
Life Conditions as Mediators of Welfare State Effect on Mental Wellbeing among Oldest Old in Europe


Abstract
1. Introduction
2. Materials and Methods
2.1. The Source of Data and Variables
2.2. Welfare State Index (WSI)
2.3. Statistical Analyses
The following Steps Were Performed
- (1)
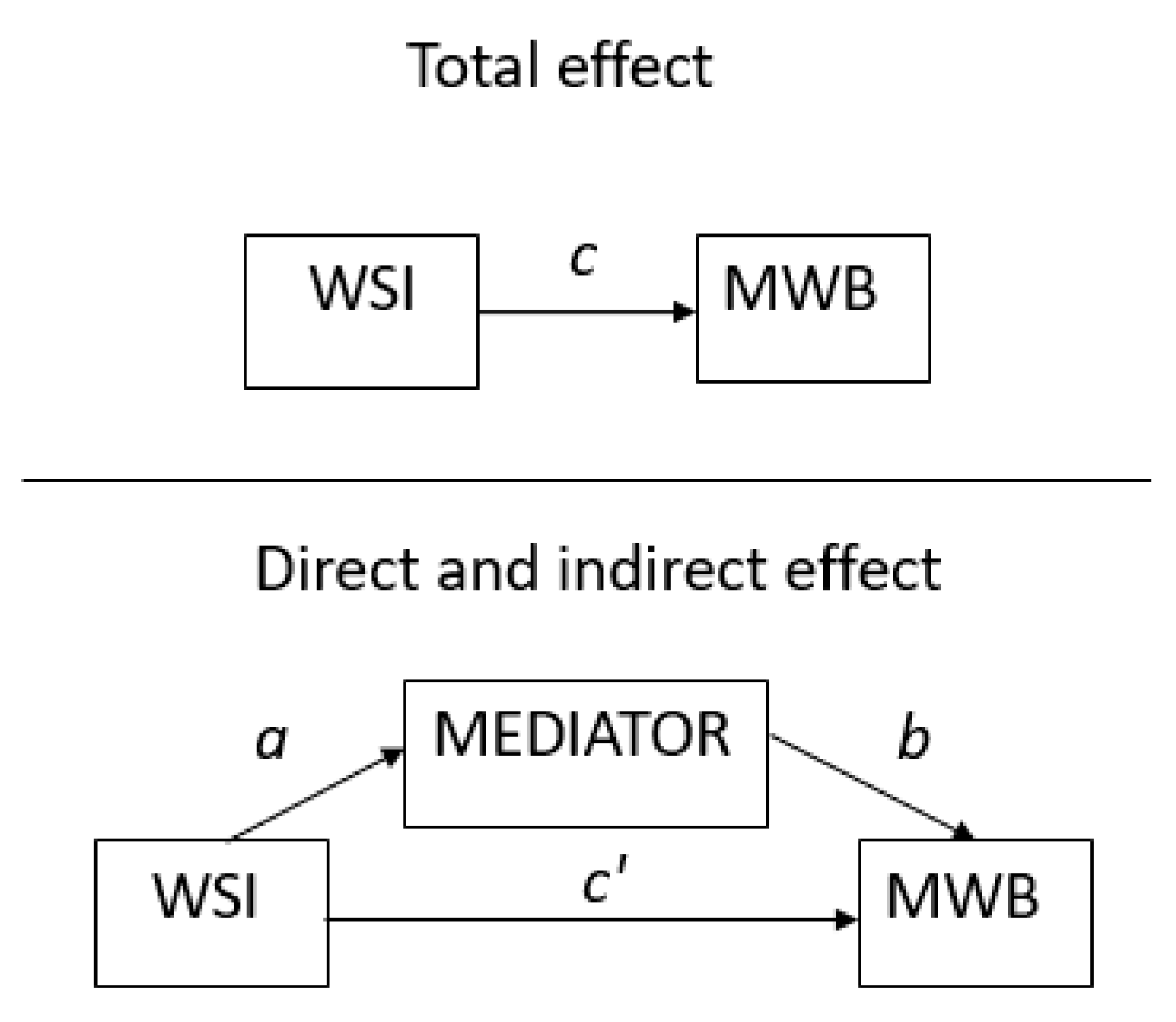
- An initial analysis of the total effect (path c in Figure 1) of WSI on mental wellbeing entailed five separate regression analyses, one for each mental wellbeing dimension, controlling for age and gender.
- (2)
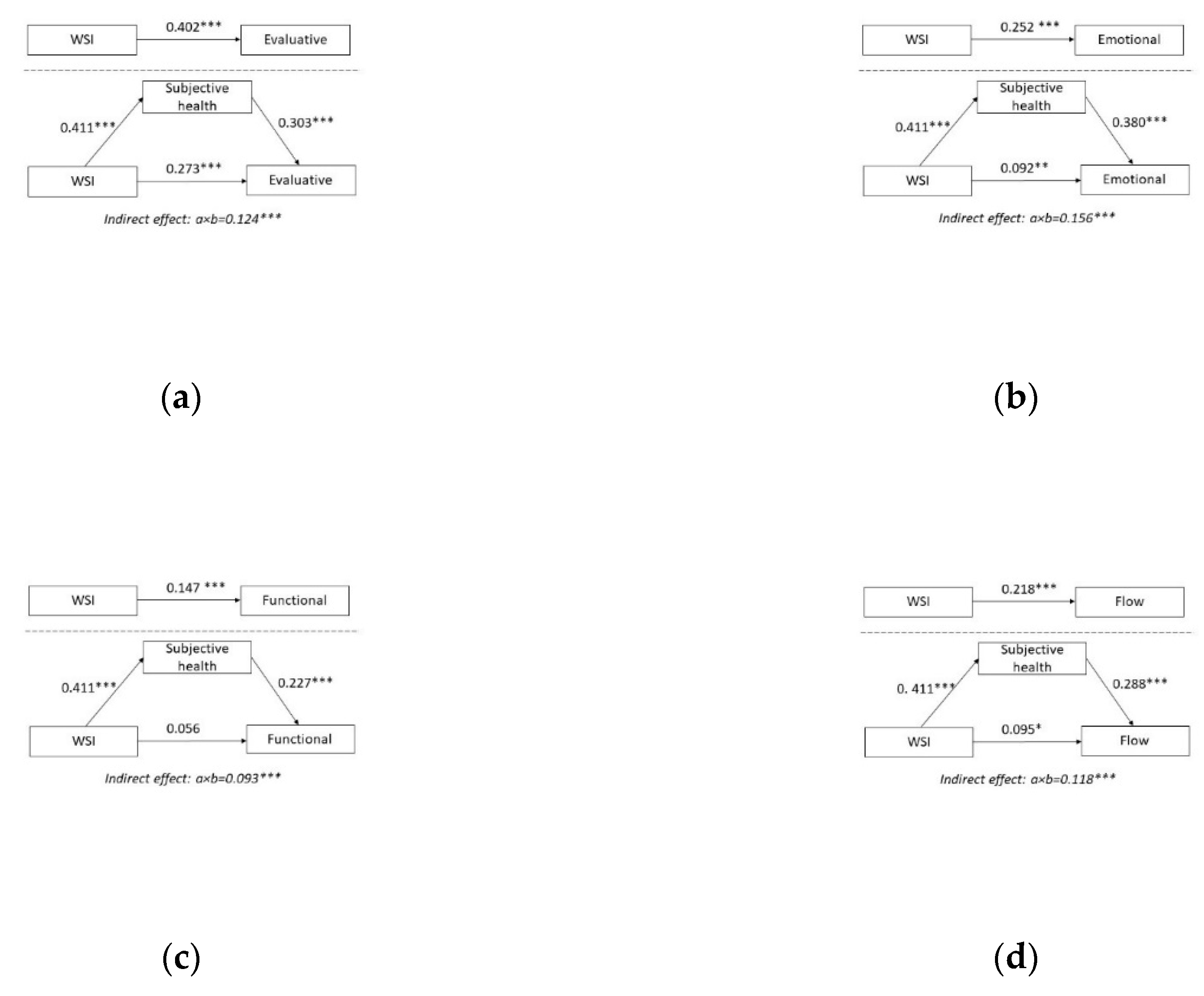
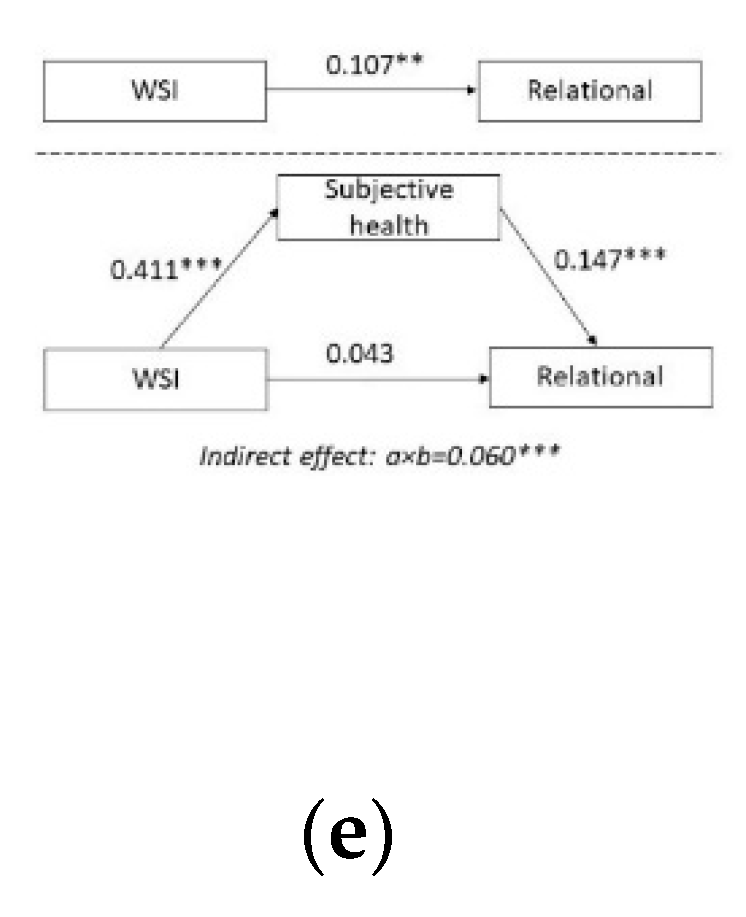
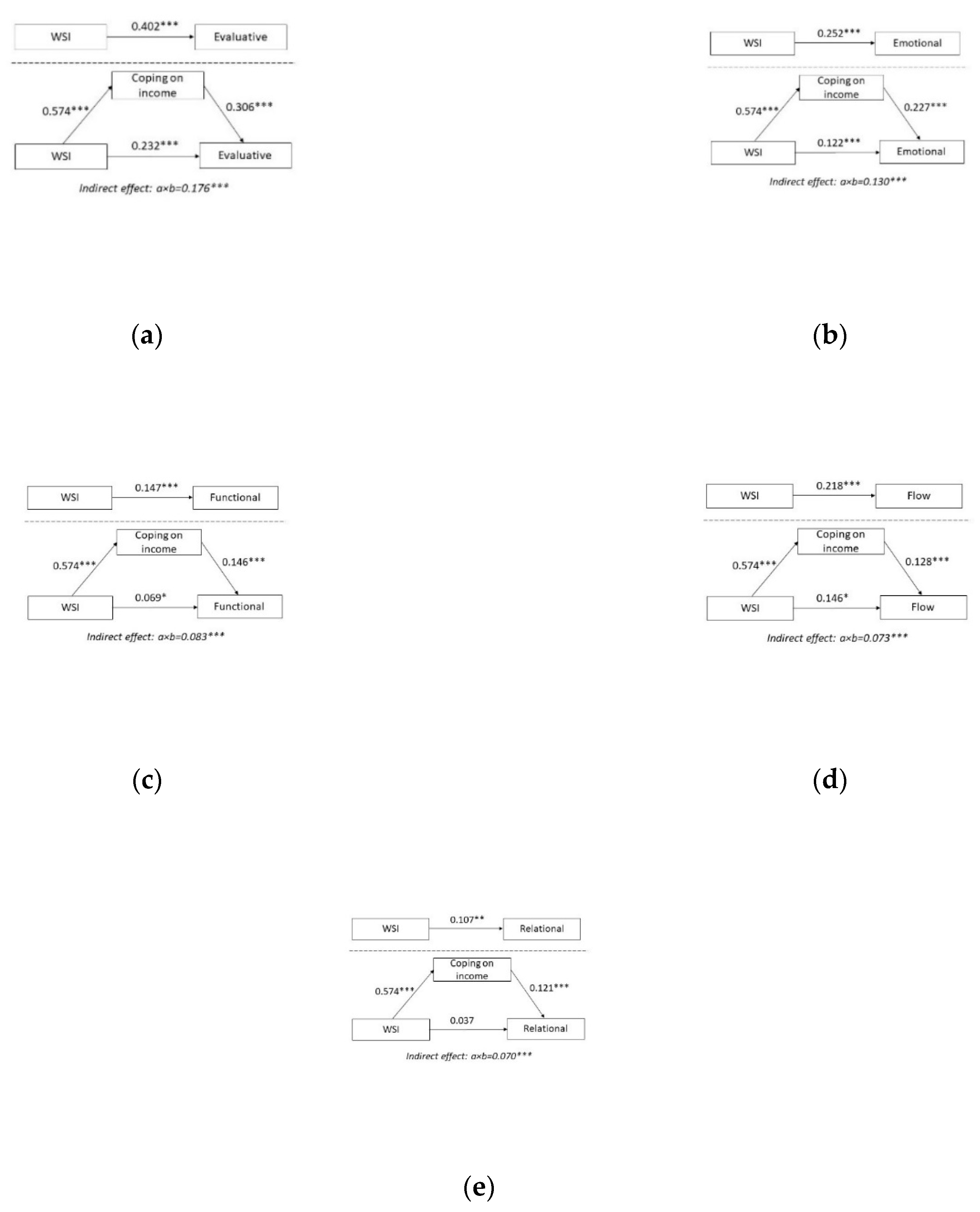
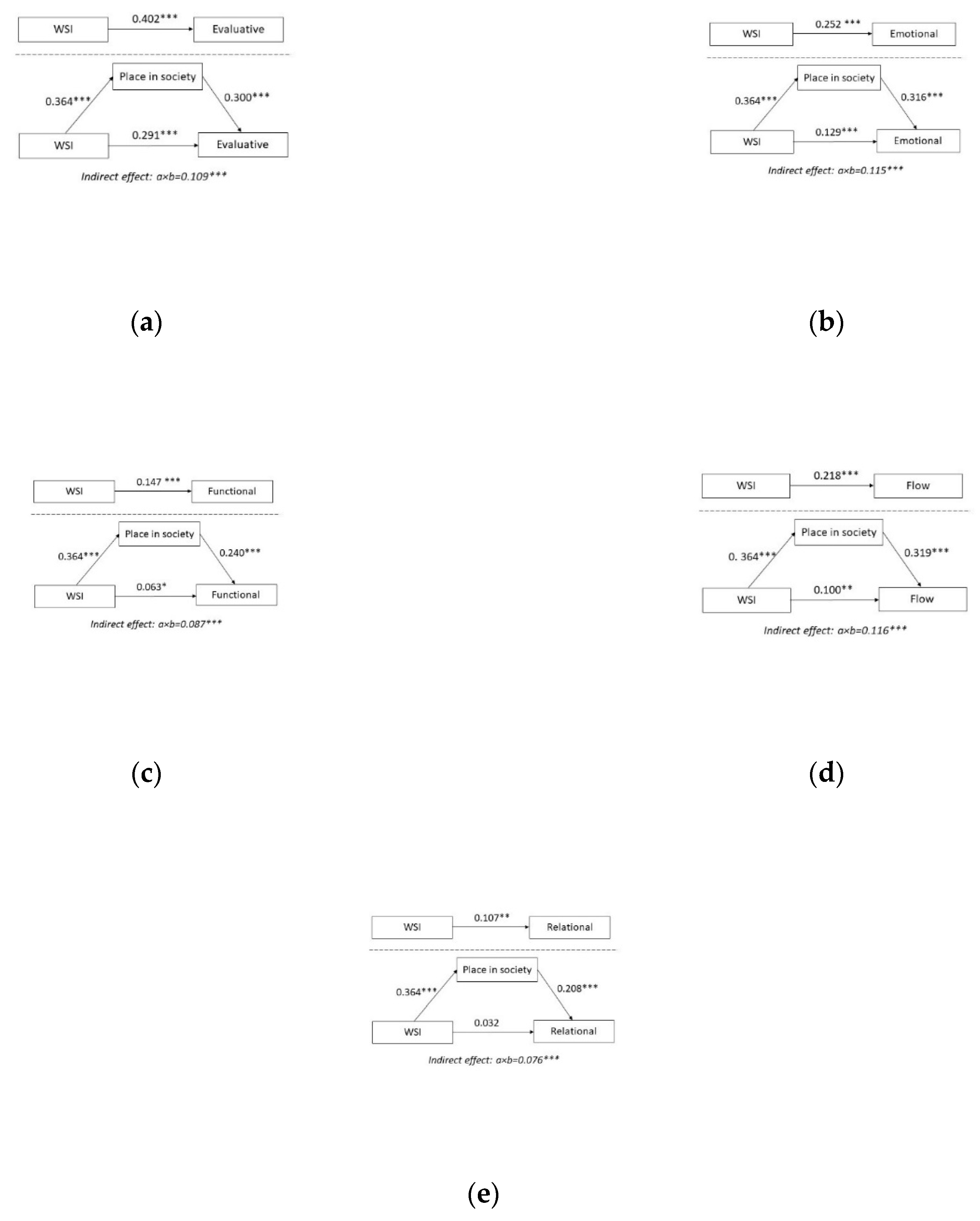
- Mediating effects. An intervening variable is considered to be a significant mediator of welfare state effects (i.e., an indirect effect) if it is significantly associated both with WSI (path a in Figure 1) and with mental wellbeing (path b in Figure 1). If the indirect effect (a×b in Figure 1) is equal to zero, this indicates that the direct effect (c’ in Figure 1) equals the total effect (c). The magnitude of the mediation effect can be assessed by comparing coefficients of path c and c’ in Table 3.
3. Results
3.1. Descriptions
3.1.1. Participants
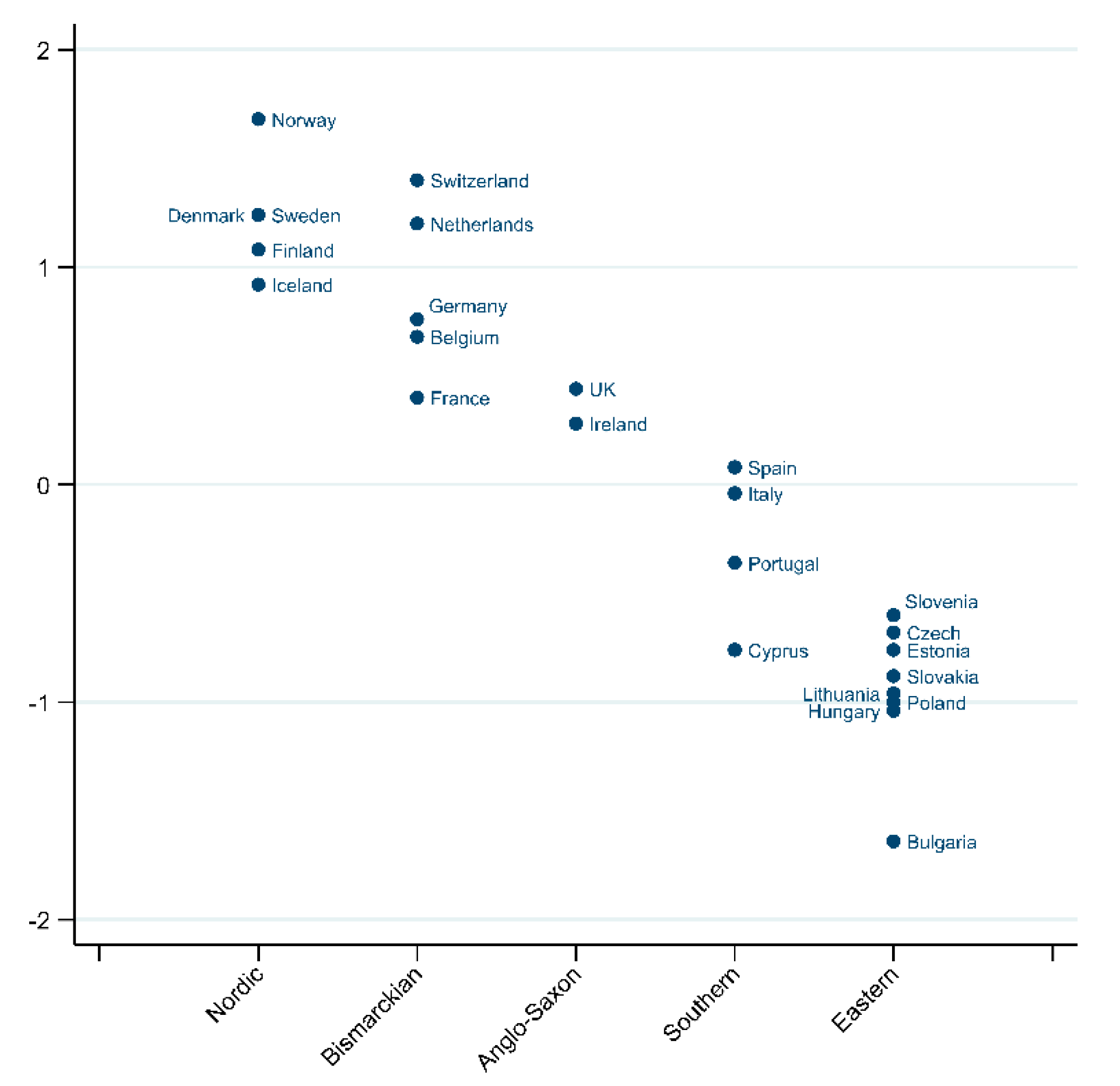
3.1.2. Welfare State Variable
3.2. Intervening Variables
3.3. Mental Wellbeing Variables
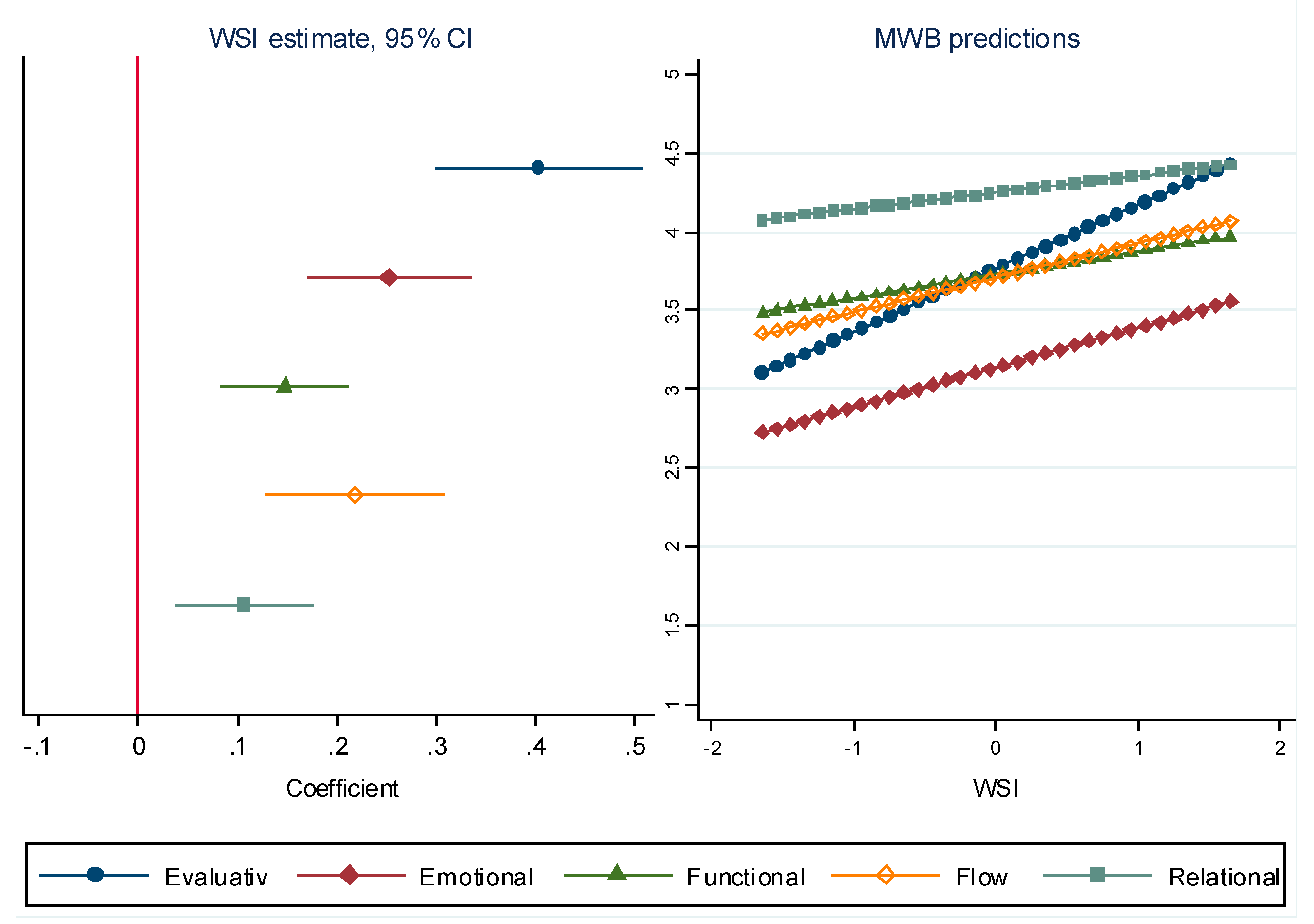
3.3.1. Step 1
3.3.2. Step 2
4. Discussion
4.1. Subjective General Health and Mental Wellbeing
4.2. Coping with Income and Mental Wellbeing
4.3. Place in Society and Mental Wellbeing
4.4. Protective Factors for Mental Wellbeing in Oldest Old Age; Some Policy Considerations
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Evaluative | Emotional | Functional | Flow | Relational | |
|---|---|---|---|---|---|
| How satisfied with life | X | ||||
| How happy are you | X | ||||
| Enjoyed life | X | ||||
| Were happy | X | ||||
| Felt calm and peaceful | X | ||||
| Had lot of energy | X | ||||
| Free to decide how to live my life | X | ||||
| Feel accomplishment | X | ||||
| What I do is valuable and worthwhile | X | ||||
| There are lots of things I am good at | X | ||||
| Feel very positive about myself | X | ||||
| Always optimistic about my future | X | ||||
| Interested | X | ||||
| Absorbed | X | ||||
| Enthusiastic | X | ||||
| Provide help and support | X | ||||
| Feel people treat you with respect | X | ||||
| Feel appreciated | X | ||||
| Receive help and support | X |
| MWIA Protective Factor | Intervening Variable |
|---|---|
| Enhancing control | Subjective general health |
| Coping with income | |
| Hampered in daily life | |
| Increasing resilience and community assets | Appreciate surroundings |
| Trust in people | |
| Facilitating participation | Voted |
| Voluntary work | |
| Social activities | |
| Promoting inclusion | Place in society |
| Learn new things | |
| Chance to show capabilities |
| Variable | Description |
|---|---|
| GDP per capita | Gross Domestic Product per capita in PPS, 2012, Index (EU28 = 100), Eurostat |
| Health/GDP + Social/GDP | Health expenditure as % of GDP, the World Bank DataBank, plus Social protection expenditure as % of GDP, 2012, Eurostat |
| Gender empowerment measure | Human Development Report 2009, United Nations (compiled by the ESS Multilevel Data Repository) |
| Life expectancy at 65 | Life expectancy in absolute value at 65 (average for male and female), 2012, Eurostat |
| Duration working life | Duration of working life, 2012, Eurostat |
| GINI | Gini coefficient of equivalised disposable income (scale from 0 to 100), EU-SILC survey, 2012, Eurostat |
| Individualism | Individualism versus Collectivism Index, Hofstede, G. (1980). Culture’s consequences: International differences in work-related values. London: Sage Publications, https://www.hofstede-insights.com/product/compare-countries/. Description: The high side of this dimension, called Individualism, can be defined as a preference for a loosely-knit social framework in which individuals are expected to take care of only themselves and their immediate families. Its opposite, Collectivism, represents a preference for a tightly-knit framework in society in which individuals can expect their relatives or members of a particular in-group to look after them in exchange for unquestioning loyalty. A society’s position on this dimension is reflected in whether people’s self-image is defined in terms of “I” or “we.” |
| Trust | Average rating of trust by domain (Trust police, Trust legal system, Trust political system, Trust others), both sexes, all educational attainment levels, 16 years or over- (rating 0–10), EU-SILC survey, 2013, Eurostat, http://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=ilc_pw03 |
Appendix B. Appendix Figures: Mediation Diagrams for Intervening Variables




References
- Andersen-Ranberg, K.; Petersen, I.; Robine, J.-M.; Christensen, K. Who Are the Oldest-Old? In Health, Ageing and Retirement in Europe: First Results from the Survey of Health, Ageing and Retirement i Europe; Börsch-Supan, A., Brugiavini, A., Jürges, H., Mackenbach, J., Siegrist, J., Weber, G., Eds.; Mannheim Research Institute for the Economics of Aging: Mannheim, Germany, 2005; pp. 35–40. [Google Scholar]
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Prospects 2019: Data Booket; ST/ESA/SER.A/424. Available online: https://population.un.org/wpp/publications/ (accessed on 31 March 2022).
- Beard, J.R.; Officer, A.; de Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.-P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; (Geeske) Peeters, G.M.E.E.; Mahanani, W.R.; et al. The World Report on Ageing and Health: A Policy Framework for Healthy Ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef]
- Huppert, F.A. Psychological Well-being: Evidence Regarding Its Causes and Consequences. Appl. Psychol. Health Well-Being 2009, 1, 137–164. [Google Scholar] [CrossRef]
- Chida, Y.; Steptoe, A. Positive Psychological Well-Being and Mortality: A Quantitative Review of Prospective Observational Studies. Psychosom. Med. 2008, 70, 741–756. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P. Investing in Health to Create a Third Demographic Dividend. Gerontologist 2016, 56 (Suppl. S2), S167–S177. [Google Scholar] [CrossRef] [PubMed]
- Knapp, M.; McDaid, D.; Parsonage, M. Mental Health Promotion and Mental Illness Prevention: The Economic Case. Available online: http://www.pssru.ac.uk/ (accessed on 21 June 2021).
- Schneider, S.M. Income Inequality and Subjective Wellbeing: Trends, Challenges, and Research Directions. J. Happiness Stud. Interdiscip. Forum Subj. Well-Being 2016, 17, 1719–1739. [Google Scholar] [CrossRef]
- Kalseth, J.; Cresswell-Smith, J.; Forsman, A.K.; Miret, M. Exploring the Association between Welfare State and Mental Wellbeing in Europe: Is There an Age Gradient? 2022, unpublished.
- Linton, M.-J.; Dieppe, P.; Medina-Lara, A. Review of 99 Self-Report Measures for Assessing Well-Being in Adults: Exploring Dimensions of Well-Being and Developments over Time. BMJ Open 2016, 6, e010641. [Google Scholar] [CrossRef] [PubMed]
- Diener, E. Subjective Well-Being. Psychol. Bull. 1984, 95, 542–575. [Google Scholar] [CrossRef] [PubMed]
- Diener, E. Guidelines for National Indicators of Subjective Well-Being and Ill-Being. J. Happiness Stud. 2006, 7, 397–404. [Google Scholar] [CrossRef]
- Dolan, P.; Metcalfe, R. Measuring Subjective Wellbeing: Recommendations on Measures for Use by National Governments. J. Soc. Policy 2012, 41, 409–427. [Google Scholar] [CrossRef]
- Kahneman, D.; Diener, E.; Schwarz, N. (Eds.) Well-Being: The Foundations of Hedonic Psychology; Russell Sage Foundation: New York, NY, USA, 1999. [Google Scholar]
- Ryff, C.D.; Singer, B.H. Know Thyself and Become What You Are: A Eudaimonic Approach to Psychological Well-Being. J. Happiness Stud. 2008, 9, 13–39. [Google Scholar] [CrossRef]
- Keyes, C.L.M. The Mental Health Continuum: From Languishing to Flourishing in Life. J. Health Soc. Behav. 2002, 43, 207–222. [Google Scholar] [CrossRef] [PubMed]
- Keyes, C.L.M. Promoting and Protecting Mental Health as Flourishing: A Complementary Strategy for Improving National Mental Health. Am. Psychol. 2007, 62, 95–108. [Google Scholar] [CrossRef]
- Seligman, M.E.P. Flourish: A Visionary New Understanding of Happiness and Well-Being; Free Press: New York, NY, USA, 2011. [Google Scholar]
- Cresswell-Smith, J.; Amaddeo, F.; Donisi, V.; Forsman, A.K.; Kalseth, J.; Martin-Maria, N.; Miret, M.; Walhbeck, K. Determinants of Multidimensional Mental Wellbeing in the Oldest Old: A Rapid Review. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Lara, E.; Martín-María, N.; Forsman, A.K.; Cresswell-Smith, J.; Donisi, V.; Ådnanes, M.; Kaasbøll, J.; Melby, L.; Nordmyr, J.; Nyholm, L.; et al. Understanding the Multi-Dimensional Mental Well-Being in Late Life: Evidence from the Perspective of the Oldest Old Population. J. Happiness Stud. 2020, 21, 465–484. [Google Scholar] [CrossRef]
- Steptoe, A.; Deaton, A.; Stone, A.A. Psychological Wellbeing, Health and Ageing. Lancet 2015, 385, 640–648. [Google Scholar] [CrossRef]
- Kieny, C.; Flores, G.; Ingenhaag, M.; Maurer, J. Healthy, Wealthy, Wise, and Happy? Assessing Age Differences in Evaluative and Emotional Well-Being Among Mature Adults from Five Low- and Middle-Income Countries. Soc. Indic. Res. 2022, 1019–1050. [Google Scholar] [CrossRef]
- Diener, E.; Diener, M.; Diener, C. Factors Predicting the Subjective Well-Being of Nations. J. Pers. Soc. Psychol. 1995, 69, 851–864. [Google Scholar] [CrossRef]
- Ejrnæs, A.; Greve, B. Your Position in Society Matters for How Happy You Are. Int. J. Soc. Welf. 2017, 26, 206–217. [Google Scholar] [CrossRef]
- Eikemo, T.A.; Bambra, C.; Joyce, K.; Dahl, E. Welfare State Regimes and Income-Related Health Inequalities: A Comparison of 23 European Countries. Eur. J. Public Health 2008, 18, 593–599. [Google Scholar] [CrossRef]
- Huppert, F.A.; So, T.T.C. Flourishing Across Europe: Application of a New Conceptual Framework for Defining Well-Being. Soc. Indic. Res. 2013, 110, 837–861. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.; Balfour, R.; Bell, R.; Marmot, M. Social Determinants of Mental Health. Int. Rev. Psychiatry 2014, 26, 392–407. [Google Scholar] [CrossRef] [PubMed]
- Cooke, A.; Friedli, L.; Coggins, T.; Edmonds, N.; Michaelson, J.; O’Hara, K.; Snowden, L.; Stansfield, J.; Steuer, N.; Scott-Samuel, A. Mental Well-being Impact Assessment, 3rd ed.; National MWIA Collaborative: London, UK, 2011. [Google Scholar]
- Miret, M.; Cabello, M.; Marchena, C.; Mellor-Marsá, B.; Caballero, F.F.; Obradors-Tarragó, C.; Haro, J.M.; Ayuso-Mateos, J.L. The State of the Art on European Well-Being Research within the Area of Mental Health. Int. J. Clin. Health Psychol. 2015, 15, 171–179. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Forsman, A.K.; Stengård, E.; Wahlbeck, K. Enhancing Mental Health and Mental Wellbeing in Older People. In nterventions and Policies to Enhance Well-being; Huppert, F.A., Cooper, C.L., Eds.; WileyBlackwell: Oxford, UK, 2014; pp. 331–354. [Google Scholar]
- European Social Survey Round 6 Data. Data File Edition 2.4. NSD—Norwegian Centre for Research Data, Norway—Data Archive and Distributor of ESS Data for ESS ERIC. 2012. Available online: https://www.europeansocialsurvey.org/data/conditions_of_use.html (accessed on 4 April 2022).
- Brown, T.A. Confirmatory Factor Analysis for Applied Research, 2nd ed.; The Guilford Press: New York, NY, USA, 2015. [Google Scholar]
- Donisi, V.; Tedeschi, F.; Gonzalez-Caballero, J.L.; Cresswell-Smith, J.; Lara, E.; Miret, M.; Forsman, A.K.; Wahlbeck, K.; Amaddeo, F.; Kalseth, J. Is Mental Well-Being in the Oldest Old Different from That in Younger Age Groups? Exploring the Mental Well-Being of the Oldest-Old Population in Europe. J. Happiness Stud. 2021, 22, 1693–1717. [Google Scholar] [CrossRef]
- Esping-Andersen, G. 4 The Three Political Economies of the Welfare State. Int. J. Sociol. 1990, 20, 92–123. [Google Scholar] [CrossRef]
- Barnish, M.; Tørnes, M.; Nelson-Horne, B. How Much Evidence Is There That Political Factors Are Related to Population Health Outcomes? An Internationally Comparative Systematic Review. BMJ Open 2018, 8, e020886. [Google Scholar] [CrossRef] [PubMed]
- Deeming, C.; Hayes, D. Worlds of Welfare Capitalism and Wellbeing: A Multilevel Analysis. J. Soc. Policy 2012, 41, 811–829. [Google Scholar] [CrossRef]
- Ebbinghaus, B.; Whiteside, N. Shifting Responsibilities in Western European Pension Systems: What Future for Social Models? Glob. Soc. Policy 2012, 12, 266–282. [Google Scholar] [CrossRef]
- Jorm, A.F.; Ryan, S.M. Cross-National and Historical Differences in Subjective Well-Being. Int. J. Epidemiol. 2014, 43, 330–340. [Google Scholar] [CrossRef] [PubMed]
- Shalev, M. Limits and Alternatives to Multiple Regression in Comparative Research. In Capitalisms Compared; Mjøset, L., Clausen, T.H., Eds.; Comparative Social Research; Emerald Group Publishing Limited: Bentley, UK, 2007; Volume 24, pp. 261–308. [Google Scholar] [CrossRef]
- Preacher, K.J.; Zyphur, M.J.; Zhang, Z. A General Multilevel SEM Framework for Assessing Multilevel Mediation. Psychol. Methods 2010, 15, 209–233. [Google Scholar] [CrossRef] [PubMed]
- Jaul, E.; Barron, J. Age-Related Diseases and Clinical and Public Health Implications for the 85 Years Old and Over Population. Front. Public Health 2017, 5, 335. [Google Scholar] [CrossRef] [PubMed]
- Högberg, B.; Strandh, M.; Baranowska-Rataj, A.; Sevä, I.J. Ageing, Health Inequalities and the Welfare State: A Multilevel Analysis. J. Eur. Soc. Policy 2018, 28, 311–325. [Google Scholar] [CrossRef]
- Moreno-Agostino, D.; Wu, Y.-T.; Daskalopoulou, C.; Hasan, M.T.; Huisman, M.; Prina, M. Global Trends in the Prevalence and Incidence of Depression:A Systematic Review and Meta-Analysis. J. Affect. Disord. 2021, 281, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Araujo, L.; Ribeiro, O.; Paúl, C. Hedonic and Eudaimonic Well-Being in Old Age through Positive Psychology Studies: A Scoping Review. An. Psicol. 2017, 33, 568–577. [Google Scholar] [CrossRef]
- Nordmyr, J.; Creswell-Smith, J.; Donisi, V.; Lara, E.; Martín-María, N.; Nyholm, L.; Forsman, A.K. Mental Well-Being among the Oldest Old: Revisiting the Model of Healthy Ageing in a Finnish Context. Int. J. Qual. Stud. Health Well-Being 2020, 15, 1734276. [Google Scholar] [CrossRef] [PubMed]
- Jarosz, E. What Makes Life Enjoyable at an Older Age? Experiential Wellbeing, Daily Activities, and Satisfaction with Life in General. Aging Ment. Health 2021, 1–11. [Google Scholar] [CrossRef]
- Nyqvist, F.; Victor, C.R.; Forsman, A.K.; Cattan, M. The Association between Social Capital and Loneliness in Different Age Groups: A Population-Based Study in Western Finland. BMC Public Health 2016, 16, 542. [Google Scholar] [CrossRef] [PubMed]
- Dykstra, P.A. Older Adult Loneliness: Myths and Realities. Eur. J. Ageing 2009, 6, 91. [Google Scholar] [CrossRef]
- Litwin, H. Social networks and well being in socio-geographical context: A comparison of older people in mediterranean and non-mediterranean european countries. Gerontologist 2009, 49, 488. [Google Scholar]
- Kahneman, D.; Deaton, A. High Income Improves Evaluation of Life but Not Emotional Well-Being. Proc. Natl. Acad. Sci. USA 2010, 107, 16489–16493. [Google Scholar] [CrossRef] [PubMed]
- Pani-Harreman, K.E.; Bours, G.J.J.W.; Zander, I.; Kempen, G.I.J.M.; van Duren, J.M.A. Definitions, Key Themes and Aspects of ‘Ageing in Place’: A Scoping Review. Ageing Soc. 2021, 41, 2026–2059. [Google Scholar] [CrossRef]
- Khalaila, R.; Vitman-Schorr, A. Internet Use, Social Networks, Loneliness, and Quality of Life among Adults Aged 50 and Older: Mediating and Moderating Effects. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2018, 27, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Iecovich, E. The Impact of Organizational Qualities of Old Age Homes in Israel on the Subjective Well-Being of Female Residents. J. Soc. Work Long-Term Care 2002, 1, 37–53. [Google Scholar] [CrossRef]
- Harrefors, C.; Sävenstedt, S.; Axelsson, K. Elderly People’s Perceptions of How They Want to Be Cared for: An Interview Study with Healthy Elderly Couples in Northern Sweden. Scand. J. Caring Sci. 2009, 23, 353–360. [Google Scholar] [CrossRef]
- Moilanen, T.; Kangasniemi, M.; Papinaho, O.; Mynttinen, M.; Siipi, H.; Suominen, S.; Suhonen, R. Older People’s Perceived Autonomy in Residential Care: An Integrative Review. Nurs. Ethics 2021, 28, 414–434. [Google Scholar] [CrossRef]
- Costa-Font, J. Housing-Related Well-Being in Older People: The Impact of Environmental and Financial Influences. Urban Stud. 2013, 50, 657–673. [Google Scholar] [CrossRef]
- Kaplan, G.A.; Shema, S.J.; Leite, C.M.A. Socioeconomic Determinants of Psychological Well-Being: The Role of Income, Income Change, and Income Sources during the Course of 29 Years. Ann. Epidemiol. 2008, 18, 531–537. [Google Scholar] [CrossRef]
- Böcker, L.; van Amen, P.; Helbich, M. Elderly Travel Frequencies and Transport Mode Choices in Greater Rotterdam, the Netherlands. Transportation 2017, 44, 831–852. [Google Scholar] [CrossRef]
- Orellana, K.; Manthorpe, J.; Tinker, A. Day Centres for Older People—Attender Characteristics, Access Routes and Outcomes of Regular Attendance: Findings of Exploratory Mixed Methods Case Study Research. BMC Geriatr. 2020, 20, 158. [Google Scholar] [CrossRef]
- Rivera-Torres, S.; Mpofu, E.; Jean Keller, M.; Ingman, S. Older Adults’ Mental Health Through Leisure Activities During COVID-19: A Scoping Review. Gerontol. Geriatr. Med. 2021, 7, 23337214211036776. [Google Scholar] [CrossRef]
- Lowenstein, A.; Katz, R.; Gur-Yaish, N. Reciprocity in Parent-Child Exchange and Life Satisfaction among the Elderly: A Cross-National Perspective. J. Soc. Issues 2007, 63, 865–883. [Google Scholar] [CrossRef]
- Schneider, S.M. Why Income Inequality Is Dissatisfying—Perceptions of Social Status and the Inequality-Satisfaction Link in Europe. Eur. Sociol. Rev. 2019, 35, 409–430. [Google Scholar] [CrossRef]
- Hoebel, J.; Lampert, T. Subjective Social Status and Health: Multidisciplinary Explanations and Methodological Challenges. J. Health Psychol. 2020, 25, 173–185. [Google Scholar] [CrossRef] [PubMed]
- Präg, P.; Mills, M.C.; Wittek, R. Subjective Socioeconomic Status and Health in Cross-National Comparison. Soc. Sci. Med. 2016, 149, 84–92. [Google Scholar] [CrossRef]
- Demakakos, P.; Nazroo, J.; Breeze, E.; Marmot, M. Socioeconomic Status and Health: The Role of Subjective Social Status. Soc. Sci. Med. 2008, 67, 330–340. [Google Scholar] [CrossRef]
- Hadjar, A.; Samuel, R. Does Upward Social Mobility Increase Life Satisfaction? A Longitudinal Analysis Using British and Swiss Panel Data. Res. Soc. Stratif. Mobil. 2015, 39, 48–58. [Google Scholar] [CrossRef]
- Navarro-Carrillo, G.; Alonso-Ferres, M.; Moya, M.; Valor-Segura, I. Socioeconomic Status and Psychological Well-Being: Revisiting the Role of Subjective Socioeconomic Status. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef]
- Read, S.; Grundy, E.; Foverskov, E. Socio-Economic Position and Subjective Health and Well-Being among Older People in Europe: A Systematic Narrative Review. Aging Ment. Health 2016, 20, 529–542. [Google Scholar] [CrossRef]
- Clench-Aas, J.; Holte, A. The Financial Crisis in Europe: Impact on Satisfaction with Life. Scand. J. Public Health 2017, 45 (Suppl. S18), 30–40. [Google Scholar] [CrossRef]
- Vauclair, C.-M.; Marques, S.; Lima, M.L.; Bratt, C.; Swift, H.J.; Abrams, D. Subjective Social Status of Older People across Countries: The Role of Modernization and Employment. J. Gerontol. B Psychol. Sci. Soc. Sci. 2015, 70, 650–660. [Google Scholar] [CrossRef]
- Chang, E.-S.; Kannoth, S.; Levy, S.; Wang, S.-Y.; Lee, J.E.; Levy, B.R. Global Reach of Ageism on Older Persons’ Health: A Systematic Review. PLoS ONE 2020, 15, e0220857. [Google Scholar] [CrossRef] [PubMed]
- Marques, S.; Mariano, J.; Mendonça, J.; De Tavernier, W.; Hess, M.; Naegele, L.; Peixeiro, F.; Martins, D. Determinants of Ageism against Older Adults: A Systematic Review. Int. J. Environ. Res. Public. Health 2020, 17, 2560. [Google Scholar] [CrossRef] [PubMed]
- Niedzwiedz, C.L.; Richardson, E.A.; Tunstall, H.; Shortt, N.K.; Mitchell, R.J.; Pearce, J.R. The Relationship between Wealth and Loneliness among Older People across Europe: Is Social Participation Protective? Prev. Med. 2016, 91, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Hank, K.; Erlinghagen, M. Dynamics of Volunteering in Older Europeans. Gerontologist 2010, 50, 170–178. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Age-Friendly Environments in Europe. A Handbook of Domains for Policy Action; Online, 2017; p. 160. Available online: https://www.euro.who.int/en/publications/abstracts/age-friendly-environments-in-europe.-a-handbook-of-domains-for-policy-action-2017 (accessed on 31 March 2022).
- Botezat, I.; Campion, J.; Garcia-Cubillana, P.; Guðmundsdóttir, D.G.; Halliday, W.; Henderson, N.; Holte, A.; Santos, M.J.H.; Japing, K.; Katschnig, H.; et al. Joint Action on Mental Health and Well-Being, Mental Health in All Policies. Situation Analysis and Recommendations for Action. 2017. Available online: https://arneholte.no/psykisk-helse/syv-prinsipper-og-tjueni-grep-for-et-psykisk-sunnere-norge/ (accessed on 15 October 2019).
- Hartfree, Y.F.; Hirsch, D.; Sutton, L. Minimum Income Standards and Older Pensioners’ Needs; Joseph Rowntree Foundation: York, UK, 2013. [Google Scholar]
- Marmot, M.; Allen, J.J. Social Determinants of Health Equity. Am. J. Public Health 2014, 104 (Suppl. S4), S517–S519. [Google Scholar] [CrossRef] [PubMed]
- Key, W.; Culliney, M. The Oldest Old and the Risk of Social Exclusion. Soc. Policy Soc. 2018, 17, 47–63. [Google Scholar] [CrossRef]
- Agler, R.; De Boeck, P. On the Interpretation and Use of Mediation: Multiple Perspectives on Mediation Analysis. Front. Psychol. 2017, 8, 1984. [Google Scholar] [CrossRef]



| Intervening Variable a | Mean | SD | CV b | WSI Effect c | N d |
|---|---|---|---|---|---|
| Subjective general health (1–5) | 3.1 | 0.93 | 0.31 | 0.411 *** | 2053 |
| Feeling about household’s income currently (1–4) | 2.9 | 0.90 | 0.31 | 0.574 *** | 2034 |
| Hampered in daily activities by illness/disability/infirmity/mental problems (1–3) | 2.2 | 0.75 | 0.34 | 0.114 * | 2055 |
| Take notice of and appreciate your surroundings (0–10) | 7.2 | 2.22 | 0.31 | 0.155 ** | 1985 |
| Most people can be trusted or you cannot be too careful (0–10) | 5.0 | 2.64 | 0.53 | 0.336 *** | 2044 |
| Voted last national election (0–1) | 0.8 | 0.42 | 0.55 | 0.183 *** | 2048 |
| Involved in work for voluntary or charitable organisations, how often past 12 months (1–6) | 1.7 | 1.42 | 0.86 | 0.310 *** | 2048 |
| Take part in social activities compared to others of same age (1–5) | 2.5 | 1.10 | 0.45 | 0.241 *** | 1968 |
| Place in society (0–10) | 5.1 | 1.93 | 0.38 | 0.364 *** | 1935 |
| Learn new things in life (0–6) | 2.8 | 1.88 | 0.66 | 0.266 *** | 1996 |
| Little chance to show how capable I am (1–5) | 2.9 | 1.03 | 0.35 | 0.038 | 1951 |
| Evaluative | Emotional | Functional | Flow | Relational | |
|---|---|---|---|---|---|
| mean | 3.80 | 3.16 | 3.76 | 3.75 | 4.27 |
| SD | 0.86 | 0.92 | 0.63 | 0.89 | 0.63 |
| CV * | 0.23 | 0.29 | 0.17 | 0.24 | 0.15 |
| N ** | 2023 | 1969 | 1886 | 1928 | 1922 |
| Evaluative | Emotional | Functional | Flow | Relational | |
|---|---|---|---|---|---|
| Total effect of WSI (c) | 0.402 *** | 0.252 *** | 0.147 *** | 0.218 *** | 0.107 *** |
| Effect of WSI (c’) after control for: | |||||
| Subjective general health | 0.273 *** (0.000) | 0.092 *** (0.000) | 0.056 (0.000) | 0.095 * (0.000) | 0.043 (0.000) |
| Coping with income | 0.232 ***(0.000) | 0.122 *** (0.000) | 0.069 ** (0.000) | 0.146 *** (0.000) | 0.037 (0.000) |
| Hampered in daily life | 0.380 *** (0.013) | 0.219 *** (0.012) | 0.128 *** (0.013) | 0.193 *** (0.014) | 0.095 ** (0.017) |
| Appreciate surroundings | 0.350 *** (0.006) | 0.203 *** (0.006) | 0.110 *** (0.006) | 0.143 ** (0.005) | 0.060 *(0.006) |
| Trust in people | 0.353 *** (0.000) | 0.213 *** (0.000) | 0.133 *** (0.010) | 0.198 *** (0.015) | 0.079 *** (0.000) |
| Voted | 0.383 *** (0.001) | 0.231 *** (0.001) | 0.133 *** (0.001) | 0.198 *** (0.001) | 0.092 ** (0.002) |
| Voluntary work | 0.368 *** (0.000) | 0.211 *** (0.000) | 0.116 *** (0.000) | 0.181 *** (0.000) | 0.089 ** (0.001) |
| Social activities | 0.360 *** (0.000) | 0.186 *** (0.000) | 0.100 ** (0.000) | 0.161 *** (0.000) | 0.078 * (0.000) |
| Place in society | 0.291 *** (0.000) | 0.129 *** (0.000) | 0.063 * (0.000) | 0.100 ** (0.000) | 0.032 (0.000) |
| Learn new things | 0.348 *** (0.000) | 0.181 *** (0.000) | 0.095 ** (0.000) | 0.132 * (0.000) | 0.067 * (0.000) |
| Chance to show capabilities | 0.402 *** (0.435) | 0.236 *** (0.433) | 0.138 *** (0.435) | 0.199 *** (0. 434) | 0.103 ** (0.435) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cresswell-Smith, J.; Wahlbeck, K.; Kalseth, J. Life Conditions as Mediators of Welfare State Effect on Mental Wellbeing among Oldest Old in Europe. Int. J. Environ. Res. Public Health 2022, 19, 4363. https://doi.org/10.3390/ijerph19074363
Cresswell-Smith J, Wahlbeck K, Kalseth J. Life Conditions as Mediators of Welfare State Effect on Mental Wellbeing among Oldest Old in Europe. International Journal of Environmental Research and Public Health. 2022; 19(7):4363. https://doi.org/10.3390/ijerph19074363
Chicago/Turabian StyleCresswell-Smith, Johanna, Kristian Wahlbeck, and Jorid Kalseth. 2022. "Life Conditions as Mediators of Welfare State Effect on Mental Wellbeing among Oldest Old in Europe" International Journal of Environmental Research and Public Health 19, no. 7: 4363. https://doi.org/10.3390/ijerph19074363
APA StyleCresswell-Smith, J., Wahlbeck, K., & Kalseth, J. (2022). Life Conditions as Mediators of Welfare State Effect on Mental Wellbeing among Oldest Old in Europe. International Journal of Environmental Research and Public Health, 19(7), 4363. https://doi.org/10.3390/ijerph19074363