
Efficacy and Sustainability of Diabetes-Specific Meal Replacement on Obese and Overweight Type-2 Diabetes Mellitus Patients: Study Approaches for a Randomised Controlled Trial and Impact of COVID-19 on Trial Progress


 ,
, 
Abstract
:1. Introduction
1.1. Research Objective
1.1.1. Primary Endpoint
1.1.2. Secondary Endpoint
- BMI
- Body Composition
- Waist and hip circumference
- Fasting blood glucose
- Insulin resistance index (HOMA-IR)
- Lipid Profile
- Satiety level
- Hormonal Changes
- Quality of life
- Cost-effectiveness
2. Methodology
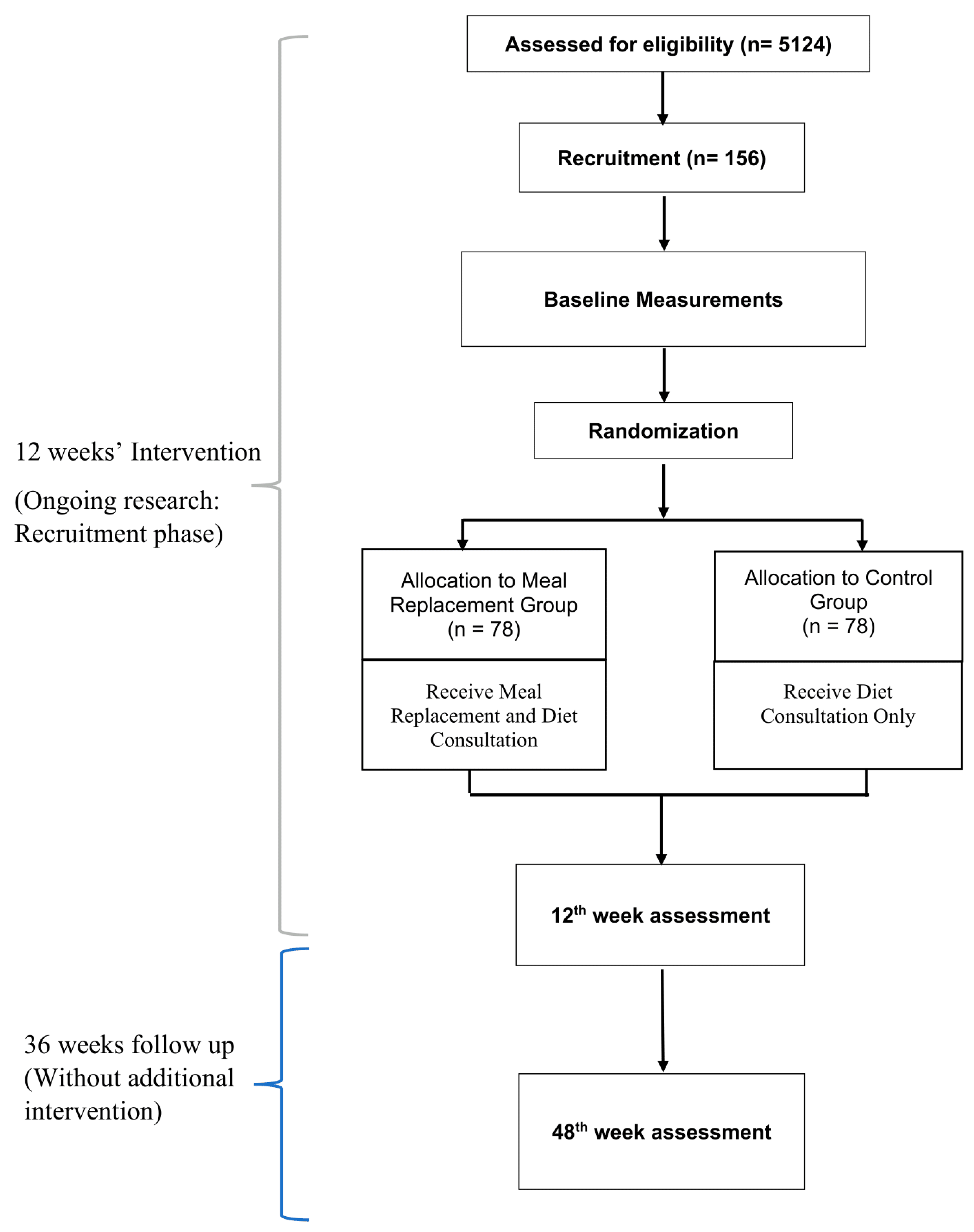
2.1. Study Design
2.2. Sample Size
2.3. Recruitment
2.4. Baseline Screening and Assessment
2.5. Randomisation
2.6. Intervention
2.6.1. Meal Replacement Arm (MR Group)
2.6.2. Control Arm (DC Group)
2.6.3. Follow-Up
2.7. Compliance and Adverse Effects Monitoring
2.8. Data Collection and Outcome Measurement
2.8.1. Socio-Demography Information
2.8.2. Physical Activity Assessment
2.8.3. Dietary Assessment
2.8.4. Anthropometry Measurements
2.8.5. Visual Analog Scale for Satiety Measurement
2.8.6. Blood Pressure
2.8.7. Metabolic Profiles
- a
- HbA1c
- b
- Fasting Blood Glucose
- c
- Fasting Insulin Level
- d
- Lipid Profile Test
- e
- Liver Profile Test
- f
- Renal Profile Test
2.8.8. Hormone Level Measurements
2.8.9. Quality of Life
Audit of Dependent Diabetes Quality of Life (ADDQOL-19)
Diabetes Treatment Satisfaction Questionnaire (DTSQ)
Diabetes Distress Scale (DDS)
2.8.10. Cost-Effectiveness
2.9. Statistical Analysis
2.10. Patient and Public Involvement
2.11. Data Monitoring
2.12. Ethics and Dissemination
3. Impact of COVID 19 on Data Collection
Preliminary Result
4. Discussion
4.1. Limitation
4.2. Implication and Future Implementation
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Diabetes; WHO: Geneva, Switzerland, 2020; Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 3 January 2021).
- United Nations. World Population Review. 2020. Available online: https://worldpopulationreview.com/country-rankings/obesity-rates-by-country (accessed on 18 November 2020).
- Institute of Public Health Malaysia. National Health and Morbidity Survey 2019; Ministry of Health Malaysia: Kuala Lumpur, Malaysia, 2019.
- Colosia, A.D.; Palencia, R.; Khan, S. Prevalence of hypertension and obesity in patients with type 2 diabetes mellitus in observational studies: A systematic literature review. Diabetes Metab. Syndr. Obes. Targets Ther. 2013, 6, 327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fetrnandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bantle, J.P.; Wylie-Rosett, J.; Albright, A.L.; Apovian, C.M.; Clark, N.G.; Franz, M.J.; Hoogwerf, B.J.; Lichtenstein, A.H.; Mayer-Davis, E.; Mooradian, A.D.; et al. Nutrition recommendations and interventions for diabetes: A position statement of the American Diabetes Association. Diabetes Care 2008, 31, S61–S78. [Google Scholar] [PubMed] [Green Version]
- Astbury, N.M.; Piernas, C.; Hartmann-Boyce, J.; Lapworth, S.; Aveyard, P.; Jebb, S.A. A systematic review and meta-analysis of the effectiveness of meal replacements for weight loss. Obes. Rev. 2019, 20, 569–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Look AHEAD Research Group. Reduction in weight and cardiovascular disease risk factors in individuals with type 2 diabetes: One-year results of the Look AHEAD trial. Diabetes Care 2007, 30, 1374. [Google Scholar] [CrossRef] [Green Version]
- Unick, J.L.; Beavers, D.; Jakicic, J.M.; Kitabchi, A.E.; Knowler, W.C.; Wadden, T.A.; Wing, R.R.; Look AHEAD Research Group. Effectiveness of lifestyle interventions for individuals with severe obesity and type 2 diabetes: Results from the Look AHEAD trial. Diabetes Care 2011, 34, 2152–2157. [Google Scholar] [CrossRef] [Green Version]
- Pi-Sunyer, X. The look AHEAD trial: A review and discussion of its outcomes. Curr. Nutr. Rep. 2014, 3, 387–391. [Google Scholar] [CrossRef]
- Johansson, K.; Sundstrom, J.; Marcus, C.; Hemmingsson, E.; Neovius, M. Risk of symptomatic gallstones and cholecystectomy after a very-low-calorie diet or low-calorie diet in a commercial weight loss program: 1-year matched cohort study. Int. J. Obes. 2013, 38, 279. [Google Scholar] [CrossRef] [Green Version]
- Tatti, P.; Di Mauro, P.; Neri, M.; Pipicelli, G.; Mussad, V.A. Effect of a low-calorie high nutritional value formula on weight loss in type 2 diabetes mellitus. Mediterr. J. Nutr. Metab. 2010, 3, 65–69. [Google Scholar] [CrossRef]
- Guo, X.; Xu, Y.; He, H.; Cai, H.; Zhang, J.; Li, Y.; Yan, X.; Zhang, M.; Zhang, N.; Maddela, R.L.; et al. Effects of a meal replacement on body composition and metabolic parameters among subjects with overweight or obesity. J. Obes. 2018, 2018, 2837367. [Google Scholar] [CrossRef] [Green Version]
- Keogh, J.B.; Clifton, P.M. Meal replacements for weight loss in type 2 diabetes in a community setting. J. Nutr. Metab. 2012, 2012, 918571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ash, S.; Reeves, M.M.; Yeo, S.; Morrison, G.; Carey, D.; Capra, S. Effect of intensive dietetic interventions on weight and glycaemic control in overweight men with Type II diabetes: A randomised trial. Int. J. Obes. 2003, 27, 797–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kementerian Kesihatan Malaysia. The Current Situation of the COVID-19 Pandemic in Malaysia; Kementerian Kesihatan Malaysia: Kuala Lumpur, Malaysia, 2021. Available online: https://covid-19.moh.gov.my/terkini (accessed on 15 June 2021).
- Brand-Miller, J.; Hayne, S.; Petocz, P.; Colagiuri, S. Low–glycemic index diets in the management of diabetes: A meta-analysis of randomized controlled trials. Diabetes Care 2003, 26, 2261–2267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abramson, J.H. WINPEPI updated: Computer programs for epidemiologists, and their teaching potential. Epidemiol. Perspect. Innov. 2011, 8, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiew, F.T.; Han, W.C.; Gan, W.X. Impact of Diabetes-Formulated Oral Nutritional Supplement Versus Instant Cocoa Drink and 3-in-1 Oatmeal on Postprandial Glucose. Int. J. Healthc. Sci. 2017, 5, 6. [Google Scholar]
- Yusof, B.N.M.; Talib, R.A.; Kamaruddin, N.A.; Karim, N.A.; Chinna, K.; Gilbertson, H. A low-GI diet is associated with a short-term improvement of glycaemic control in Asian patients with type 2 diabetes. Diabetes Obes. Metab. 2009, 11, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Zare, R.; Nadjarzadeh, A.; Zarshenas, M.M.; Shams, M.; Heydari, M. Efficacy of cinnamon in patients with type II diabetes mellitus: A randomized controlled clinical trial. Clin. Nutr. 2019, 38, 549–556. [Google Scholar] [CrossRef]
- Costello, R.B.; Dwyer, J.T.; Saldanha, L.; Bailey, R.L.; Merkel, J.; Wambogo, E. Do Cinnamon Supplements Have a Role in Glycemic Control in Type 2 Diabetes? A Narrative Review. J. Acad. Nutr. Diet. 2016, 116, 1794–1802. [Google Scholar] [CrossRef] [Green Version]
- Soo, K.L.; Wan Abdul Manan, W.M.; Wan Suriati, W.N. The Bahasa Melayu Version of the Global Physical Activity Questionnaire: Reliability and Validity Study in Malaysia. Asia Pac. J. Public Health 2012, 27, NP184–NP193. [Google Scholar] [CrossRef]
- Ortega, R.M.; Pérez-Rodrigo, C.; López-Sobaler, A.M. Dietary assessment methods: Dietary records. J. Nutr. Hosp. 2015, 31, 38–45. [Google Scholar]
- Suzana, S.; Shanita, S.N.; Zahara, A.; Hasnah, H. Atlas of Food Exchange & Portion Sizes; MDC Publishers Sdn. Bhd.: Kuala Lumpur, Malaysia, 2015. [Google Scholar]
- Norimah, A. Development and validation of a Food Frequency Questionnaire (FFQ) for assessing sugar consumption among adults in Klang Valley, Malaysia. Malays. J. Nutr. 2012, 18, 283–293. [Google Scholar]
- Gibson, R.S. Principles of Nutritional Assessment; Oxford University Press: New York, NY, USA, 2005. [Google Scholar]
- World Health Organization. Physical Status: The Use of and Interpretation of Anthropometry, Report of a WHO Expert Committee; World Health Organization: Geneva, Switzerland, 1995. [Google Scholar]
- Li, Y.C.; Li, C.I.; Lin, W.Y.; Liu, C.S.; Hsu, H.S.; Lee, C.C.; Chen, F.N.; Li, T.C.; Lin, C.C. Percentage of body fat assessment using bioelectrical impedance analysis and dual-energy X-ray absorptiometry in a weight loss program for obese or overweight Chinese adults. PLoS ONE 2013, 8, e58272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lukaski, H.C.; Johnson, P.E.; Bolonchuk, W.W.; Lykken, G.I. Assessment of fat-free mass using bioelectrical impedance measurements of the human body. Am. J. Clin. Nutr. 1985, 41, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Jannoo, Z.; Yap, B.W.; Musa, K.I.; Lazim, M.A.; Hassali, M.A. An audit of diabetes-dependent quality of life in patients with type 2 diabetes mellitus in Malaysia. Qual. Life Res. 2015, 24, 2297–2302. [Google Scholar] [CrossRef]
- Bradley, C.; Todd, C.; Gorton, T.; Symonds, E.; Martin, A.; Plowright, R. The development of an individualized questionnaire measure of perceived impact of diabetes on quality of life: The ADDQoL. Qual. Life Res. 1999, 8, 79–91. [Google Scholar] [CrossRef]
- Blundell, J.; De Graaf, C.; Hulshof, T.; Jebb, S.; Livingstone, B.; Lluch, A.; Mela, D.; Salah, S.; Schuring, E.; Van Der Knaap, H.; et al. Appetite control: Methodological aspects of the evaluation of foods. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2010, 11, 251–270. [Google Scholar] [CrossRef] [Green Version]
- Anderson, G.H.; Catherine, N.L.; Woodend, D.M.; Wolever, T.M. Inverse association between the effect of carbohydrates on blood glucose and subsequent short-term food intake in young men. Am. J. Clin. Nutr. 2002, 76, 1023–1030. [Google Scholar] [CrossRef]
- Salgado, A.L.; Carvalho, L.D.; Oliveira, A.C.; Santos, V.N.; Vieira, J.G.; Parise, E.R. Insulin resistance index (HOMA-IR) in the differentiation of patients with non-alcoholic fatty liver disease and healthy individuals. Arq. Gastroenterol. 2010, 47, 165–169. [Google Scholar] [CrossRef] [Green Version]
- Bradley, C. The diabetes treatment satisfaction questionnaire: DTSQ. Handb. Psychol. Diabetes A Guide Psychol. Meas. Diabetes Res. Pract. 1994, 111, 132. [Google Scholar]
- Bradley, C.; Gamsu, D.S.; Psychological Well-being Working Group of the WHO/IDF St Vincent Declaration Action Programme for Diabetes. Guidelines for encouraging psychological well-being: Report of a working group of the world health organization regional office for Europe and international diabetes federation European region St Vincent declaration action programme for diabetes. Diabet. Med. 1994, 11, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Bradley, C. Diabetes treatment satisfaction questionnaire. Change version for use alongside status version provides appropriate solution where ceiling effects occur. Diabetes Care 1999, 22, 530–532. [Google Scholar] [CrossRef] [PubMed]
- Bradley, C.; Plowright, R.; Stewart, J.; Valentine, J.; Witthaus, E. The Diabetes Treatment Satisfaction Questionnaire change version (DTSQc) evaluated in insulin glargine trials shows greater responsiveness to improvements than the original DTSQ. Health Qual. Life Outcomes 2007, 5, 57. [Google Scholar] [CrossRef] [PubMed]
- Polonsky, W.H.; Fisher, L.; Earles, J.; Dudl, R.J.; Lees, J.; Mullan, J.; Jackson, R.A. Assessing psychosocial distress in diabetes: Development of the diabetes distress scale. Diabetes Care 2005, 28, 626–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chew, B.H.; Mukhtar, F.; Sherina, M.S.; Paimin, F.; Hassan, N.H.; Jamaludin, N.K. The reliability and validity of the Malay version 17-item Diabetes Distress Scale. Malays. Fam. Phys. 2015, 10, 22–35. [Google Scholar]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.F.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Shafie, A.A.; Vasan Thakumar, A.; Lim, C.J.; Luo, N.; Rand-Hendriksen, K.; Md Yusof, F.A. EQ-5D-5L valuation for the Malaysian population. PharmacoEconomics 2019, 37, 715–725. [Google Scholar] [CrossRef]
- Shafie, A.A.; Vasan Thakumar, A.; Lim, C.J.; Luo, N. Psychometric performance assessment of Malay and Malaysian English version of EQ-5D-5L in the Malaysian population. Qual. Life Res. 2019, 28, 153–162. [Google Scholar] [CrossRef]
- Koohkan, S.; McCarthy, D.; Berg, A. The effect of a soy-yoghurt-honey product on excess weight and related health risk factors-A review. J. Nutr. Health Food Sci. 2017, 5, 1–10. [Google Scholar]
- Lean, M.E.; Leslie, W.S.; Barnes, A.C.; Brosnahan, N.; Thom, G.; McCombie, L.; Peters, C.; Zhyzhneuskaya, S.; Al-Mrabeh, A.; Hollingsworth, K.G.; et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): An open-label, cluster-randomised trial. Lancet 2018, 391, 541–551. [Google Scholar] [CrossRef] [Green Version]
- Astbury, N.M.; Aveyard, P.; Nickless, A.; Hood, K.; Corfield, K.; Lowe, R.; Jebb, S.A. Doctor Referral of Overweight People to Low Energy total diet replacement Treatment (DROPLET): Pragmatic randomised controlled trial. BMJ 2018, 362, k3760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, J.; Lu, J.; Ma, X.; Ying, L.; Lu, W.; Zhu, W.; Bao, Y.; Zhou, J. Breakfast replacement with a liquid formula improves glycaemic variability in patients with type 2 diabetes: A randomised clinical trial. Br. J. Nutr. 2019, 121, 560–566. [Google Scholar] [CrossRef]
- Boonyavarakul, A.; Leelawattana, R.; Pongchaiyakul, C.; Buranapin, S.; Phanachet, P.; Pramyothin, P. Effects of meal replacement therapy on metabolic outcomes in Thai patients with type 2 diabetes: A randomized controlled trial. Nutr. Health 2018, 24, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Jáquez, A.; Sánchez, J.J.; Acevedo, N.; Guzmán, E. Efficacy of Diabetes-Specific Formulas as Meal Replacements in Diabetic Pa-tients: An Overview. Int. J. Endocrinol. Metab. Disord. 2020, 6, 1–10. [Google Scholar]
- Ames, G.E.; Thomas, C.S.; Patel, R.H.; McMullen, J.S.; Lutes, L.D. Should providers encourage realistic weight expectations and satisfaction with lost weight in commercial weight loss programs? a preliminary study. SpringerPlus 2014, 3, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemmingsson, E.; Johansson, K.; Eriksson, J.; Sundström, J.; Neovius, M.; Marcus, C. Weight loss and dropout during a commercial weight-loss program including a very-low-calorie diet, a low-calorie diet, or restricted normal food: Observational cohort study. Am. J. Clin. Nutr. 2012, 96, 953–961. [Google Scholar] [CrossRef] [PubMed]
- Svetkey, L.P.; Stevens, V.J.; Brantley, P.J.; Appel, L.J.; Hollis, J.F.; Loria, C.M.; Vollmer, W.M.; Gullion, C.M.; Funk, K.; Smith, P.; et al. Comparison of strategies for sustaining weight loss: The weight loss maintenance randomized controlled trial. JAMA 2008, 299, 1139–1148. [Google Scholar] [CrossRef] [Green Version]
- Turner, J.R. New FDA guidance on general clinical trial conduct in the era of COVID-19. Ther. Innov. Regul. Sci. 2020, 54, 723–724. [Google Scholar] [CrossRef]
- European Medicines Agency. Guidance on the Management of Clinical Trials during the COVID-19 (Coronavirus) Pandemic; European Commission: Brussels, Belgium, 2020. [Google Scholar]
- Doherty, G.J.; Goksu, M.; de Paula, B.H.R. Rethinking cancer clinical trials for COVID-19 and beyond. Nat. Cancer 2020, 1, 568–572. [Google Scholar] [CrossRef]
- Dorsey, E.R.; Kluger, B.; Lipset, C.H. The New Normal in Clinical Trials: Decentralized Studies. Ann. Neurol. 2020, 88, 863–866. [Google Scholar] [CrossRef]
- Ponvel, P.; Shahar, S.; Singh, D.K.; Ludin, A.F.; Rajikan, R.; Rajab, N.F.; Ai-Vyrn, C.; Din, N.C.; Ibrahim, N.; Subramaniam, P.; et al. Multidomain Intervention for Reversal of Cognitive Frailty: Towards a Personalized Approach (AGELESS Trial): Study Design. J. Alzheimer’s Dis. 2021, 82, 673–687. [Google Scholar] [CrossRef] [PubMed]
- Waterhouse, D.M.; Harvey, R.D.; Hurley, P.; Levit, L.A.; Kim, E.S.; Klepin, H.D.; Mileham, K.F.; Nowakowski, G.; Schenkel, C.; Davis, C.; et al. Early Impact of COVID-19 on the Conduct of Oncology Clinical Trials and Long-Term Opportunities for Transformation: Findings From an American Society of Clinical Oncology Survey. JCO Oncol. Pract. 2020, 16, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Aravindhan, K.; Mat, S.; Hamid, T.A.; Shahar, S.; Majeed, A.B.; Teh, P.L.; Ramasamy, K.; Singh, D.K.; Tan, M.P. Development of Virtual Surveys for the COVID-19 Wave of the AGELESS Longitudinal Study in Malaysia. Gerontology 2021, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.C.; Ashley, D.M.; Khasraw, M. Adapting to a Pandemic—Conducting Oncology Trials during the SARS-CoV-2 Pandemic. Clin. Cancer Res. 2020, 26, 3100–3103. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Adherence to Long-Term Therapies: Evidence for Action; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Chan, A.W.; Tetzlaff, J.M.; Gøtzsche, P.C.; Altman, D.G.; Mann, H.; Berlin, J.A.; Dickersin, K.; Hróbjartsson, A.; Schulz, K.F.; Parulekar, W.R.; et al. SPIRIT 2013 explanation and elaboration: Guidance for protocols of clinical trials. BMJ 2013, 346, e7586. [Google Scholar] [CrossRef] [Green Version]
- Mogre, V.; Johnson, N.A.; Tzelepis, F.; Shaw, J.E.; Paul, C. A systematic review of adherence to diabetes self-care behaviours: Evidence from low-and middle-income countries. J. Adv. Nurs. 2019, 75, 3374–3389. [Google Scholar] [CrossRef]
- Osterberg, L.; Blaschke, T. Adherence to medication. N. Engl. J. Med. 2005, 353, 487–497. [Google Scholar] [CrossRef] [Green Version]
- Yu, K.; Ke, M.-Y.; Li, W.-H.; Zhang, S.-Q.; Fang, X.-C. The impact of soluble dietary fibre on gastric emptying, postprandial blood glucose and insulin in patients with type 2 diabetes. Asia Pac. J. Clin. Nutr. 2014, 23, 210–218. [Google Scholar]
- Burger, K.N.J.; Beulens, J.W.J.; Van Der Schouw, Y.T.; Sluijs, I.; Spijkerman, A.M.W.; Sluik, D.; Boeing, H.; Kaaks, R.; Teucher, B.; Dethlefsen, C.; et al. Dietary Fiber, Carbohydrate Quality and Quantity, and Mortality Risk of Individuals with Diabetes Mellitus. PLoS ONE 2012, 7, e43127. [Google Scholar] [CrossRef]
- Han, J.R.; Deng, B.; Sun, J.; Chen, C.G.; Corkey, B.; Kirkland, J.L.; Ma, J.; Guo, W. Effects of dietary medium-chain triglyceride on weight loss and insulin sensitivity in a group of moderately overweight free-living type 2 diabetic Chinese subjects. Metabolism 2007, 56, 985–991. [Google Scholar] [CrossRef]
- Maresch, C.C.; Petry, S.F.; Theis, S.; Bosy-Westphal, A.; Linn, T. Low Glycemic Index Prototype Isomaltulose—Update of Clinical Trials. Nutrients 2017, 9, 381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunner, S.; Holub, I.; Theis, S.; Gostner, A.; Melcher, R.; Wolf, P.; Amann-Gassner, U.; Scheppach, W.; Hauner, H. Metabolic Effects of Replacing Sucrose by Isomaltulose in Subjects With Type 2 Diabetes. Diabetes Care 2012, 35, 1249–1251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pipe, E.A.; Gobert, C.P.; Capes, S.E.; Darlington, G.A.; Lampe, J.W.; Duncan, A.M. Soy Protein Reduces Serum LDL Cholesterol and the LDL Cholesterol:HDL Cholesterol and Apolipoprotein B:Apolipoprotein A-I Ratios in Adults with Type 2 Diabetes. J. Nutr. 2009, 139, 1700–1706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Hong, K.; Saltsman, P.; Deshields, S.; Bellman, M.; Thames, G.; Liu, Y.; Wang, H.-J.; Elashoff, R.M.; Heber, D. Long-term efficacy of soy-based meal replacements vs an individualized diet plan in obese type II DM patients: Relative effects on weight loss, metabolic parameters, and C-reactive protein. Eur. J. Clin. Nutr. 2004, 59, 411–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bierenbaum, M.L.; Reichstein, R.P.; Watkins, T.R.; Maginnis, W.P.; Geller, M. Effects of canola oil on serum lipids in humans. J. Am. Coll. Nutr. 1991, 10, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, D.J.; Kendall, C.W.; Vuksan, V.; Faulkner, D.; Augustin, L.S.; Mitchell, S.; Ireland, C.; Srichaikul, K.; Mirrahimi, A.; Chiavaroli, L.; et al. Effect of Lowering the Glycemic Load With Canola Oil on Glycemic Control and Cardiovascular Risk Factors: A Randomized Controlled Trial. Diabetes Care 2014, 37, 1806–1814. [Google Scholar] [CrossRef] [Green Version]
- Kirkham, S.; Akilen, R.; Sharma, S.; Tsiami, A. The potential of cinnamon to reduce blood glucose levels in patients with type 2 diabetes and insulin resistance. Diabetes Obes. Metab. 2009, 11, 1100–1113. [Google Scholar] [CrossRef]
- Qin, B.; Panickar, K.S.; Anderson, R.A. Cinnamon: Potential Role in the Prevention of Insulin Resistance, Metabolic Syndrome, and Type 2 Diabetes. J. Diabetes Sci. Technol. 2010, 4, 685–693. [Google Scholar] [CrossRef] [Green Version]
- Heshmat-Ghahdarijani, K.; Mashayekhiasl, N.; Amerizadeh, A.; Jervekani, Z.T.; Sadeghi, M. Effect of fenugreek consumption on serum lipid profile: A systematic review and meta-analysis. Phytotherapy Res. 2020, 34, 2230–2245. [Google Scholar] [CrossRef]
- Tavakoly, R.; Maracy, M.R.; Karimifar, M.; Entezari, M. Does fenugreek ( Trigonella foenum-graecum ) seed improve inflammation, and oxidative stress in patients with type 2 diabetes mellitus? A parallel group randomized clinical trial. Eur. J. Integr. Med. 2018, 18, 13–17. [Google Scholar] [CrossRef]
- Najdi, R.; Hagras, M.M.; Kamel, F.; Magadmi, R. A randomized controlled clinical trial evaluating the effect of Trigonella foenum-graecum (fenugreek) versus glibenclamide in patients with diabetes. Afr. Health Sci. 2019, 19, 1594–1601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shanmugasundaram, E.; Rajeswari, G.; Baskaran, K.; Kumar, B.; Shanmugasundaram, K.; Ahmath, B. Use of Gymnema sylvestre leaf extract in the control of blood glucose in insulin-dependent diabetes mellitus. J. Ethnopharmacol. 1990, 30, 281–294. [Google Scholar] [CrossRef]
- Khan, F.; Sarker, M.R.; Ming, L.C.; Mohamed, I.N.; Zhao, C.; Sheikh, B.Y.; Tsong, H.F.; Rashid, M.A. Comprehensive Review on Phytochemicals, Pharmacological and Clinical Potentials of Gymnema sylvestre. Front. Pharmacol. 2019, 10, 1223. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, P.; Ahmad, K.; Baig, M.H. Gymnema sylvestre for Diabetes: From Traditional Herb to Future’s Therapeutic. Curr. Pharm. Des. 2017, 23, 1667–1676. [Google Scholar] [CrossRef] [PubMed]
- Joseph, B.; Jini, D. Antidiabetic effects of Momordica charantia (bitter melon) and its medicinal potency. Asian Pac. J. Trop. Dis. 2013, 3, 93–102. [Google Scholar] [CrossRef]
- Kim, S.K.; Jung, J.; Jung, J.H.; Yoon, N.; Kang, S.S.; Roh, G.S.; Hahm, J.R. Hypoglycemic efficacy and safety of Momordica charantia (bitter melon) in patients with type 2 diabetes mellitus. Complement. Ther. Med. 2020, 52, 102524. [Google Scholar] [CrossRef]
- Jayachandran, M.; Vinayagam, R.; Ambati, R.R.; Xu, B.; Chung, S.S.M. Guava Leaf Extract Diminishes Hyperglycemia and Oxidative Stress, Prevents β-Cell Death, Inhibits Inflammation, and Regulates NF-kB Signaling Pathway in STZ Induced Diabetic Rats. BioMed Res. Int. 2018, 2018, 4601649. [Google Scholar] [CrossRef] [Green Version]
- Brumatti, L.V.; Marcuzzi, A.; Tricarico, P.M.; Zanin, V.; Girardelli, M.; Bianco, A.M. Curcumin and Inflammatory Bowel Disease: Potential and Limits of Innovative Treatments. Molecules 2014, 19, 21127–21153. [Google Scholar] [CrossRef] [Green Version]
- Margina, D.; Olaru, O.T.; Ilie, M.; Grădinaru, D.; Guțu, C.; Voicu, S.; Dinischiotu, A.; Spandidos, D.A.; Tsatsakis, A.M. Assessment of the potential health benefits of certain total extracts from Vitis vinifera, Aesculus hyppocastanum and Curcuma longa. Exp. Ther. Med. 2015, 10, 1681–1688. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, J.; Kabiru, A.Y.; Abdulrasheed-Adeleke, T.; Lawal, B.; Adewuyi, A.H. Antioxidant and hepatoprotective potentials of curcuminoid isolates from turmeric (Curcuma longa) rhizome on CCl4-induced hepatic damage in Wistar rats. J. Taibah Univ. Sci. 2020, 14, 908–915. [Google Scholar] [CrossRef]
- Karlowicz-Bodalska, K.; Han, S.; Freier, J.; Smoleński, M.; Bodalska, A. Curcuma longa as medicinal herb in the treatment of diabet- ic complications. Acta Pol. Pharm. Drug Res. 2017, 74, 605–610. [Google Scholar]
- Amin, A.R.; Kassab, R.; Moneim, A.E.A.; Amin, H.K. Comparison Among Garlic, Berberine, Resveratrol, Hibiscus sabdariffa, GenusZizyphus, Hesperidin, Red Beetroot, Catha edulis, Portulaca oleracea, and Mulberry Leaves in the Treatment of Hypertension and Type 2 DM: A Comprehensive Review. Nat. Prod. Commun. 2020, 15. [Google Scholar] [CrossRef]
- Sheng, Y.; Liu, J.; Zheng, S.; Liang, F.; Luo, Y.; Huang, K.; Xu, W.; He, X. Mulberry leaves ameliorate obesity through enhancing brown adipose tissue activity and modulating gut microbiota. Food Funct. 2019, 10, 4771–4781. [Google Scholar] [CrossRef] [PubMed]
- Kaur, M.; Agarwal, C.; Agarwal, R. Anticancer and Cancer Chemopreventive Potential of Grape Seed Extract and Other Grape-Based Products. J. Nutr. 2009, 139, 1806S–1812S. [Google Scholar] [CrossRef] [Green Version]
- Kwatra, B. A review on potential properties and therapeutic applications of grape seed extract. World J. Pharm. Res. 2020, 9, 2519–2540. [Google Scholar]

{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Aged 20–65 years old | On insulin treatment |
| Diagnosed with T2DM for at least 6 months with baseline HbA1c levels between 7.5% and 12% for the past 3 months | With chronic kidney disease or on continuous ambulatory peritoneal dialysis or hemodialysis (GFR < 30 mL/min/1.73 m2) |
| Overweight or obese with BMI ≥ 25 kg/m2 | With hepatic diseases (ALT > 120 IU/L) |
| On stable doses of any oral hypoglycaemic agents for the past 3 months | With history of chronic alcohol abuse |
| Pregnant and lactating women | |
| Currently consuming any weight reduction products or any slimming prescriptions | |
| Currently involving in weight loss programs | |
| Record of COVID-19 diagnosis |
| Sample Size Calculation | |
| F tests—ANOVA: Repeated measures, between factors | |
| Analysis: A priori: Compute required sample size | |
| Input | |
| Effect size f | = 0.2055067 |
| α err prob | = 0.05 |
| Power (1-β err prob) | = 0.80 |
| Number of groups | = 2 |
| Number of measurements | = 4 |
| Corr among rep measures | = 0.5 |
| Output | |
| Noncentrality parameter λ | = 8.1087367 |
| Critical F | = 3.9214782 |
| Numerator df | = 1.0000000 |
| Denominator df | = 118 |
| Total sample size | = 120 |
| Actual power | = 0.8063091 |
| Data Collected/Session | Week 0 | Week 6 | Week 12 | Week 24 | Week 36 | Week 48 |
|---|---|---|---|---|---|---|
| Socio-demography information | / | |||||
| Global Physical Activity Questionnaire | / | / | / | / | / | |
| Dietary Assessment | ||||||
| 3-day dietary recall | / | / | / | / | / | / |
| Food Frequency Questionnaire | / | / | / | / | / | / |
| Anthropometry Measurements | ||||||
| Height | / | / | / | / | / | / |
| Weight | / | / | / | / | / | / |
| Neck circumference | / | / | / | / | / | / |
| Waist circumference | / | / | / | / | / | / |
| Hip circumference | / | / | / | / | / | / |
| Body composition (muscle mass, fat mass, fat percentage) | / | / | / | / | / | / |
| Metabolic Profiles | ||||||
| HbA1c | / | / | / | |||
| Fasting Blood Glucose | / | / | / | |||
| Insulin Resistance Index (HOMA-IR) | / | / | / | |||
| Lipid profile | / | / | / | |||
| Renal Profile | / | / | / | |||
| Liver Profile | / | / | / | |||
| Hormone related to Glycemic Control | ||||||
| Adiponectin, Leptin | / | / | / | |||
| Satiety Measurements | ||||||
| VAS | / | / | / | / | / | / |
| Ghrelin, obestatin, peptide YY | / | / | / | / | ||
| Quality of life | ||||||
| ADDQOL-19 | / | / | / | / | / | |
| DTSQ | / | / | / | / | / | |
| DDS | / | / | / | / | / | |
| Cost-effectiveness | ||||||
| EQ-5D-5L | / | / | / | / | / | |
| Parameters | Numbers/Mean |
|---|---|
| Gender | |
| Male | 81 (59.5%) |
| Female | 55 (40.5%) |
| Age | 54.9 ± 9.3 |
| Race | |
| Malay | 87 (63.97%) |
| Chinese | 25 (18.38%) |
| Indian | 21 (15.44%) |
| Others | 3 (0.02%) |
| Duration of diagnosis for T2DM (Years) | 6.4 ± 4.3 |
| HbA1c Levels (%) | 8.5 ± 1.0 |
| Fasting Plasma Glucose (mmol/L) | 8.6 ± 2.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lew, L.C.; Mat Ludin, A.F.; Shahar, S.; Abdul Manaf, Z.; Mohd Tohit, N. Efficacy and Sustainability of Diabetes-Specific Meal Replacement on Obese and Overweight Type-2 Diabetes Mellitus Patients: Study Approaches for a Randomised Controlled Trial and Impact of COVID-19 on Trial Progress. Int. J. Environ. Res. Public Health 2022, 19, 4188. https://doi.org/10.3390/ijerph19074188
Lew LC, Mat Ludin AF, Shahar S, Abdul Manaf Z, Mohd Tohit N. Efficacy and Sustainability of Diabetes-Specific Meal Replacement on Obese and Overweight Type-2 Diabetes Mellitus Patients: Study Approaches for a Randomised Controlled Trial and Impact of COVID-19 on Trial Progress. International Journal of Environmental Research and Public Health. 2022; 19(7):4188. https://doi.org/10.3390/ijerph19074188
Chicago/Turabian StyleLew, Leong Chen, Arimi Fitri Mat Ludin, Suzana Shahar, Zahara Abdul Manaf, and Noorlaili Mohd Tohit. 2022. "Efficacy and Sustainability of Diabetes-Specific Meal Replacement on Obese and Overweight Type-2 Diabetes Mellitus Patients: Study Approaches for a Randomised Controlled Trial and Impact of COVID-19 on Trial Progress" International Journal of Environmental Research and Public Health 19, no. 7: 4188. https://doi.org/10.3390/ijerph19074188
APA StyleLew, L. C., Mat Ludin, A. F., Shahar, S., Abdul Manaf, Z., & Mohd Tohit, N. (2022). Efficacy and Sustainability of Diabetes-Specific Meal Replacement on Obese and Overweight Type-2 Diabetes Mellitus Patients: Study Approaches for a Randomised Controlled Trial and Impact of COVID-19 on Trial Progress. International Journal of Environmental Research and Public Health, 19(7), 4188. https://doi.org/10.3390/ijerph19074188