
Evaluation Methods Applied to Digital Health Interventions: What Is Being Used beyond Randomised Controlled Trials?—A Scoping Review

 ,
, 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Literature Search
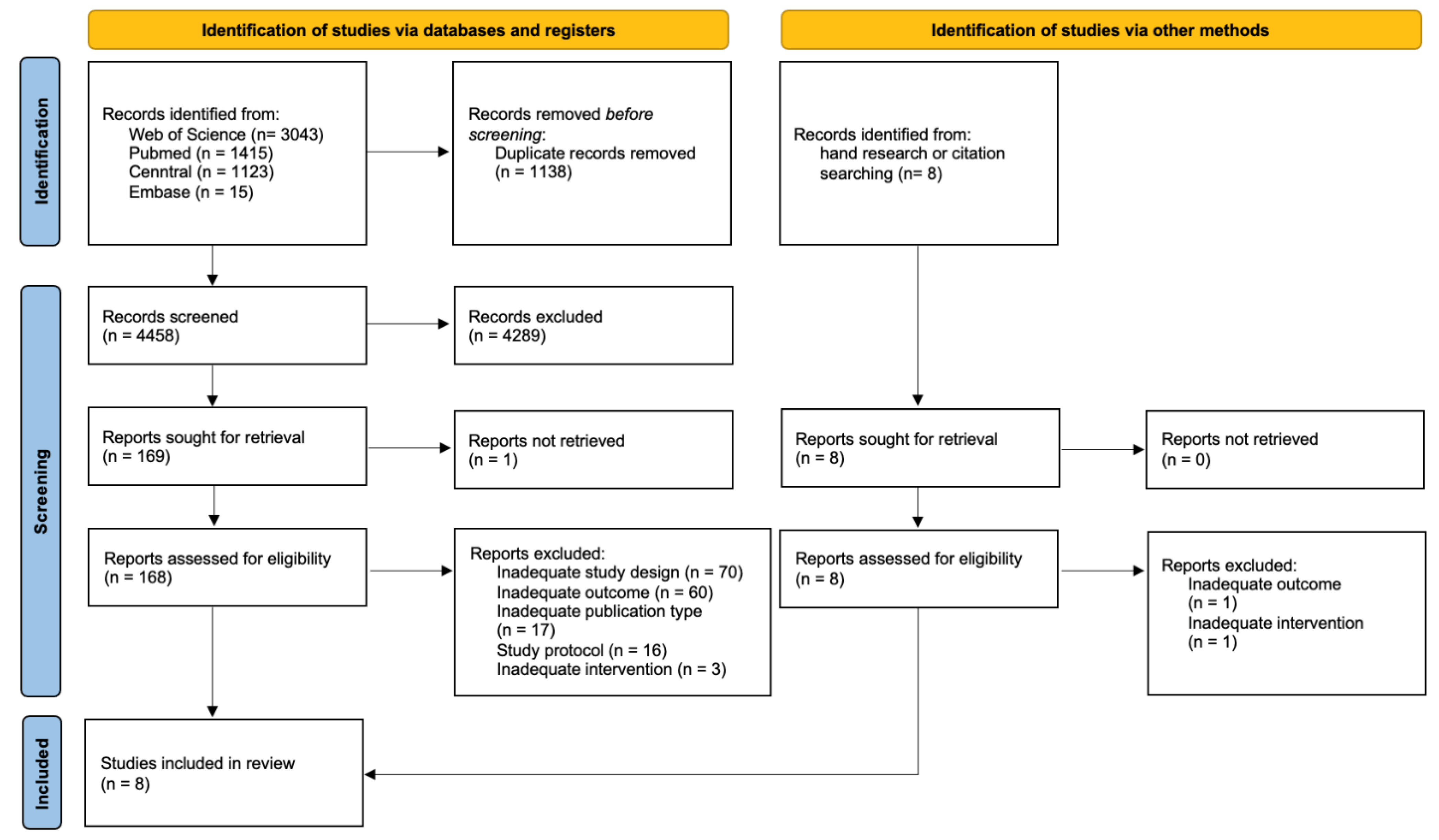
3. Results
3.1. Description of the Study Characteristics
3.2. Difference of Identified Studies Compared to RCTs
3.2.1. Micro Randomisation Trial
3.2.2. (Fractional) Factorial Randomised Controlled Trials
3.2.3. Sequential Multiple Assignment Randomised Trial
3.2.4. Stepped-Wedge Cluster Randomised Trials
4. Discussion
4.1. Comparison to Other Work
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Torous, J.; Jän Myrick, K.; Rauseo-Ricupero, N.; Firth, J. Digital Mental Health and COVID-19: Using Technology Today to Accelerate the Curve on Access and Quality Tomorrow. JMIR Ment Health 2020, 7, e18848. [Google Scholar] [CrossRef] [PubMed]
- Kwasnicka, D.; Keller, J.; Perski, O.; Potthoff, S.; Ten Hoor, G.A.; Ainsworth, B.; Crutzen, R.; Dohle, S.; van Dongen, A.; Heino, M. White Paper: Open Digital Health–accelerating transparent and scalable health promotion and treatment. Health Psychol. Rev. 2022, 1–37. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, J.A.; Clark, C.R.; Bates, D.W. Digital Health Equity as a Necessity in the 21st Century Cures Act Era. JAMA 2020, 323, 2381–2382. [Google Scholar] [CrossRef] [PubMed]
- Willis, V.C.; Thomas Craig, K.J.; Jabbarpour, Y.; Scheufele, E.L.; Arriaga, Y.E.; Ajinkya, M.; Rhee, K.B.; Bazemore, A. Digital Health Interventions to Enhance Prevention in Primary Care: Scoping Review. JMIR Med. Inform. 2022, 10, e33518. [Google Scholar] [CrossRef] [PubMed]
- Newzoo. Number of Smartphone Users Worldwide from 2016 to 2020 and Forecast for 2024. Available online: https://de.statista.com/statistik/daten/studie/309656/umfrage/prognose-zur-anzahl-der-smartphone-nutzer-weltweit/ (accessed on 11 March 2022).
- Marcolino, M.S.; Oliveira, J.A.Q.; D’Agostino, M.; Ribeiro, A.L.; Alkmim, M.B.M.; Novillo-Ortiz, D. The Impact of mHealth Interventions: Systematic Review of Systematic Reviews. JMIR mHealth uHealth 2018, 6, e23. [Google Scholar] [CrossRef] [Green Version]
- Piantadosi, S. Clinical Trials: A Methodologic Perspective; John Wiley & Sons: New York, NY, USA, 2017. [Google Scholar]
- Thiese, M.S. Observational and interventional study design types; an overview. Biochem. Med. 2014, 24, 199–210. [Google Scholar] [CrossRef]
- Ioannidis, J.P. Effect of the statistical significance of results on the time to completion and publication of randomized efficacy trials. JAMA 1998, 279, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Mohr, D.C.; Schueller, S.M.; Riley, W.T.; Brown, C.H.; Cuijpers, P.; Duan, N.; Kwasny, M.J.; Stiles-Shields, C.; Cheung, K. Trials of Intervention Principles: Evaluation Methods for Evolving Behavioral Intervention Technologies. J. Med. Internet Res. 2015, 17, e166. [Google Scholar] [CrossRef]
- Bonten, T.N.; Rauwerdink, A.; Wyatt, J.C.; Kasteleyn, M.J.; Witkamp, L.; Riper, H.; van Gemert-Pijnen, L.J.; Cresswell, K.; Sheikh, A.; Schijven, M.P.; et al. Online Guide for Electronic Health Evaluation Approaches: Systematic Scoping Review and Concept Mapping Study. J. Med. Internet Res. 2020, 22, e17774. [Google Scholar] [CrossRef]
- Alqahtani, F.; Orji, R. Insights from user reviews to improve mental health apps. Health Inform. J. 2020, 26, 2042–2066. [Google Scholar] [CrossRef]
- Torous, J.; Nicholas, J.; Larsen, M.E.; Firth, J.; Christensen, H. Clinical review of user engagement with mental health smartphone apps: Evidence, theory and improvements. Evid. Based Ment. Health 2018, 21, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Skivington, K.; Matthews, L.; Simpson, S.A.; Craig, P.; Baird, J.; Blazeby, J.M.; Boyd, K.A.; Craig, N.; French, D.P.; McIntosh, E. A new framework for developing and evaluating complex interventions: Update of Medical Research Council guidance. BMJ 2021, 374, n2061. [Google Scholar] [CrossRef] [PubMed]
- McDonald, S.; Quinn, F.; Vieira, R.; O’Brien, N.; White, M.; Johnston, D.W.; Sniehotta, F.F. The state of the art and future opportunities for using longitudinal n-of-1 methods in health behaviour research: A systematic literature overview. Health Psychol. Rev. 2017, 11, 307–323. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almirall, D.; Nahum-Shani, I.; Sherwood, N.E.; Murphy, S.A. Introduction to SMART designs for the development of adaptive interventions: With application to weight loss research. Transl. Behav. Med. 2014, 4, 260–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, S.A. An experimental design for the development of adaptive treatment strategies. Stat. Med. 2005, 24, 1455–1481. [Google Scholar] [CrossRef] [Green Version]
- Collins, L.M.; Murphy, S.A.; Strecher, V. The multiphase optimization strategy (MOST) and the sequential multiple assignment randomized trial (SMART): New methods for more potent eHealth interventions. Am. J. Prev. Med. 2007, 32, 112–118. [Google Scholar] [CrossRef] [Green Version]
- Pham, Q.; Wiljer, D.; Cafazzo, J.A. Beyond the randomized controlled trial: A review of alternatives in mHealth clinical trial methods. JMIR mHealth uHealth 2016, 4, e5720. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.; Colquhoun, H.; Kastner, M.; Levac, D.; Ng, C.; Sharpe, J.P.; Wilson, K. A scoping review on the conduct and reporting of scoping reviews. BMC Med. Res. Methodol. 2016, 16, 15. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 88, 105906. [Google Scholar]
- Klasnja, P.; Hekler, E.B.; Shiffman, S.; Boruvka, A.; Almirall, D.; Tewari, A.; Murphy, S.A. Microrandomized trials: An experimental design for developing just-in-time adaptive interventions. Health Psychol. 2015, 34, 1220–1228. [Google Scholar] [CrossRef]
- Adams, M.A.; Hurley, J.C.; Todd, M.; Bhuiyan, N.; Jarrett, C.L.; Tucker, W.J.; Hollingshead, K.E.; Angadi, S.S. Adaptive goal setting and financial incentives: A 2 × 2 factorial randomized controlled trial to increase adults’ physical activity. BMC Public Health 2017, 17, 286. [Google Scholar]
- Du, H.L.; Venkatakrishnan, A.; Youngblood, G.M.; Ram, A.; Pirolli, P. A Group-Based Mobile Application to Increase Adherence in Exercise and Nutrition Programs: A Factorial Design Feasibility Study. JMIR mHealth uHealth 2016, 4, 140–155. [Google Scholar] [CrossRef] [Green Version]
- Palermo, T.M.; de la Vega, R.; Murray, C.; Law, E.; Zhou, C. A digital health psychological intervention (WebMAP Mobile) for children and adolescents with chronic pain: Results of a hybrid effectiveness-implementation stepped-wedge cluster randomized trial. Pain 2020, 161, 2763. [Google Scholar] [CrossRef] [PubMed]
- Spring, B.; Pfammatter, A.F.; Marchese, S.H.; Stump, T.; Pellegrini, C.; McFadden, H.G.; Hedeker, D.; Siddique, J.; Jordan, N.; Collins, L.M. A factorial experiment to optimize remotely delivered behavioral treatment for obesity: Results of the Opt-IN Study. Obesity 2020, 28, 1652–1662. [Google Scholar] [CrossRef]
- Strecher, V.J.; McClure, J.B.; Alexander, G.L.; Chakraborty, B.; Nair, V.N.; Konkel, J.M.; Greene, S.M.; Collins, L.M.; Carlier, C.C.; Wiese, C.J. Web-based smoking-cessation programs: Results of a randomized trial. Am. J. Prev. Med. 2008, 34, 373–381. [Google Scholar] [CrossRef] [Green Version]
- Schroé, H.; Van Dyck, D.; De Paepe, A.; Poppe, L.; Loh, W.W.; Verloigne, M.; Loeys, T.; De Bourdeaudhuij, I.; Crombez, G. Which behaviour change techniques are effective to promote physical activity and reduce sedentary behaviour in adults: A factorial randomized trial of an e-and m-health intervention. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 127. [Google Scholar] [CrossRef]
- Gonze, B.D.B.; Padovani, R.D.C.; Simoes, M.D.S.; Lauria, V.; Proença, N.L.; Sperandio, E.F.; Ostolin, T.L.V.D.P.; Gomes, G.A.D.O.; Castro, P.C.; Romiti, M. Use of a Smartphone App to Increase Physical Activity Levels in Insufficiently Active Adults: Feasibility Sequential Multiple Assignment Randomized Trial (SMART). JMIR Res. Protoc. 2020, 9, e14322. [Google Scholar] [CrossRef]
- Hurley, J.C.; Hollingshead, K.E.; Todd, M.; Jarrett, C.L.; Tucker, W.J.; Angadi, S.S.; Adams, M.A. The walking interventions through texting (WalkIT) trial: Rationale, design, and protocol for a factorial randomized controlled trial of adaptive interventions for overweight and obese, Inactive Adults. JMIR Res. Protoc. 2015, 4, e4856. [Google Scholar] [CrossRef] [PubMed]
- Collins, L.M.; Dziak, J.J.; Kugler, K.C.; Trail, J.B. Factorial experiments: Efficient tools for evaluation of intervention components. Am. J. Prev. Med. 2014, 47, 498–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, E.; Hekler, E.B.; Andersson, G.; Collins, L.M.; Doherty, A.; Hollis, C.; Rivera, D.E.; West, R.; Wyatt, J.C. Evaluating Digital Health Interventions: Key Questions and Approaches. Am. J. Prev. Med. 2016, 51, 843–851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavori, P.W.; Dawson, R.; Rush, A.J. Flexible treatment strategies in chronic disease: Clinical and research implications. Biol. Psychiatry 2000, 48, 605–614. [Google Scholar] [CrossRef]
- Gensorowsky, D.; Lampe, D.; Hasemann, L.; Düvel, J.; Greiner, W. Alternative study designs for the evaluation of digital health applications—A real alternative? Z. Für Evidenz Fortbild. Und Qual. Im Gesundh. 2021, 161, 33–41. [Google Scholar] [CrossRef]
- Rothwell, P.M. Factors That Can Affect the External Validity of Randomised Controlled Trials. PLoS Clin. Trials 2006, 1, e9. [Google Scholar] [CrossRef]
- Ho, A.M.H.; Phelan, R.; Mizubuti, G.B.; Murdoch, J.A.C.; Wickett, S.; Ho, A.K.; Shyam, V.; Gilron, I. Bias in Before–After Studies: Narrative Overview for Anesthesiologists. Anesth. Analg. 2018, 126, 1755–1762. [Google Scholar] [CrossRef] [Green Version]
- Noser, A.E.; Cushing, C.C.; McGrady, M.E.; Amaro, C.M.; Huffhines, L.P. Adaptive intervention designs in pediatric psychology: The promise of sequential multiple assignment randomized trials of pediatric interventions. Clin. Pract. Pediatric Psychol. 2017, 5, 170. [Google Scholar] [CrossRef]
- Baker, T.B.; Smith, S.S.; Bolt, D.M.; Loh, W.-Y.; Mermelstein, R.; Fiore, M.C.; Piper, M.E.; Collins, L.M. Implementing Clinical Research Using Factorial Designs: A Primer. Behav. Ther. 2017, 48, 567–580. [Google Scholar] [CrossRef]
- Dziak, J.J.; Nahum-Shani, I.; Collins, L.M. Multilevel factorial experiments for developing behavioral interventions: Power, sample size, and resource considerations. Psychol Methods 2012, 17, 153–175. [Google Scholar] [CrossRef]
- Brown, C.A.; Lilford, R.J. The stepped wedge trial design: A systematic review. BMC Med. Res. Methodol. 2006, 6, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, F. Digitale Interventionen in Prävention und Gesundheitsförderung: Welche Form der Evidenz haben wir und welche wird benötigt? Bundesgesundheitsblatt-Gesundh.-Gesundh. 2020, 63, 674–680. [Google Scholar] [CrossRef] [PubMed]
- Whitney, R.L.; Ward, D.H.; Marois, M.T.; Schmid, C.H.; Sim, I.; Kravitz, R.L. Patient perceptions of their own data in mHealth technology–enabled N-of-1 trials for chronic pain: Qualitative study. JMIR mHealth and uHealth 2018, 6, e10291. [Google Scholar] [CrossRef]
- van der Meulen, H.; McCashin, D.; O’Reilly, G.; Coyle, D. Using computer games to support mental health interventions: Naturalistic deployment study. JMIR Ment. Health 2019, 6, e12430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smiley, S.L.; Elmasry, H.; Hooper, M.W.; Niaura, R.S.; Hamilton, A.B.; Milburn, N.G. Feasibility of ecological momentary assessment of daily sexting and substance use among young adult African American gay and bisexual men: A pilot study. JMIR Res. Protoc. 2017, 6, e6520. [Google Scholar] [CrossRef] [PubMed]
- Holl, F.; Kircher, J.; Swoboda, W.J.; Schobel, J. Methods Used to Evaluate mHealth Applications for Cardiovascular Disease: A Quasi-Systematic Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 12315. [Google Scholar] [CrossRef] [PubMed]
- Pawson, R.; Manzano-Santaella, A. A realist diagnostic workshop. Evaluation 2012, 18, 176–191. [Google Scholar] [CrossRef] [Green Version]
- Pawson, R.; Tilley, N. Realist Evaluation; Sage: London, UK, 1997. [Google Scholar]
- Pawson, R. The Science of Evaluation: A Realist Manifesto; Sage: London, UK, 2013. [Google Scholar]
- Enam, A.; Torres-Bonilla, J.; Eriksson, H. Evidence-Based Evaluation of eHealth Interventions: Systematic Literature Review. J. Med. Internet Res. 2018, 20, e10971. [Google Scholar] [CrossRef]

{kind=link}
| Search Terms | Synonyms |
|---|---|
| Digital Health | Electronic Health, EHealth, Mobile Health, MHealth, Digital Health, Telehealth, Health Technology |
| Evaluation methods | Summative evaluation, Evaluation Studies as Topic (MeSH), Evaluation Methods, Alternative Study Designs, Evaluation Study (MeSH), effective*, efficacy, trial, “Research Design” “Randomised Controlled Trials as Topic/methods”, “Evaluation Studies as Topic”, Research Method*[tiab], Research Strateg*[tiab], Methodolog*[tiab], Alternative*[tiab] Effective*[tiab], Evaluation*[tiab], Quality[tiab]) |
| Author (Year) & Country | Study Design | Study Purpose | Study Sponsor | Targeted Condition | Data Collection Time-Points (Amount) | Duration (Weeks) | Sample Size | Control Group (CG) & Intervention Group (IG) | Masking | Group Assignment |
|---|---|---|---|---|---|---|---|---|---|---|
| Klasnja et al. (2019) [25] United States | MRT | Evaluation of efficacy of activity suggestions | Public funding | Physical activity | Daily (7540) | 6 | 44 | CG: None IG: Tailored walking suggestions | Participant: N.A. Practitioner: N.A. Assessors: N.A. | At each decision point: Individual randomisation to either no suggestion, walking suggestion or anti-sedentary suggestion |
| Adams et al. (2017) [26] United States | Factorial 2 × 2 design | Evaluation of effects for goal setting and rewards to increase daily steps | Public funding | Physical activity | Baseline and 4-months follow-up (2) | 16 | 96 | CG: None IG: Four intervention components (adaptive vs. static goal setting and immediate vs. delayed rewards) | Participant: None Practitioner: N.A. Assessors: Yes | Individual randomisation to one of four intervention components after baseline |
| Gonze et al. (2020) [32] Brazil | SMART | Evaluation of effects of a smartphone app for physical activity | Public funding | Physical activity | Baseline, 12-week follow-up and 24-week follow- up (3) | 24 | 18 | CG: TAU IG: Three intervention components (app only, app + tailored messages, and app + tailored messages and gamification) | Participant: None Practitioner: N.A. Assessors: Yes | First stage intervention: Individual randomisation to Group 1 (app only), Group 2 (app + tailored messages) or control group Second stage intervention: Individual rerandomisation of non-responders to Group 1 or 2 or Group 3 (app + tailored messages and gamification) |
| Du et al. (2016) [27] United States | Factorial 2 × 2 design | Evaluation of effects of a mHealth application on eating behaviour, physical activity, and stress level | Public and private funding | eating behaviour, physical activity, and stress level | Baseline, pre-test, and post-test follow-up (3) | 8 | 124 | CG: TAU IG: Four intervention conditions (emailed wellness programme, emailed wellness programme + team support, mobile walking and stress intervention, and mobile walking and stress intervention + team support) | Participant: Yes Practitioner: N.A. Assessors: N.A. | Individual randomisation to one of four intervention components before baseline |
| Palermo et al. (2020) [28] United States | Stepped-wedge cluster randomised trial | Evaluation of effectiveness and implementation of a digitally delivered psychosocial intervention for paediatric chronic pain | Public and private funding | Paediatric chronic pain | Baseline, 8ƒ-week follow-up and 3-month follow-up (3) | 20 | 143 | CG: TAU IG: Self-guided smartphone app for patients and their parents | Participant: None Practitioner: None Assessors: Yes | Random sequential crossover of the clinics in 1 of 4 waves from control to intervention |
| Schroé et al. (2020) [31] Belgium | Factorial 2 × 2 × 2 design | Evaluation of efficacy of behaviour change techniques on physical activity and sedentary behaviour | Public funding | Physical activity and sedentary behaviour | Baseline and 5-week follow-up (2) | 5 | 473 | CG: No behavioural technique IG: Seven intervention conditions consisting of action planning, coping planning, and self-monitoring | Participant: Yes Practitioner: None Assessors: N.A. | Block randomisation of participants to one of eight (control group counted in here) intervention groups |
| Spring et al. (2020) [29] United States | Factorial 2 × 5 design | Identification of intervention components that enhanced weight loss | In part Public Funding | Weight | Baseline, 3-months follow-up and 6-months follow-up (3) | 24 | 562 | CG: None IG: 32 intervention conditions consisting of coaching calls, primary care provider reports, meal replacements, buddy training, and text messaging | Participant: None Practitioner: None Assessors: Yes | Block randomisation of participants to one of 32 intervention groups |
| Strecher et al. (2008) [30] United States | Fractional factorial 2 × 4 design | Identify intervention components of a web-based smoking cessation programme | Public funding | Smoking | Baseline and 6-months follow-up (2) | 24 | 1866 | CG: None IG: 16 intervention conditions consisting of tailored success story, outcome expectation, efficacy expectation messages, source personalization, and exposure | Participant: Yes Practitioner: N.A. Assessors: N.A. | Individual randomisation to one of 16 intervention components |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hrynyschyn, R.; Prediger, C.; Stock, C.; Helmer, S.M. Evaluation Methods Applied to Digital Health Interventions: What Is Being Used beyond Randomised Controlled Trials?—A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 5221. https://doi.org/10.3390/ijerph19095221
Hrynyschyn R, Prediger C, Stock C, Helmer SM. Evaluation Methods Applied to Digital Health Interventions: What Is Being Used beyond Randomised Controlled Trials?—A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(9):5221. https://doi.org/10.3390/ijerph19095221
Chicago/Turabian StyleHrynyschyn, Robert, Christina Prediger, Christiane Stock, and Stefanie Maria Helmer. 2022. "Evaluation Methods Applied to Digital Health Interventions: What Is Being Used beyond Randomised Controlled Trials?—A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 9: 5221. https://doi.org/10.3390/ijerph19095221
APA StyleHrynyschyn, R., Prediger, C., Stock, C., & Helmer, S. M. (2022). Evaluation Methods Applied to Digital Health Interventions: What Is Being Used beyond Randomised Controlled Trials?—A Scoping Review. International Journal of Environmental Research and Public Health, 19(9), 5221. https://doi.org/10.3390/ijerph19095221