
A Comparison of Pre-Emptive Co-Amoxiclav, Postoperative Amoxicillin, and Metronidazole for Prevention of Postoperative Complications in Dentoalveolar Surgery: A Randomized Controlled Trial

Abstract
:1. Introduction
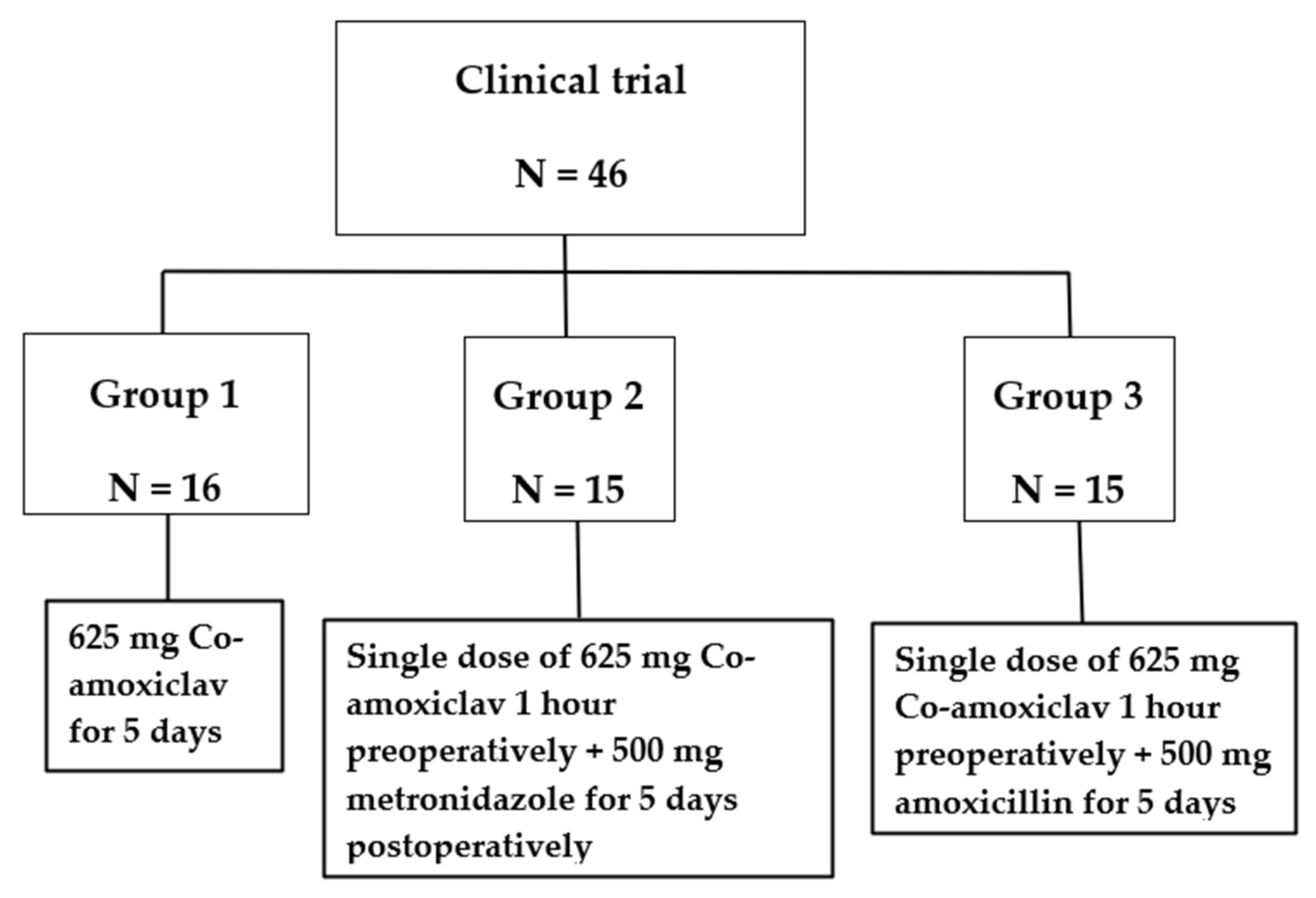
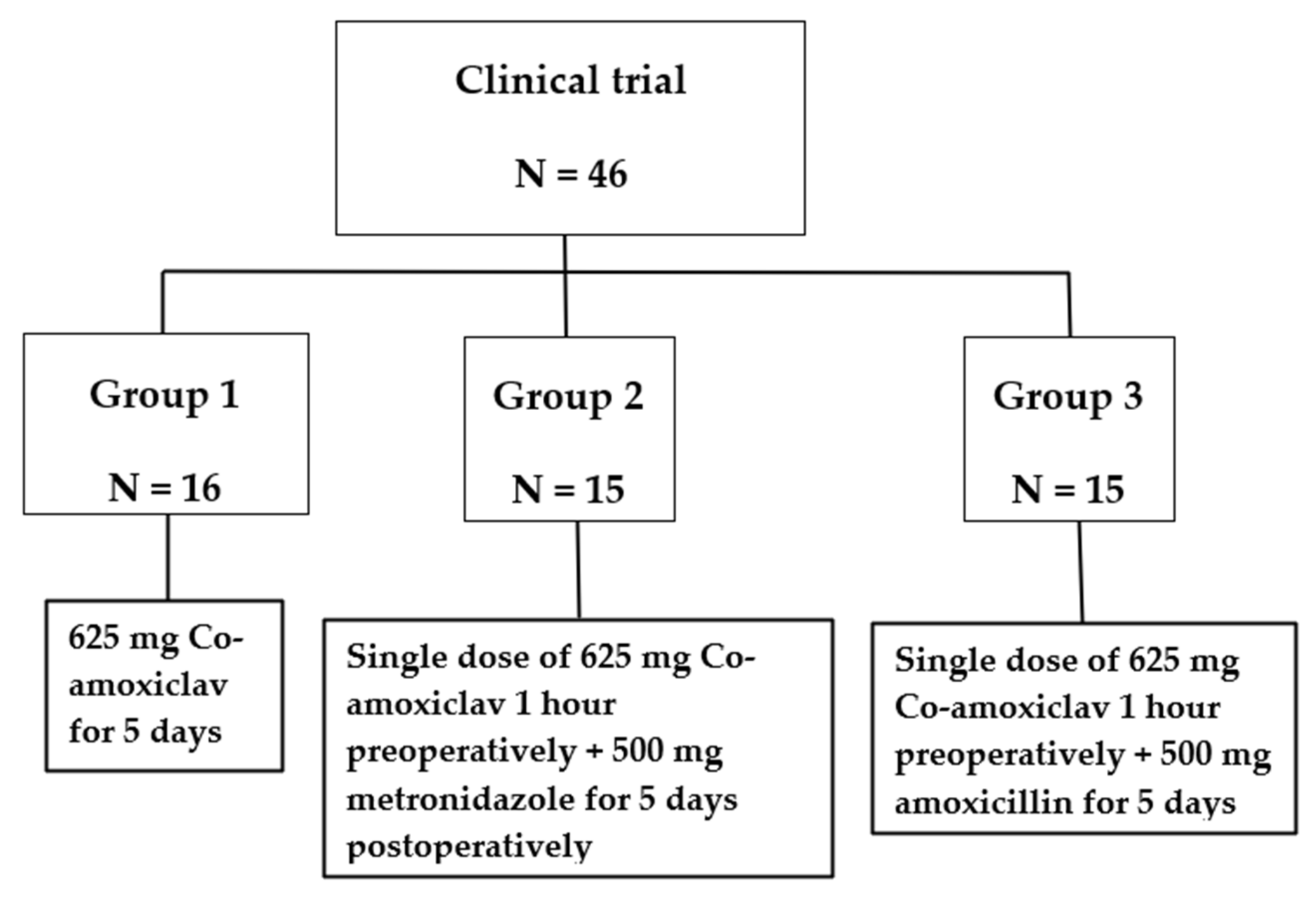
2. Materials and Methods
Statistical Analysis
3. Results
3.1. The Main Results
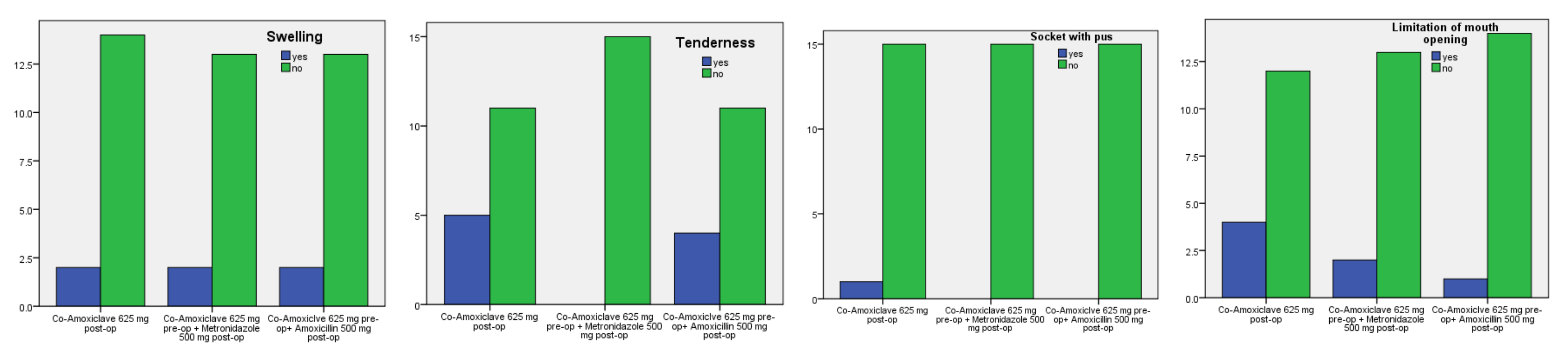
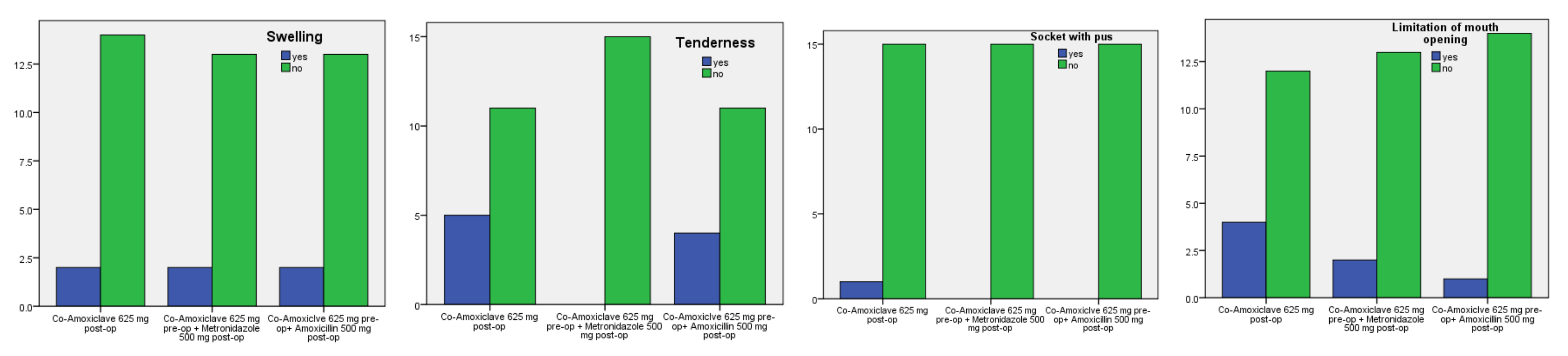
3.2. Surgical Site Infection (SSI)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khooharo, T.S.; Hassan, S.U.; Shaikh, A.H. Prevention of dry socket in mandibular 3rd molars with single preoperative oral dose of metronidazole and amoxicillin compared to conventional therapy. J. Pak. Med. Assoc. 2021, 71, 585–589. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Kodama, Y.; Nishikawa, A.; Estacio Salazar, A.R.; Toyama, A.; Takagi, R. Comparison between the prophylactic effects of amoxicillin 24 and 48 hours pre-operatively on surgical site infections in Japanese patients with impacted mandibular third molars: A prospective cohort study. J. Infect. Chemother. 2021, 27, 845–851. [Google Scholar] [CrossRef] [PubMed]
- Yanine, N.; Sabelle, N.; Vergara-Gárate, V.; Salazar, J.; Araya-Cabello, I.; Carrasco-Labra, A.; Martin, C.; Villanueva, J. Effect of antibiotic prophylaxis for preventing infectious complications following impacted mandibular third molar surgery. A randomized controlled trial. Med. Oral Patol. Oral Cirugía Bucal 2021, 26, e703–e710. [Google Scholar] [CrossRef] [PubMed]
- Isiordia-Espinoza, M.A.; Aragon-Martinez, O.H.; Bollogna-Molina, R.E.; Alonso-Castro, Á.J. Infection, Alveolar Alveolar alveolar osteitis, and Adverse Effects Using Metronidazole in Healthy Patients Undergoing Third Molar Surgery: A Meta-analysis. J. Maxillofac. Oral Surg. 2018, 17, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Tarakji, B.; Saleh, L.A.; Umair, A.; Azzeghaiby, S.N.; Hanouneh, S. Systemic review of dry socket: Aetiology, treatment, and prevention. J. Clin. Diagn. Res. JCDR 2015, 9, ZE10–ZE13. [Google Scholar] [CrossRef]
- Thabit, A.K.; Fatani, D.F.; Bamakhrama, M.S.; Barnawi, O.A.; Basudan, L.O.; Alhejaili, S.F. Antibiotic penetration into bone and joints: An updated review. Int. J. Infect. Dis. 2019, 81, 128–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urbina, T.; Razazi, K.; Ourghanlian, C.; Woerther, P.L.; Chosidow, O.; Lepeule, R.; de Prost, N. Antibiotics in Necrotizing Soft Tissue Infections. Antibiotics 2021, 10, 1104. [Google Scholar] [CrossRef]
- Ghosh, A.; Aggarwal, V.R.; Moore, R. Aetiology, Prevention and Management of Alveolar Alveolar alveolar osteitis-A Scoping Review. J. Oral Rehabil. 2022, 49, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Al-Mahdi, R.; Malcolm, W.; Palmer, N.; Dahlen, G.; Al-Haroni, M. Comparison of antimicrobial prescribing for dental and oral infections in England and Scotland with Norway and Sweden and their relative contribution to national consumption 2010–2016. BMC Oral Health 2020, 20, 172. [Google Scholar] [CrossRef]
- Mellon, G.; Hammas, K.; Burdet, C.; Duval, X.; Carette, C.; El-Helali, N.; Massias, L.; Mentré, F.; Czernichow, S.; Crémieux, A.C. Population pharmacokinetics and dosing simulations of amoxicillin in obese adults receiving co-amoxiclav. J. Antimicrob. Chemother. 2020, 75, 3611–3618. [Google Scholar] [CrossRef] [PubMed]
- Veeraraghavan, B.; Bakthavatchalam, Y.D.; Sahni, R.D. Orally Administered Amoxicillin/Clavulanate: Current Role in Outpatient Therapy. Infect. Dis. Ther. 2021, 10, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Reichman, E.F. Reichman’s Emergency Medicine Procedures [Chapter 178. Post-Extraction Pain and Dry Socket (Alveolar Osteitis) Management], 3rd ed.; McGraw-Hill Education/Medical: New York, NY, USA, 2018. [Google Scholar]
- Bortoluzzi, M.C.L.; Capella, D.L.; Barbieri, T.; Pagliarini, M.; Cavalieri, T.; Manfro, R. A single dose of amoxicillin and dexamethasone for prevention of postoperative complications in third molar surgery: A randomized, double-blind, placebo controlled clinical trial. J. Clin. Med. Res. 2013, 5, 26–33. [Google Scholar] [PubMed] [Green Version]
- Gazal, G.; Aljohani, H.; Al-Samadani, K.H.; Nassani, M.Z. Measuring the Level of Medical-Emergency-Related Knowledge among Senior Dental Students and Clinical Trainers. Int. J. Environ. Res. Public Health 2021, 18, 6889. [Google Scholar] [CrossRef] [PubMed]
- Gazal, G. Management of an emergency tooth extraction in diabetic patients on the dental chair. Saudi Dent. J. 2020, 32, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Gazal, G. Surgical removal for khat inducible verruca vulgaris lesion of the oral mucosa. Niger. J. Clin. Pract. 2019, 22, 439–441. [Google Scholar] [CrossRef] [PubMed]
- Cabras, M.; Gambino, A.; Broccoletti, R.; Sciascia, S.; Arduino, P.G. Lack of evidence in reducing risk of MRONJ after teeth extractions with systemic antibiotics. J. Oral Sci. 2021, 63, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Amate, B.; Figueiredo, R.; Cortés-Peral, S.; Sánchez-Torres, A.; Valmaseda-Castellón, E. Patient perception about the need for antibiotics after tooth extractions: A cross-sectional study. J. Clin. Exp. Dent. 2021, 13, e499–e504. [Google Scholar] [CrossRef]
- Kiencało, A.; Jamka-Kasprzyk, M.; Panaś, M.; Wyszyńska-Pawelec, G. Analysis of complications after the removal of 339 third molars. Dent. Med. Probl. 2021, 58, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Delilbasi, C.; Saracoglu, U.; Keskin, A. Effects of 0.2% chlorhexidine gluconate and amoxicillin plus clavulanic acid on the prevention of alveolar osteitis following mandibular third molar extractions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2002, 94, 301–304. [Google Scholar] [CrossRef] [PubMed]
- Cinquini, C.; Marchionni, S.; Derchi, G.; Miccoli, M.; Gabriele, M.; Barone, A. Non-impacted tooth extractions and antibiotic treatment: A RCT study. Oral Dis. 2021, 27, 1042–1051. [Google Scholar] [CrossRef] [PubMed]
- Moratin, J.; Freudlsperger, C.; Metzger, K.; Braß, C.; Berger, M.; Engel, M.; Hoffmann, J.; Ristow, O. Development of osteomyelitis following dental abscesses-influence of therapy and comorbidities. Clin. Oral Investig. 2021, 25, 1395–1401. [Google Scholar] [CrossRef] [PubMed]
- Iguchi, R.; Moroi, A.; Saito, Y.; Takayama, A.; Hiraide, R.; Yoshizawa, K.; Ueki, K. Evaluation of intravenous prophylaxis antibiotics for third molar extraction under general anesthesia. Odontology 2020, 108, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Lodi, G.; Azzi, L.; Varoni, E.M.; Pentenero, M.; del Fabbro, M.; Carrassi, A.; Sardella, A.; Manfredi, M. Antibiotics to prevent complications following tooth extractions. Cochrane Database Syst. Rev. 2021, 2, CD003811. [Google Scholar] [CrossRef] [PubMed]
- Garola, F.; Gilligan, G.; Panico, R.; Leonardi, N.; Piemonte, E. Clinical management of alveolar osteitis. A systematic review. Med. Oral Patol. Oral Cirugía Bucal 2021, 26, e691–e702. [Google Scholar] [CrossRef] [PubMed]
- Esen, A. The effects of amoxicillin with or without clavulanic acid on the postoperative complaints after third molar surgery: A retrospective chart analysis. J. Istanb. Univ. Fac. Dent. 2017, 51, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Barone, A.; Marchionni, F.S.; Cinquini, C.; Cipolli Panattoni, A.; Toti, P.; Marconcini, S.; Covani, U.; Gabriele, M. Antibiotic treatment to prevent postextraction complications: A monocentric, randomized clinical trial. Preliminary outcomes. Minerva Stomatol. 2017, 66, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Chehabeddine, N.; Lahoud, N.; Noujeim, Z.E.F.; Zeidan, R.K.; El Toum, S.; Maison, P.; Saleh, N. An evaluation of prophylactic and therapeutic antibiotic prescribing in Lebanese dental practice. Int. J. Pharm. Pract. 2022, 30, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Pejicic, R.; Bichsel, D.; Valdec, S. Management der Alveolitis sicca/Ostitis circumscripta mit Socketol®-Paste [Management of the dry socket with Socketol® paste]. Swiss Dent. J. 2021, 131, 607–609. [Google Scholar] [PubMed]
- Blanco, C.; Pico, A.; Dopico, J.; Gándara, P.; Blanco, J.; Liñares, A. Adjunctive benefits of systemic metronidazole on non-surgical treatment of peri-implantitis. A randomized placebo-controlled clinical trial. J. Clin. Periodontol. 2022, 49, 15–27. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Treatment Groups | Number of Patients % 46 (100%) | X2 (DF = 2) | p-Value | |||
|---|---|---|---|---|---|---|
| Dry socket (DS) signs 5 days postoperatively | Empty socket | Co-amoxiclav 625 mg post-op | Yes | 4 (9%) | 0.672 | 0.715 |
| No | 12 (26%) | |||||
| Co-amoxiclav 625 mg pre-op + Metronidazole 500 mg post-op | Yes | 3 (7%) | ||||
| No | 12 (26%) | |||||
| Amoxiclv 625 mg pre-op + Amoxicillin 500 mg post-op | Yes | 2 (4%) | ||||
| No | 13 (28%) | |||||
| Bone exposure at the site of extraction | Co-amoxiclav 625 mg post-op | Yes | 2 (4%) | 0.399 | 0.819 | |
| No | 14 (31%) | |||||
| Co-amoxiclav 625 mg pre-op + Metronidazole 500 mg post-op | Yes | 3 (7%) | ||||
| No | 12 (26%) | |||||
| Amoxiclv 625 mg pre-op + Amoxicillin 500 mg post-op Yes | yes | 2 (4%) | ||||
| No | 13 (28%) | |||||
| Soft tissue inflammation | Co-amoxiclav 625 mg post-op | Yes | 6 (13%) | 2.349 | 0.309 | |
| No | 10 (22%) | |||||
| Co-amoxiclav 625 mg pre-op + Metronidazole 500 mg post-op | Yes | 2 (4%) | ||||
| No | 13 (28%) | |||||
| Amoxiclv 625 mg pre-op + Amoxicillin 500 mg post-op | Yes | 4 (9%) | ||||
| No | 11 (24%) | |||||
| Treatment Groups | Number of Patients % 46 (100%) | X2 (DF = 2) | p-Value | |||
|---|---|---|---|---|---|---|
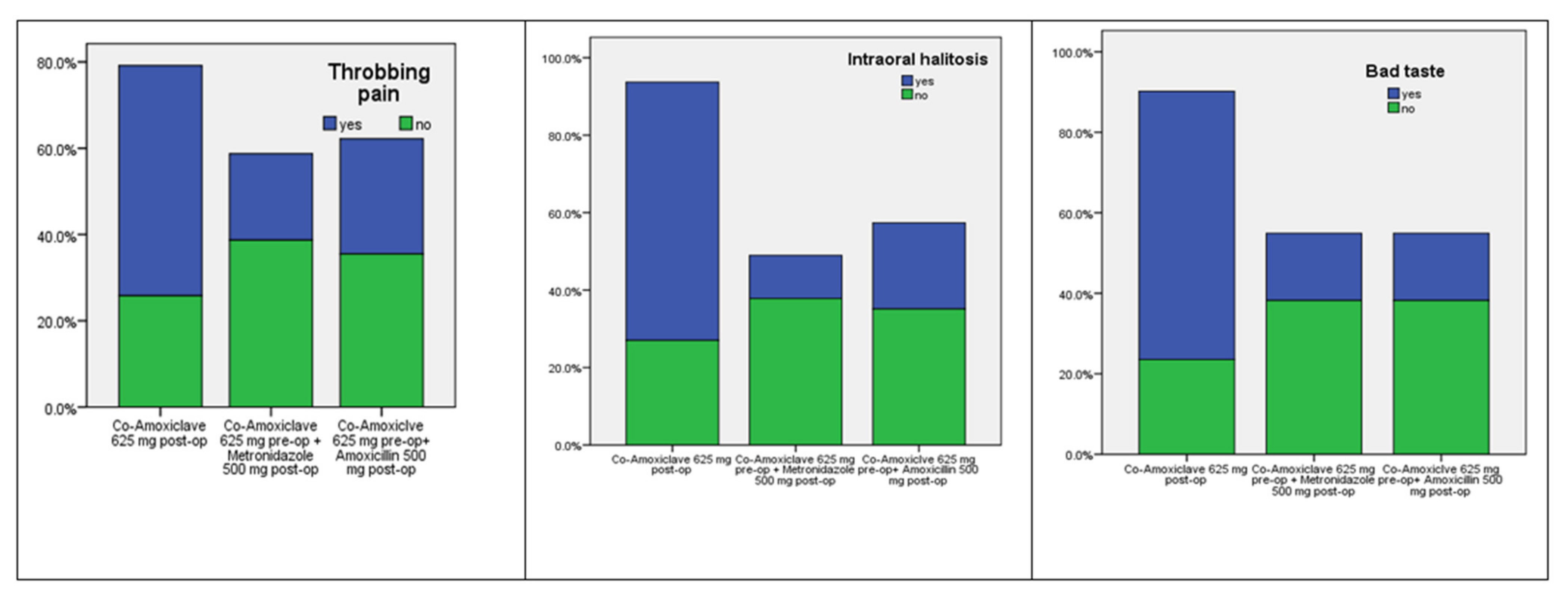
| Dry socket (DS) symptoms 5 days postoperatively | Throbbing pain | Co-amoxiclav 625 mg post-op | Yes | 8 (18%) | 3.53 | 0.171 |
| No | 8 (18%) | |||||
| Co-amoxiclav 625 mg pre-op + Metronidazole 500 mg post-op | Yes | 3 (7%) | ||||
| No | 12 (26%) | |||||
| Co-amoxiclav 625 mg pre-op + Amoxicillin 500 mg post-op | Yes | 4 (9%) | ||||
| No | 11 (24%) | |||||
| Intraoral halitosis | Co-amoxiclav 625 mg post-op | Yes | 6 (13%) | 5.23 | 0.073 | |
| No | 10 (22%) | |||||
| Co-amoxiclav 625 mg pre-op + Metronidazole 500 mg post-op | Yes | 1 (2%) | ||||
| No | 14 (31%) | |||||
| Co-amoxiclav 625 mg pre-op + Amoxicillin 500 mg post-op Yes | yes | 2 (4%) | ||||
| No | 13 (28%) | |||||
| Bad test | Co-amoxiclav 625 mg post-op | Yes | 8 (18%) | 7.28 | 0.026 | |
| No | 8 (18%) | |||||
| Co-amoxiclav 625 mg pre-op + Metronidazole 500 mg post-op | Yes | 2 (4%) | ||||
| No | 13 (28%) | |||||
| Co-amoxiclav 625 mg pre-op + Amoxicillin 500 mg post-op | Yes | 2 (4%) | ||||
| No | 13 (28%) | |||||
| Treatment Groups | Number of Patients % 46 (100%) | X2 (DF = 2) | p-Value | |||
|---|---|---|---|---|---|---|
| Surgical site infection (SSI) 5 days postoperatively | Oral swelling | Co-amoxiclav 625 mg post-op | Yes | 2 (4%) | 0.006 | 0.997 |
| No | 14 (32%) | |||||
| Co-amoxiclav 625 mg pre-op + Metronidazole 500 mg post-op | Yes | 2 (4%) | ||||
| No | 13 (28%) | |||||
| Co-amoxiclav 625 mg pre-op + Amoxicillin 500 mg post-op | Yes | 2 (4%) | ||||
| No | 13 (28%) | |||||
| Tenderness to touch | Co-amoxiclav 625 mg post-op | Yes | 5 (11%) | 5.517 | 0.063 | |
| No | 11 (23.5%) | |||||
| Co-amoxiclav 625 mg pre-op + Metronidazole 500 mg post-op | Yes | 0 (0%) | ||||
| No | 15 (33%) | |||||
| Amoxiclv 625 mg pre-op + Amoxicillin 500 mg post-op | yes | 4 (9%) | ||||
| No | 11 (23.5%) | |||||
| Drainage of pus | Co-amoxiclav 625 mg post-op | Yes | 1 (2%) | 1.917 | 0.384 | |
| No | 15 (32.7%) | |||||
| Co-amoxiclav 625 mg pre-op + Metronidazole 500 mg post-op | Yes | 0 (0%) | ||||
| No | 15 (32.7%) | |||||
| Amoxiclv 625 mg pre-op + Amoxicillin 500 mg post-op | Yes | 0 (0%) | ||||
| No | 15 (32.7%) | |||||
| Limitation of mouth opening | Co-amoxiclav 625 mg post-op | Yes | 4(9%) | 2.078 | 0.354 | |
| No | 12(26%) | |||||
| Co-amoxiclav 625 mg pre-op + Metronidazole 500 mg post-op | Yes | 2(4%) | ||||
| No | 13(28%) | |||||
| Amoxiclv 625 mg pre-op + Amoxicillin 500 mg post-op | Yes | 1(2%) | ||||
| No | 14(31%) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gazal, G.; Al-Samadani, K.H.; Alsaidalani, H.M.; Karbouji, G.A.; Alharbi, A.M. A Comparison of Pre-Emptive Co-Amoxiclav, Postoperative Amoxicillin, and Metronidazole for Prevention of Postoperative Complications in Dentoalveolar Surgery: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 4178. https://doi.org/10.3390/ijerph19074178
Gazal G, Al-Samadani KH, Alsaidalani HM, Karbouji GA, Alharbi AM. A Comparison of Pre-Emptive Co-Amoxiclav, Postoperative Amoxicillin, and Metronidazole for Prevention of Postoperative Complications in Dentoalveolar Surgery: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(7):4178. https://doi.org/10.3390/ijerph19074178
Chicago/Turabian StyleGazal, Giath, Khalid H. Al-Samadani, Hamdi Mohammed Alsaidalani, Ghofran Ali Karbouji, and Abdullah Mohammed Alharbi. 2022. "A Comparison of Pre-Emptive Co-Amoxiclav, Postoperative Amoxicillin, and Metronidazole for Prevention of Postoperative Complications in Dentoalveolar Surgery: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 7: 4178. https://doi.org/10.3390/ijerph19074178
APA StyleGazal, G., Al-Samadani, K. H., Alsaidalani, H. M., Karbouji, G. A., & Alharbi, A. M. (2022). A Comparison of Pre-Emptive Co-Amoxiclav, Postoperative Amoxicillin, and Metronidazole for Prevention of Postoperative Complications in Dentoalveolar Surgery: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 19(7), 4178. https://doi.org/10.3390/ijerph19074178