
Enhancing Parents’ Well-Being after Preterm Birth—A Qualitative Evaluation of the “Transition to Home” Model of Care

 , ,
, ,
Abstract
:1. Introduction
1.1. Models of Care to Provide Family Support
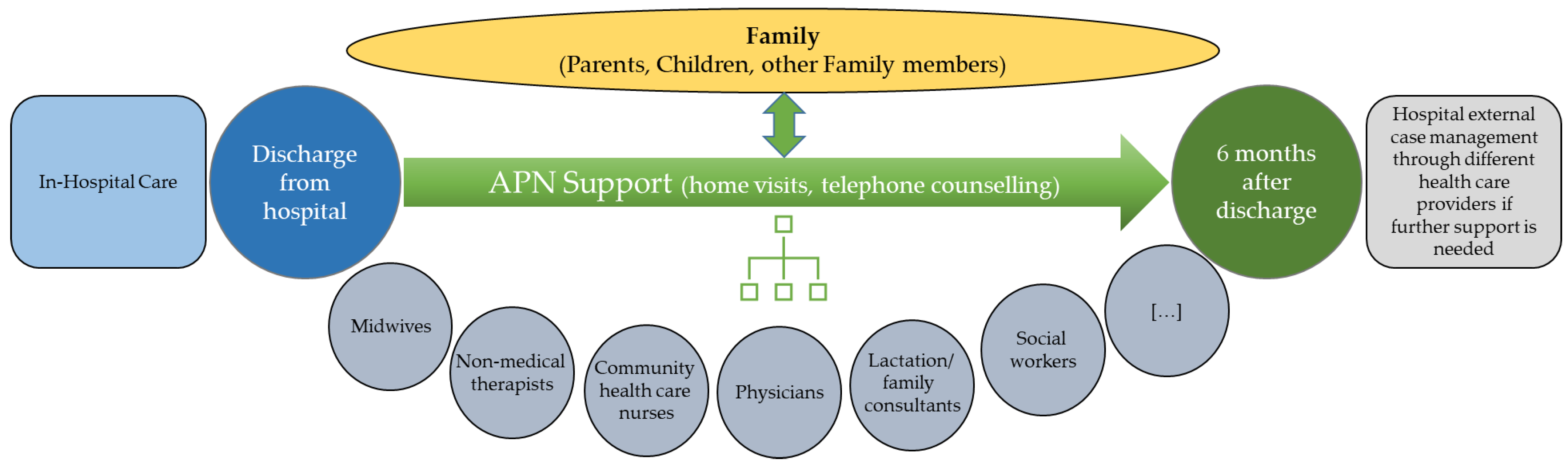
1.2. The “Transition to Home (TtH)” Model
1.3. Aims
2. Materials and Methods
2.1. Participants
2.2. Semi-Structured Interview Guide
2.3. Data Collection Procedures
2.4. Data Analysis
3. Results
3.1. Sample Characteristics
3.2. Findings
“In the beginning we didn’t really know, well, what do we need to do? What (support) can we actually ask for? […] It wasn’t fully comprehensible. We didn’t know in detail what “Transition to Home” meant for us.”(D10; 10:18)
3.2.1. TtH and the Relevance of Continuity of Care
“[…] it (the in-patient care) does not end all of a sudden […], it is a somewhat stepwise leaving the hospital. In my view this is very good.”(D7, 7:160)
“In my view you need the support especially after discharge, then, actually, you would need it 24 h/7 days. But pretty soon thereafter you don’t need it anymore.”(D64; 64:14)
“Without her (lactation consultant) I hadn’t managed the breastfeeding.”(D5; 5:22)
The Advanced Practice Nurse: The Bridge Home
“Well, surely, many issues could be recognized early on that otherwise had potentially caused problems.”(D2; 2:114)
“When she (the APN) visited us the first time, it was just the right moment. He (the child) had cried all night and didn’t drink. I was glad to know that she (the APN) was due to visit such that I could ask her whether this behaviour was normal or not […] she then checked him […] and gave me an all-clear […] this was such a relief.”(D4; 4:37)
“What was most important, in my view, was this contact person. The APN […] who we could contact […] she knew us and knew how things were…”(D11; 11:40)
Continuity of Care and Parents’ Unmet Expectations
“When I came to the NICU, the bed of my child had gone.”(D24; 24:68)
“I think what the experts don’t understand so much is the fact that the cultures are so very different.”(D3; 3:119)
“Well, this was a huge difference to the neonatal intensive care unit. At the NICU, we basically had to ask for permission if we wanted to do something, and now on the intermediate care unit, they assumed that we’d just do and only ask if we needed something.”(D20; 20:17)
3.2.2. Enhancement of Parents’ Autonomy and Self-Confidence
“[…] (it was a) triangle: work, hospital, going home to sleep and again work, hospital, home to sleep […] a tight timetable also without any time for us as a couple.”(D50; 50:31)
“She (the APN) always pointed-out options […] and left it to us to decide […] and whatever we went for, it was good. We felt very well supported.”(D20; 20:53)
Acquiring Knowledge
“We noticed that she (the APN) was very well prepared for the home visits. She got back to topics that we had mentioned during our last conversation, and she had answers. She really made an effort to impart knowledge. This was a huge additional value.”(D25; 25:46)
“The APN and this program helped us to see the difference in her (the child’s) development from the beginning until now. […] So, we really pay more attention to how things go.”(D39; 39:127)
“Body weight is a key factor, you want to know if she (the child) is gaining weight, is drinking enough, you feed her correctly […] in this aspect she (the APN) helped.”(D41; 41:185)
“Sometimes the consultations were not about fields in which she (the APN) was strong […] perhaps this was because of my questions, but, when you are at home, it is about the child at home, not so much about preterm birth.”(D4; 4:11)
Parental Emotional Support
“Most important is this encouragement, to know that you’re doing it right.”(D42; 42:63)
“Relaxing, taking time […] the music is supporting […] it calms down […] and it is also unconsciously knowing that nothing else will happen for the next 20 min.”(D50; 50:67)
“I saw the psychologist. She was very supportive such that I felt more confident and comfortable in my role as a mother and started to build trust in the relationship (to the child). I no longer felt anxious or guilty as at the beginning.”(D6; 6:82)
3.2.3. Perception of Interprofessional Collaboration
Perception of Health Care Professionals’ Roles and Competencies
“At the beginning, when the role (of the APN) wasn’t fully clear to me, I sometimes wondered why she was also present. There were already so many people.”(D26; 26:78)
“The APN and the midwife had arranged alternating visits. Thus, someone came to see us at home every week. This was very convenient.”(D8; 8:345)
The Impact of Different Forms of Communication
“…if they didn’t communicate such things (diagnostic findings). You can’t communicate nothing to a waiting family. Even if one doesn’t say anything, you realize their facial expressions and you know what’s up.”(D50; 50:89)
“They were always positive, even if something was going on, they always saw something positive. Not like the others, who then said, oh the child is ill, so ill.”(D16; 16:44)
The Impact of Interprofessional Roundtable Discussions
“I see it like this: you learn about the problem and then discuss together how to handle it”(D50; 50:69)
“There were so many people. At first we thought that we massively underestimated the situation. Does it need so many people to support us?”(D12; 12:50)
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huhtala, M.; Korja, R.; Lehtonen, L.; Haataja, L.; Lapinleimu, H.; Rautava, P. Associations between parental psychological well-being and socio-emotional development in 5-year-old preterm children. Early Hum. Dev. 2014, 90, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Haemmerli, N.S.; Lemola, S.; Holditch-Davis, D.; Cignacco, E. Comparative evaluation of parental stress experiences up to 2 to 3 years after preterm and term birth. Adv. Neonatal Care 2020, 20, 301–313. [Google Scholar] [CrossRef] [PubMed]
- Kantrowitz-Gordon, I.; Altman, M.R.; Vandermause, R. Prolonged distress of parents after early preterm birth. J. Obstet. Gynecol. Neonatal Nurs. 2016, 45, 196–209. [Google Scholar] [CrossRef] [PubMed]
- Treyvaud, K. Parent and family outcomes following very preterm or very low birth weight birth: A review. Semin. Fetal. Neonatal Med. 2014, 19, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Roque, A.T.F.; Lasiuk, G.C.; Radünz, V.; Hegadoren, K. Scoping review of the mental health of parents of infants in the nicu. J. Obstet. Gynecol. Neonatal Nurs. 2017, 46, 576–587. [Google Scholar] [CrossRef] [Green Version]
- Cheong, J.L.Y.; Burnett, A.C.; Treyvaud, K.; Spittle, A.J. Early environment and long-term outcomes of preterm infants. J. Neural Transm. 2020, 127, 1–8. [Google Scholar] [CrossRef]
- Pladys, P.; Zaoui, C.; Girard, L.; Mons, F.; Reynaud, A.; Casper, C.; The group for reflections on and evaluation of the neonatal environment of the French neonatal society. French neonatal society position paper stresses the importance of an early family-centred approach to discharging preterm infants from hospital. Acta. Paediatr. 2020, 109, 1302–1309. [Google Scholar] [CrossRef]
- Ding, X.; Zhu, L.; Zhang, R.; Wang, L.; Wang, T.-T.; Latour, J.M. Effects of family-centred care interventions on preterm infants and parents in neonatal intensive care units: A systematic review and meta-analysis of randomised controlled trials. Aust. Crit. Care 2019, 32, 63–75. [Google Scholar] [CrossRef]
- Roué, J.M.; Kuhn, P.; Maestro, M.L.; Maastrup, R.A.; Mitanchez, D.; Westrup, B.; Sizun, J. Eight principles for patient-centred and family-centred care for newborns in the neonatal intensive care unit. Arch. Dis. Child. -Fetal. Neonatal Ed. 2017, 102, F364–F368. [Google Scholar] [CrossRef]
- Reijneveld, S.A.; Hielkema, M.; Stewart, R.E.; de Winter, A.F. The added value of a family-centered approach to optimize infants’ social-emotional development: A quasi-experimental study. PLoS ONE 2017, 12, e0187750. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, K.; Robson, K.; Bracht, M.; Cruz, M.; Lui, K.; Alvaro, R.; da Silva, O.; Monterrosa, L.; Narvey, M.; Ng, E.; et al. Effectiveness of family integrated care in neonatal intensive care units on infant and parent outcomes: A multicentre, multinational, cluster-randomised controlled trial. Lancet Child Adolesc. Health 2018, 2, 245–254. [Google Scholar] [CrossRef]
- Franck, L.S.; Waddington, C.; O’Brien, K. Family integrated care for preterm infants. Crit. Care Nurs. Clin. N. Am. 2020, 32, 149–165. [Google Scholar] [CrossRef] [PubMed]
- Van Hus, J.W.P.; Jeukens-Visser, M.; Koldewijn, K.; Holman, R.; Kok, J.H.; Nollet, F.; Wassenaer-Leemhuis, A.G. Early intervention leads to long-term developmental improvements in very preterm infants, especially infants with bronchopulmonary dysplasia. Acta Paediatr. 2016, 105, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Baraldi, E.; Allodi, M.W.; Löwing, K.; Smedler, A.C.; Westrup, B.; Ådén, U. Stockholm preterm interaction-based intervention (spibi)-study protocol for an rct of a 12-month parallel-group post-discharge program for extremely preterm infants and their parents. BMC Pediatr. 2020, 20, 49. [Google Scholar] [CrossRef]
- Jeukens-Visser, M.; Koldewijn, K.; van Wassenaer-Leemhuis, A.G.; Flierman, M.; Nollet, F.; Wolf, M.J. Development and nationwide implementation of a postdischarge responsive parenting intervention program for very preterm born children: The top program. Infant Ment. Health J. 2021, 42, 423–437. [Google Scholar] [CrossRef]
- Newnham, C.A.; Milgrom, J.; Skouteris, H. Effectiveness of a modified mother-infant transaction program on outcomes for preterm infants from 3 to 24 months of age. Infant Behav. Dev. 2009, 32, 17–26. [Google Scholar] [CrossRef]
- Als, H.; Butler, S.; Kosta, S.; McAnulty, G. The assessment of preterm infants’ behavior (apib): Furthering the understanding and measurement of neurodevelopmental competence in preterm and full-term infants. Ment. Retard. Dev. Disabil. Res. Rev. 2005, 11, 94–102. [Google Scholar] [CrossRef]
- Treyvaud, K.; Spittle, A.; Anderson, P.J.; O’Brien, K. A multilayered approach is needed in the nicu to support parents after the preterm birth of their infant. Early Hum. Dev. 2019, 139, 104838. [Google Scholar] [CrossRef]
- Hynan, M.T.; Mounts, K.O.; Vanderbilt, D.L. Screening parents of high-risk infants for emotional distress: Rationale and recommendations. J. Perinatol. 2013, 33, 748–753. [Google Scholar] [CrossRef] [Green Version]
- Purdy, I.B.; Craig, J.W.; Zeanah, P. Nicu discharge planning and beyond: Recommendations for parent psychosocial support. J. Perinatol. 2015, 35, S24–S28. [Google Scholar] [CrossRef] [Green Version]
- Haemmerli, N.S.; von Gunten, G.; Khan, J.; Stoffel, L.; Humpl, T.; Cignacco, E. Interprofessional collaboration in a new model of transitional care for families with preterm infants—The health care professional’s perspective. J. Multidiscip. Health 2021, 14, 897–908. [Google Scholar] [CrossRef] [PubMed]
- Tracy, M.F.; O’Grady, E.T. Hamric and Hanson’s Advanced Practice Nursing: An Integrative Approach, 6th ed.; Elsevier: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Canadian Nurses Association. Advanced Practice Nursing. A Pan-Canadian Framework. Available online: https://hl-prod-ca-oc-download.s3-ca-central-1.amazonaws.com/CNA/2f975e7e-4a40-45ca-863c-5ebf0a138d5e/UploadedImages/documents/Advanced_Practice_Nursing_framework_EN.pdf (accessed on 30 January 2022).
- Bryant-Lukosius, D.; Spichiger, E.; Martin, J.; Stoll, H.; Kellerhals, S.D.; Fliedner, M.; Grossmann, F.; Henry, M.; Herrmann, L.; Koller, A.; et al. Framework for evaluating the impact of advanced practice nursing roles. J. Nurs. Scholarsh. 2016, 48, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Gysin, S.; Sottas, B.; Odermatt, M.; Essig, S. Advanced practice nurses’ and general practitioners’ first experiences with introducing the advanced practice nurse role to swiss primary care: A qualitative study. BMC Fam. Pract. 2019, 20, 163. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. To saturate or not to saturate? Questioning data saturation as a useful concept for thematic analysis and sample-size rationales. Qual. Res. Sport Exerc. Health 2021, 13, 201–216. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Lincoln, Y.S.; Guba, E.G. Naturalistic Inquiry; Sage Publications: Thousand Oaks, CA, USA, 1985. [Google Scholar]
- Wreesmann, W.-J.W.; Lorié, E.S.; van Veenendaal, N.R.; van Kempen, A.A.; Ket, J.C.; Labrie, N.H. The functions of adequate communication in the neonatal care unit: A systematic review and meta-synthesis of qualitative research. Patient Educ. Couns. 2021, 104, 1505–1517. [Google Scholar] [CrossRef]
- Baird, J.; Rehm, R.S.; Hinds, P.S.; Baggott, C.; Davies, B. Do you know my child? Continuity of nursing care in the pediatric intensive care unit. Nurs. Res. 2016, 65, 142–150. [Google Scholar] [CrossRef] [Green Version]
- Seppänen, A.-V.; Sauvegrain, P.; Draper, E.S.; Toome, L.; El Rafei, R.; Petrou, S.; Barros, H.; Zimmermann, L.J.I.; Cuttini, M.; Zeitlin, J. Parents’ ratings of post-discharge healthcare for their children born very preterm and their suggestions for improvement: A european cohort study. Pediatr. Res. 2021, 89, 1004–1012. [Google Scholar] [CrossRef]
- Enke, C.; Hausmann, A.O.; Miedaner, F.; Roth, B.; Woopen, C. Communicating with parents in neonatal intensive care units: The impact on parental stress. Patient Educ. Couns. 2017, 100, 710–719. [Google Scholar] [CrossRef]
- Lorié, E.S.; Wreesmann-jan, W.W.; van Veenendaal, N.R.; van Kempen, A.A.; Labrie, N.H. Parents’ needs and perceived gaps in communication with healthcare professionals in the neonatal (intensive) care unit: A qualitative interview study. Patient Educ. Couns. 2021, 104, 1518–1525. [Google Scholar] [CrossRef] [PubMed]
- Baraldi, E.; Allodi, M.W.; Smedler, A.C.; Westrup, B.; Löwing, K.; Ådén, U. Parents’ experiences of the first year at home with an infant born extremely preterm with and without post-discharge intervention: Ambivalence, loneliness, and relationship impact. Int. J. Environ. Res. Public Health 2020, 17, 9326. [Google Scholar] [CrossRef] [PubMed]
- Jerntorp, S.H.; Sivberg, B.; Lundqvist, P. Fathers’ lived experiences of caring for their preterm infant at the neonatal unit and in neonatal home care after the introduction of a parental support programme: A phenomenological study. Scand. J. Caring Sci. 2021, 35, 1143–1151. [Google Scholar] [CrossRef] [PubMed]
- Pace, C.C.; Spittle, A.J.; Molesworth, C.M.L.; Lee, K.J.; Northam, E.A.; Cheong, J.L.; Davis, P.G.; Doyle, L.W.; Treyvaud, K.; Anderson, P.J. Evolution of depression and anxiety symptoms in parents of very preterm infants during the newborn period. JAMA Pediatr. 2016, 170, 863–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hynan, M.T.; Steinberg, Z.; Baker, L.; Cicco, R.; Geller, P.A.; Lassen, S.; Milford, C.; Mounts, K.O.; Patterson, C.; Saxton, S.; et al. Recommendations for mental health professionals in the nicu. J. Perinatol. 2015, 35, S14–S18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bieleninik, L.; Ghetti, C.; Gold, C. Music therapy for preterm infants and their parents: A meta-analysis. Pediatrics 2016, 138, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kehl, S.M.; La Marca-Ghaemmaghami, P.; Haller, M.; Pichler-Stachl, E.; Bucher, H.U.; Bassler, D.; Haslbeck, F.B. Creative music therapy with premature infants and their parents: A mixed-method pilot study on parents’anxiety, stress and depressive symptoms and parent-infant attachment. Int. J. Environ. Res. Public Health 2020, 18, 265. [Google Scholar] [CrossRef]
- Jouybari, L.; Abbariki, E.; Jebeli, M.; Mehravar, F.; Asadi, L.; Akbari, N.; Sanagoo, A.; Moradi, Z. Comparison of the effect of narrative writing and art therapy on maternal stress in neonatal intensive care settings. J. Matern. Neonatal Med. 2020, 33, 664–670. [Google Scholar] [CrossRef]
- Howland, L.C.; Jallo, N.; Connelly, C.D.; Pickler, R.H. Feasibility of a relaxation guided imagery intervention to reduce maternal stress in the nicu. J. Obstet. Gynecol. Neonatal Nurs. 2017, 46, 532–543. [Google Scholar] [CrossRef]
- Afand, N.; Keshavarz, M.; Fatemi, N.S.; Montazeri, A. Effects of infant massage on state anxiety in mothers of preterm infants prior to hospital discharge. J. Clin. Nurs. 2017, 26, 1887–1892. [Google Scholar] [CrossRef]
- Schussele Filliettaz, S.S.; Berchtold, P.; Kohler, D.; Peytremann-Bridevaux, I. Integrated care in switzerland: Results from the first nationwide survey. Health Policy 2018, 122, 568–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desomer, A.; Van den Heede, K.; Triemstra, M.; Paget, J.; De Boer, D.; Kohn, L.; Cleemput, I. Use of Patient-Reported Outcome and Experience Measures in Patient Care and Policy; KCE Report 303; KCE: Brussels, Belgium, 2018. [Google Scholar]
- Bauer, M.S.; Kirchner, J. Implementation science: What is it and why should i care? Psychiatry Res. 2020, 283, 112376. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Components of Model | Description |
|---|---|
| Advanced Practice Nurse (APN) support | All team members contribute to a comprehensive plan for individual discharges, hold consultations, coordinate and collaborate closely with different HCPs so that information flows freely, and they participate in regular interprofessional exchanges. The APN takes a family-centered approach in assessing the needs of the families and in making shared decisions. The APN regularly visits, consults with and educates parents and acts as a continuous partner. After discharge, the APN offers three systematic follow-up calls, telephone support when needed and up to nine follow-up home visits to assess the physical health of infants and parents and the mental health of parents, with a view of evaluating interventions and adapting the care as the family’s needs evolve. |
| Psychological support | A psychologist provides psychological support to all families, comprising assessment and at least three follow-up consultations before the infant is discharged. The goal is to re-establish emotional stability, improve parents’ ability to cope, prevent the parents and family from developing adaptive disorders and protect the infant from developmental disorders. |
| Lactation consultation | During hospitalization, the lactation consultant responds to the needs of the families, including fathers. The aim is to strengthen parent–child bonds and to show parents how to meet their child’s nutritional needs. |
| Physical therapy | The physical therapist provides treatment after an assessment. In a single consultation, the family learns how to handle their premature infant in everyday life, in a manner appropriate to the infant’s developmental stage. |
| Support by social worker | Social workers collaborate closely with the APN and are involved with every family. They help families cope with daily life after preterm birth and during and after hospitalization. |
| Music therapy | A music therapist offers music therapy during hospitalization to stabilize the child, support its development, reduce parents’ anxiety and enhance their self-efficacy. |
| Interprofessional roundtable discussion | Interprofessional roundtable discussions with involved HCPs and parents are held twice while the preterm infant is hospitalized and once three months after discharge. The meetings seek consensus on the optimal support for families in care. |
| Characteristic | Mothers N = 20 | Fathers N = 19 | Infants N = 22 |
|---|---|---|---|
| n (%) or median (IQ-range) or mean ± sd | n (%) or median (IQ-range) or mean ± sd | n (%) or median (IQ-range) or mean ± sd | |
| Age, years | 32.5 (31.0; 35.8) 33.3 ± 2.8 | 35.0 (31.0; 38.0) 36.5 ± 8.1 | |
| Nationality | |||
| Swiss | 16 (80%) | 16 (84%) | |
| German | 1 (5%) | 2 (11%) | |
| Macedonian | 1 (5%) | ||
| Italian | 1 (5%) | ||
| Other | 2 (10%) | ||
| Marital status | |||
| Married | 14 (70%) | ||
| Unmarried | 6 (30%) | ||
| Living in Switzerland since | |||
| Birth | 15 (75%) | 16 (84%) | |
| >20 years | 1 (5%) | 2 (11%) | |
| >5 years | 2 (10%) | ||
| >2 years | 1 (5%) | 1 (5%) | |
| <2 years | 1 (5%) | ||
| Highest education level | |||
| Primary and secondary school | 2 (10%) | ||
| Apprenticeship | 3 (15%) | 5 (26%) | |
| College of higher education | 6 (30%) | 1 (5%) | |
| University of applied science | 3 (15%) | 2 (11%) | |
| University | 6 (30%) | 9 (47%) | |
| Other | 2 (11%) | ||
| Employment status | |||
| Full-time | 5 (25%) | 11 (58%) | |
| Part-time | 11 (55%) | 5 (26%) | |
| Not employed | 4 (20%) | 3 (16%) | |
| Yearly family income | |||
| 40,000–60,000 Swiss francs | 1 (5%) | ||
| 60,000–80,000 Swiss francs | 3 (15%) | ||
| 80,000–100,000 Swiss francs | 5 (25%) | ||
| >100,000 Swiss francs | 11 (55%) | ||
| Method of delivery | |||
| Planned caesarean | 6 (30%) | ||
| Unplanned caesarean | 12 (60%) | ||
| Vaginal delivery | 2 (10%) | ||
| Multiple birth | 2 (10%) | ||
| Infant’s gender | |||
| Male | 11 (50%) | ||
| Female | 11 (50%) | ||
| Gestational age at birth, weeks | 28.0 (26.0; 32.8) 29.0 ± 3.3 | ||
| Birth weight, g | 1097.5 (706.3; 1677.5) 1209.5 ± 548.3 | ||
| Birth length, cm | 40.0 (32.8; 43.5) 38.6 ± 5.8 | ||
| Length of hospital stay, days | 63.0 (28.3; 94.8) 71.7 ± 52.9 |
| Thematic Analysis of the Parent Interviews | |||
|---|---|---|---|
| Main theme | TtH and the relevance of continuity of care | Enhancement of parents’ autonomy and self-confidence | Perception of interprofessional collaboration |
| Sub-themes |
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schuetz Haemmerli, N.; Stoffel, L.; Schmitt, K.-U.; Khan, J.; Humpl, T.; Nelle, M.; Cignacco, E. Enhancing Parents’ Well-Being after Preterm Birth—A Qualitative Evaluation of the “Transition to Home” Model of Care. Int. J. Environ. Res. Public Health 2022, 19, 4309. https://doi.org/10.3390/ijerph19074309
Schuetz Haemmerli N, Stoffel L, Schmitt K-U, Khan J, Humpl T, Nelle M, Cignacco E. Enhancing Parents’ Well-Being after Preterm Birth—A Qualitative Evaluation of the “Transition to Home” Model of Care. International Journal of Environmental Research and Public Health. 2022; 19(7):4309. https://doi.org/10.3390/ijerph19074309
Chicago/Turabian StyleSchuetz Haemmerli, Natascha, Liliane Stoffel, Kai-Uwe Schmitt, Jeannine Khan, Tilman Humpl, Mathias Nelle, and Eva Cignacco. 2022. "Enhancing Parents’ Well-Being after Preterm Birth—A Qualitative Evaluation of the “Transition to Home” Model of Care" International Journal of Environmental Research and Public Health 19, no. 7: 4309. https://doi.org/10.3390/ijerph19074309
APA StyleSchuetz Haemmerli, N., Stoffel, L., Schmitt, K.-U., Khan, J., Humpl, T., Nelle, M., & Cignacco, E. (2022). Enhancing Parents’ Well-Being after Preterm Birth—A Qualitative Evaluation of the “Transition to Home” Model of Care. International Journal of Environmental Research and Public Health, 19(7), 4309. https://doi.org/10.3390/ijerph19074309