
Development and Initial Validation of the Oral Health Activities Questionnaire


 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Development of the Oral Health Activities Questionnaire (OHAQ)
2.3. Self-Reported Oral Health Status Questionnaire
2.4. Application of the OHAQ on a Sample of University Students
2.5. Data Analysis
3. Results
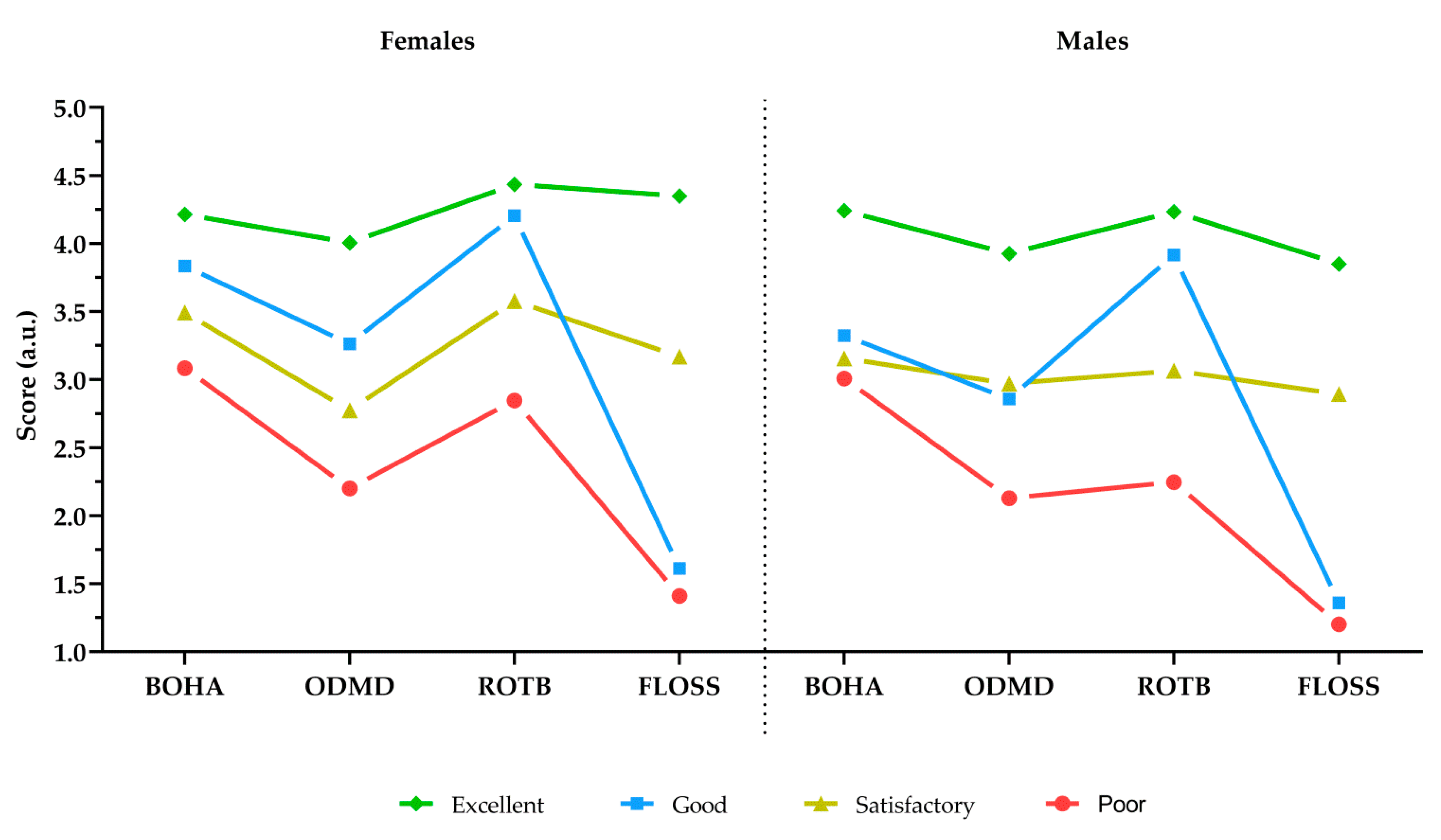
- The first type, which included 19.6% of female students, was called the excellent OH type because their scores on all OHAQ scales were very high;
- The second type, which included 27.3% of female students, was identified as the good OH type without flossing because their scores on the three OHAQ scales were approximately high and the flossing score was extremely low;
- The third type, which included 27.3% of female students, was called the satisfactory OH type because their scores on all four OHAQ scales were approximately moderate;
- The fourth type, which included 25.7% of female students, was called the poor OH type because their assessments of the three OHAQ scales were low and the assessment of flossing was extremely low.
- The first type, which included only 9.1% of male students, was called the excellent OH type because their scores on all OHAQ scales were very high;
- The second type, which included 32.4% of male students, was called the good OH type without flossing because their ratings on the three OHAQ scales were approximately satisfactory and the flossing score was extremely low;
- The third type, which included 30.1% of male students, was called the satisfactory OH type because their assessments on all four OHAQ scales were moderate;
- The fourth type, which included 28.3% of male students, was referred to as the poor OH type because their scores on three OHAQ scales were low and their assessment of flossing was extremely low.
4. Discussion
4.1. Dimensions of Oral Health Activities
4.2. Frequencies and Gender Differences of Oral Health Activities
4.3. Types of Oral Health Activities
4.4. Self-Reported Oral Health Status and OHAQ Measures
4.5. Usage of the OHAQ Index Criteria
4.6. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marchetti, E.; Monaco, A.; Procaccini, L.; Mummolo, S.; Gatto, R.; Tetè, S.; Baldini, A.; Tecco, S.; Marzo, G. Periodontal disease: The influence of metabolic syndrome. Nutr. Metab. 2012, 9, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baldini, A.; Nota, A.; Cioffi, C.; Ballanti, F.; Cozza, P. Infrared thermographic analysis of craniofacial muscles in military pilots affected by bruxism. Aerosp. Med. Hum. Perform. 2015, 86, 374–378. [Google Scholar] [CrossRef] [PubMed]
- Baldini, A.; Nota, A.; Cravino, G.; Cioffi, C.; Rinaldi, A.; Cozza, P. Influence of vision and dental occlusion on body posture in pilots. Aviat. Space Environ. Med. 2013, 84, 823–827. [Google Scholar] [CrossRef] [PubMed]
- Leao, A.; Sheiham, A. Relation between clinical dental status and subjective impacts on daily living. J. Dent. Res. 1995, 74, 1408–1413. [Google Scholar] [CrossRef]
- Pellizzer, C.; Pejda, S.; Špalj, S.; Plančak, D. Unrealistic Optimism and Demographic Influence on Oral Health-Related Behaviour and Perception in Adolescents in Croatia. Acta Stomatol. Croat. Int. J. Oral Sci. Dent. Med. 2007, 41, 215. [Google Scholar]
- Schou, L.; Blinkhorn, A.S. Oral Health Promotion; Oxford University Press: Oxford, UK, 1993. [Google Scholar]
- Choo, A.; Delac, D.M.; Messer, L.B. Oral hygiene measures and promotion: Review and considerations. Aust. Dent. J. 2001, 46, 166–173. [Google Scholar] [CrossRef]
- Badovinac, A.; Božić, D.; Vučinac, I.; Vešligaj, J.; Vražić, D.; Plancak, D. Oral health attitudes and behavior of dental students at the University of Zagreb, Croatia. J. Dent. Educ. 2013, 77, 1171–1178. [Google Scholar] [CrossRef]
- Marchetti, E.; Mummolo, S.; Di Mattia, J.; Casalena, F.; Di Martino, S.; Mattei, A.; Marzo, G. Efficacy of essential oil mouthwash with and without alcohol: A 3-day plaque accumulation model. Trials 2011, 12, 262. [Google Scholar] [CrossRef] [Green Version]
- Marchetti, E.; Tecco, S.; Caterini, E.; Casalena, F.; Quinzi, V.; Mattei, A.; Marzo, G. Alcohol-free essential oils containing mouthrinse efficacy on three-day supragingival plaque regrowth: A randomized crossover clinical trial. Trials 2017, 18, 154. [Google Scholar] [CrossRef] [Green Version]
- Bader, J.D.; Shugars, D.A.; Bonito, A.J. A systematic review of selected caries prevention and management methods. Community Dent. Oral Epidemiol. 2001, 29, 399–411. [Google Scholar] [CrossRef]
- Ostberg, A.L.; Halling, A.; Lindblad, U. A gender perspective of self-perceived oral health in adolescents: Associations with attitudes and behaviours. Community Dent. Health 2001, 18, 110–116. [Google Scholar] [PubMed]
- Kawamura, M.; Honkala, E.; Widström, E.; Komabayashi, T. Cross-cultural differences of self-reported oral health behaviour in Japanese and Finnish dental students. Int. Dent. J. 2000, 50, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, M.; Spadafora, A.; Kim, K.J.; Komabayashi, T. Comparison of United States and Korean dental hygiene students using the Hiroshima university-dental behavioural inventory(HU-DBI). Int. Dent. J. 2002, 52, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, M.; Yip, H.K.; Hu, D.Y.; Komabayashi, T. A cross-cultural comparison of dental health attitudes and behaviour among freshman dental students in Japan, Hong Kong and West China. Int. Dent. J. 2001, 51, 159–163. [Google Scholar] [CrossRef]
- Komabayashi, T.; Kwan, S.Y.; Hu, D.Y.; Kajiwara, K.; Sasahara, H.; Kawamura, M. A comparative study of oral health attitudes and behaviour using the Hiroshima University—Dental Behavioural Inventory (HU-DBI) between dental students in Britain and China. J. Oral Sci. 2005, 47, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Riad, A.; Põld, A.; Olak, J.; Howaldt, H.P.; Klugar, M.; Krsek, M.; Attia, S. Estonian Dental Students’ Oral Health-Related Knowledge, Attitudes and Behaviours (KAB): National Survey-Based Study. Int. J. Environ. Res. Public Health 2022, 19, 1908. [Google Scholar] [CrossRef]
- Riad, A.; Al-Khanati, N.M.; Issa, J.; Zenati, M.; Abdesslem, N.B.; Attia, S.; Krsek, M. Oral Health-Related Knowledge, Attitudes and Behaviours of Arab Dental Students: Multi-National Cross-Sectional Study and Literature Analysis 2000–2020. Int. J. Environ. Res. Public Health 2022, 19, 1658. [Google Scholar] [CrossRef]
- Kawamura, M.; Iwamoto, Y.; Wright, F.A. A comparison of self-reported dental health attitudes and behavior between selected Japanese and Australian students. J. Dent. Educ. 1997, 61, 354–360. [Google Scholar] [CrossRef]
- Polychronopoulou, A.; Kawamura, M. Oral self-care behaviours: Comparing Greek and Japanese dental students. Eur. J. Dent. Educ. Off. J. Assoc. Dent. Educ. Eur. 2005, 9, 164–170. [Google Scholar] [CrossRef]
- Khan, S.Q. Dental caries in Arab League countries: A systematic review and meta-analysis. Int. Dent. J. 2014, 64, 173–180. [Google Scholar] [CrossRef]
- Kazeminia, M.; Abdi, A.; Shohaimi, S.; Jalali, R.; Vaisi-Raygani, A.; Salari, N.; Mohammadi, M. Dental caries in primary and permanent teeth in children’s worldwide, 1995 to 2019: A systematic review and meta-analysis. Head Face Med. 2020, 16, 22. [Google Scholar] [CrossRef] [PubMed]
- Hugoson, A.; Koch, G.; Göthberg, C.; Helkimo, A.N.; Lundin, S.A.; Norderyd, O.; Sjödin, B.; Sondell, K. Oral health of individuals aged 3–80 years in Jönköping, Sweden during 30 years (1973–2003). I. Review of findings on dental care habits and knowledge of oral health. Swed. Dent. J. 2005, 29, 125–138. [Google Scholar] [PubMed]
- Zukanović, A. Caries risk assessment models in caries prediction. Acta Med. Acad. 2013, 42, 198–208. [Google Scholar] [CrossRef] [Green Version]
- Mostarčić, K.I.; Šimat, S.; Matijević, J.; Krmek-Jukić, S.J.A.S.C. Comparison of Oral Hygiene Habits of the 4th Year Students of Different Faculties of University of Zagreb. Acta Stomatol. Croat. 2009, 43, 310–318. [Google Scholar]
- Jensen, O.; Gabre, P.; Sköld, U.M.; Birkhed, D. Is the use of fluoride toothpaste optimal? Knowledge, attitudes and behaviour concerning fluoride toothpaste and toothbrushing in different age groups in Sweden. Community Dent. Oral Epidemiol. 2012, 40, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Lopez, R.; Baelum, V. Factors associated with dental attendance among adolescents in Santiago, Chile. BMC Oral Health 2007, 7, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguilar-Díaz, F.C.; Ponce-Cruz, Y.R.; Mortellaro, C.; Giacomello, M.; Manfredi, B.; Khijmatgar, S.; Biagi, R.; Greco Lucchina, A.; Del Fabbro, M. Knowledge, practices and perceptions regarding oral health preventive measures among Mexican dental students: A cross-sectional survey study. J. Biol. Regul. Homeost. Agents 2021, 35, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Pınar Erdem, A.; Peker, K.; Kuru, S.; Sepet, E. Evaluation of Final-Year Turkish Dental Students’ Knowledge, Attitude, and Self-Perceived Competency towards Preventive Dentistry. BioMed Res. Int. 2019, 2019, 2346061. [Google Scholar] [CrossRef] [Green Version]
- Peker, I.; Alkurt, M.T. Oral Health Attitudes and Behavior among a Group of Turkish Dental Students. Eur. J. Dent. 2009, 3, 24–31. [Google Scholar] [CrossRef] [Green Version]
- Al-Ansari, J.; Honkala, E.; Honkala, S. Oral health knowledge and behavior among male health sciences college students in Kuwait. BMC Oral Health 2003, 3, 2. [Google Scholar] [CrossRef] [Green Version]
- Al-Hussaini, R.; Al-Kandari, M.; Hamadi, T.; Al-Mutawa, A.; Honkala, S.; Memon, A. Dental health knowledge, attitudes and behaviour among students at the Kuwait University Health Sciences Centre. Med. Princ. Pract. Int. J. Kuwait Univ. Health Sci. Cent. 2003, 12, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Yao, K.; Yao, Y.; Shen, X.; Lu, C.; Guo, Q. Assessment of the oral health behavior, knowledge and status among dental and medical undergraduate students: A cross-sectional study. BMC Oral Health 2019, 19, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karem Hassan, B.; Jabbar Ali, B.; Mahmood Alwan, A.; Badeia, R.A. Self-Reported Oral Health Attitudes and Behaviors, and Gingival Status of Dental Students. Clin. Cosmet. Investig. Dent. 2020, 12, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Pitiphat, W.; Garcia, R.I.; Douglass, C.W.; Joshipura, K.J. Validation of self-reported oral health measures. J. Public Health Dent. 2002, 62, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Buhlin, K.; Gustafsson, A.; Andersson, K.; Håkansson, J.; Klinge, B. Validity and limitations of self-reported periodontal health. Community Dent. Oral Epidemiol. 2002, 30, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Franciscatto, G.J.; Koppe, B.T.F.; Hoppe, C.B.; Oliveira, J.A.P.; Haas, A.N.; Grecca, F.S.; Rossi-Fedele, G.; Gomes, M.S. Validation of self-reported history of root canal treatment in a southern Brazilian subpopulation. Braz. Oral Res. 2019, 33, e007. [Google Scholar] [CrossRef]
- Farmer, J.; Ramraj, C.; Azarpazhooh, A.; Dempster, L.; Ravaghi, V.; Quiñonez, C. Comparing self-reported and clinically diagnosed unmet dental treatment needs using a nationally representative survey. J. Public Health Dent. 2017, 77, 295–301. [Google Scholar] [CrossRef]
- Margozzini, P.; Berríos, R.; Cantarutti, C.; Veliz, C.; Ortuno, D. Validity of the self-reported number of teeth in Chilean adults. BMC Oral Health 2019, 19, 99. [Google Scholar] [CrossRef]
- Matsui, D.; Yamamoto, T.; Nishigaki, M.; Miyatani, F.; Watanabe, I.; Koyama, T.; Ozaki, E.; Kuriyama, N.; Kanamura, N.; Watanabe, Y. Validity of self-reported number of teeth and oral health variables. BMC Oral Health 2016, 17, 17. [Google Scholar] [CrossRef] [Green Version]
- Douglass, C.W.; Berlin, J.; Tennstedt, S. The validity of self-reported oral health status in the elderly. J. Public Health Dent. 1991, 51, 220–222. [Google Scholar] [CrossRef]
- Ueno, M.; Zaitsu, T.; Shinada, K.; Ohara, S.; Kawaguchi, Y. Validity of the self-reported number of natural teeth in Japanese adults. J. Investig. Clin. Dent. 2010, 1, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Høvik, H.; Kolberg, M.; Gjøra, L.; Nymoen, L.C.; Skudutyte-Rysstad, R.; Hove, L.H.; Sun, Y.Q.; Fagerhaug, T.N. The validity of self-reported number of teeth and edentulousness among Norwegian older adults, the HUNT Study. BMC Oral Health 2022, 22, 82. [Google Scholar] [CrossRef] [PubMed]
- Abbood, H.M.; Hinz, J.; Cherukara, G.; Macfarlane, T.V. Validity of Self-Reported Periodontal Disease: A Systematic Review and Meta-Analysis. J. Periodontol. 2016, 87, 1474–1483. [Google Scholar] [CrossRef] [PubMed]
- Eke, P.I.; Dye, B. Assessment of self-report measures for predicting population prevalence of periodontitis. J. Periodontol. 2009, 80, 1371–1379. [Google Scholar] [CrossRef]
- Ho, A.W.; Grossi, S.G.; Dunford, R.G.; Genco, R.J. Reliability of a self-reported health questionnaire in a periodontal disease study. J. Periodontal. Res. 1997, 32, 646–650. [Google Scholar] [CrossRef]
- Nilsson, I.M.; List, T.; Drangsholt, M. The reliability and validity of self-reported temporomandibular disorder pain in adolescents. J. Orofac. Pain 2006, 20, 138–144. [Google Scholar]
- Liu, Y. The relationship between lifestyle and self-reported oral health among American adults. Int. Dent. J. 2014, 64, 46–51. [Google Scholar] [CrossRef]
- Obregón-Rodríguez, N.; Fernández-Riveiro, P.; Piñeiro-Lamas, M.; Smyth-Chamosa, E.; Montes-Martínez, A.; Suárez-Cunqueiro, M.M. Prevalence and caries-related risk factors in schoolchildren of 12- and 15-year-old: A cross-sectional study. BMC Oral Health 2019, 19, 120. [Google Scholar] [CrossRef]
- Zhang, M.; Lan, J.; Zhang, T.; Sun, W.; Liu, P.; Wang, Z. Oral health and caries/gingivitis-associated factors of adolescents aged 12–15 in Shandong province, China: A cross-sectional Oral Health Survey. BMC Oral Health 2021, 21, 288. [Google Scholar] [CrossRef]
- Bramantoro, T.; Santoso, C.M.A.; Hariyani, N.; Setyowati, D.; Zulfiana, A.A.; Nor, N.A.M.; Nagy, A.; Pratamawari, D.N.P.; Irmalia, W.R. Effectiveness of the school-based oral health promotion programmes from preschool to high school: A systematic review. PLoS ONE 2021, 16, e0256007. [Google Scholar] [CrossRef]
- Geetha Priya, P.R.; Asokan, S.; Janani, R.G.; Kandaswamy, D. Effectiveness of school dental health education on the oral health status and knowledge of children: A systematic review. Indian J. Dent. Res. Off. Publ. Indian Soc. Dent. Res. 2019, 30, 437–449. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Item | Component * | ||||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |
| I am certain I brush my teeth properly | 0.68 | 0.01 | 0.17 | 0.03 | −0.07 |
| I use small, circular rotations while tooth brushing | 0.63 | 0.14 | −0.01 | 0.12 | −0.06 |
| I replace my toothbrush every 3 months | 0.60 | 0.16 | 0.04 | 0.10 | 0.20 |
| I use fluoride toothpaste | 0.48 | 0.13 | 0.11 | 0.00 | 0.39 |
| I brush my teeth for at least 3 min | 0.42 | 0.17 | 0.23 | 0.16 | −0.09 |
| I brush my tongue when tooth brushing | 0.43 | −0.12 | 0.16 | 0.18 | 0.33 |
| I have professional dental scaling at least once per year | 0.01 | 0.74 | 0.03 | 0.28 | 0.16 |
| I have professional dental scaling regularly | 0.05 | 0.73 | 0.08 | 0.35 | 0.15 |
| I visit a doctor of dental medicine twice per year for regular check-ups | 0.20 | 0.60 | 0.27 | 0.04 | 0.04 |
| I visit a doctor of dental medicine mostly for regular check-ups | 0.38 | 0.53 | 0.07 | −0.16 | 0.06 |
| I brush my teeth at least three times per day | 0.10 | 0.11 | 0.81 | 0.13 | 0.17 |
| I brush my teeth after each meal | 0.03 | 0.15 | 0.77 | 0.14 | 0.17 |
| I never omit evening tooth brushing | 0.27 | 0.09 | 0.64 | 0.00 | −0.18 |
| I use dental floss at least once per day | 0.18 | 0.18 | 0.15 | 0.82 | 0.05 |
| I use dental floss often during the day | 0.09 | 0.22 | 0.10 | 0.81 | 0.14 |
| I use interdental brushes | 0.02 | 0.17 | 0.13 | −0.06 | 0.66 |
| I use an electric toothbrush | −0.20 | 0.14 | −0.13 | 0.05 | 0.59 |
| When I brush my teeth, I intentionally massage the gingiva | 0.17 | 0.00 | 0.07 | 0.27 | 0.50 |
| I use mouth rinse | 0.27 | −0.02 | 0.07 | 0.30 | 0.36 |
| EIGEN | 2.27 | 2.00 | 1.93 | 1.85 | 1.66 |
| % VAR | 12.0 | 10.5 | 10.9 | 9.7 | 8.7 |
| Total % | 51.1 | ||||
| Basic Oral Hygiene Activities Scale | |||||
|---|---|---|---|---|---|
| Items | EIGEN | % VAR | Alpha | FS | Mean ± SD |
| 2.16 | 36.1 | 0.64 | |||
| I replace my toothbrush every 3 months | −0.67 | 3.48 ± 1.30 | |||
| I am certain I brush my teeth properly | −0.65 | 3.81 ± 1.03 | |||
| I use small, circular rotations while tooth brushing | −0.63 | 3.53 ± 1.17 | |||
| I use fluoride toothpaste | −0.60 | 3.22 ± 1.34 | |||
| I brush my teeth for at least 3 min | −0.54 | 3.55 ± 1.13 | |||
| I brush my tongue when tooth brushing | −0.50 | 3.44 ± 1.37 | |||
| Orientation to Dental Medicine Doctor Scale | |||||
| Items | EIGEN | % VAR | Alpha | FS | Mean ± SD |
| 2.06 | 51.5 | 0.68 | |||
| I have professional dental scaling regularly | 0.83 | 2.34 ± 1.26 | |||
| I have professional dental scaling at least once per year | 0.81 | 2.64 ± 1.42 | |||
| I visit a doctor of dental medicine twice per year for regular check-ups | 0.66 | 3.47 ± 1.34 | |||
| I visit a doctor of dental medicine mostly for regular dental check-ups | 0.54 | 3.27 ± 1.27 | |||
| Regularity of Tooth Brushing Scale | |||||
| Items | EIGEN | % VAR | Alpha | FS | Mean ± SD |
| 1.84 | 61.3 | 0.68 | |||
| I brush my teeth at least three times per day | 0.85 | 3.57 ± 1.27 | |||
| I brush my teeth after each meal | 0.82 | 2.98 ± 1.26 | |||
| I never omit evening tooth brushing | 0.67 | 4.13 ± 1.15 | |||
| Use of Dental Floss Scale | |||||
| Items | EIGEN | % VAR | Alpha | FS | Mean ± SD |
| 1.69 | 84.3 | 0.81 | |||
| I use dental floss often during the day | 0.92 | 2.28 ± 1.27 | |||
| I use dental floss at least once per day | 0.92 | 2.42 ± 1.43 | |||
| Additional and Detail Oral Hygiene Activities Scale | |||||
| Items | EIGEN | % VAR | Alpha | FS | Mean ± SD |
| 1.47 | 36.7 | 0.42 | |||
| I use interdental brushes | −0.65 | 2.61 ± 1.31 | |||
| When I brush my teeth, I intentionally massage the gingiva | −0.64 | 3.06 ± 1.32 | |||
| I use mouth rinse | −0.58 | 3.06 ± 1.42 | |||
| I use an electric toothbrush | −0.55 | 1.70 ± 1.15 | |||
| Variable | Female Students (N = 439) | Male Students (N = 219) | t-Test | p | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | MED | SKEW | KURT | K–S D | Mean ± SD | MED | SKEW | KURT | K–S D | |||
| Basic oral hygiene activities | 3.62 ± 0.74 | 3.50 | −0.01 | −0.46 | 0.08 * | 3.27 ± 0.66 | 3.17 | 0.33 | −0.02 | 0.11 * | 6.01 | <0.001 |
| Orientation to DMD | 3.00 ± 0.96 | 3.00 | 0.23 | −0.50 | 0.09 * | 2.78 ± 0.89 | 2.75 | 0.19 | −0.15 | 0.07 | 2.82 | 0.005 |
| Regularity of tooth brushing | 3.73 ± 0.92 | 4.00 | −0.60 | −0.05 | 0.14 * | 3.22 ± 0.96 | 3.00 | −0.03 | −0.56 | 0.09 | 6.65 | <0.001 |
| Use of dental floss | 2.52 ± 1.28 | 2.50 | 0.47 | −0.87 | 0.14 * | 2.00 ± 1.08 | 2.00 | 0.85 | −0.28 | 0.21 * | 5.15 | <0.001 |
| OHAQ Sum | 12.88 ± 2.81 | 12.58 | 0.24 | −0.24 | 0.06 | 11.27 ± 2.49 | 11.00 | 0.48 | 0.44 | 0.05 | 7.16 | <0.001 |
| Variable | Females (N = 439) | |||
| Basic Oral Hygiene Activities | Orientation to DMD | Regularity of Tooth Brushing | Use of Dental Floss | |
| Basic oral hygiene activities | 1.00 | 0.39 ** | 0.37 ** | 0.32 ** |
| Orientation to DMD | 0.39 ** | 1.00 | 0.35 ** | 0.40 ** |
| Regularity of tooth brushing | 0.37 ** | 0.35 ** | 1.00 | 0.28 ** |
| Use of dental floss | 0.32 ** | 0.40 ** | 0.28 ** | 1.00 |
| OHAQ Sum | 0.66 ** | 0.74 ** | 0.67 ** | 0.77 ** |
| Variable | Males (N = 219) | |||
| Basic Oral Hygiene Activities | Orientation to DMD | Regularity of Tooth Brushing | Use of Dental Floss | |
| Basic oral hygiene activities | 1.00 | 0.36 ** | 0.30 ** | 0.29 ** |
| Orientation to DMD | 0.36 ** | 1.00 | 0.29 ** | 0.39 ** |
| Regularity of tooth brushing | 0.30 ** | 0.29 ** | 1.00 | 0.21 * |
| Use of dental floss | 0.29 ** | 0.39 ** | 0.21 * | 1.00 |
| OHAQ Sum | 0.64 ** | 0.74 ** | 0.66 ** | 0.73 ** |
| Variable | Female OH Types | F | p | |||
| Excellent (N = 86) | Good (N = 120) | Satisfactory (N = 120) | Poor (N = 113) | |||
| Basic oral hygiene activities | 4.22 ± 0.60 | 3.83 ± 0.63 | 3.49 ± 0.61 | 3.08 ± 0.65 | 60.52 | <0.001 |
| Orientation to DMD | 4.01 ± 0.82 | 3.26 ± 0.78 | 2.78 ± 0.70 | 2.20 ± 0.61 | 109.15 | <0.001 |
| Regularity of tooth brushing | 4.43 ± 0.53 | 4.21 ± 0.60 | 3.58 ± 0.75 | 2.85 ± 0.82 | 111.81 | <0.001 |
| Use of dental floss | 4.35 ± 0.69 | 1.61 ± 0.54 | 3.17 ± 0.56 | 1.41 ± 0.51 | 587.78 | <0.001 |
| OHAQ Sum | 17.00 ± 1.37 | 12.92 ± 1.41 | 13.02 ± 1.13 | 9.54 ± 1.26 | 543.61 | <0.001 |
| Variable | Male OH Types | F | p | |||
| Excellent (N = 20) | Good (N = 71) | Satisfactory (N = 66) | Poor (N = 62) | |||
| Basic oral hygiene activities | 4.24 ± 0.53 | 3.32 ± 0.59 | 3.16 ± 0.53 | 3.01 ± 0.61 | 24.42 | <0.001 |
| Orientation to DMD | 3.93 ± 0.89 | 2.86 ± 0.85 | 2.97 ± 0.61 | 2.13 ± 0.69 | 33.38 | <0.001 |
| Regularity of tooth brushing | 4.23 ± 0.77 | 3.92 ± 0.65 | 3.07 ± 0.63 | 2.25 ± 0.57 | 95.93 | <0.001 |
| Use of dental floss | 3.85 ± 0.73 | 1.36 ± 0.47 | 2.89 ± 0.68 | 1.20 ± 0.36 | 213.85 | <0.001 |
| OHAQ Sum | 16.25 ± 1.51 | 11.46 ± 1.39 | 12.09 ± 1.27 | 8.59 ± 1.17 | 192.68 | <0.001 |
| Variable | Female Students | Male Students | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median | Min | Max | Mean ± SD | Median | Min | Max | |
| Tooth extraction | 0.69 ± 1.16 | 0 | 0 | 8 | 0.49 ± 1.05 | 0 | 0 | 5 |
| Filled teeth | 2.92 ± 2.30 | 2 | 0 | 9 | 2.27 ± 2.27 | 1 | 0 | 9 |
| Root canal treatment | 1.31 ± 1.67 | 1 | 0 | 9 | 1.00 ± 1.16 | 1 | 0 | 6 |
| Toothache | 2.08 ± 0.89 | 2 | 1 | 5 | 2.02 ± 0.91 | 2 | 1 | 5 |
| Use of analgesics | 1.46 ± 0.71 | 1 | 1 | 5 | 1.41 ± 0.68 | 1 | 1 | 5 |
| Use of antibiotics | 1.35 ± 0.67 | 1 | 1 | 5 | 1.26 ± 0.57 | 1 | 1 | 4 |
| Variable | Yes answer | No answer | Yes answer | No answer | ||||
| Frequency | % | Frequency | % | Frequency | % | Frequency | % | |
| Malocclusion | 122 | 27.8 | 317 | 72.2 | 57 | 26.0 | 162 | 74.0 |
| Orthodontic treatment | 200 | 45.6 | 239 | 54.4 | 82 | 37.4 | 137 | 62.6 |
| Dental crown or veneer | 25 | 5.7 | 414 | 94.3 | 12 | 5.5 | 207 | 94.5 |
| Prosthetic treatment | 10 | 2.3 | 429 | 97.7 | 6 | 2.7 | 213 | 97.3 |
| Variable | Female OH Types | F | p | |||
| Excellent (N = 86) | Good (N = 120) | Satisfactory (N = 120) | Poor (N = 113) | |||
| Tooth extraction | 0.81 ± 1.23 | 0.57 ± 1.02 | 0.66 ± 1.15 | 0.77 ± 1.27 | 0.92 | 0.43 |
| Filled teeth | 3.57 ± 2.76 | 3.09 ± 2.23 | 2.79 ± 2.25 | 2.39 ± 1.91 | 4.75 | 0.003 |
| Root canal treatment | 1.20 ± 1.75 | 1.49 ± 1.86 | 1.25 ± 1.55 | 1.25 ± 1.54 | 0.70 | 0.55 |
| Toothache | 1.87 ± 0.84 | 2.05 ± 0.86 | 2.02 ± 0.81 | 2.34 ± 0.99 | 5.08 | 0.002 |
| Use of analgesics | 1.45 ± 0.70 | 1.42 ± 0.63 | 1.42 ± 0.71 | 1.54 ± 0.81 | 0.66 | 0.57 |
| Use of antibiotics | 1.36 ± 0.61 | 1.33 ± 0.64 | 1.34 ± 0.64 | 1.38 ± 0.76 | 0.11 | 0.95 |
| Malocclusion | 0.22 ± 0.42 | 0.33 ± 0.47 | 0.26 ± 0.44 | 0.29 ± 0.46 | 1.02 | 0.38 |
| Orthodontic treatment | 0.47 ± 0.50 | 0.49 ± 0.50 | 0.43 ± 0.50 | 0.43 ± 0.50 | 0.37 | 0.77 |
| Variable | Male OH types | F | p | |||
| Excellent (N = 20) | Good (N = 71) | Satisfactory (N = 66) | Poor (N = 62) | |||
| Tooth extraction | 0.40 ± 0.75 | 0.45 ± 0.97 | 0.58 ± 1.12 | 0.47 ± 1.16 | 0.24 | 0.87 |
| Filled teeth | 2.10 ± 2.07 | 2.14 ± 2.06 | 2.61 ± 2.47 | 2.11 ± 2.35 | 0.69 | 0.56 |
| Root canal treatment | 0.75 ± 1.25 | 1.11 ± 1.32 | 1.08 ± 1.19 | 0.87 ± 0.88 | 0.88 | 0.45 |
| Toothache | 1.55 ± 0.94 | 2.04 ± 0.92 | 2.05 ± 0.88 | 2.11 ± 0.91 | 2.04 | 0.11 |
| Use of analgesics | 1.25 ± 0.44 | 1.32 ± 0.55 | 1.59 ± 0.86 | 1.35 ± 0.63 | 2.49 | 0.06 |
| Use of antibiotics | 1.15 ± 0.37 | 1.17 ± 0.38 | 1.41 ± 0.74 | 1.26 ± 0.57 | 2.40 | 0.07 |
| Malocclusion | 0.15 ± 0.37 | 0.30 ± 0.46 | 0.21 ± 0.41 | 0.31 ± 0.46 | 1.07 | 0.36 |
| Orthodontic treatment | 0.25 ± 0.44 | 0.42 ± 0.50 | 0.33 ± 0.48 | 0.40 ± 0.49 | 0.90 | 0.44 |
| Variable | Frequency of toothache groups | F | p | |||
| Never (N = 113) | Very Rarely (N = 219) | Rarely (N = 69) | Sometimes + Often (N = 38) | |||
| Basic oral hygiene activities | 3.77 ± 0.78 | 3.66 ± 0.71 | 3.38 ± 0.71 | 3.43 ± 0.71 | 5.11 | 0.002 |
| Orientation to DMD | 3.15 ± 1.00 | 3.02 ± 0.96 | 2.97 ± 0.89 | 2.49 ± 0.81 | 4.63 | 0.003 |
| Regularity of tooth brushing | 3.86 ± 0.89 | 3.77 ± 0.94 | 3.52 ± 0.88 | 3.49 ± 0.84 | 2.92 | 0.034 |
| Use of dental floss | 2.80 ± 1.34 | 2.50 ± 1.26 | 2.38 ± 1.22 | 2.12 ± 1.21 | 3.43 | 0.017 |
| Variable | Number of filled teeth groups | F | p | |||
| 0–1 (N = 170) | 2–3 (N = 106) | 4–5 (N = 111) | 6 or more (N = 52) | |||
| Basic oral hygiene activities | 3.45 ± 0.69 | 3.67 ± 0.77 | 3.74 ± 0.71 | 3.87 ± 0.78 | 6.35 | <0.001 |
| Orientation to DMD | 2.99 ± 0.97 | 2.95 ± 0.96 | 2.92 ± 0.97 | 3.34 ± 0.88 | 2.62 | 0.050 |
| Regularity of tooth brushing | 3.70 ± 0.98 | 3.74 ± 0.95 | 3.70 ± 0.81 | 3.89 ± 0.85 | 0.66 | 0.58 |
| Use of dental floss | 2.51 ± 1.27 | 2.31 ± 1.18 | 2.51 ± 1.35 | 3.01 ± 1.26 | 3.54 | 0.015 |
| Variable | Frequency of toothache groups | F | p | |||
| Never (N = 67) | Very Rarely (N = 99) | Rarely (N = 39) | Sometimes + Often (N = 14) | |||
| Basic oral hygiene activities | 3.50 ± 0.69 | 3.16 ± 0.65 | 3.16 ± 0.54 | 3.20 ± 0.68 | 4.16 | 0.007 |
| Orientation to DMD | 2.93 ± 1.04 | 2.76 ± 0.83 | 2.64 ± 0.65 | 2.70 ± 1.11 | 0.97 | 0.41 |
| Regularity of tooth brushing | 3.42 ± 1.04 | 3.18 ± 0.87 | 3.00 ± 0.93 | 3.12 ± 1.19 | 1.76 | 0.16 |
| Use of dental floss | 2.10 ± 1.16 | 1.97 ± 1.07 | 1.99 ± 0.98 | 1.79 ± 1.05 | 0.41 | 0.75 |
| Variable | Number of filled teeth groups | F | p | |||
| 0–1 (N = 121) | 2–3 (N = 43) | 4–5 (N = 32) | 6 or more (N = 23) | |||
| Basic oral hygiene activities | 3.22 ± 0.62 | 3.48 ± 0.67 | 3.31 ± 0.72 | 3.06 ± 0.70 | 2.48 | 0.06 |
| Orientation to DMD | 2.83 ± 0.91 | 2.66 ± 0.90 | 2.88 ± 0.87 | 2.66 ± 0.86 | 0.63 | 0.60 |
| Regularity of tooth brushing | 3.22 ± 0.96 | 3.40 ± 0.92 | 3.11 ± 0.97 | 3.00 ± 1.03 | 1.05 | 0.37 |
| Use of dental floss | 2.00 ± 1.12 | 2.02 ± 1.03 | 2.05 ± 1.12 | 1.93 ± 0.91 | 0.05 | 0.98 |
| Female students | OHAQ index group | All | Test of Association | ||||
| High | Moderate | Low | |||||
| OH type | Excellent | 86 | 0 | 0 | 86 | Chi-square test | 529.31 |
| Good | 26 | 88 | 6 | 120 | df | 6 | |
| Satisfactory | 29 | 88 | 3 | 120 | p | <0.001 | |
| Poor | 0 | 13 | 100 | 113 | Cramer’s V | 0.78 | |
| All | 141 | 189 | 109 | 439 | p | <0.001 | |
| Male students | OHAQ index group | All | Test of Association | ||||
| High | Moderate | Low | |||||
| OH type | Excellent | 20 | 0 | 0 | 20 | Chi-square test | 241.68 |
| Good | 2 | 42 | 27 | 71 | df | 6 | |
| Satisfactory | 4 | 43 | 19 | 66 | p | <0.001 | |
| Poor | 0 | 1 | 61 | 62 | Cramer’s V | 0.74 | |
| All | 26 | 86 | 107 | 219 | p | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aranza, D.; Nota, A.; Galić, T.; Kozina, S.; Tecco, S.; Poklepović Peričić, T.; Milavić, B. Development and Initial Validation of the Oral Health Activities Questionnaire. Int. J. Environ. Res. Public Health 2022, 19, 5556. https://doi.org/10.3390/ijerph19095556
Aranza D, Nota A, Galić T, Kozina S, Tecco S, Poklepović Peričić T, Milavić B. Development and Initial Validation of the Oral Health Activities Questionnaire. International Journal of Environmental Research and Public Health. 2022; 19(9):5556. https://doi.org/10.3390/ijerph19095556
Chicago/Turabian StyleAranza, Diana, Alessandro Nota, Tea Galić, Slavica Kozina, Simona Tecco, Tina Poklepović Peričić, and Boris Milavić. 2022. "Development and Initial Validation of the Oral Health Activities Questionnaire" International Journal of Environmental Research and Public Health 19, no. 9: 5556. https://doi.org/10.3390/ijerph19095556
APA StyleAranza, D., Nota, A., Galić, T., Kozina, S., Tecco, S., Poklepović Peričić, T., & Milavić, B. (2022). Development and Initial Validation of the Oral Health Activities Questionnaire. International Journal of Environmental Research and Public Health, 19(9), 5556. https://doi.org/10.3390/ijerph19095556