.; Paterno, A.; Granqvist, P. The role of attachment to God in secular and religious/spiritual ways of coping with a serious disease. Ment. Health Relig. Cult. 2014, 17, 252–261. [Google Scholar] [CrossRef]
- Koenig, H.G.; George, L.K.; Titus, P.; Meador, K.G. Religion, spirituality, and acute care hospitalization and long-term care use by older patients. Arch. Intern. Med. 2004, 164, 1579–1585. [Google Scholar] [CrossRef]
- Stavrova, O. Religion, self-rated health, and mortality: Whether religiosity delays death depends on the cultural context. Soc. Psychol. Personal. Sci. 2015, 6, 911–922. [Google Scholar] [CrossRef]
- Guo, Q.; Liu, Z.; Tian, Q. Religiosity and prosocial behavior at national level. Psychol. Relig. Spiritual. 2020, 12, 55. [Google Scholar] [CrossRef]
- Naghi, J.J.; Philip, K.J.; Phan, A.; Cleenewerck, L.; Schwarz, E.R. The effects of spirituality and religion on outcomes in patients with chronic heart failure. J. Relig. Health 2012, 51, 1124–1136. [Google Scholar] [CrossRef]
- Hvidt, N.C.; Hvidtjørn, D.; Christensen, K.; Nielsen, J.B.; Søndergaard, J. Faith moves mountains—mountains move faith: Two opposite epidemiological forces in research on religion and health. J. Relig. Health 2017, 56, 294–304. [Google Scholar] [CrossRef] [Green Version]
- Number of Casinos in Macao 2010–2020. Available online: https://www.statista.com/statistics/253763/number-of-casinos-in-macao/ (accessed on 27 January 2022).
- Loi, K.-I.; Kim, W.G. Macao’s casino industry: Reinventing Las Vegas in Asia. Cornell Hosp. Q. 2010, 51, 268–283. [Google Scholar] [CrossRef]
- Wang, F.; Meng, L.-R.; Zhang, Q.E.; Li, L.; Nogueira, B.O.L.; Ng, C.H.; Ungvari, G.S.; Liu, L.; Zhao, W.; Jia, F.-J. Sleep disturbance and its relationship with quality of life in older Chinese adults living in nursing homes. Perspect. Psychiatr. Care 2019, 55, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Lok, G.K.I.; Ng, M.W.I.; Zhu, M.M.X.; Chao, S.K.K.; Li, S.X. Mediating effect of religious belief on death anxiety in Chinese adolescents: A cross-sectional study. Int. J. Sch. Health 2019, 6, 14–20. [Google Scholar]
- Li, S.D.; Cai, T.; Wang, H.; Kuo, S.-Y. Macau Social Survey; Wu-Nan Book Inc: Miaoli County, Taiwan, 2020; ISBN 978-986-522-001-3. [Google Scholar]
- Life Expectancy at Birth, Total (Years). Available online: https://data.worldbank.org/indicator/SP.DYN.LE00.IN (accessed on 3 February 2022).
- Manuti, A.; Scardigno, R.; Mininni, G. Me, myself, and God: Religion as a psychocultural resource of meaning in later life. Cult. Psychol. 2016, 22, 3–34. [Google Scholar] [CrossRef]
- Silberman, I. Religion as a meaning system: Implications for the new millennium. J. Soc. Issues 2005, 61, 641–663. [Google Scholar] [CrossRef]
- Schwartz, S.H.; Sagiv, L. Identifying culture-specifics in the content and structure of values. J. Cross-Cult. Psychol. 1995, 26, 92–116. [Google Scholar] [CrossRef]
- Post, S.G. Altruism, happiness, and health: It’s good to be good. Int. J. Behav. Med. 2005, 12, 66–77. [Google Scholar] [CrossRef]
- Hasanović, M.; Pajević, I. Religious moral beliefs as mental health protective factor of war veterans suffering from PTSD, depressiveness, anxiety, tobacco and alcohol abuse in comorbidity. Psychiatr. Danub. 2010, 22, 203–210. [Google Scholar]
- Gomes, F.C.; Andrade, A.G.d.; Izbicki, R.; Moreira-Almeida, A.; Oliveira, L.G.d. Religion as a protective factor against drug use among Brazilian university students: A national survey. Braz. J. Psychiatry 2013, 35, 29–37. [Google Scholar] [CrossRef] [Green Version]
- Homan, K.J.; Boyatzis, C.J. Religiosity, sense of meaning, and health behavior in older adults. Int. J. Psychol. Relig. 2010, 20, 173–186. [Google Scholar] [CrossRef]
- Chen, M. A Mental Examination—Using Personality to predict Happiness, Altruism and Health. In Proceedings of the SHS Web of Conferences, Beaverton, OR, USA, 14 January 2019; p. 01006. [Google Scholar]
- Reed, P.B.; Selbee, L.K. Formal and Informal Volunteering and Giving: Regional and Community Patterns in Canada; Statistics Canada: Ottawa, ON, Canada, 2000. [Google Scholar]
- Oman, D.; Thoresen, C.E.; McMahon, K. Volunteerism and mortality among the community-dwelling elderly. J. Health Psychol. 1999, 4, 301–316. [Google Scholar] [CrossRef]
- Schwartz, C.; Meisenhelder, J.B.; Ma, Y.; Reed, G. Altruistic social interest behaviors are associated with better mental health. Psychosom. Med. 2003, 65, 778–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, C.E.; Sendor, R.M. Helping others helps oneself: Response shift effects in peer support. Soc. Sci. Med. 1999, 48, 1563–1575. [Google Scholar] [CrossRef]
- Ashwini, U.; Indumathy, J. Altruism and general well-being among adults. Int. J. Res. Soc. Sci. 2018, 8, 528–540. [Google Scholar]
- Kahana, E.; Bhatta, T.; Lovegreen, L.D.; Kahana, B.; Midlarsky, E. Altruism, helping, and volunteering: Pathways to well-being in late life. J. Aging Health 2013, 25, 159–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennett, M.R.; Einolf, C.J. Religion, altruism, and helping strangers: A multilevel analysis of 126 countries. J. Sci. Study Relig. 2017, 56, 323–341. [Google Scholar] [CrossRef]
- Ruiter, S.; de Graaf, N.D. National context, religiosity, and volunteering: Results from 53 countries. Am. Sociol. Rev. 2006, 71, 191–210. [Google Scholar] [CrossRef] [Green Version]
- Barasch, A.; Levine, E.E.; Berman, J.Z.; Small, D.A. Selfish or selfless? On the signal value of emotion in altruistic behavior. J. Personal. Soc. Psychol. 2014, 107, 393. [Google Scholar] [CrossRef] [Green Version]
- Einolf, C.J. The link between religion and helping others: The role of values, ideas, and language. Sociol. Relig. 2011, 72, 435–455. [Google Scholar] [CrossRef] [Green Version]
- Stavrova, O.; Siegers, P. Religious prosociality and morality across cultures: How social enforcement of religion shapes the effects of personal religiosity on prosocial and moral attitudes and behaviors. Personal. Soc. Psychol. Bull. 2014, 40, 315–333. [Google Scholar] [CrossRef]
- Zabielskis, P. Too big to be bad? Implications for theory and review of research on crimes, vices, and misdeeds in the casino culture of Macau. Crime Law Soc. Change 2015, 64, 127–152. [Google Scholar]
- Lo, S. Casino capitalism and its legitimacy impact on the politico-administrative state in Macau. J. Curr. Chin. Aff. 2009, 38, 19–47. [Google Scholar] [CrossRef] [Green Version]
- van der Noll, J. Prejudice and religion. In Oxford Research Encyclopedia of Politics; Oxford University Press: Oxford, UK, 2019. [Google Scholar]
- Hunsberger, B.; Jackson, L.M. Religion, meaning, and prejudice. J. Soc. Issues 2005, 61, 807–826. [Google Scholar] [CrossRef]
- Van Assche, J.; Bahamondes, J.; Sibley, C. Religion and prejudice across cultures: A test of the threat-constraint model. Soc. Psychol. Personal. Sci. 2021, 12, 287–295. [Google Scholar] [CrossRef]
- Burch-Brown, J.; Baker, W. Religion and reducing prejudice. Group Processes Intergroup Relat. 2016, 19, 784–807. [Google Scholar] [CrossRef] [Green Version]
- Xia, W.; Guo, X.; Luo, J.; Ye, H.; Chen, Y.; Chen, S.; Xia, W. Religious identity, between-group effects and prosocial behavior: Evidence from a field experiment in China. J. Behav. Exp. Econ. 2021, 91, 101665. [Google Scholar] [CrossRef]
- Albertsen, E.J.; O’connor, L.E.; Berry, J.W. Religion and interpersonal guilt: Variations across ethnicity and spirituality. Ment. Health Relig. Cult. 2006, 9, 67–84. [Google Scholar] [CrossRef]
- Allport, G.W.; Ross, J.M. Personal religious orientation and prejudice. J. Personal. Soc. Psychol. 1967, 5, 432. [Google Scholar] [CrossRef]
- Jackson, L.M.; Hunsberger, B. An intergroup perspective on religion and prejudice. J. Sci. Study Relig. 1999, 38, 509–523. [Google Scholar] [CrossRef]
- Agyekumhene, E.; Amega, D.; Appau, S.; Awaworyi Churchill, S.; Ocloo, J. Ethnic diversity, prejudice and wellbeing among older Chinese. In Measuring, Understanding and Improving Wellbeing Among Older People; Springer: Berlin/Heidelberg, Germany, 2020; pp. 161–185. [Google Scholar]
- Page-Gould, E. Warning: Racism Is Bad for Your Health. Greater Good. Available online: https://greatergood.berkeley.edu/article/item/why_racism_is_bad_for_your_health (accessed on 2 February 2022).
- Lee, Y.; Muennig, P.; Kawachi, I.; Hatzenbuehler, M.L. Effects of racial prejudice on the health of communities: A multilevel survival analysis. Am. J. Public Health 2015, 105, 2349–2355. [Google Scholar] [CrossRef]
- Berry Mendes, W.; Gray, H.M.; Mendoza-Denton, R.; Major, B.; Epel, E.S. Why egalitarianism might be good for your health: Physiological thriving during stressful intergroup encounters. Psychol. Sci. 2007, 18, 991–998. [Google Scholar] [CrossRef] [Green Version]
- Blascovich, J.; Mendes, W.B.; Hunter, S.B.; Lickel, B.; Kowai-Bell, N. Perceiver threat in social interactions with stigmatized others. J. Personal. Soc. Psychol. 2001, 80, 253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page-Gould, E.; Mendoza-Denton, R.; Tropp, L.R. With a little help from my cross-group friend: Reducing anxiety in intergroup contexts through cross-group friendship. J. Personal. Soc. Psychol. 2008, 95, 1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, A. Life Satisfaction, Concept of. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer Netherlands: Dordrecht, The Netherlands, 2014; pp. 3599–3601. [Google Scholar]
- Siahpush, M.; Spittal, M.; Singh, G.K. Happiness and life satisfaction prospectively predict self-rated health, physical health, and the presence of limiting, long-term health conditions. Am. J. Health Promot. 2008, 23, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.; Mota, J.; Gaspar, T.; de Matos, M.G. Associations between self-reported fitness and self-rated health, life-satisfaction and health-related quality of life among adolescents. J. Exerc. Sci. Fit. 2017, 15, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Prasoon, R.; Chaturvedi, K. Life satisfaction: A literature review. Res. Int. J. Manag. Humanit. Soc. Sci. 2016, 1, 24–31. [Google Scholar]
- Kim, E.S.; Delaney, S.W.; Tay, L.; Chen, Y.; Diener, E.; Vanderweele, T.J. Life satisfaction and subsequent physical, behavioral, and psychosocial health in older adults. Milbank Q. 2021, 99, 209–239. [Google Scholar] [CrossRef]
- Kushlev, K.; Heintzelman, S.J.; Lutes, L.D.; Wirtz, D.; Kanippayoor, J.M.; Leitner, D.; Diener, E. Does happiness improve health? Evidence from a randomized controlled trial. Psychol. Sci. 2020, 31, 807–821. [Google Scholar]
- Aydogdu, R.; Yildiz, M.; Orak, U. Religion and wellbeing: Devotion, happiness and life satisfaction in Turkey. Ment. Health Relig. Cult. 2021, 24, 961–975. [Google Scholar] [CrossRef]
- Fastame, M.C.; Ruiu, M.; Mulas, I. Mental health and religiosity in the sardinian blue zone: Life satisfaction and optimism for aging well. J. Relig. Health 2021, 60, 2450–2462. [Google Scholar] [CrossRef]
- Chen, Y.; VanderWeele, T.J. Associations of religious upbringing with subsequent health and well-being from adolescence to young adulthood: An outcome-wide analysis. Am. J. Epidemiol. 2018, 187, 2355–2364. [Google Scholar] [CrossRef] [Green Version]
- Arafat, R.; Ratna, S.; Majid, A. Spiritual coping in people living with stroke. Int. J. Caring Sci. 2018, 11, 658. [Google Scholar]
- Ngamaba, K.H.; Soni, D. Are happiness and life satisfaction different across religious groups? Exploring determinants of happiness and life satisfaction. J. Relig. Health 2018, 57, 2118–2139. [Google Scholar] [PubMed]
- Collins, A.L.; Glei, D.A.; Goldman, N. The role of life satisfaction and depressive symptoms in all-cause mortality. Psychol. Aging 2009, 24, 696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, T.W.; Marsden, P.; Hout, M.; Kim, J. General Social Surveys, 1972–2014: Cumulative Codebook; National Opinion Research Center: Chicago, IL, USA, 2012. [Google Scholar]
- European Social Survey. ESS Round 8 Source Questionnaire; ESS ERIC Headquarters c/o City University London: London, UK, 2018. [Google Scholar]
- Baier, C.J.; Wright, B.R. “If you love me, keep my commandments”: A meta-analysis of the effect of religion on crime. J. Res. Crime Delinq. 2001, 38, 3–21. [Google Scholar] [CrossRef]
- Evans, T.D.; Cullen, F.T.; Dunaway, R.G.; Burton, V.S., Jr. Religion and crime reexamined: The impact of religion, secular controls, and social ecology on adult criminality. Criminology 1995, 33, 195–224. [Google Scholar] [CrossRef]
- Tittle, C.R.; Welch, M.R. Religiosity and deviance: Toward a contingency theory of constraining effects. Soc. Forces 1983, 61, 653–682. [Google Scholar] [CrossRef]
- Saroglou, V. Believing, bonding, behaving, and belonging: The big four religious dimensions and cultural variation. J. Cross Cult. Psychol. 2011, 42, 1320–1340. [Google Scholar] [CrossRef]
- Durkheim, E.; Swain, J.W. The Elementary Forms of the Religious Life; Courier Corporation: Chelmsford, MA, USA, 2008. [Google Scholar]
- Gorsuch, R.L.; McFarland, S.G. Single vs. multiple-item scales for measuring religious values. J. Sci. Study Relig. 1972, 11, 53–64. [Google Scholar] [CrossRef]
- Voas, D. Surveys of behaviour, beliefs and affiliation: Micro-quantitative. In The SAGE Handbook of the Sociology of Religion; SAGE Publications Ltd.: London, UK, 2007; pp. 144–166. [Google Scholar]
- Xi, J.; Lee, M.; LeSuer, W.; Barr, P.; Newton, K.; Poloma, M. Altruism and existential well-being. Appl. Res. Qual. Life 2017, 12, 67–88. [Google Scholar] [CrossRef]
- Allport, G.W.; Clark, K.; Pettigrew, T. The Nature of Prejudice. 1954. Available online: http://althaschool.org/_cache/files/7/1/71f96bdb-d4c3-4514-bae2-9bf809ba9edc/97F5FE75CF9A120E7DC108EB1B0FF5EC.holocaust-the-nature-of-prejudice.doc (accessed on 3 February 2022).
- Bogardus, E.S. A social distance scale. Sociol. Soc. Res. 1933, 17, 265–271. [Google Scholar]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Personal. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Ferris, J.A.; Wynne, H.J. The Canadian Problem Gambling Index; Canadian Centre on Substance Abuse Ottawa: Ottawa, ON, Canada, 2001. [Google Scholar]
- Casinos Worldwide—Statistics & Facts. Available online: https://www.statista.com/topics/1053/casinos/#topicHeader__wrapper (accessed on 10 February 2022).
- Jones, J.M. How Religious are Americans? Available online: https://news.gallup.com/poll/358364/religious-americans.aspx (accessed on 30 April 2022).
- Pew Research Center. The Age Gap in Religion Around the World. Available online: https://www.pewresearch.org/religion/2018/06/13/the-age-gap-in-religion-around-the-world/ (accessed on 30 April 2022).
- Charles, K. When Religion Becomes Evil: Five Warning Signs; Harper Collins, SFO: San Francisco, CA, USA, 2008. [Google Scholar]
- Morone, J.A. Hellfire Nation; Yale University Press: London, UK, 2008. [Google Scholar]
- La Cour, P.; Avlund, K.; Schultz-Larsen, K. Religion and survival in a secular region. A twenty year follow-up of 734 Danish adults born in 1914. Soc. Sci. Med. 2006, 62, 157–164. [Google Scholar] [CrossRef] [PubMed]
- La Cour, P. Existential and religious issues when admitted to hospital in a secular society: Patterns of change. Ment. Health Relig. Cult. 2008, 11, 769–782. [Google Scholar] [CrossRef]
- Hvidtjørn, D.; Hjelmborg, J.; Skytthe, A.; Christensen, K.; Hvidt, N.C. Religiousness and religious coping in a secular society: The gender perspective. J. Relig. Health 2014, 53, 1329–1341. [Google Scholar] [CrossRef] [PubMed]
- Svensson, N.H.; Hvidt, N.C.; Nissen, S.P.; Storsveen, M.M.; Hvidt, E.A.; Søndergaard, J.; Thilsing, T. Religiosity and Health-Related Risk Behaviours in a Secular Culture—Is there a Correlation? J. Relig. Health 2020, 59, 2381–2396. [Google Scholar] [CrossRef] [Green Version]
- Hvidt, N.C.; Assing Hvidt, E. Religiousness, spirituality and health in secular society: Need for spiritual care in health care? In Spirituality, Religiousness and Health; Springer: Berlin/Heidelberg, Germany, 2019; pp. 133–152. [Google Scholar]
- Nickerson, R.S. Confirmation bias: A ubiquitous phenomenon in many guises. Rev. Gen. Psychol. 1998, 2, 175–220. [Google Scholar] [CrossRef]
| Variables | ||||
|---|---|---|---|---|
| Demographic characteristic | % | S.D. | Min | Max |
| Female | 52.30% | 0.50 | 0 | 1 |
| Birthplace (Macau) | 52.46% | 0.50 | 0 | 1 |
| Demographic characteristic | Mean | S.D. | Min | Max |
| Age (years) | 43.78 | 17.11 | 16 | 96 |
| Education level | 2.93 | 1.69 | 0 | 7 |
| Problem gambling | 0.06 | 0.34 | 0 | 3 |
| Religiosity | ||||
| Religious activity attendance | 1.06 | 2.13 | 0 | 7 |
| Religious salience | 2.15 | 1.27 | 1 | 5 |
| Belief in God | 3.09 | 2.05 | 1 | 6 |
| Altruism | ||||
| Social contribution | 4.55 | 1.55 | 1 | 7 |
| Helping others | 4.87 | 1.45 | 1 | 7 |
| Caring for nature | 4.82 | 1.49 | 1 | 7 |
| Prejudice | 1.77 | 1.81 | 0 | 10 |
| Life satisfaction | ||||
| Life is close to ideal | 5.29 | 1.13 | 1 | 7 |
| Conditions are excellent | 5.03 | 1.26 | 1 | 7 |
| Satisfied with life | 5.04 | 1.25 | 1 | 7 |
| Have important things | 4.95 | 1.29 | 1 | 7 |
| Would change almost nothing | 4.68 | 1.51 | 1 | 7 |
| Health | ||||
| Health condition compared to peer(s) | 3.28 | 0.80 | 1 | 5 |
| Health condition compared to last year | 3.07 | 0.79 | 1 | 5 |
| General health | 2.69 | 0.96 | 1 | 5 |
| Religious Affiliation | N | % | Cumulative% |
|---|---|---|---|
| No religion | 2228 | 68.38 | 68.38 |
| Buddhism | 506 | 15.53 | 83.91 |
| Catholicism | 212 | 6.51 | 90.42 |
| Protestantism | 154 | 4.73 | 95.15 |
| Other | 126 | 3.87 | 99.02 |
| Daoism | 22 | 0.68 | 99.70 |
| Mazuism | 5 | 0.15 | 99.85 |
| Islam | 5 | 0.15 | 100.00 |
| Std. Coef. | S.E | |
|---|---|---|
| Religion on life satisfaction | ||
| Direct effect | ||
| Religion →satisfaction | 0.038 | 0.013 |
| Indirect effect | ||
| Religion → altruism → satisfaction | 0.031 *** | 0.007 |
| Religion → prejudice → satisfaction | 0.014 *** | 0.004 |
| Total effect | 0.083 *** | 0.014 |
| Religion on health | ||
| Direct effect | ||
| Religion → health | 0.181 *** | 0.012 |
| Indirect effect | ||
| Religion → altruism → health | 0.012 ** | 0.004 |
| Religion → prejudice → health | 0.018 *** | 0.005 |
| Religion → satisfaction → health | 0.006 | 0.004 |
| Religion → altruism → satisfaction → health | 0.005 ** | 0.001 |
| Religion → prejudice → satisfaction → health | 0.002 ** | 0.001 |
| Total effect | 0.225 *** | 0.012 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.; Lu, J.; Guan, C.; Zhang, S.; Li, S.D. In the Shadow of the Casinos: The Relationship between Religion and Health in Macau. Int. J. Environ. Res. Public Health 2022, 19, 5605. https://doi.org/10.3390/ijerph19095605
Chen Y, Lu J, Guan C, Zhang S, Li SD. In the Shadow of the Casinos: The Relationship between Religion and Health in Macau. International Journal of Environmental Research and Public Health. 2022; 19(9):5605. https://doi.org/10.3390/ijerph19095605
Chicago/Turabian StyleChen, Yiyi, Jiaqi Lu, Canghai Guan, Shiyang Zhang, and Spencer De Li. 2022. "In the Shadow of the Casinos: The Relationship between Religion and Health in Macau" International Journal of Environmental Research and Public Health 19, no. 9: 5605. https://doi.org/10.3390/ijerph19095605
APA StyleChen, Y., Lu, J., Guan, C., Zhang, S., & Li, S. D. (2022). In the Shadow of the Casinos: The Relationship between Religion and Health in Macau. International Journal of Environmental Research and Public Health, 19(9), 5605. https://doi.org/10.3390/ijerph19095605