
Exploratory Study of Palliative Care Utilization and Medical Expense for Inpatients at the End-of-Life


Abstract
:1. Introduction
2. Materials and Methods
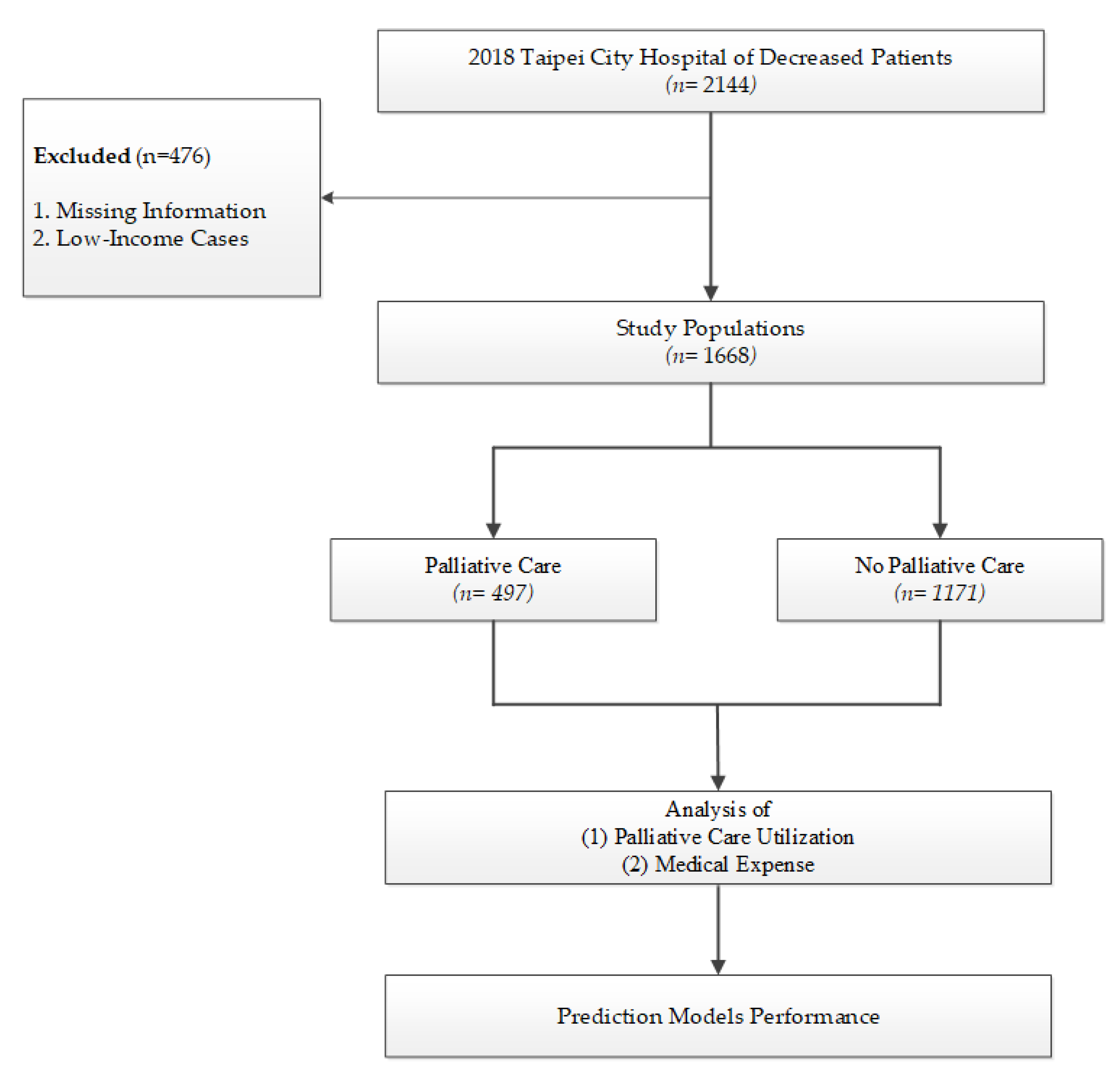
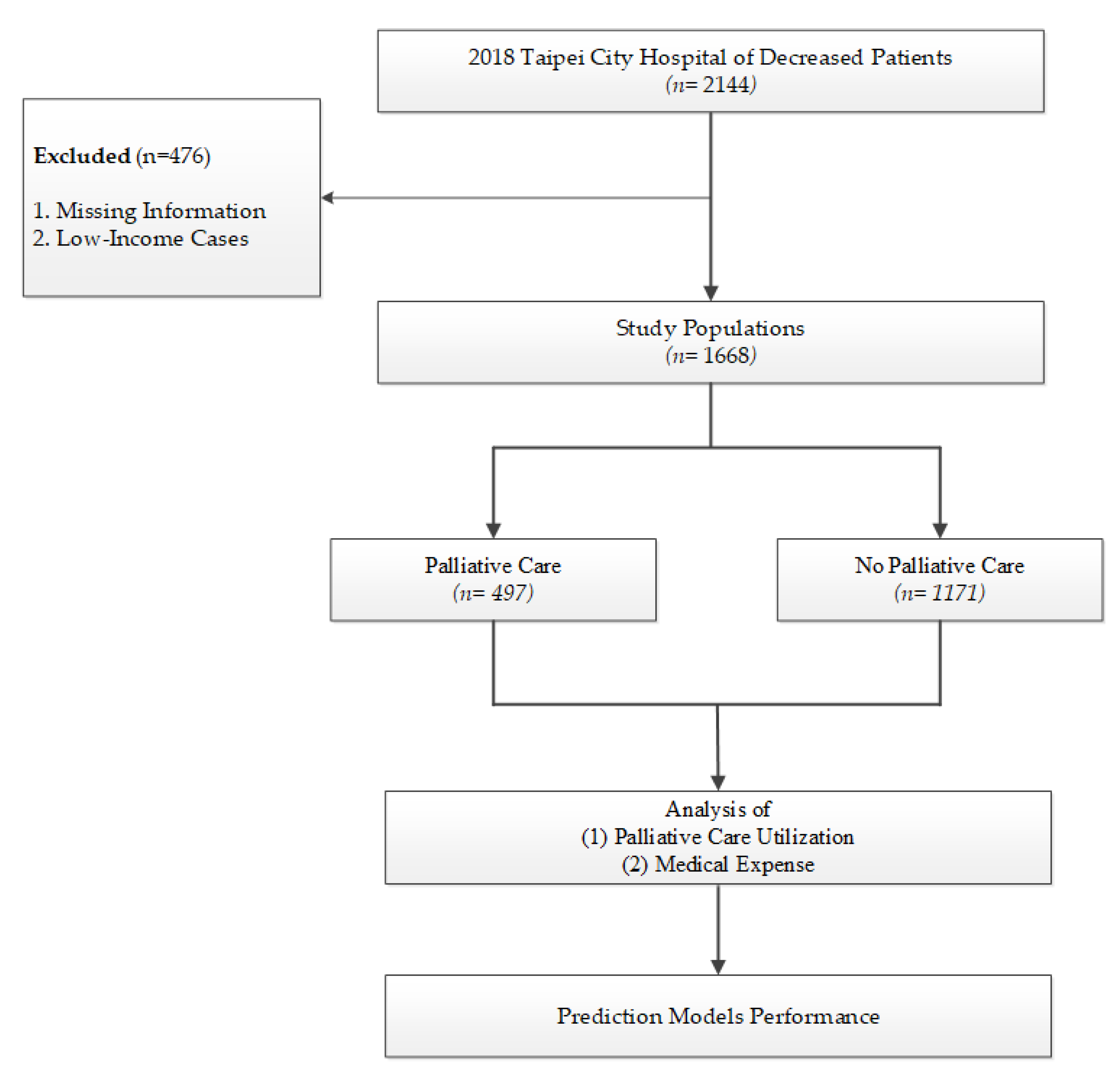
2.1. Study Design and Population
2.2. Baseline Variables
2.3. Statistical Analysis
3. Results
3.1. Study Population Characteristics
3.2. Palliative Care Utilization for Inpatients
3.3. Impact of Palliative Utilization on Medical Expense
3.4. Palliative Care Utilization
3.5. Prediction Model for Palliative Care Utilization
4. Discussion
4.1. Factors Influencing Palliative Care Utilization
4.2. Effect of Usage of Palliative Care on Medical Expense
4.3. Decision of Palliative Care Models
5. Conclusions
6. Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. World Health Organization Definition of Palliative Care. World Health Organization Website. Available online: http://www.who.int/cancer/palliative/definition/en (accessed on 28 March 2022).
- Teno, J.M.; Connor, S.R. Referring a patient and family to high-quality palliative care at the close of life:“We met a new personality... with this level of compassion and empathy”. JAMA 2009, 301, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Meier, D.E. Increased access to palliative care and hospice services: Opportunities to improve value in health care. Milbank Q. 2011, 89, 343–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braus, N.; Campbell, T.C.; Kwekkeboom, K.L.; Ferguson, S.; Harvey, C.; Krupp, A.E.; Lohmeier, T.; Repplinger, M.D.; Westergaard, R.P.; Jacobs, E.A. Prospective study of a proactive palliative care rounding intervention in a medical ICU. Intensive Care Med. 2016, 42, 54–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thongprayoon, C.; Kaewput, W.; Petnak, T.; O’Corragain, O.A.; Boonpheng, B.; Bathini, T.; Vallabhajosyula, S.; Pattharanitima, P.; Lertjitbanjong, P.; Qureshi, F. Impact of palliative care services on treatment and resource utilization for hepatorenal syndrome in the United States. Medicines 2021, 8, 21. [Google Scholar] [CrossRef] [PubMed]
- Sepúlveda, C.; Marlin, A.; Yoshida, T.; Ullrich, A. Palliative care: The World Health Organization’s global perspective. J. Pain Symptom Manag. 2002, 24, 91–96. [Google Scholar] [CrossRef]
- Ferrell, B.R.; Temel, J.S.; Temin, S.; Alesi, E.R.; Balboni, T.A.; Basch, E.M.; Firn, J.I.; Paice, J.A.; Peppercorn, J.M.; Phillips, T. Integration of palliative care into standard oncology care: American Society of Clinical Oncology clinical practice guideline update. J. Clin. Oncol. 2017, 35, 96–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gidwani-Marszowski, R.; Asch, S.M.; Mor, V.; Wagner, T.H.; Faricy-Anderson, K.; Illarmo, S.; Hsin, G.; Patel, M.I.; Ramchandran, K.; Lorenz, K.A. Health system and beneficiary costs associated with intensive end-of-life medical services. JAMA Netw. Open 2019, 2, e1912161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, H.-M.; Liu, C.-K.; Huang, Y.-C.; Ho, C.-W.; Chen, M. Investigating Key Factors Related to the Decision of a Do-Not-Resuscitate Consent. Int. J. Environ. Res. Public Health 2022, 19, 428. [Google Scholar] [CrossRef] [PubMed]
- Kelley, A.S.; Morrison, R.S. Palliative care for the seriously ill. N. Engl. J. Med. 2015, 373, 747–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakitas, M.; Lyons, K.D.; Hegel, M.T.; Balan, S.; Brokaw, F.C.; Seville, J.; Hull, J.G.; Li, Z.; Tosteson, T.D.; Byock, I.R.; et al. Effects of a palliative care intervention on clinical outcomes in patients with advanced cancer: The Project ENABLE II randomized controlled trial. JAMA 2009, 302, 741–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, S.; Brick, A.; O’Hara, S.; Normand, C. Evidence on the cost and cost-effectiveness of palliative care: A literature review. Palliat. Med. 2014, 28, 130–150. [Google Scholar] [CrossRef]
- May, P.; Garrido, M.M.; Cassel, J.B.; Kelley, A.S.; Meier, D.E.; Normand, C.; Smith, T.J.; Stefanis, L.; Morrison, R.S. Prospective cohort study of hospital palliative care teams for inpatients with advanced cancer: Earlier consultation is associated with larger cost-saving effect. J. Clin. Oncol. 2015, 33, 2745–2752. [Google Scholar] [CrossRef]
- Wang, L.; Piet, L.; Kenworthy, C.M.; Dy, S.M. Association between palliative case management and utilization of inpatient, intensive care unit, emergency department, and hospice in Medicaid beneficiaries. Am. J. Hosp. Palliat. Med. 2015, 32, 216–220. [Google Scholar] [CrossRef]
- Huang, Y.C.; Li, S.J.; Chen, M.; Lee, T.S.; Chien, Y.N. Machine-Learning Techniques for Feature Selection and Prediction of Mortality in Elderly CABG Patients. Healthcare 2021, 9, 547. [Google Scholar] [CrossRef]
- Wu, C.-W.; Shen, H.-L.; Lu, C.-J.; Chen, S.-H.; Chen, H.-Y. Comparison of Different Machine Learning Classifiers for Glaucoma Diagnosis Based on Spectralis OCT. Diagnostics 2021, 11, 1718. [Google Scholar] [CrossRef] [PubMed]
- Friedman, J.H. Multivariate adaptive regression splines. Ann. Stat. 1991, 19, 1–67. [Google Scholar] [CrossRef]
- Clark, K.; Phillips, J. End of life care: The importance of culture and ethnicity. Aust. Fam. Physician 2010, 39, 210–213. [Google Scholar] [PubMed]
- May, P.; Garrido, M.M.; Cassel, J.B.; Kelley, A.S.; Meier, D.E.; Normand, C.; Smith, T.J.; Morrison, R.S. Cost analysis of a prospective multi-site cohort study of palliative care consultation teams for adults with advanced cancer: Where do cost-savings come from? Palliat. Med. 2017, 31, 378–386. [Google Scholar] [CrossRef]
- Sadler, K.; Abudari, G.; Aljawi, D.; Snelling, D. Deaths in the emergency department: An assessment of patient’s end-of-life trajectory and quality of care. Indian J. Palliat. Care 2020, 26, 352. [Google Scholar] [CrossRef] [PubMed]
- Rafiq, A.; Ullah, W.; Naglak, M.; Schneider, D. Characteristics and outcomes of patients with partial do not resuscitate orders in a large community hospital. Cureus 2019, 11, e6048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaertner, J.; Frechen, S.; Sladek, M.; Ostgathe, C.; Voltz, R. Palliative care consultation service and palliative care unit: Why do we need both? Oncologist 2012, 17, 428. [Google Scholar] [CrossRef] [PubMed]
- Weissman, D.E.; Meier, D.E. Identifying patients in need of a palliative care assessment in the hospital setting a consensus report from the Center to Advance Palliative Care. J. Palliat. Med. 2011, 14, 17–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quill, T.E.; Abernethy, A.P. Generalist plus specialist palliative care—creating a more sustainable model. N. Engl. J. Med. 2013, 368, 1173–1175. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Baseline | N % | (%) | |
|---|---|---|---|
| Overall population | 1668 | 100% | |
| Sex | Male | 916 | 54.92% |
| Female | 752 | 45.08% | |
| Age group | <65 | 225 | 13.49% |
| 65–79 | 440 | 26.38% | |
| ≥80 | 1003 | 60.13% | |
| Age (mean, std) | 80.32 (13.49) | ||
| DNR | Yes | 1332 | 79.86% |
| No | 336 | 20.14% | |
| Diagnosis | Cancer | 349 | 20.92% |
| Others | 1319 | 79.08% | |
| Hospital | Zhongxiao | 287 | 17.21% |
| Zhongxing | 243 | 14.57% | |
| Heping Fuyou | 347 | 20.80% | |
| Yangming | 221 | 13.25% | |
| Renai | 570 | 34.17% | |
| Family palliative care consultation | Yes | 1226 | 73.50% |
| No | 442 | 26.50% | |
| Palliative consultation services | Yes | 377 | 22.60% |
| No | 1291 | 77.40% | |
| Palliative care units | Yes | 241 | 14.45% |
| No | 1427 | 85.55% | |
| Palliative care a | Yes | 497 | 29.80% |
| No | 1171 | 70.20% | |
| Length of stay (days) | 1–10 | 778 | 46.64% |
| 11–20 | 348 | 20.86% | |
| 21–30 | 219 | 13.13% | |
| >30 | 323 | 19.36% | |
| Length of stay (mean, std) | 27.30 (73.63) | ||
| TW-PCST score | (Mean, std) | 3.51 (2.16) | |
| Unknown (N) | 378 | ||
| Medical expense, NTD (mean, std) | 194,818 (426,945) | ||
| Baseline | Palliative Care | No Palliative Care | p | |||
|---|---|---|---|---|---|---|
| (n = 497) | (n = 1171) | |||||
| N | % | N | % | |||
| Sex | Male | 237 | 47.69 | 515 | 43.98 | 0.1641 |
| Female | 260 | 52.31 | 656 | 56.02 | ||
| Age group | <65 | 61 | 12.27 | 164 | 14.01 | 0.5232 |
| 65–79 | 138 | 27.77 | 302 | 25.79 | ||
| ≥80 | 298 | 59.96 | 705 | 60.20 | ||
| Age mean (std) | 80.91 (13.12) | 80.07 (13.64) | 0.2453 | |||
| DNR | Yes | 406 | 81.69 | 926 | 79.08 | 0.2237 |
| No | 91 | 18.31 | 245 | 20.92 | ||
| Diagnosis | Cancer | 164 | 33.00 | 185 | 15.80 | ≤0.001 |
| Non-cancer | 333 | 67.00 | 986 | 84.20 | ||
| Hospital | Zhongxiao | 146 | 29.38 | 141 | 12.04 | ≤0.001 |
| Zhongxing | 86 | 17.30 | 157 | 13.41 | ||
| Heping Fuyou | 38 | 7.65 | 309 | 26.39 | ||
| Yangming | 7 | 1.41 | 214 | 18.27 | ||
| Renai | 220 | 44.27 | 350 | 29.89 | ||
| Family palliative care consultation | Yes | 128 | 25.75 | 314 | 26.81 | 0.6536 |
| No | 369 | 74.25 | 857 | 73.19 | ||
| Length of stay (days) | 1–10 | 185 | 37.22 | 593 | 50.64 | ≤0.001 |
| 11–20 | 126 | 25.35 | 222 | 18.96 | ||
| 21–30 | 80 | 16.10 | 139 | 11.87 | ||
| >30 | 106 | 21.33 | 217 | 18.53 | ||
| TW-PCST score | (Mean, std) | 3.54 (2.13) | 3.50 (2.17) | 0.7459 | ||
| Unknown (N) | 143 | 28.77 | 253 | 21.61 | 0.0312 | |
| Baseline | Palliative Care | No Palliative Care | p | |
|---|---|---|---|---|
| Medical Cost, NTD | Medical Cost, NTD | |||
| (n = 497) | (n = 1171) | |||
| Sex | Male | 195,004 (562,629) | 214,813 (445,634) | 0.6117 |
| Female | 154,594 (316,466) | 187,767 (362,371) | 0.2031 | |
| Age group | <65 | 176,236 (384,486) | 193,772 (301,040) | 0.7206 |
| 65–79 | 222,033 (680,109) | 209,985 (442,960) | 0.8492 | |
| ≥80 | 154,191 (333,399) | 202,019 (419,551) | 0.0557 | |
| DNR | Yes | 159,637 (320,538) | 192,234 (356,897) | 0.0995 |
| No | 247,553 (840,891) | 243,300 (570,642) | 0.9645 | |
| Diagnosis | Cancer | 91,527 (107,970) | 186,981 (427,035) | 0.0037 |
| Non-cancer | 217,206 (554,796) | 205,908 (408,255) | 0.7328 | |
| Family palliative care consultation | Yes | 197,256 (471,275) | 206,306 (344,590) | 0.7396 |
| No | 113,692 (429,506) | 193,673 (554,107) | 0.105 | |
| Length of stay mean (std) | 30.33 (81.60) | 26.02 (69.97) | 0.3046 | |
| TW-PCST score | (Mean, std) | 158,662 (331,716) | 189,907 (360,096) | 0.1557 |
| Unknown | 254,741 (37,115) | 217,887 (684,968) | 0.5738 | |
| Medical expense (std) | 175,734 (461,906) | 202,918 (411,150) | 0.2567 | |
| Average (Medical expense)/average (LOS) | 5789.1 (3855.4) | 12,115.8 (13,991.5) | ≤ 0.001 | |
| Hospital | Palliative Consultation Services (N = 256) | Palliative Care Units (N = 241) | ||
|---|---|---|---|---|
| N | % | N | % | |
| Renai | 79 | 30.86 | 141 | 55.83 |
| Zhongxiao | 46 | 17.97 | 100 | 44.17 |
| Zhongxing | 86 | 33.59 | – | |
| Heping Fuyou | 38 | 14.84 | – | |
| Yangming | 7 | 2.73 | – | |
| Baseline | Estimate | Error | Pr (>Chi) |
|---|---|---|---|
| Intercept | −1.660 | 0.4372 | |
| Hospital | −0.2351 | 0.04925 | 0.01866 * |
| Sex | 0.130 | 0.1251 | 0.18719 |
| Age | 0.0059 | 0.0046 | 0.15969 |
| DNR | 0.2419 | 0.1618 | 0.18063 |
| Medical expense | −3.080 × 10−6 | 6.398 × 10−7 | <0.001 *** |
| Family palliative care consultation | 0.1030 | 0.1443 | 0.87391 |
| TW-PCST scores | 0.09851 | 0.01695 | <0.001 *** |
| LOS (days) | 0.01741 | 0.00351 | 0.24705 |
| Accuracy | Kappa | Sensitivity | Specificity | AUC | |
|---|---|---|---|---|---|
| LGR | 0.6736 | 0.2673 | 0.8012 | 0.4625 | 0.7058 |
| CART | 0.6943 | 0.3495 | 0.8464 | 0.5213 | 0.7286 |
| MARS | 0.7510 | 0.4501 | 0.8692 | 0.5722 | 0.7847 |
| GB | 0.7357 | 0.4311 | 0.8865 | 0.5251 | 0.8213 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, H.-M.; Liu, C.-K.; Huang, Y.-C.; Chen, M.-C. Exploratory Study of Palliative Care Utilization and Medical Expense for Inpatients at the End-of-Life. Int. J. Environ. Res. Public Health 2022, 19, 4263. https://doi.org/10.3390/ijerph19074263
Lin H-M, Liu C-K, Huang Y-C, Chen M-C. Exploratory Study of Palliative Care Utilization and Medical Expense for Inpatients at the End-of-Life. International Journal of Environmental Research and Public Health. 2022; 19(7):4263. https://doi.org/10.3390/ijerph19074263
Chicago/Turabian StyleLin, Hui-Mei, Chih-Kuang Liu, Yen-Chun Huang, and Ming-Chih Chen. 2022. "Exploratory Study of Palliative Care Utilization and Medical Expense for Inpatients at the End-of-Life" International Journal of Environmental Research and Public Health 19, no. 7: 4263. https://doi.org/10.3390/ijerph19074263
APA StyleLin, H.-M., Liu, C.-K., Huang, Y.-C., & Chen, M.-C. (2022). Exploratory Study of Palliative Care Utilization and Medical Expense for Inpatients at the End-of-Life. International Journal of Environmental Research and Public Health, 19(7), 4263. https://doi.org/10.3390/ijerph19074263