
Standardising Training of Nurses in an Evidence-Based Psychosocial Intervention for Perinatal Depression: Randomized Trial of Electronic vs. Face-to-Face Training in China

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participant Flow and Numbers Analysed
2.3. Settings and Participants
Demographic Characteristics of Participants
2.4. Sample Size, Sampling Method, and Inclusion Criteria
2.5. Randomization and Masking
2.6. Intervention Arm: E-Training in the Thinking Healthy Programme
2.7. Control Arm—Conventional Specialist-Delivered Training
2.8. Measurements
2.9. Primary Outcome
2.10. Secondary Outcomes
2.10.1. Counsellor Self-Efficacy
2.10.2. Attitudes and Beliefs
2.10.3. Satisfaction with Training
2.11. Data Collection Procedures
2.12. Statistical Analysis
3. Results
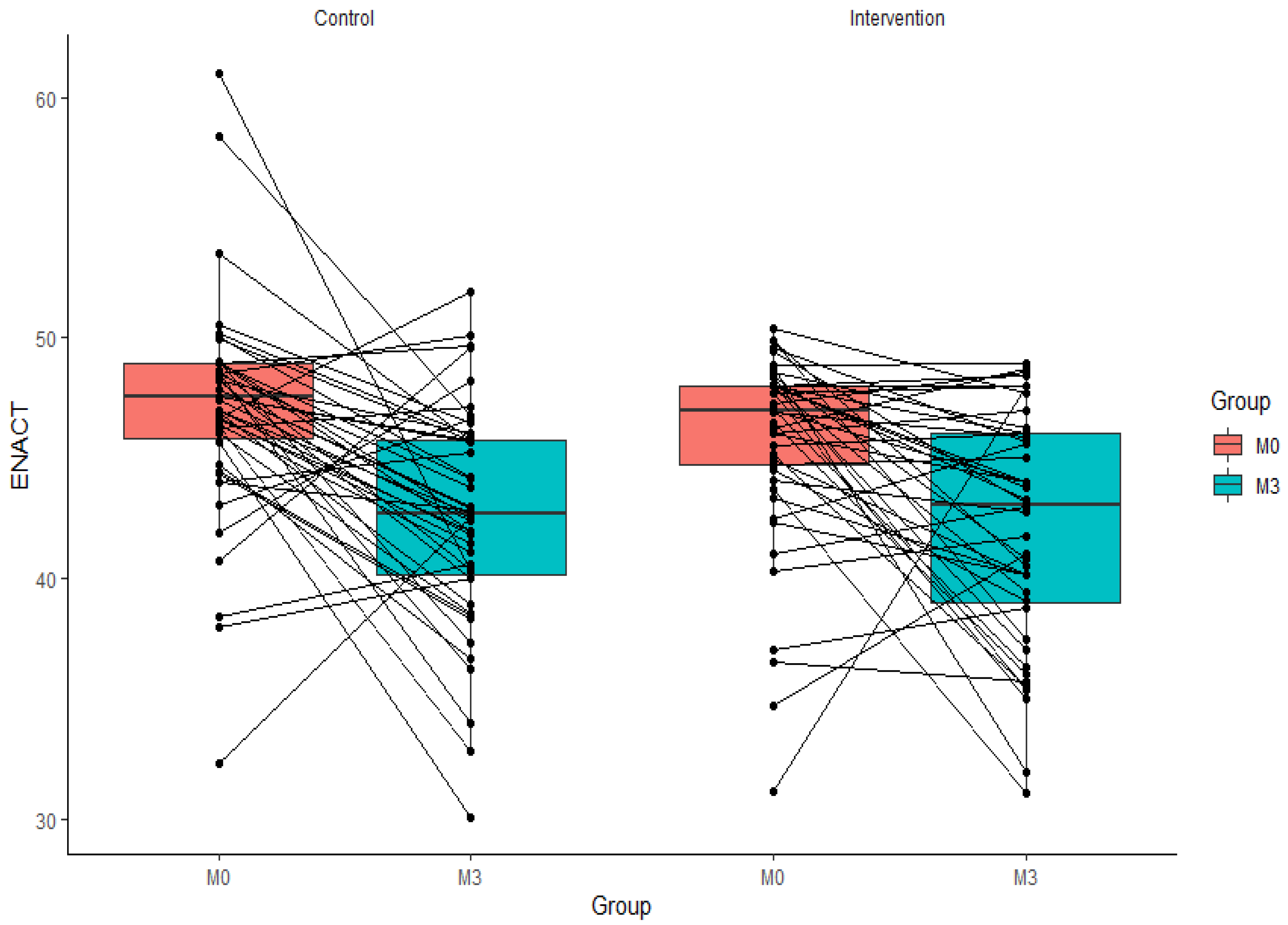
3.1. Training Competency in the Thinking Healthy Programme
3.2. Attitudes and Beliefs about Perinatal Depression
3.3. Self-Efficacy
3.4. Satisfaction with Training
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gelaye, B.; Rondon, M.B.; Araya, R.; Williams, M.A. Epidemiology of maternal depression, risk factors, and child outcomes in low-income and middle-income countries. Lancet Psychiatry 2016, 3, 973–982. [Google Scholar] [CrossRef]
- Nisar, A.; Yin, J.; Waqas, A.; Bai, X.; Wang, D.; Rahman, A.; Li, X. Prevalence of perinatal depression and its determinants in Mainland China: A systematic review and meta-analysis. J. Affect. Disord. 2020, 277, 1022–1037. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Zhang, C.; Liu, H.; Duan, C.; Li, C.; Fan, J.; Li, H.; Chen, L.; Xu, H.; Li, X. Perinatal depressive and anxiety symptoms of pregnant women during the coronavirus disease 2019 outbreak in China. Am. J. Obstet. Gynecol. 2020, 223, 240.e1–240.e9. [Google Scholar] [CrossRef] [PubMed]
- Atif, N.; Lovell, K.; Rahman, A. Maternal mental health: The missing “m” in the global maternal and child health agenda. Semin. Perinatol. 2015, 39, 345–352. [Google Scholar] [CrossRef]
- Psychiatric institutions in China. Lancet 2010, 376, P2. [CrossRef]
- Liu, S.; Page, A. Reforming mental health in China and India. Lancet 2016, 388, 314–316. [Google Scholar] [CrossRef]
- Xiang, Y.-T.; Yu, X.; Sartorius, N.; Ungvari, G.S.; Chiu, H.F.K. Mental health in China: Challenges and progress. Lancet 2012, 380, 1715–1716. [Google Scholar] [CrossRef]
- Xiong, W.; Phillips, M.R. Translated and annotated version of the 2015–2020 National Mental Health Work Plan of the People’s Republic of China. Shanghai Arch. Psychiatry 2016, 28, 4–17. [Google Scholar]
- Xu, X.; Li, X.-M.; Xu, D.; Wang, W. Psychiatric and mental health nursing in China: Past, present and future. Arch. Psychiatr. Nurs. 2017, 31, 470–476. [Google Scholar] [CrossRef]
- Singla, D.R.; Kohrt, B.A.; Murray, L.K.; Anand, A.; Chorpita, B.F.; Patel, V. Psychological treatments for the world: Lessons from low-and middle-income countries. Annu. Rev. Clin. Psychol. 2017, 13, 149–181. [Google Scholar] [CrossRef]
- Josephine, K.; Josefine, L.; Philipp, D.; David, E.; Harald, B. Internet-and mobile-based depression interventions for people with diagnosed depression: A systematic review and meta-analysis. J. Affect. Disord. 2017, 223, 28–40. [Google Scholar] [CrossRef]
- Naslund, J.A.; Aschbrenner, K.A.; Araya, R.; Marsch, L.A.; Unützer, J.; Patel, V.; Bartels, S.J. Digital technology for treating and preventing mental disorders in low-income and middle-income countries: A narrative review of the literature. Lancet Psychiatry 2017, 4, 486–500. [Google Scholar] [CrossRef]
- Rahman, A.; Surkan, P.J.; Cayetano, C.E.; Rwagatare, P.; Dickson, K.E. Grand challenges: Integrating maternal mental health into maternal and child health programmes. PLoS Med. 2013, 10, e1001442. [Google Scholar] [CrossRef]
- Rahman, A.; Fisher, J.; Bower, P.; Luchters, S.; Tran, T.; Yasamy, M.T.; Saxena, S.; Waheed, W. Interventions for common perinatal mental disorders in women in low-and middle-income countries: A systematic review and meta-analysis. Bull. World Health Organ. 2013, 91, 593–601. [Google Scholar] [CrossRef]
- Rahman, A.; Malik, A.; Sikander, S.; Roberts, C.; Creed, F. Cognitive behaviour therapy-based intervention by community health workers for mothers with depression and their infants in rural Pakistan: A cluster-randomised controlled trial. Lancet 2008, 372, 902–909. [Google Scholar] [CrossRef]
- Nisar, A.; Yin, J.; Yiping, N.; Lanting, H.; Zhang, J.; Wang, D.; Rahman, A.; Li, X. Making therapies culturally relevant: Translation, cultural adaptation and field-testing of the Thinking Healthy Programme for perinatal depression in China. BMC Pregnancy Childbirth 2020, 20, 368. [Google Scholar] [CrossRef]
- Rahman, A. Challenges and opportunities in developing a psychological intervention for perinatal depression in rural Pakistan—A multi-method study. Arch. Women Ment. Health 2007, 10, 211–219. [Google Scholar] [CrossRef]
- Rahman, A.; Waqas, A.; Nisar, A.; Nazir, H.; Sikander, S.; Atif, N. Improving access to psychosocial interventions for perinatal depression in low-and middle-income countries: Lessons from the field. Int. Rev. Psychiatry 2021, 33, 198–201. [Google Scholar] [CrossRef]
- Rahman, A.; Akhtar, P.; Hamdani, S.U.; Atif, N.; Nazir, H.; Uddin, I.; Nisar, A.; Huma, Z.; Maselko, J.; Sikander, S.; et al. Using technology to scale-up training and supervision of community health workers in the psychosocial management of perinatal depression: A non-inferiority, randomized controlled trial. Glob. Ment. Health 2019, 6, e8. [Google Scholar] [CrossRef]
- Kobak, K.A.; Craske, M.G.; Rose, R.D.; Wolitsky-Taylor, K. Web-based therapist training on cognitive behavior therapy for anxiety disorders: A pilot study. Psychotherapy 2013, 50, 235. [Google Scholar] [CrossRef]
- Leykin, Y.; Cucciare, M.A.; Weingardt, K.R. Differential effects of online training on job-related burnout among substance abuse counsellors. J. Subst. Use 2011, 16, 127–135. [Google Scholar] [CrossRef]
- Puspitasari, A.; Kanter, J.W.; Murphy, J.; Crowe, A.; Koerner, K. Developing an online, modular, active learning training program for behavioral activation. Psychotherapy 2013, 50, 256. [Google Scholar] [CrossRef][Green Version]
- Jackson, C.B.; Quetsch, L.B.; Brabson, L.A.; Herschell, A.D. Web-based training methods for behavioral health providers: A systematic review. Adm. Policy Ment. Health Ment. Health Serv. Res. 2018, 45, 587–610. [Google Scholar] [CrossRef]
- Xi’an Statistical Yearbook. Available online: https://www.chinayearbooks.com/xian-statistical-yearbook-2017.html (accessed on 29 December 2021).
- Stirman, S.W.; Miller, C.J.; Toder, K.; Calloway, A. Development of a framework and coding system for modifications and adaptations of evidence-based interventions. Implement. Sci. 2013, 8, 65. [Google Scholar] [CrossRef]
- Valenstein-Mah, H.; Greer, N.; McKenzie, L.; Hansen, L.; Strom, T.Q.; Stirman, S.W.; Wilt, T.J.; Kehle-Forbes, S.M. Effectiveness of training methods for delivery of evidence-based psychotherapies: A systematic review. Implement. Sci. 2020, 15, 40. [Google Scholar] [CrossRef]
- Kohrt, B.A.; Jordans, M.J.D.; Rai, S.; Shrestha, P.; Luitel, N.P.; Ramaiya, M.K.; Singla, D.R.; Patel, V. Therapist competence in global mental health: Development of the ENhancing Assessment of Common Therapeutic factors (ENACT) rating scale. Behav. Res. 2015, 69, 11–21. [Google Scholar] [CrossRef]
- McBride, K.A.; Harrison, S.; Mahata, S.; Pfeffer, K.; Cardamone, F.; Ngigi, T.; Kohrt, B.A.; Pedersen, G.A.; Greene, C.; Viljoen, D. Building mental health and psychosocial support capacity during a pandemic: The process of adapting problem management plus for remote training and implementation during COVID-19 in New York city, Europe and east africa. Intervention 2021, 19, 37–47. [Google Scholar]
- Sangraula, M.; Turner, E.; Luitel, N.; van‘t Hof, E.; Shrestha, P.; Ghimire, R.; Bryant, R.; Marahatta, K.; Van Ommeren, M.; Kohrt, B.A. Feasibility of Group Problem Management Plus (PM+) to improve mental health and functioning of adults in earthquake-affected communities in Nepal. Epidemiol. Psychiatr. Sci. 2020, 29, e130. [Google Scholar] [CrossRef]
- Asher, L.; Birhane, R.; Teferra, S.; Milkias, B.; Worku, B.; Habtamu, A.; Kohrt, B.A.; Hanlon, C. “Like a doctor, like a brother”: Achieving competence amongst lay health workers delivering community-based rehabilitation for people with schizophrenia in Ethiopia. PLoS ONE 2021, 16, e0246158. [Google Scholar] [CrossRef]
- Atif, N.; Bibi, A.; Nisar, A.; Zulfiqar, S.; Ahmed, I.; LeMasters, K.; Hagaman, A.; Sikander, S.; Maselko, J.; Rahman, A. Delivering maternal mental health through peer volunteers: A 5-year report. Int. J. Ment. Health Syst. 2019, 13, 1–8. [Google Scholar] [CrossRef]
- Lent, R.W.; Hill, C.E.; Hoffman, M.A. Development and validation of the Counselor Activity Self-Efficacy Scales. J. Couns. Psychol. 2003, 50, 97–108. [Google Scholar] [CrossRef]
- Peters, G.-J. The Alpha and the Omega of Scale Reliability and Validity: Why and how to Abandon Cronbach’ s Alpha. Eur. Health Psychol. 2014, 16, 576. [Google Scholar]
- Highet, N.J.; Gemmill, A.W.; Milgrom, J. Depression in the perinatal period: Awareness, attitudes and knowledge in the Australian population. Aust. N. Z. J. Psychiatry 2011, 45, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Sitzmann, T.; Kraiger, K.; Stewart, D.; Wisher, R. The comparative effectiveness of web-based and classroom instruction: A meta-analysis. Pers. Psychol. 2006, 59, 623–664. [Google Scholar] [CrossRef]
- Means, B.; Toyama, Y.; Murphy, R.; Bakia, M.; Jones, K. Evaluation of Evidence-Based Practices in Online Learning: A Meta-Analysis and Review of Online Learning Studies; US Department of Education: Washington, DC, USA, 2009. Available online: https://www2.ed.gov/rschstat/eval/tech/evidence-based-practices/finalreport.pdf (accessed on 29 December 2021).
- Murray, L.K.; Dorsey, S.; Bolton, P.; Jordans, M.J.D.; Rahman, A.; Bass, J.; Verdeli, H. Building capacity in mental health interventions in low resource countries: An apprenticeship model for training local providers. Int. J. Ment. Health Syst. 2011, 5, 30. [Google Scholar] [CrossRef]
- Atif, N.; Nisar, A.; Bibi, A.; Khan, S.; Zulfiqar, S.; Ahmad, I.; Sikander, S.; Rahman, A. Scaling-up psychological interventions in resource-poor settings: Training and supervising peer volunteers to deliver the ‘Thinking Healthy Programme’ for perinatal depression in rural Pakistan. Glob. Ment. Health 2019, 6, e4. [Google Scholar] [CrossRef]
- Mutamba, B.B.; van Ginneken, N.; Paintain, L.S.; Wandiembe, S.; Schellenberg, D. Roles and effectiveness of lay community health workers in the prevention of mental, neurological and substance use disorders in low and middle income countries: A systematic review. BMC Health Serv. Res. 2013, 13, 412. [Google Scholar] [CrossRef]
- Tuckson, R.V.; Edmunds, M.; Hodgkins, M.L. Telehealth. N. Engl. J. Med. 2017, 377, 1585–1592. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | E-Training (n = 50) | Specialist Led Training (n = 50) | p-Value |
|---|---|---|---|
| Mean age (SD), Median (IQR) | 20 (1.94); 20 (18–22) | 19.45 (1.57); 19 (18–21) | 0.13 |
| Gender | 0.08 | ||
| Male | 7 (14.9%) | 14 (29.8%) | |
| Female | 40 (85.1%) | 33 (70.2%) | |
| Grade | 0.09 | ||
| Year 1 | 23 (48.9%) | 31 (66.0%) | |
| Year 4 | 24 (51.1%) | 16 (34.0%) | |
| Work experience (n [%]) * | 1.00 | ||
| Yes | 10 (21.3%) | 10 (21.3%) | |
| No | 37 (78.7%) | 37 (78.7%) | |
| Prior mental health training (n [%]) ** | 10.12 | 11.02 | 0.61 |
| Yes | 3 (6.4%) | 1 (2.1%) | |
| No | 44 (93.6%) | 46 (97.9%) | |
| Knowledge of perinatal depression ** | 17.04 (1.40) | 17.23 (1.13) | 0.43 |
| Generalized Linear Mixed Model Analysis * | ||||||
|---|---|---|---|---|---|---|
| Primary Analysis | Covariate Analysis | Imputation Analysis | ||||
| Mean Difference (95% CI) | p-Value | Mean Difference (95% CI) | p-Value | Mean Difference (95% CI) | p-Value | |
| ENACT Scores | ||||||
| Post-training | −1.35 (−3.17, 0.46) | 0.14 | −1.20 (−3.05, 0.65) | 0.20 | −1.18 (−3.04, 0.66) | 0.20 |
| Post 3 months | −0.48 (−2.35, 1.39) | 0.61 | −0.32 (−2.23, 1.59) | 0.73 | 0.16 (−1.69, 2.01) | 0.86 |
| Attitude and beliefs scores | ||||||
| Post-training | 2.149 (−1.338, 5.636) | 0.22 | 0.49 (0.01, 0.98) | 0.16 | 0.48 (0.05, 0.92) | 0.28 |
| Post 3 months | −1.686 (−5.358, 1.986) | 0.36 | −1.544 (−5.275, 2.188) | 0.41 | −1.532 (−5.080, 2.015) | 0.39 |
| Self-Efficacy scores | ||||||
| Post-training | −19.13 (39.54, 1.27) | 0.06 | −16.44 (−37.23, 4.34) | 0.11 | −15.93 (−35.71, 3.84) | 0.11 |
| Post 3 months | −9.17 (−30.44, 12.08) | 0.39 | −6.52 (−28.22, 15.16) | 0.55 | −7.24 (−27.02, 12.53) | 0.46 |
| Category | Outcome | Month | Statistics | E-Training | Specialist Led Training | All |
|---|---|---|---|---|---|---|
| Primary outcome | ENACT | Post training | n, mean (SD) | 49, 45.73 (4.03) | 47, 47.08 (4.53) | 96, 46.39 (4.31) |
| Post 3 months | n, mean (SD) | 44, 42.16 (4.85) | 47, 42.65 (4.56) | 91, 42.41 (4.68) | ||
| Secondary outcome | Attitude and Beliefs | Post training | n, mean (SD) | 47, 32.81 (8.60) | 47, 30.66 (7.38) | 94, 31.73 (8.04) |
| Post 3 months | n, mean (SD) | 40, 31.78 (7.72) | 45, 33.47 (10.01) | 85, 32.67 (9.00) | ||
| Self-efficacy | Post training | n, mean (SD) | 47, 159.11 (53.88) | 45, 178.24 (40.78) | 92, 168.47 (48.62) | |
| Post 3 months | n, mean (SD) | 40, 178.20 (54.19) | 45, 187.38 (47.05) | 85, 183.06 (50.44) |
| Variable | Subgroup | Mean Difference | n | Estimate (95% CI) | p-Value |
|---|---|---|---|---|---|
| Age | <19 | A vs. B at month 0 | 52 | −1.19 (−3.83, 1.44) | 0.36 |
| A vs. B at month 3 | 52 | −0.86 (−3.63, 1.89) | 0.53 | ||
| ≥19 | A vs. B at month 0 | 44 | −1.51 (−4.13, 1.09) | 0.24 | |
| A vs. B at month 3 | 44 | −0.28 (−2.92, 2.39) | 0.82 | ||
| Gender | Male | A vs. B at month 0 | 21 | −1.26 (−5.47, 2.95) | 0.53 |
| A vs. B at month 3 | 21 | −0.51 (−4.72, 3.69) | 0.80 | ||
| Female | A vs. B at month 0 | 75 | −1.18 (−3.31, 0.94) | 0.26 | |
| A vs. B at month 3 | 75 | −0.41 (−2.60, 1.77) | 0.70 | ||
| Grade | 1st year | A vs. B at month 0 | 56 | −1.04 (−3.52, 1.43) | 0.40 |
| A vs. B at month 3 | 56 | −0.35 (−3.00, 2.28) | 0.78 | ||
| 4th year | A vs. B at month 0 | 40 | −1.66 (−4.58, 1.25) | 0.25 | |
| A vs. B at month 3 | 40 | −0.76 (−3.67, 2.15) | 0.59 | ||
| Work experience | Yes | A vs. B at month 0 | 20 | −1.34 (−4.53, 1.85) | 0.38 |
| A vs. B at month 3 | 20 | −1.08 (−4.36, 2.18) | 0.49 | ||
| No | A vs. B at month 0 | 76 | −1.34 (−3.51, 0.82) | 0.22 | |
| A vs. B at month 3 | 76 | −0.30 (−2.53, 1.92) | 0.78 |
| Primary Analysis * | Covariate Analysis ** | Imputation Analysis **† | |||||
|---|---|---|---|---|---|---|---|
| Outcome | Odds Ratio | Estimate (95% CI) | p-Value | Estimate (95% CI) | p-Value | Estimate (95% CI) | p-Value |
| ENACT (≥43) | A vs. B at month 0 | 0.61 (0.17, 2.10) | 0.42 | 0.59 (0.16, 2.10) | 0.41 | 0.59 (0.16, 2.12) | 0.42 |
| A vs. B at month 3 | 1.36 (0.57, 3.26) | 0.47 | 1.33 (0.53, 3.37) | 0.53 | 1.67 (0.67, 4.15) | 0.26 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nisar, A.; Yin, J.; Nan, Y.; Luo, H.; Han, D.; Yang, L.; Li, J.; Wang, D.; Rahman, A.; Li, X. Standardising Training of Nurses in an Evidence-Based Psychosocial Intervention for Perinatal Depression: Randomized Trial of Electronic vs. Face-to-Face Training in China. Int. J. Environ. Res. Public Health 2022, 19, 4094. https://doi.org/10.3390/ijerph19074094
Nisar A, Yin J, Nan Y, Luo H, Han D, Yang L, Li J, Wang D, Rahman A, Li X. Standardising Training of Nurses in an Evidence-Based Psychosocial Intervention for Perinatal Depression: Randomized Trial of Electronic vs. Face-to-Face Training in China. International Journal of Environmental Research and Public Health. 2022; 19(7):4094. https://doi.org/10.3390/ijerph19074094
Chicago/Turabian StyleNisar, Anum, Juan Yin, Yiping Nan, Huanyuan Luo, Dongfang Han, Lei Yang, Jiaying Li, Duolao Wang, Atif Rahman, and Xiaomei Li. 2022. "Standardising Training of Nurses in an Evidence-Based Psychosocial Intervention for Perinatal Depression: Randomized Trial of Electronic vs. Face-to-Face Training in China" International Journal of Environmental Research and Public Health 19, no. 7: 4094. https://doi.org/10.3390/ijerph19074094
APA StyleNisar, A., Yin, J., Nan, Y., Luo, H., Han, D., Yang, L., Li, J., Wang, D., Rahman, A., & Li, X. (2022). Standardising Training of Nurses in an Evidence-Based Psychosocial Intervention for Perinatal Depression: Randomized Trial of Electronic vs. Face-to-Face Training in China. International Journal of Environmental Research and Public Health, 19(7), 4094. https://doi.org/10.3390/ijerph19074094