
Systematic Review of the Health and Equity Impacts of Remediation and Redevelopment of Contaminated Sites †


 , ,
, ,
Abstract
1. Introduction
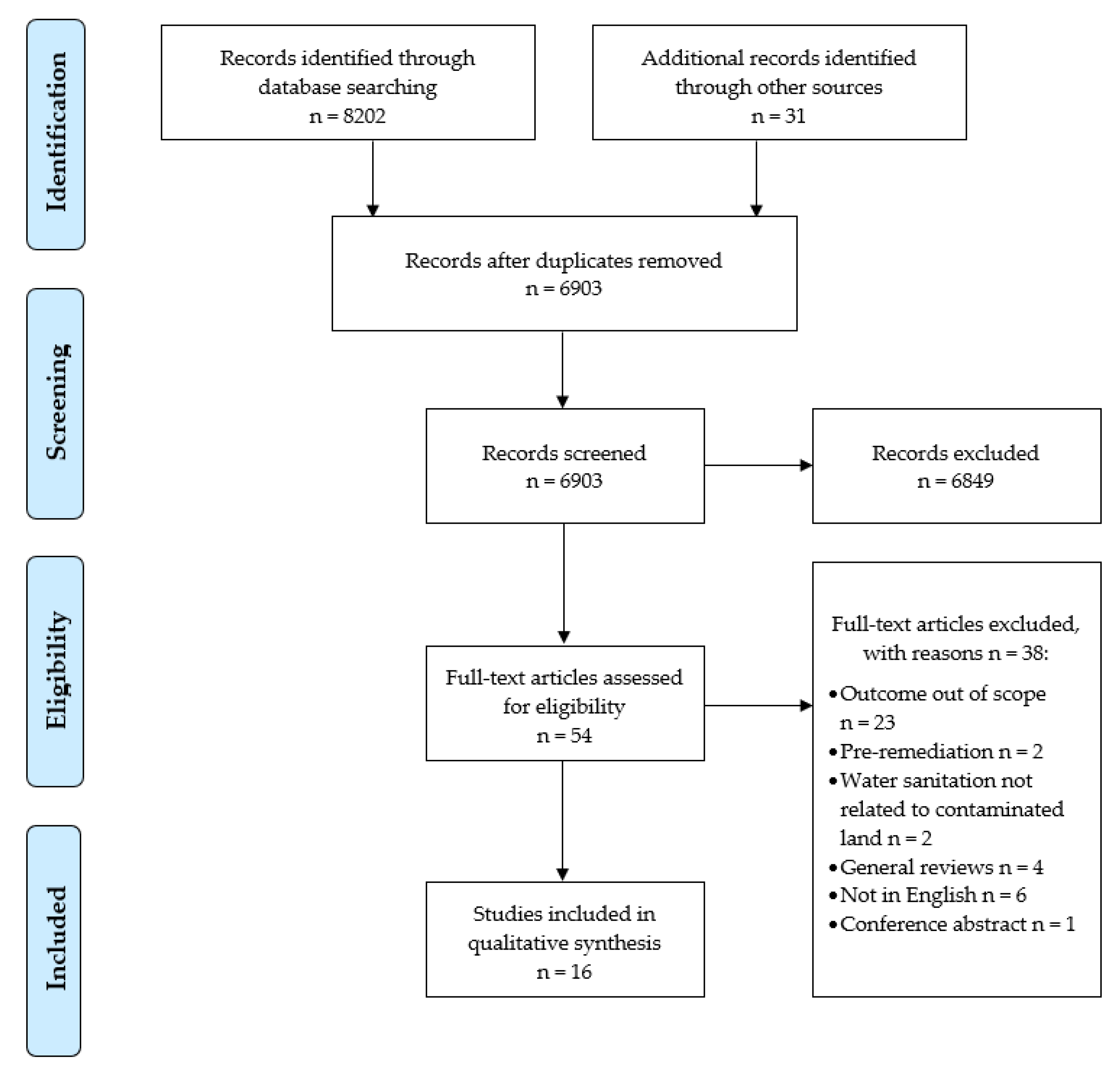
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Quality Appraisal
3. Results
3.1. Study Characteristics
3.2. Remediation Followed by Redevelopment
3.3. Existing Populations with Remediation and Public Health Intervention
3.4. Existing Population with Remediation Only
4. Discussion
4.1. Strengths and Limitations
4.2. Policy Implications and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Criteria | Scores | ||
|---|---|---|---|
| (A) SELECTION BIAS (Q1) Are the individuals selected to participate in the study likely to be representative of the target population? | Very likely = 11 Somewhat likely = 2 Can’t tell = 3 | ||
| (Q2) What percentage of selected individuals agreed to participate? | 80 to 100% = 4 60 to 79% = 3 Less than 60% = 3 Can’t tell = 6 | ||
| (B) STUDY DESIGN | Randomised control trial = 1 Cohort analytic = 2 Cohort (one group pre + post) = 1 Case control = 1 Interrupted time series = 3 Cross-sectional = 8 | ||
| (C) CONFOUNDERS (Q1) Were there important differences between groups prior to the intervention? | Yes = 10 No = 0 Can’t tell = 6 | ||
| (Q2) If yes, indicate the percentage of relevant confounders that were controlled (either in the design (e.g. stratification, matching) or analysis)? | 80 to 100% = 7 60 to 79% = 1 Less than 60% = 2 | ||
| (D) BLINDING (Q1) Was (were) the outcome assessor(s) aware of the intervention or exposure status of participants? | Yes = 4 No = 1 Can’t tell = 11 | ||
| (Q2) Were the study participants aware of the research question? | Yes = 3 No = 1 Can’t tell = 12 | ||
| (E) DATA COLLECTION METHODS (Q1) Were data collection tools shown to be valid? | Yes = 7 No = 1 Can’t tell = 8 | ||
| (Q2) Were data collection tools shown to be reliable? | Yes = 3 No = 1 Can’t tell = 12 | ||
| (F) WITHDRAWALS AND DROP-OUTS (Q1) Were withdrawals and drop-outs reported in terms of numbers and/or reasons per group? | Yes = 2 No = 2 N/A = 12 | ||
| (Q2) Indicate the percentage of participants completing the study. (If the percentage differs by groups, record the lowest). | 80 to 100% = 1 60 to 79% = 2 Less than 60% = 1 N/A = 12 | ||
| Strong | Moderate | Weak | |
| (A) SELECTION BIAS | 4 | 6 | 6 |
| (B) STUDY DESIGN | 1 | 7 | 8 |
| (C) CONFOUNDERS | 7 | 1 | 8 |
| (D) BLINDING | 1 | 0 | 15 |
| (E) DATA COLLECTION METHODS | 3 | 4 | 9 |
| (F) WITHDRAWALS AND DROP-OUTS (N/A = 12) | 1 | 1 | 2 |
| GLOBAL RATING | 0 | 0 | 16 |
References
- Souza, L.R.R.; Pomarolli, L.C.; da Veiga, M.A.M.S. From classic methodologies to application of nanomaterials for soil remediation: An integrated view of methods for decontamination of toxic metal(oid)s. Environ. Sci. Pollut. Res. 2020, 27, 10205–10227. [Google Scholar] [CrossRef] [PubMed]
- Coelho, P.C.D.S.; García-Lestón, J.; Silva, S.P.; da Costa, C.S.; da Costa, S.C.; Coelho, M.I.; Lage, B.L.; Mendez, E.P.; Teixeira, J.P. Geno- and immunotoxic effects on populations living near a mine: A case study of panasqueira mine in Portugal. J. Toxicol. Environ. Health Part A 2011, 74, 1076–1086. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Yan, X.; Zhong, L.; Tong, X. Benzene homologues contaminants in a former herbicide factory site: Distribution, attenuation, risk, and remediation implication. Environ. Geochem. Health 2020, 42, 241–253. [Google Scholar] [CrossRef] [PubMed]
- Payá Pérez, A.; Rodriguez Eugenio, N. Status of local soil contamination in Europe. In Revision of the Indicator “Progress in the Management Contaminated Sites in Europe”, EUR 29124 EN; Publications Office of the European Union: Luxembourg, 2018. [Google Scholar]
- WHO Regional Office for Europe. Human Health in Areas with Industrial Contamination; WHO Regional Office for Europe: Copenhagen, Denmark, 2014. [Google Scholar]
- WHO Regional Office for Europe. Declaration of Sixth Ministerial Conference on Environmental and Health; WHO Regional Office for Europe: Copenhagen, Denmark, 2017; Available online: https://apps.who.int/iris/handle/10665/347444 (accessed on 26 November 2021).
- WHO Regional Office for Europe. Protecting Health through Urban Redevelopment of Contaminated Sites; A Planning Brief. WHO Regional Office for Europe: Copenhagen, Denmark, 2021; Available online: https://apps.who.int/iris/handle/10665/349922 (accessed on 26 November 2021).
- European Commission. EU Soil Policy; European Commission: Brussels, Belgium, 2021; Available online: https://ec.europa.eu/environment/soil/soil_policy_en.htm (accessed on 26 November 2021).
- Martin-Olmedo, P.; Ranzi, A.; Santoro, M.; Dack, S.; de Hoogh, K.; Martuzzi, M.; Dogliotti, E.; Hoek, G.; Tomasova, J.; Dimovska, M.; et al. Methods and data needs to assess health impacts of chemicals in industrial contaminated sites. Epidemiol. Prev. 2019, 43, 223–237. [Google Scholar] [PubMed]
- Martuzzi, M.; Pasetto, R.; Martin-Olmedo, P. Industrially contaminated sites and health. J. Environ. Pub. Health 2014, 2014, 198574. [Google Scholar] [CrossRef] [PubMed]
- Engelhaupt, E. Happy birthday, Love Canal. Environ. Sci. Technol. 2008, 42, 8179–8186. [Google Scholar] [CrossRef] [PubMed]
- Green, D.; Sullivan, M.; Cooper, N.; Dean, A.; Marquez, C. A pilot study of children’s blood lead levels in Mount Isa, Queensland. Int. J. Environ. Res. Public Health 2017, 14, 1567. [Google Scholar] [CrossRef]
- Kalsi, A.; Celin, S.M.; Bhanot, P.; Sahai, S.; Sharma, J.G. Microbial remediation approaches for explosive contaminated soil: Critical assessment of available technologies, recent innovations and Future prospects. Environ. Technol. Innov. 2020, 18, 100721. [Google Scholar] [CrossRef]
- Kiaghadi, A.; Rifai, H.S.; Dawson, C.N. The presence of Superfund sites as a determinant of life expectancy in the United States. Nat. Commun. 2021, 12, 1947. [Google Scholar] [CrossRef]
- Prasad, L.R.; Nazareth, B. Contamination of allotment soil with lead: Managing potential risks to health. J. Public Health Med. 2020, 22, 525–530. [Google Scholar] [CrossRef][Green Version]
- Reisinger, H.J.; Burris, D.R.; Hering, J.G. Remediating subsurface arsenic contamination with monitored natural attenuation. Environ. Sci. Technol. 2005, 39, 458A–464A. [Google Scholar] [CrossRef] [PubMed]
- Farmer, J.G.; Jarvis, R. Strategies for improving human health in contaminated situations: A review of past, present and possible future approaches. Environ. Geochem. Health 2009, 31, 227–238. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Ros, J.M.; Garcia, G.; Penas, J.M. Assessment of restoration success of former metal mining areas after 30 years in a highly polluted Mediterranean mining area: Cartagena-La union. Ecol. Eng. 2013, 57, 393–402. [Google Scholar] [CrossRef]
- Eckley, C.S.; Gilmour, C.C.; Janssen, S.; Luxton, T.P.; Randall, P.M.; Whalin, L.; Austin, C. The assessment and remediation of mercury contaminated sites: A review of current approaches. Sci. Total Environ. 2020, 707, 136031. [Google Scholar] [CrossRef]
- Wcisło, E.; Bronder, J.; Bubak, A.; Rodríguez-Valdés, E.; Gallego, J.L.R. Human health risk assessment in restoring safe and productive use of abandoned contaminated sites. Environ. Int. 2016, 94, 436–448. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, S.M.; Pereira, M.E.; da Silva, E.F.; Hursthouse, A.S.; Duarte, A.C. A review of regulatory decisions for environmental protection: Part I—Challenges in the implementation of national soil policies. Environ. Int. 2009, 35, 202–213. [Google Scholar] [CrossRef] [PubMed]
- Environment Agency. Dealing with Contaminated Land in England and Wales; Environment Agency: Bristol, UK, 2009. [Google Scholar]
- Wcisło, E.; Ioven, D.; Kucharski, R.; Szdzuj, J. Human health risk assessment case study: An abandoned metal smelter site in Poland. Chemosphere 2002, 47, 507–515. [Google Scholar] [CrossRef]
- Yaffee, A.Q.; Scott, B.; Kaelin, C.; Cambron, J.; Sanderson, W.; Christian, W.J.; Moran, T.P.; Chamness, J. Collaborative response to arsenic-contaminated soil in an Appalachian Kentucky neighborhood. J. Toxicol. Environ. Health Part A 2019, 82, 697–701. [Google Scholar] [CrossRef]
- Gore, D.B.; Preston, N.J.; Fryirs, K.A. Post-rehabilitation environmental hazard of Cu, Zn, As and Pb at the derelict Conrad Mine, eastern Australia. Environ. Pollut 2007, 148, 491–500. [Google Scholar] [CrossRef]
- Jain, P.; Townsend, T.G.; Johnson, P. Case study of landfill reclamation at a Florida landfill site. Waste Manag. 2013, 33, 109–116. [Google Scholar] [CrossRef]
- Gong, Y.; Zhao, D.; Wang, W. An overview of field-scale studies on remediation of soil contaminated with heavy metals and metalloids: Technical progress over the last decade. Water Res. 2018, 147, 440–460. [Google Scholar] [CrossRef] [PubMed]
- Jing, R.; Fusi, S.; Kjellerup, B.V. Remediation of Polychlorinated Biphenyls (PCBs) in contaminated soils and sediment: State of knowledge and perspectives. Front. Environ. Sci. 2018, 6, 79. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 105906. [Google Scholar] [CrossRef]
- De Sario, M.; Pasetto, R.; Vecchi, S.; Zeka, A.; Hoek, G.; Michelozzi, P.; Iavarone, I.; Fletcher, T.; Bauleo, L.; Ancona, C. A scoping review of the epidemiological methods used to investigate the health effects of industrially contaminated sites. Epidemiol. Prev. 2018, 42, 59–68. [Google Scholar] [PubMed]
- Tabacaru, S. Web of Science versus Scopus: Journal Coverage Overlap Analysis. Texas A&M University Libraries. 2019. Available online: https//hdl.handle.net/1969.1/175137 (accessed on 21 April 2022).
- Falagas, M.E.; Pitsouni, E.I.; Malietzis, G.A.; Pappas, G. Comparison of PubMed, Scopus, Web of Science, and Google Scholar: Strengths and weaknesses. FASEB J. 2008, 22, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Effective Public Healthcare Panacea Project. Quality Assessment Tool for Quantitative Studies. 2022. Available online: https://www.ephpp.ca/quality-assessment-tool-for-quantitative-studies/ (accessed on 25 April 2022).
- Louekari, K.; Mroueh, U.M.; Maidell-Münster, L.; Valkonen, S.; Tuomi, T.; Savolainen, K. Reducing the risks of children living near the site of a former lead smeltery. Sci. Total Environ. 2004, 319, 65–75. [Google Scholar] [CrossRef]
- Schoof, R.A.; Johnson, D.L.; Handziuk, E.R.; Landingham, C.V.; Feldpausch, A.M.; Gallagher, A.E.; Dell, L.D.; Kephart, A. Assessment of blood lead level declines in an area of historical mining with a holistic remediation and abatement program. Environ. Res. 2016, 150, 582–591. [Google Scholar] [CrossRef]
- Mielke, H.W.; Gonzales, C.R.; Powell, E.T.; Mielke, P.W. Environmental and health disparities in residential communities of New Orleans: The need for soil lead intervention to advance primary prevention. Environ. Int. 2013, 51, 73–81. [Google Scholar] [CrossRef]
- Maisonet, M.; Bove, F.J.; Kaye, W.E. A case-control study to determine risk factors for elevated blood lead levels in children, Idaho. Toxicol. Ind. Health 1997, 13, 67–72. [Google Scholar] [CrossRef]
- Sheldrake, S.; Stifelman, M. A case study of lead contamination cleanup effectiveness at Bunker Hill. Sci. Total Environ. 2003, 303, 105–123. [Google Scholar] [CrossRef]
- Von Lindern, I.; Spalinger, S.; Petroysan, V.; von Braun, M. Assessing remedial effectiveness through the blood lead:soil/dust lead relationship at the Bunker Hill Superfund Site in the Silver Valley of Idaho. Sci. Total Environ. 2003, 303, 139–170. [Google Scholar] [CrossRef]
- Hilts, S.R.; Bock, S.E.; Oke, T.L.; Yates, C.L.; Copes, R.A. Effect of interventions on children’s blood lead levels. Environ. Health Persp. 1998, 106, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Goulet, L.; Messier, A.; Gaudreau, J. Results of a lead decontamination program. Arch. Environ. Health 1996, 51, 68–72. [Google Scholar] [CrossRef]
- Tirima, S.; Bartrem, C.; von Lindern, I.; von Braun, M.; Lind, D.; Anka, S.M.; Abdullahi, A. Environmental remediation to address childhood lead poisoning epidemic due to artisanal gold mining in Zamfara, Nigeria. Environ. Health Persp. 2016, 124, 1471–1478. [Google Scholar] [CrossRef]
- Boreland, F.; Lesjak, M.S.; Lyle, D.M. Managing environmental lead in Broken Hill: A public health success. New South Wales Public Health Bull. 2008, 19, 174–179. [Google Scholar] [CrossRef]
- Aschengrau, A.; Beiser, A.; Bellinger, D.; Copenhafer, D.; Weitzman, M. Residential lead-based-paint hazard remediation and soil lead abatement: Their impact among children with mildly elevated blood lead levels. Am. J. Public Health 1997, 87, 1698–1702. [Google Scholar] [CrossRef]
- Freeman, N.C.G.; Wainman, T.; Lioy, P.J.; Stern, A.H.; Shupack, S.I. The effect of remediation of chromium waste sites on chromium levels in urine of children living in the surrounding neighborhood. J. Air Waste Manag. Assoc. 1995, 45, 604–614. [Google Scholar] [CrossRef]
- Lanphear, B.P.; Succop, P.; Roda, S.; Henningsen, G. The effect of soil abatement on blood lead levels in children living near a former smelting and milling operation. Public Health Rep. 2003, 118, 83–91. [Google Scholar] [CrossRef]
- Choi, A.L.; Levy, J.I.; Dockery, D.W.; Ryan, L.M.; Tolbert, P.E.; Altshul, L.M.; Korrick, S.A. Does living near a Superfund site contribute to higher polychlorinated biphenyl (PCB) exposure? Environ. Health Persp. 2006, 114, 1092–1098. [Google Scholar] [CrossRef]
- Burgos, S.; Tenorio, M.; Zapata, P.; Cáceres, D.D.; Klarian, J.; Alvarez, N.; Oviedo, R.; Toro-Campos, R.; Claudio, L.; Iglesias, V. Cognitive performance among cohorts of children exposed to a waste disposal site containing heavy metals in Chile. Int. J. Environ. Health Res. 2017, 27, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Madeddu, R.; Tolu, P.; Asara, Y.; Farace, C.; Forte, G.; Bocca, B. Blood biomonitoring of metals in subjects living near abandoned mining and active industrial areas. Environ. Monit. Assess. 2013, 185, 5837–5846. [Google Scholar] [CrossRef] [PubMed]
- Mielke, H.W.; Covington, T.P.; Mielke, P.W., Jr.; Wolman, F.J.; Powell, E.T.; Gonzales, C.R. Soil intervention as a strategy for lead exposure prevention: The New Orleans lead-safe childcare playground project. Environ. Pollut. 2011, 159, 2071–2077. [Google Scholar] [CrossRef] [PubMed]
- Greene, N.A.; White, J.D.; Morris, V.R.; Roberts, S.; Jones, K.L.; Warrick, C. Evidence for environmental contamination in residential neighborhoods surrounding the defense depot of Memphis, Tennessee. Int. J. Environ. Res. Public Health 2006, 3, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Pasetto, R.; Mattioli, B.; Marsili, D. Environmental justice in industrially contaminated sites. A review of scientific evidence in the WHO European Region. Int. J. Environ. Res. Public Health 2019, 16, 998. [Google Scholar] [CrossRef] [PubMed]
- Colles, A.; Ardeleanu, E.R.; Candeias, C.; Ranzi, A.; Demeter, Z.; Hofer, A.; Kowalska, M.; Makris, K.C.; Arrebola, J.P.; Schoeters, G.; et al. Human biomonitoring as a tool for exposure assessment in industrially contaminated sites (ICSs). Lessons learned within the ICS and Health European Network. Epidemiol. E Prev. 2019, 43, 249–259. [Google Scholar]
- Panagos, P.; Van Liedekerke, M.; Yigini, Y.; Montanarella, L. Contaminated sites in Europe: Review of the current situation based on data collected through a European network. J. Environ. Public Health 2013, 2013, 158764. [Google Scholar] [CrossRef]
- European Environment Agency. Land and Soil in Europe: Why We Need to Use These Vital and Finite Resources Sustainably; European Environment Agency: Copenhagen, Denmark, 2019; Available online: https://www.eea.europa.eu/signals/signals-2019-content-list/articles/land-and-soil-towards-the (accessed on 26 November 2021).
- United Nations. Sustainable Development Goals—Goal 12: Sustainable Consumption and Production Patterns; United Nations: New York, NY, USA, 2020; Available online: https://www.un.org/sustainabledevelopment/sustainable-consumption-production (accessed on 26 November 2021).
- WHO Regional Office for Europe. Circular Economy and Health: Opportunities and Risks; WHO Regional Office for Europe: Copenhagen, Denmark, 2018; Available online: https://apps.who.int/iris/handle/10665/342218 (accessed on 26 November 2021).
- European Commission. A European Green Deal. European Commission: Brussels, Belgium, 2020. Available online: europa.eu (accessed on 26 November 2021).
- Cummins, S.; Clark, C.; Lewis, D.; Smith, N.; Thompson, C.; Smuk, M.; Stansfeld, S.; Taylor, S.; Fahy, A.; Greenhalgh, T.; et al. The effects of the London 2012 Olympics and related urban regeneration on physical and mental health: The ORiEL mixed-methods evaluation of a natural experiment. Public Health Res. 2018, 6, 1–248. [Google Scholar] [CrossRef]

| # | Terms (adj = Adjacent) |
|---|---|
| 1 | ((industr * OR mining OR mine OR quarries OR quarry OR waste OR incinerat * OR landfill * OR port OR harbor OR harbour OR ship OR dock OR superfund OR brownfield OR contaminat * OR site OR plant OR plants OR mill OR farm * OR agricult * OR land OR soil OR rail * OR derelict) AND (petro * OR pesticide * OR polymer * OR organochemical * OR colouring OR pharmaceutical OR paper OR metallurg * OR potter * OR fertilizer * OR footwear OR shoe * OR lindane OR plastic OR rubber OR detergent * OR lubricant * OR lubricating * OR weapon * OR glass OR iron OR steel OR asbestos OR fluoroedenite OR fluoro-edenite OR amosite OR erionite OR balangeroite OR tremolite OR crocidolite OR chrysotile OR serpentine OR antigorite OR anthophyllite OR actinolite OR ferroactinolite OR amphibole * OR lead OR cadmium OR arsenic OR nickel OR tin OR mercury OR chromium OR polyaromatic hydrocarbons OR cyanide OR polychlorinated biphenyls OR phenol OR BTEX OR benzene OR toluene OR ethylbenzene OR xylene OR trichloroethane OR vinyl chloride OR blue billy OR leblanc OR methane OR sewage sludge OR metal * OR gasworks OR filling station OR coal tar OR pulverised fly ash OR furnace bottom ash OR chemical OR oil OR chlorinate * OR volatile organic compound *)) |
| 2 | “data mining” |
| 3 | 1 NOT 2 |
| 4 | (remediat * OR conver * OR renewal OR regenerat * OR rehabilitat * OR redevelop * OR reclamat * OR reuse OR re-use OR “clean-up *” OR restorat * OR cleanup * OR “clean * up *”) |
| 5 | 3 AND 4 |
| 6 | (health * OR mortality OR morbidity OR disease OR chronic OR infection OR syndrome * OR irritation OR ache * OR headache * OR nausea * OR sick OR pain OR sclerosis OR dent * OR neoplasm * OR tumor * OR tumour * OR cancer * OR lymphoma * OR leukaemia * OR leukemia * OR myelodysplas * OR myalgia * OR neuralgia * OR respirator * OR heart OR cardio * OR vascular OR stroke OR pulmonary OR lung OR respiratory OR renal OR kidney * OR bone OR digestive OR congenital OR reproductive OR semen OR retard * OR fetal OR foetal OR preterm OR pre-term OR miscarriage OR abort * OR pregnan * OR birth * OR death * OR neuro * OR muscl * OR urin * OR blood OR serum OR hair OR gland * OR throat OR eye * OR genotoxic * OR muta * OR biomonitoring OR bio-monitoring OR psych * OR brain OR skin OR epiderm * OR quality of life OR QoL OR satisfaction OR depression OR anxi * OR nervous OR stress OR sleep OR insomnia OR concentrat * OR cognitive) |
| 7 | 5 AND 6 |
| 8 | remove duplicates from 7 |
| # | Author and Date | Title |
|---|---|---|
| 35 | Louekari et al., 2004 | Reducing the risks of children living near the site of a former lead smeltery |
| 36 | Schoof et al., 2015 | Assessment of blood lead level declines in an area of historical mining with a holistic remediation and abatement program. |
| 37 | Mielke et al., 2013 | Environmental and health disparities in residential communities of New Orleans: The need for soil lead intervention to advance primary prevention |
| 38 | Maisonet et al., 1997 | A case-control study to determine risk factors for elevated blood lead levels in children, Idaho |
| 39 | Sheldrake and Stifleman 2003 | A case study of lead contamination cleanup effectiveness at Bunker Hill |
| 40 | Von Lindern et al., 2003 | Assessing remedial effectiveness through the blood lead:soil/dust lead relationship at the Bunker Hill Superfund Site in the Silver Valley of Idaho |
| 41 | Hilts et al., 1998 | Effect of interventions on children’s blood lead levels |
| 42 | Goulet et al., 1996 | Results of a lead decontamination program |
| 43 | Tirima et al., 2016 | Environmental remediation to address childhood lead poisoning epidemic due to artisanal gold mining in Zamfara, Nigeria |
| 44 | Boreland et al., 2008 | Managing environmental lead in Broken Hill: a public health success |
| 45 | Aschengrau et al., 1997 | Residential lead-based-paint hazard remediation and soil lead abatement: Their impact among children with mildly elevated blood lead levels |
| 46 | Freeman et al., 1995 | The effect of remediation of chromium waste sites on chromium levels in urine of children living in the surrounding neighborhood |
| 47 | Lanphear et al., 2003 | The effect of soil abatement on blood lead levels in children living near a former smelting and milling operation |
| 48 | Choi et al., 2006 | Does living near a Superfund site contribute to higher polychlorinated biphenyl (PCB) exposure? |
| 49 | Burgos et al., 2017 | Cognitive performance among cohorts of children exposed to a waste disposal site containing heavy metals in Chile |
| 50 | Madeddu et al., 2013 | Blood biomonitoring of metals in subjects living near abandoned mining and active industrial areas |
| Study | Contaminant, Source and Remediation | Location | Study Design and Comparator | Population and Sample Size | Outcome Measures | Results |
|---|---|---|---|---|---|---|
| Louekari et al., 2004 | Pb from a smelter (active 1929–1984). Surface soil replacement of area with Pb > 300 mg/kg prior to construction of new apartments, and in school and day care centre yards. | Tikkurila, Vantaa, Finland | Cross-sectional; comparators are unremediated areas and remote reference site. Secondary environmental data used to estimate exposure. | Population: 678 children aged 0–6 years living near smelter. Sample: 52 children from population (10 from unremediated area) and 11 from reference area. | Pb in air, water, lettuce, berries, and dust in household and day care centre. BLL | Air and water not important exposure route. Soil Pb ~20 mg/kg in remediated and reference areas, and >300 mg/kg in unremediated areas. blood lead levels (BLLs) in unremediated areas = 2.7 µg/dL, greater than in remediated areas (2.1 µg/dL) (p = 0.027); remediated areas comparable to reference areas of <2.0 µg/dL. |
| Mielke et al., 2013 | Pb from multiple sources including industry and incinerator. Surface soil replacement of soils with >1000 mg/kg in homes; childcare centres (also had geotextile beneath soil), eleven public parks and 9 out of 10 public housing projects (during reconstruction). | New Orleans, LA, USA | Cohort analytic; comparator is low (< 100 mg/kg) soil Pb areas. | Pre-Katrina: 55,551 blood Pb samples from children. Post-Katrina: 7384 blood Pb samples from children. | BLL Percentage of children with BLL > 10 µg/dL. Percentage of children with BLL > 5 µg/dL. | Differences between soil and BLLs are significant (p < 0.001) between high Pb (median = 425 mg/kg) and low Pb (45 mg/kg) areas. BLLs reduced post-Katrina, in low (both medians = 3.0 µg/dL) and high Pb areas (3.0 vs. 5.6 µg/dL) (p < 0.001). Proportion of children with BLLs > 5 µg/dL reduced post-Katrina in low (7.5% vs. 24.8%) and high Pb areas (29.6% vs. 58.5%). Proportion of children with BLLs > 10 µg/dL reduced post-Katrina in low (3.0% vs. 1.0%) and high Pb areas (6.5% vs. 21.8%). |
| Schoof et al., 2015 | Pb from copper mine. Stabilising, capping or removing waste and contaminated soils. Redevelopment to parks, activity centers and trails. Remediation ongoing. | Butte, MT, USA | Repeat cross-sectional; comparator is reference dataset. | 2796 children aged 1–5 years (2003–2010) covering pre- and post-remediation. | BLL Percentage of children with BLL > 5 µg/dL and >10 µg/dL. | Decline in children with BLLs > 10 µg/dL from 3.4% to 1.5%; BLLs > 5 µg/dL from 33.6% to 9.5%. Butte BLLs greater than reference BLLs for 2003–2004 (mean = 3.48 vs. 2.05 µg/dL; p < 0.05), 2005–2006 (2.65 vs. 1.80 µg/dL; p < 0.05), and 2007–2008 (2.2 vs. 1.72 µg/dL; p < 0.05), but comparable for 2009–2010 (1.53 vs. 1.51 µg/dL). Butte BLL declined by 24% per 2-year increment, reference by 9% (p < 0.001). BLL greater in the uptown/historic area closer to mine, than ‘the flats’ area but only significant in 2007–2008 (p = 0.001) and 2009–2010 (p = 0.02). |
| Study | Contaminant, Source and Remediation | Location | Study Design and Comparator | Population and Sample Size | Outcome Measures | Results |
|---|---|---|---|---|---|---|
| Freeman et al., 1995 | Cr, wastes from Cr manufacturing and refining. Sites capped and/or soil replaced (early 1990–late 1991). Public health campaign to reduce dust exposure. | Hudson County, NJ, USA | Cross-sectional; comparator is control areas (public housing and more affluent neighbourhoods) and pre-remediation data. | 64 children: 41 children from Lafayette Gardens (public housing project surrounded on three sides by Cr waste sites) and 23 children from three control areas. | Cr levels in urine. | Cr concentrations in urine in children from Lafayette Gardens in Summer greater than controls (median 0.28 µg/L vs. 0.17 µg/L; p = 0.055) N.B. not significant in Winter. Cr concentrations in urine were age-dependent and related to home location. Controlling for personal rate of excretion and age, exposure status predicted Cr (regression coefficient = −0.347, SE 0.155, p = 0.03). Direct relationship between activities and Cr levels not confirmed. |
| Aschengrau et al., 1997 | Pb from unspecified sources in soil and house paint. Phase 1: soil removal, addition of geotextile and soil replacement, dust abatement in homes and loose-paint stabilisation. Phase 2: soil remediation and interior and exterior paint remediation. Public health campaign. | Boston, MA, USA | Randomised control trial with three groups (Phase 1: 1: all treatments, 2: dust abatement and paint stabilisation, 3: paint stablisation; Phase 2: groups 2 and 3 offered soil remediation; all groups offered paint remediation. | 152 children aged <4 years, with BLLs 7–24 µg/dL. Group 1 n = 54; group 2 n = 51; group 3 n = 47. | BLL | After Phase 2: group 1 children whose homes received only paint hazard remediation had mean blood lead levels (BLLs) 2.6 µg/dL (Confidence Interval (CI) = −0.6–5.9 µg/dL) greater than children who received no intervention. Group 2/3 children whose homes received paint hazard remediation and soil remediation had mean BLLs 1.4 µg/dL (CI = −0.73.5 µg/dL) greater than those whose homes had only soil abatement. After adjustment for confounders: group 1 children receiving paint hazard remediation had 6.5 µg/dL greater BLLs than those who did not (p = 0.05), there was no significant difference between the BLLs in group 2/3 children who did or did not receive paint hazard remediation (p = 0.36) suggesting soil remediation is effective. |
| Goulet et al., 1996 | Pb from Pb reclamation plant (closed 1989). Asphalting plant yard, removing dust from roads and sidewalks, soil replacement, professional home cleaning (1989–1990). Public health targeting families with young children. | St-Jean-sur-Richelieu, QC, Canada | Cohort, one group pre-post remediation. | Children who lived 200 m from plant in 1991. Sample of 101 children aged 6 months-10 years (79.2% of population), 75 children in 1989 and 1991 sample. | BLL Percentage of children with BLL > 15 µg/dL. | In children who had participated in both surveys BLLs reduced from 9.7 µg/dL (95% CI = 8.6–10.9) in 1989 to 5.0 µg/dL (CI = 4.5–5.6) in 1991 (p < 0.001); children 6 months-5 years reduced from 9.8 µg/dL (CI = 8.6–11.2) to 5.5 µg/dL (CI = 4.9–6.3) (p < 0.001). In 1991, no children had blood Pb > 15 µg/dL compared with 21.3% in 1989. Percentage of children engaged in pica reduced from 35.5% (1989) to 18.8% (1991) (p = 0.004); putting things in mouth reduced from 46.2% to 31.7% (p = 0.03). |
| Hilts et al., 1998 | Pb from a Pb/Zn smelter. Dust abatement including capping soils, use of a dust suppressant and greening. Public health campaign to raise awareness including provision of cleaning materials. | Trail, QC, Canada | Interrupted time series, screening programme, comparator is preceding year’s BLL. | Children aged 6–72 months. Sample size declined from 169 in 1989 to 46 in 1996. | BLL | BLLs reduced by 0.6 µg/dL (≈5%) per year between 1989 and 1996. In case management children, decline in BLLs (2.3 to 4.0 µg/dL) in the year following the intervention was significant for those receiving the intervention in 1991 (p < 0.001), 1992 (p < 0.001) and 1994 (p = 0.001). |
| Boreland et al., 2008 | Pb from Pb mine. Capping of soil material, greening of bare soil. Public health campaign to raise awareness. | Broken Hill, New South Wales, Australia | Interrupted time series, screening programme, comparator is preceding years’ BLL. | Children aged 1–4 years, participation declined from 72% in 1994 to 46% in 2007. | BLL Dust Pb levels. | Mean BLLs reduced from 16.3 µg/dL (in 1991) to 5.8 µg/dL in 2007. Mean BLLs in the highest risk zone reduced from 27.3 µg/dL in 1991 to 8.3 µg/dL in 2007. Dust concentrations were significantly greater in 1991–1994, compared with 1995–1999 (p < 0.05). |
| Tirima et al., 2016 | Pb from informal gold mining. Soil removal from residential and communal areas and ponds; landfill disposal. Public health campaign to reduce exposure through safer mining practices. | Eight villages, northern Nigeria | Repeat cross-sectional screening programme to identify at children at risk, alongside phased remediation. | 4399 children aged < 5 years. | BLL Soil Pb levels. | Mean BLL reduced from 149 µg/dL to 15 µg/L over four-year period. Phase 1 (2 villages) soil Pb levels reduced by 98% and 96% to 83 mg/kg and 179 mg/kg respectively; 74 children screened before and during remediation had mean BLL of 149 µg/dL and 230 screened after remediation had mean BLL 76 µg/dL. Phase 2 (5 villages) soil Pb between 300 mg/kg and 1343 mg/kg reduced by 77% and 93% respectively; 3326 children screened and BLLs drop from ~48 µg/dL to ~25 µg/dL. Phase 3 (1 village with industrial area) mean soil Pb concentrations reduced by 87% from 670 to 90 mg/kg; BLL reduced from 25 to 15 µg/dL. |
| Maisonet et al., 1997 | Pb from mine and smelter (closed 1981). Yard remediation; new yards remediated each summer since 1989. | Bunker Hill Superfund Site, ID, USA. | Case-control study, comparator is age and sex-matched children with BLL <10 µg/dL. | Population: 295 children aged 1–9 years. Sample: 138 participants (69 matched pairs). | BLL | Logistic regression: yard remediation associated with blood Pb levels after adjustment for income and education (Odds Ratio = 0.28, CI = 0.08–0.92, p < 0.05); pets in and out of house, hours spent playing outdoors, smoking inside house, child washes hands before bed, child puts dirt in mouth all non-significant. |
| Sheldrake and Stifleman 2003 | As above. Pb from mine and smelter (closed 1981) Soil capping in parks and schools (1986), soil removal in residential yards, commercial properties and rights of way, and indoor dust based on child BLLs, soil concentrations and risk (1989-). Program expanded (1994-) to clean up adjacent parcels of land and areas with soils with >1000 mg/kg. Public health campaign to raise awareness and reduce exposure. By 2001, 80% of homes exceeding 1000 mg/kg were remediated. | Repeat cross-sectional, comparator is pre-remediation. | Children aged 9 months-9 years in the area offered annual BLL screening; percentage of eligible in sample exceeded 50% each year. | BLL Percentage of children with BLL > 10 µg/dL. | Percentage of children with BLL > 10 µg/dL; reduced over 80% un 1983 to 57.1% in 1998 to 4.4% in 2001 in 1-year-olds, 2-year-olds 60.9% to 9.8%, 3-year-olds 62.1% to 2.5%, 4-year-olds 36.8% to 4.3%; all children (<9 years) 46% to 3%. | |
| Von Lindern et al., 2003 | Interrupted time series, comparator is preceding year’s BLLs | Children in the area which is home to 7000 people in 5 communities; 230 to 445 children aged 9 months-9 years tested each year between 1988 and 2001; estimated as 50% of children on school records. 4000 paired BLL and environmental samples. | BLL Percentage of children with BLL > 10 µg/dL. Percentage of children with BLL > 15 µg/dL. | Percentage of children with BLL > 15 µg/dL reduced from 15% to 1.2% between 1988 and 2001; percentage with >10 µg/dL reduced from 45% to 3.1% between 1988 and 2001. Average BLL significantly different (p < 0.05) compared with preceding year in 1989–1994, and 1998. BLLs reduced 50–60% with greatest decrease corresponding with initial home yard remediation. Proportion of children living with contaminated yards (>1000 mg/kg) decreased from 80% in 1988–1989, to 43% in 1990 and 25% in 1991, fluctuated between 18–29% between 1992 and 1996 despite remediation of additional 551 homes (inward migration), by 1999 only 4% had contaminated yards. BLLs in control, remediation and public health intervention group reduced by 0.4 µg/dL, 2.5 µg/dL and 4.8 µg/dL respectively (p < 0.001). Suggests remediation reduces typical 2-year old’s BLLs by 7.5 µg/dL between 1989 and 2001 (1.7 µg/dL from individual yard, 5.6 µg/dL from community and neighbourhood), and public health intervention results in an additional 3.9 µg/dL reduction. |
| Study | Contaminant, Source and Remediation | Location | Study Design and Comparator | Population and Sample Size | Outcome Measures | Results |
|---|---|---|---|---|---|---|
| Lanphear et al., 2003 | Pb and As from a mine and smelter. Tailings capped, soil removed from yards with Pb concentrations <500 mg/kg and replaced with clean soil. | Midvale, UT, USA | Repeat cross-sectional, comparator is yards without remediation. | Children aged 6–72 months in 1989 (n = 112) and 1998 (n = 215) | BLLs As and Pb in soil and dust. | 1989: Greater levels of As and Pb soil and dust concentrations (p = 0.0001), interior and exterior paint Pb concentrations (p = 0.004 and p = 0.006 respectively), and = blood lead levels (BLLs) in children (5.6 µg/dL vs. 3.9 µg/dL; p = 0.0001) in homes eligible for soil remediation compared with those that were not; 11% of children in homes eligible for yard remediation had BLLs > 10 µg/dL, compared with 2.6% in the control group. 1998: no significant differences between the intervention and the control groups for BLLs (3.0 µg/dL vs. 2.6 µg/dL), dust As and Pb concentrations and soil As concentrations; soil Pb concentrations greater in control homes compared with yard remediation (95 vs. 54 mg/kg; p = 0.02); 1% of children in homes with yard remediation had BLLs > 10 µg/dL. After adjustment for potential confounders (age, mouthing behaviour, socioeconomic status, year) BLL declined by 2.3 µg/dL (CI = 1.8–2.9 µg/dL), BLLs intervention group reduced 42.8% faster than control group (p = 0.14), BLLs declined faster in children aged 6-36 months (2.5 µg/dL, CI = 1.8–3.5 µg/dL; p = 0.03) than those aged 36–72 months (2.0 µg/dL, CI = 1.3–3.0 µg/dL; p = 0.03). |
| Burgos et al., 2017 | Pb (with As, Cd, Cu) in abandoned waste site (active 1984–1999) Waste removed, roofs of homes cleaned, decontamination of other areas of the city, site fenced and covered (1999–2003). | Arica, Chile | Cross-sectional, comparator is children born post-remediation. | Population: 735 children aged 6–15 years Sample: 180 children selected at random. | BLLs As levels in urine. Cognitive performance (Wechsler Intelligence Scale for Children). | BLLs 2 µg/dL in both cohorts (p = 0.059), no significant difference in As in urine (p = 0.369). Cognitive performance greater in post-remediation cohort (91.1 points) compared with pre-remediation (81.9 points). Processing Speed Index and Absence of Distractibility Index were the only components that were not different between cohorts, other components were statistically significant. After adjusting for age, sex, maternal IQ and paternal education, the estimated difference in total IQ between cohorts increases (pre-remediation is reference): during remediation β = 9.97; 95% CI 0.82 to 19.13; post remediation β = 16.14; 95% CI 1.53 to 30.74. |
| Choi et al., 2006 | PCBs, waste disposal from local industry (1940s–1977) Dredging of contaminated sediments (1994–1995). | New Bedford Harbour Superfund Site, MA, USA | Cohort analytic study of infants, comparator is infants born pre-remediation. | Population: 788 mother-infant pairs where mother >18 years old Sample: 720 (69 excluded). | Umbilical cord PCB levels; total PCBs, light PCBs, heavy PCBs, 51 congeners and PCB-118. | Multivariate models: maternal age and birthplace were the strongest predictors of ΣPCB levels (p < 0.001). Maternal consumption of organ meat and local dairy products was associated with higher, and smoking and previous lactation with lower, ΣPCB levels (p < 0.05). Infants born later in the study had lower ΣPCB levels than infants born earlier in the study. There was a 17% change (−3 to 40%) in ΣPCB for infants born before/during dredging compared with those born after dredging (p < 0.10). |
| Madeddu et al., 2013 | Cd, Cr, Cu, Mn, Pb and Zn. Two former metal mines, one former coal mine, one active industrial area (mines restored 1990s). | Sulcis-Iglesiente, Sardinia, Italy | Cross-sectional study, comparator is a control area with no industry or mining. | Sample: 265 healthy adults. | Cd, Cr, Cu, Mn, Pb and Zn blood levels (BLs). | Participants within 5 km of active industrial site (n = 29) have greater BLs than those in the control area: Cd (p = 0.05), Cu (p = 0.031), Mn (p = 0.05) and Pb (p < 0.001); within 2 km of coal mine (n = 48): Cd (p = 0.036), Mn (p = 0.005), Pb (p = 0.006) and Zn (p = 0.005); within 4 km of Pb/Zn mine (n = 129): Cd (p = 0.041), Mn (p = 0.037), Pb (p = 0.005) and Zn (p = 0.004); and within 3 km of Pb/Zn mine (n = 32): Mn (p = 0.022). Those within 3 km of Pb/Zn mine restored (n = 32) have greater BLs than control: Cu (p = 0.019) and Pb (p = 0.011). Cd, Pb and Zn positively correlated with age. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sinnett, D.; Bray, I.; Baranyi, G.; Braubach, M.; Netanyanhu, S. Systematic Review of the Health and Equity Impacts of Remediation and Redevelopment of Contaminated Sites. Int. J. Environ. Res. Public Health 2022, 19, 5278. https://doi.org/10.3390/ijerph19095278
Sinnett D, Bray I, Baranyi G, Braubach M, Netanyanhu S. Systematic Review of the Health and Equity Impacts of Remediation and Redevelopment of Contaminated Sites. International Journal of Environmental Research and Public Health. 2022; 19(9):5278. https://doi.org/10.3390/ijerph19095278
Chicago/Turabian StyleSinnett, Danielle, Isabelle Bray, Gergő Baranyi, Matthias Braubach, and Sinaia Netanyanhu. 2022. "Systematic Review of the Health and Equity Impacts of Remediation and Redevelopment of Contaminated Sites" International Journal of Environmental Research and Public Health 19, no. 9: 5278. https://doi.org/10.3390/ijerph19095278
APA StyleSinnett, D., Bray, I., Baranyi, G., Braubach, M., & Netanyanhu, S. (2022). Systematic Review of the Health and Equity Impacts of Remediation and Redevelopment of Contaminated Sites. International Journal of Environmental Research and Public Health, 19(9), 5278. https://doi.org/10.3390/ijerph19095278