
Inspiratory Muscle Training in Patients with Chronic Obstructive Pulmonary Disease (COPD) as Part of a Respiratory Rehabilitation Program Implementation of Mechanical Devices: A Systematic Review

 ,
, 

Abstract
1. Introduction and Objectives
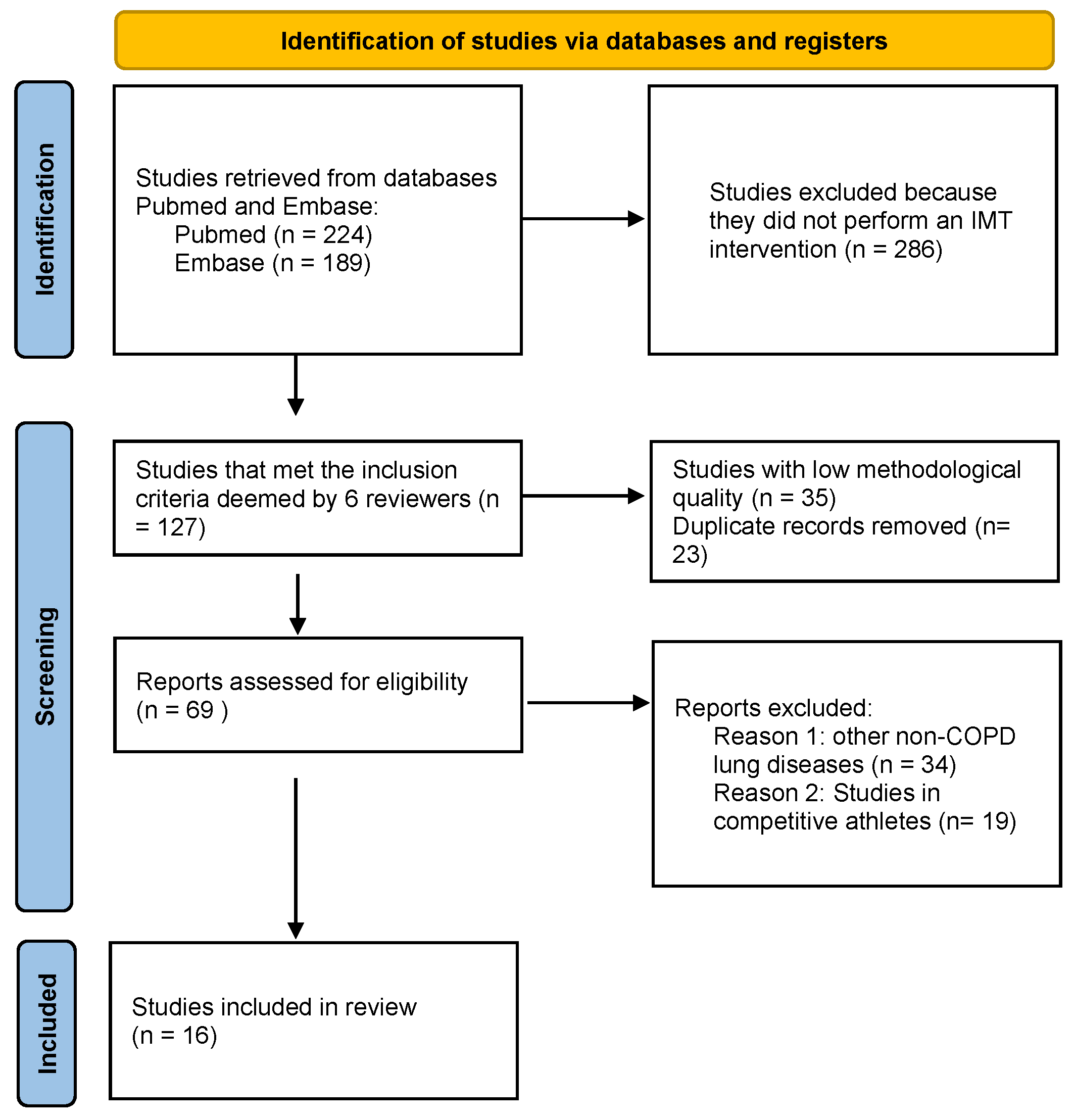
2. Material and Methods
3. Results
3.1. Profile of COPD Patients Who Are Candidates for IMT What Is a RR Program with IMT?
3.2. What Is a Respiratory Rehabilitation Program with Inspiratory Muscle Training?
- Threshold device: training with this type of device is obtained with a hand-held device that allows airflow during inspiration after reaching an inspiratory pressure. The effort required by the inspiratory muscles can be adjusted by the tension of a spring; this tension determines the opening of the valve;
- Resistive loading device: this is one of the most commonly used categories. In this category we have different devices. The PFLEX resistive Trainer device (Respironics HealthScan Inc., Cedar Grove, NJ, USA), consists of a mouthpiece and a circular dial. Turning the dial varies the size of the opening through which the patient breathes. The smaller the opening, the greater the resistance to inspiration. It has 6 diameter sizes. The objective of this exercise is to increase the load on the inspiratory muscles progressively. Many studies have used this device for IMT [25,29]. The PowerBreathe® device also stands out for its widespread use [30]. The Feelbreathe® device also behaves like a resistive load device, but in this case it is nasal and not buccal. It is a nasal ventilatory flow restriction device composed by a strip of hypoallergenic material that is placed and adhered under the nostrils, provoking resistance to flow. Depending on the size and porosity of the device material, the inspiratory process is more or less difficult. This device has the possibility of using it not only in a static situation but also dynamically during exercise [31];
- Voluntary isocapnic hyperpnea device: consisting of a device that increases the ventilation level of the subject to a predetermined level. The increase in ventilation causes an increase in respiratory rate, which can reach 50–60 rpm. This type of respiratory muscle training requires the patient to perform prolonged periods of hyperpnea, lasting up to 15 min and with a frequency of twice a day, 3 times a week, for 4–5 weeks [32]. To avoid hypocapnia, exercise should be performed on an isocapnic circuit, which maintains stable CO2 levels. One device using this method is the SpiroTiger® (Ideag Lab, Ziirich, Switzerland).
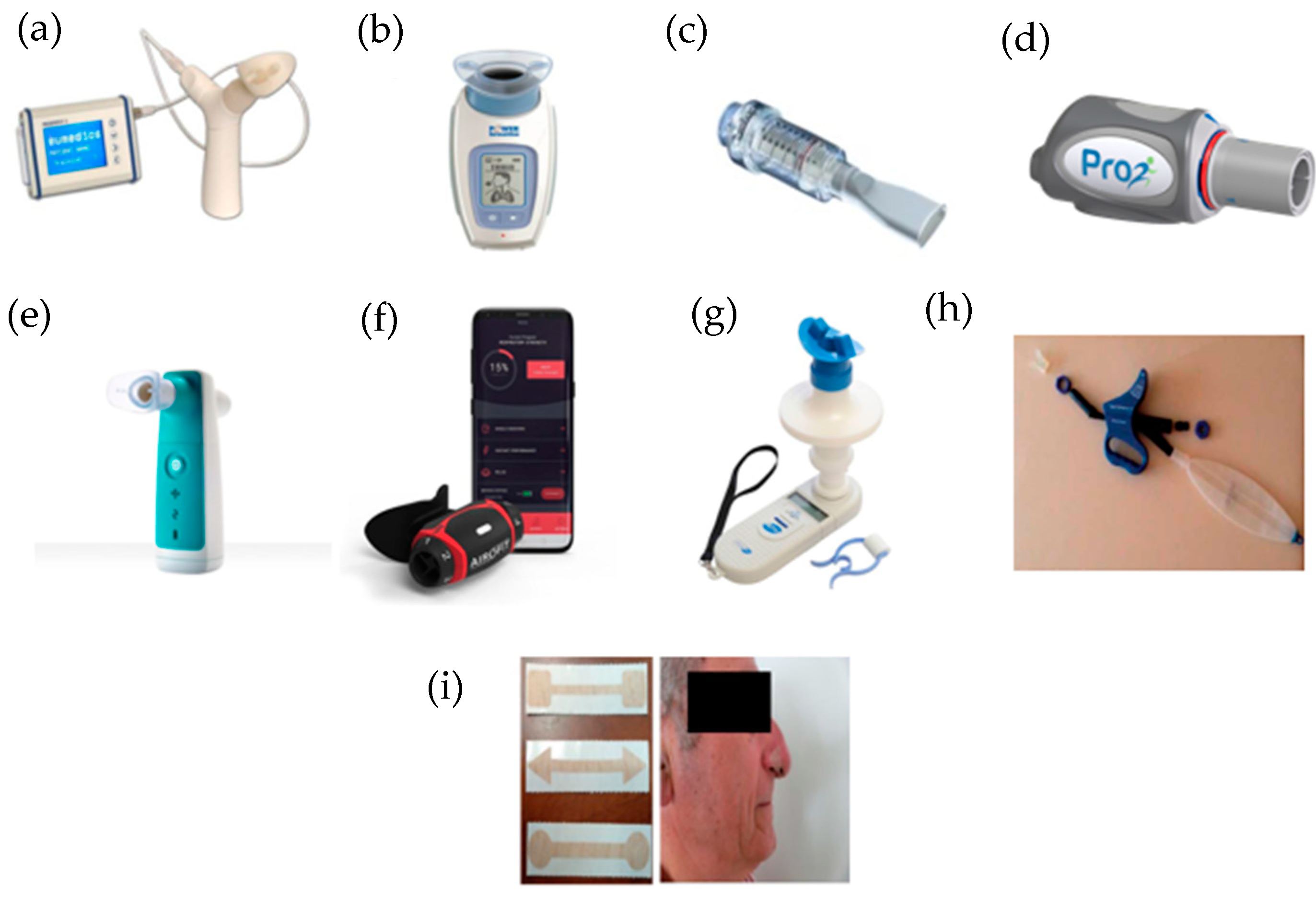
4. Inspiratory Muscle Training Programs Based on the Use of Mechanical Devices
4.1. Respifit STM
4.2. PowerBreathe®
4.3. Threshold IMT®
4.4. PrO2Fit TM®
4.5. Aerosure Medic®
4.6. AeroFit IMT®
4.7. MicroRPM
4.8. SpiroTiger®
4.9. FeelBreathe®
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| COPD | Chronic Obstructive Pulmonary Disease |
| RM | Respiratory muscles |
| RR | Respiratory rehabilitation |
| IMT | Inspiratory muscle training |
| T.lim | Endurance capacity of inspiratory muscles |
| 6MWT | 6 min walking test |
| SGRQ | St. George’s Respiratory Questionnaire |
| BBS | Berg Balance Scale |
| ABC | Activity specific Balance Confidence scale |
| VO2 | Oxygen uptake |
| VCO2 | Carbon dioxide output |
| FVC | Forced vital capacity |
| FEV1 | Forced expiratory volume in first second |
| MIP | Maximal inspiratory pressure |
| ID | Inspiratory duration |
| SMIP | Sustained maximal inspiratory pressure |
| mMRC | Modified Medical Research Council |
| PImax | Maximum inspiratory pressure |
| PEmax | Maximum expiratory pressure |
| ISWT | Incremental shuttle walk test |
| ESWT | Endurance shuttle walk test |
| PSQI | Pittsburgh Sleep Quality Index |
References
- Global Strategy for Diagnosis, Management, and Prevention of COPD. 2022. Available online: https://goldcopd.org/2022-gold-reports/ (accessed on 1 February 2022).
- Rabe, K.F.; Watz, H. Chronic obstructive pulmonary disease. Lancet 2017, 389, 1931–1940. [Google Scholar] [CrossRef]
- Agustí, A.; Sobradillo, P.; Celli, B. Addressing the complexity of chronic obstructive pulmonary disease: From phenotypes and biomarkers to scale-free networks, systems biology, and P4 medicine. Am. J. Respir. Crit. Care Med. 2011, 183, 1129–1137. [Google Scholar] [CrossRef] [PubMed]
- Agusti, A. The path to personalised medicine in copd. Thorax 2014, 69, 857–864. [Google Scholar] [CrossRef]
- Miravitlles, M.; Izquierdo, J.L.; Esquinas, C.; Pérez, M.; Calle, M.; López-Campos, J.L.; González-Moro, J.M.R.; Casanova, C.; Esteban, C.; de Lucas, P. The variability of respiratory symptoms and associated factors in COPD. Respir. Med. 2017, 129, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Anzueto, A.; Miravitlles, M. Pathophysiology of dyspnea in COPD. Postgrad. Med. 2017, 129, 366–374. [Google Scholar] [CrossRef] [PubMed]
- Cosío, B.G.; Hernández, C.; Chiner, E.; Gimeno-Santos, E.; Pleguezuelos, E.; Seijas, N.; Rigau, D.; López-Campos, J.L.; Soler-Cataluña, J.J.; Calle, M.; et al. Spanish COPD Guidelines (GesEPOC 2021): Non-pharmacological Treatment Update. Arch. Bronconeumol. 2022, 58, 69–81. [Google Scholar]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; Zu Wallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.-C.; et al. An official American thoracic society/European respiratory society statement: Key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef]
- Puhan, M.A.; Gimeno-Santos, E.; Scharplatz, M.; Troosters, T.; Walters, E.H.; Steurer, J. Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2016, 12, CD00530510. [Google Scholar] [CrossRef]
- Larson, J.L.; Covey, M.K.; Corbridge, S. Inspiratory muscle strength in chronic obstructive pulmonary disease. AACN Clin. Issues 2002, 13, 320–332. [Google Scholar] [CrossRef]
- Chen, H.I.; Dukes, R.; Martin, B.J. Inspiratory muscle training in patients with chronic obstructive pulmonary disease. Am. Rev. Respir. Dis. 1985, 131, 251–255. [Google Scholar]
- Petrovic, M.; Reiter, M.; Zipko, H.; Pohl, W.; Wanke, T. Effects of inspiratory muscle training on dynamic hyperinflation in patients with COPD. Int. J. COPD 2012, 7, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Gosselink, R.; De Vos, J.; Van Den Heuvel, S.P.; Segers, J.; Decramer, M.; Kwakkel, G. Impact of inspiratory muscle training in patients with COPD: What is the evidence? Eur. Respir. J. 2011, 37, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Geddes, E.L.; O’Brien, K.; Reid, W.D.; Brooks, D.; Crowe, J. Inspiratory muscle training in adults with chronic obstructive pulmonary disease: An update of a systematic review. Respir. Med. 2008, 102, 1715–1729. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The prisma 2020 statement: An updated guideline for reporting systematic reviews. Med. Flum. 2021, 57, 444–465. [Google Scholar] [CrossRef]
- Hanania, N.A.; O’donnell, D.E. Activity-related dyspnea in chronic obstructive pulmonary disease: Physical and psychological consequences, unmet needs, and future directions. Int. J. COPD 2019, 14, 1127–1138. [Google Scholar] [CrossRef]
- Marciniuk, D.D.; Goodridge, D.; Hernandez, P.; Rocker, G.; Balter, M.; Bailey, P.; Ford, G.; Bourbeau, J.; E O’Donnell, D.; Maltais, F.; et al. Managing dyspnea in patients with advanced chronic obstructive pulmonary disease: A Canadian Thoracic Society clinical practice guideline. Can. Respir. J. 2011, 18, 69–78. [Google Scholar] [CrossRef]
- Harms, C.A.; Babcock, M.A.; McClaran, S.R.; Pegelow, D.F.; Nickele, G.A.; Nelson, W.B.; Dempsey, J.A. Respiratory muscle work compromises leg blood flow during maximal exercise. J. Appl. Physiol. 1997, 82, 1573–1583. [Google Scholar] [CrossRef]
- Harms, C.A.; Wetter, T.J.; McClaran, S.R.; Pegelow, D.F.; Nickele, G.A.; Nelson, W.B.; Dempsey, J.A. Effects of respiratory muscle work on cardiac output and its distribution during maximal exercise. J. Appl. Physiol. 1998, 85, 609–618. [Google Scholar] [CrossRef]
- Aubier, M. Respiratory muscle fatigue. Intensive Care Med. 1989, 15 (Suppl. 1), 17–20. [Google Scholar] [CrossRef]
- McConnell, A.K.; Sharpe, G.R. The effect of inspiratory muscle training upon maximum lactate steady-state and blood lactate concentration. Eur. J. Appl. Physiol. 2005, 94, 277–284. [Google Scholar] [CrossRef]
- Charususin, N.; Gosselink, R.; Decramer, M.; McConnell, A.; Saey, D.; Maltais, F.; Derom, E.; Vermeersch, S.; van Helvoort, H.; Heijdra, Y.; et al. Inspiratory muscle training protocol for patients with chronic obstructive pulmonary disease (IMTCO study): A multicentre randomised controlled trial. BMJ Open 2013, 3, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Magadle, R.; McConnell, A.K.; Beckerman, M.; Weiner, P. Inspiratory muscle training in pulmonary rehabilitation program in COPD patients. Respir. Med. 2007, 101, 1500–1505. [Google Scholar] [CrossRef] [PubMed]
- Langer, D.; Ciavaglia, C.; Faisal, A.; Webb, K.A.; Neder, J.A.; Gosselink, R.; Dacha, S.; Topalovic, M.; Ivanova, A.; O’Donnell, D.E. Inspiratory muscle training reduces diaphragm activation and dyspnea during exercise in COPD. J. Appl. Physiol. 2018, 125, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Romer, L.M.; McConnell, A.K.; Jones, D.A. Effects of inspiratory muscle training on time-trial performance in trained cyclists. J. Sports Sci. 2002, 20, 547–562. [Google Scholar] [CrossRef]
- Brown, P.I.; Sharpe, G.R.; Johnson, M.A. Loading of trained inspiratory muscles speeds lactate recovery kinetics. Med. Sci. Sports Exerc. 2010, 42, 1103–1112. [Google Scholar] [CrossRef]
- de Lucas Ramos, P.; Rodríguez González-Moro, J.M.; García de Pedro, J.; Santacruz Siminiani, A.; Tatay Martí, E.; Cubillo Marcos, J.M. Entrenamiento de los músculos inspiratorios en la enfermedad pulmonar obstructiva crónica. Su impacto sobre las alteraciones funcionales y sobre la tolerancia al ejercicio. Arch. Bronconeumol. 1998, 34, 64–70. [Google Scholar] [CrossRef]
- González-Montesinos, J.L.; Vaz Pardal, C.; Fernández Santos, C.R.; Arnedillo Muñoz, A.; Costa Sepúlveda, J.L.; Gomez Espinosa de los Monteros, R. Efectos del entrenamiento de la musculatura respiratoria sobre el rendimiento. Revisión bibliográfica. Rev. Andal. Med. Deporte 2012, 3, 171–178. [Google Scholar] [CrossRef]
- Downey, A.E.; Chenoweth, L.M.; Townsend, D.K.; Ranum, J.D.; Ferguson, C.S.; Harms, C.A. Effects of inspiratory muscle training on exercise responses in normoxia and hypoxia. Respir. Physiol. Neurobiol. 2007, 156, 137–146. [Google Scholar] [CrossRef]
- Dickinson, J.; Whyte, G.; McConnell, A. Inspiratory muscle training: A simple cost-effective treatment for inspiratory stridor. Br. J. Sports Med. 2007, 41, 694–695. [Google Scholar] [CrossRef]
- Gonzalez-Montesinos, J.L.; Arnedillo, A.; Fernandez-Santos, J.R.; Vaz-Pardal, C.; García, P.A.; Castro-Piñero, J.; Ponce-González, J.G. A new nasal restriction device called feelbreathe® improves breathing patterns in chronic obstructive pulmonary disease patients during exercise. Int. J. Environ. Res. Public Health 2020, 17, 4876. [Google Scholar] [CrossRef]
- Boutellier, U.; Büchel, R.; Kundert, A.; Spengler, C. Applied Physiology in normal trained subjects. Eur. J. Appl. Physiol. Occup. Physiol. 1992, 65, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Beaumont, M.; Forget, P.; Couturaud, F.; Reychler, G. Effects of inspiratory muscle training in COPD patients: A systematic review and meta-analysis. Clin. Respir. J. 2018, 12, 2178–2188. [Google Scholar] [CrossRef] [PubMed]
- Camillo, C.A.; Osadnik, C.R.; van Remoortel, H.; Burtin, C.; Janssens, W.; Troosters, T. Effect of “add-on” interventions on exercise training in individuals with COPD: A systematic review. ERJ Open Res. 2016, 2, 00078–2015. [Google Scholar] [CrossRef]
- Bolton, C.E.; Bevan-Smith, E.F.; Blakey, J.D.; Crowe, P.; Elkin, S.L.; Garrod, R.; Greening, N.J.; Heslop, K.; Hull, J.H.; Man, W.D.-C.; et al. British Thoracic Society guideline on pulmonary rehabilitation in adults. Thorax 2013, 68 (Suppl. 2), ii1–ii30. [Google Scholar] [CrossRef] [PubMed]
- Güell Rous, M.R.; Díaz Lobato, S.; Rodríguez Trigo, G.; Morante Vélez, F.; San Miguel, M.; Cejudo, P.; Ortega Ruiz, F.; Muñoz, Á.; Galdiz Iturri, J.B.; Garcia, A.; et al. Rehabilitación respiratoria. Arch. Bronconeumol. 2014, 50, 332–344. [Google Scholar] [CrossRef]
- Sonne, L.J.; Davis, J.A. Increased exercise performance in patients with severe COPD following inspiratory resistive training. Chest 1982, 81, 436–439. [Google Scholar] [CrossRef]
- Andersen, J.B.; Falk, P. Clinical experience with inspiratory resistive breathing training. Disabil. Rehabil. 1984, 6, 183–185. [Google Scholar] [CrossRef]
- Belman, M.J.; Shadmehr, R. Targeted resistive ventilatory muscle training in chronic obstructive pulmonary disease. J. Appl. Physiol. 1988, 65, 2726–2735. [Google Scholar] [CrossRef]
- Dekhuijzen, P.N.R.; Beek, M.M.L.; Folgering, H.T.M.; van Herwaarden, C.L.A. Psychological changes during pulmonary rehabilitation and target-flow inspiratory muscle training in COPD patients with a ventilatory limitation during exercise. Int. J. Rehabil. Res. 1990, 13, 109–118. [Google Scholar] [CrossRef]
- Tounsi, B.; Acheche, A.; Lelard, T.; Tabka, Z.; Trabelsi, Y.; Ahmaidi, S. Effects of specific inspiratory muscle training combined with whole-body endurance training program on balance in COPD patients: Randomized controlled trial. PLoS ONE 2021, 16, e0257595. [Google Scholar] [CrossRef]
- Charususin, N.; Gosselink, R.; Decramer, M.; Demeyer, H.; McConnell, A.; Saey, D.; Maltais, F.; Derom, E.; Vermeersch, S.; Heijdra, Y.F.; et al. Randomised controlled trial of adjunctive inspiratory muscle training for patients with COPD. Thorax 2018, 73, 942–950. [Google Scholar] [CrossRef] [PubMed]
- Langer, D.; Charususin, N.; Jácome, C.; Hoffman, M.; McConnell, A.; Decramer, M.; Gosselink, R. Efficacy of a novel method for inspiratory muscle training in people with chronic obstructive pulmonary disease. Phys. Ther. 2015, 95, 1264–1273. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, F.V.; Gavin, J.P.; Wainwright, T.; McConnell, A. The effects of 8 weeks of inspiratory muscle training on the balance of healthy older adults: A randomized, double-blind, placebo-controlled study. Physiol. Rep. 2019, 7, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Nield, M.A. Inspiratory muscle training protocol using a pressure threshold device: Effect on dyspnea in chronic obstructive pulmonary disease. Arch. Phys. Med. Rehabil. 1999, 80, 100–102. [Google Scholar] [CrossRef]
- Beaumont, M.; Mialon, P.; Ber-Moy, C.; Lochon, C.; Péran, L.; Pichon, R.; Gut-Gobert, C.; Leroyer, C.; Morelot-Panzini, C.; Couturaud, F. Inspiratory muscle training during pulmonary rehabilitation in chronic obstructive pulmonary disease. Chron. Respir. Dis. 2015, 12, 305–312. [Google Scholar] [CrossRef]
- Wang, K.; Zeng, G.Q.; Li, R.; Luo, Y.W.; Wang, M.; Hu, Y.H.; Xu, W.-H.; Zhou, L.-Q.; Chen, R.-C.; Chen, X. Cycle ergometer and inspiratory muscle training offer modest benefit compared with cycle ergometer alone: A comprehensive assessment in stable COPD patients. Int. J. COPD 2017, 12, 2655–2668. [Google Scholar] [CrossRef]
- Formiga, M.F.; Roach, K.E.; Vital, I.; Urdaneta, G.; Balestrini, K.; Calderon-Candelario, R.A.; Campos, M.; Cahalin, L.P. Reliability and validity of the test of incremental respiratory endurance measures of inspiratory muscle performance in COPD. Int. J. COPD 2018, 13, 1569–1576. [Google Scholar] [CrossRef]
- McCreery, J.L.; Mackintosh, K.A.; Mills-Bennett, R.; McNarry, M.A. The effect of a high-intensity pro2fit inspiratory muscle training intervention on physiological and psychological health in adults with bronchiectasis: A mixed-methods study. Int. J. Environ. Res. Public Health 2021, 18, 3051. [Google Scholar]
- Formiga, M.F.; Dosbaba, F.; Hartman, M.; Batalik, L.; Plutinsky, M.; Brat, K.; Ludka, O.; Cahalin, L.P. Novel versus traditional inspiratory muscle training regimens as home-based, stand-alone therapies in copd: Protocol for a randomized controlled trial. Int. J. COPD 2020, 15, 2147–2155. [Google Scholar] [CrossRef]
- Daynes, E.; Greening, N.J.; Harvey-Dunstan, T.C.; Singh, S.J. High-frequency airway oscillating device for respiratory muscle training in subjects with copd. Respir. Care 2018, 63, 584. [Google Scholar] [CrossRef]
- Stavrou, V.T.; Tourlakopoulos, K.N.; Daniil, Z.; Gourgoulianis, K.I. Respiratory Muscle Strength: New Technology for Easy Assessment. Cureus 2021, 13, e14803. [Google Scholar] [CrossRef] [PubMed]
- Włodarczyk, O.M.; Barinow-Wojewódzki, A. The impact of resistance respiratory muscle training with a SpiroTiger® device on lung function, exercise performance, and health-related quality of life in respiratory diseases. Kardiochirurgia Torakochirurgia Pol. 2015, 12, 386–390. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, E.; Pomidori, L.; Bassal, F.; Contoli, M.; Cogo, A. Respiratory muscle training with normocapnic hyperpnea improves ventilatory pattern and thoracoabdominal coordination, and reduces oxygen desaturation during endurance exercise testing in COPD patients. Int. J. COPD 2015, 10, 1899–1906. [Google Scholar] [CrossRef] [PubMed]
- Arnedillo, A.; Gonzalez-Montesinos, J.L.; Fernandez-Santos, J.R.; Vaz-Pardal, C.; España-Domínguez, C.; Ponce-González, J.G.; Marin-Galindo, A.; Arnedillo, A. Effects of a rehabilitation programme with a nasal inspiratory restriction device on exercise capacity and quality of life in COPD. Int. J. Environ. Res. Public Health 2020, 17, 3669. [Google Scholar] [CrossRef]
- Gonzalez-Montesinos, J.L.; Fernandez-Santos, J.R.; Vaz-Pardal, C.; Ponce-Gonzalez, J.G.; Marin-Galindo, A.; Arnedillo, A. Effects of a rehabilitation programme using a nasal inspiratory restriction device in copd. Int. J. Environ. Res. Public Health 2021, 18, 4207. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author | Publication Date | Device | Type of Devices | Subject Study | Duration | Method | Results |
|---|---|---|---|---|---|---|---|
| Petrovic et al. | 2012 | Respifit | Threshold | 20 COPD | 8 weeks | Direct by cardiopulmonary and stress test | Enhances inspiratory muscle function, dyspnea, and quality of life. |
| Magadle et al. | 2007 | PowerBreathe® | Resistive load and | 34 COPD | 12 weeks | 6MWT, SGRQ | Enhances inspiratory muscle function and dyspnea perception. |
| Tounsi et al. | 2021 | PowerBreathe® | Resistive load and | 32 COPD | 8 weeks | BBS, ABC, 6MWT | Enhances inspiratory muscle function and functional balance according to BBS and ABC. |
| Charususin et al. | 2018 | PowerBreathe® | Resistive load and | 219 COPD | 5–8 weeks | 6MWT. | No differences in 6MWT. Gains in respiratory muscle function and also endurance exercise capacity. |
| Langer et al. | 2018 | PowerBreathe® | Resistive load and | 20 COPD | 8 weeks | PImax, T.lim | Improvments in Pi,max and T,lim. Telemonitorization. |
| Beaumont et al. | 2015 | Threshold IMT® | Threshold | 23 COPD | 3 weeks | Borg scale, 6MWT, PImax. Cycle ergometer | Subgroup of patients with FEV1 < 50% pred., dyspnea was significantly improved. |
| McCreery et al. | 2021 | PrO2 Fit | Resistive load | 10 BQ | 8 weeks | VO2, VCO2 and pulmonary function (FVC, FEV1) | Increased inspiratory muscle strength and endurance. Telemonitorization. |
| Formiga et al. | 2018 | PrO2 Fit | Resistive load | 81 COPD | 1 day | FEV1, FVC, 6MWT, MIP, ID, SMIP. | Increased inspiratory muscle strength and endurance |
| Formiga et al. | 2020 | PrO2 Fit | Resistive load | On going | 8 weeks | mMRC, FEV1, FVC, 6MWT. | Test of incremental respiratory endurance training method has the potential to provide additional clinical benefits in COPD. |
| Daynes et al. | 2018 | Aerosure Medic® | Resistive load | 23 COPD | 8 weeks | mMRC, PImax, PEmax. ISWT, ESWT | Improvmente PI max, PE max, and reducing dyspnoea. |
| Stavrou et al. | 2021 | AeroFit IMT® MicroRPM | Resistive load | 21 athletes | 1 day | PSQI, pulmonary function test, ergospirometry | Compare both not differences between devices. AirOFitPRO™ is easier to operate as a device and provides more information. |
| Bernardi et al. | 2015 | SpiroTiger® | Resistive load | 20 COPD | 4 weeks | Spirometry 6MWT, VO2max, SGRQ | Increased inspiratory muscle and quality of life. |
| Włodarczyk et al. | 2015 | SpiroTiger® | Voluntary isocapnic hyperpnea | - | - | 6MWT | Improve quality of life and distance in 6MWT |
| Gonzalez-Montesinos et al. | 2020 | FeelBreathe® | Nasal restriction | 18 COPD | 8 weeks | PI max y VO2max | Positive effects in dynamic hyperinflation, breathing pattern, and breathing efficiency, with higher expiratory and inspiratory time. |
| Arnedillo et al. | 2020 | FeelBreathe® | Nasal restriction | 16 COPD | 8 weeks | Inspiratory muscle strength (PImax), dyspnea (mMRC), quality of life (CAT) and exercise capacity (6MWT) | Improvements in quality of life, dyspnea, exercise capacity, and inspiratory muscle strength |
| Gonzalez-Montesinos et al. | 2021 | FeelBreathe® | Nasal restriction | 20 COPD | 8 weeks | VO2, VCO2, respiratory rate | FB added to a pulmonary rehabilitation program in COPD patients could improve tolerance in the incremental exercise test and energy efficiency |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vázquez-Gandullo, E.; Hidalgo-Molina, A.; Montoro-Ballesteros, F.; Morales-González, M.; Muñoz-Ramírez, I.; Arnedillo-Muñoz, A. Inspiratory Muscle Training in Patients with Chronic Obstructive Pulmonary Disease (COPD) as Part of a Respiratory Rehabilitation Program Implementation of Mechanical Devices: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 5564. https://doi.org/10.3390/ijerph19095564
Vázquez-Gandullo E, Hidalgo-Molina A, Montoro-Ballesteros F, Morales-González M, Muñoz-Ramírez I, Arnedillo-Muñoz A. Inspiratory Muscle Training in Patients with Chronic Obstructive Pulmonary Disease (COPD) as Part of a Respiratory Rehabilitation Program Implementation of Mechanical Devices: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(9):5564. https://doi.org/10.3390/ijerph19095564
Chicago/Turabian StyleVázquez-Gandullo, Eva, Antonio Hidalgo-Molina, Francisca Montoro-Ballesteros, María Morales-González, Isabel Muñoz-Ramírez, and Aurelio Arnedillo-Muñoz. 2022. "Inspiratory Muscle Training in Patients with Chronic Obstructive Pulmonary Disease (COPD) as Part of a Respiratory Rehabilitation Program Implementation of Mechanical Devices: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 9: 5564. https://doi.org/10.3390/ijerph19095564
APA StyleVázquez-Gandullo, E., Hidalgo-Molina, A., Montoro-Ballesteros, F., Morales-González, M., Muñoz-Ramírez, I., & Arnedillo-Muñoz, A. (2022). Inspiratory Muscle Training in Patients with Chronic Obstructive Pulmonary Disease (COPD) as Part of a Respiratory Rehabilitation Program Implementation of Mechanical Devices: A Systematic Review. International Journal of Environmental Research and Public Health, 19(9), 5564. https://doi.org/10.3390/ijerph19095564