
Influence of Socio-Economic Factors and Region of Birth on the Risk of Preeclampsia in Sweden



Abstract
:1. Background
2. Materials and Methods
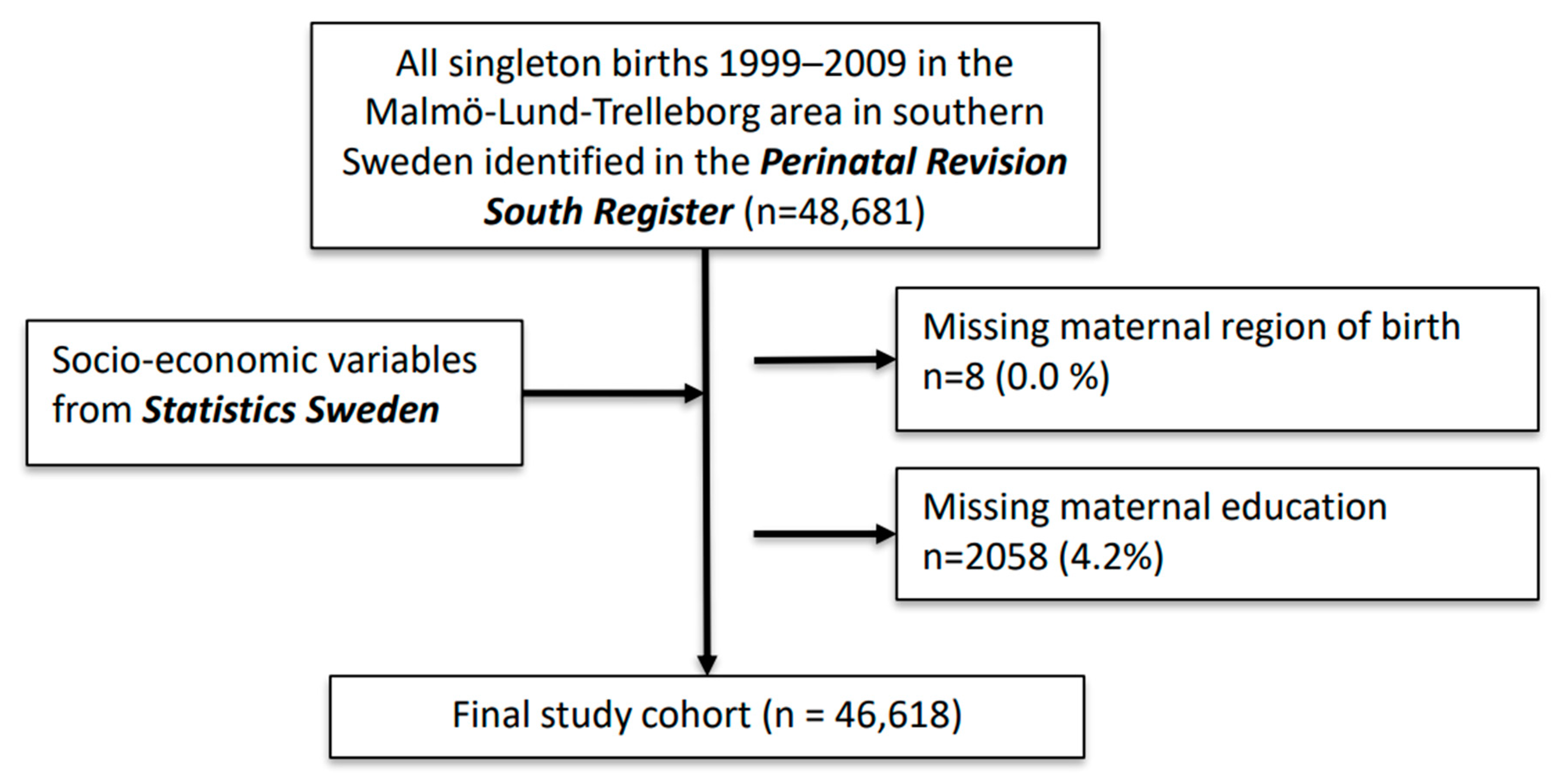
2.1. Data Sources and Study Population
2.2. Outcomes
2.3. Exposure Assessment—Socio-Economic Measures
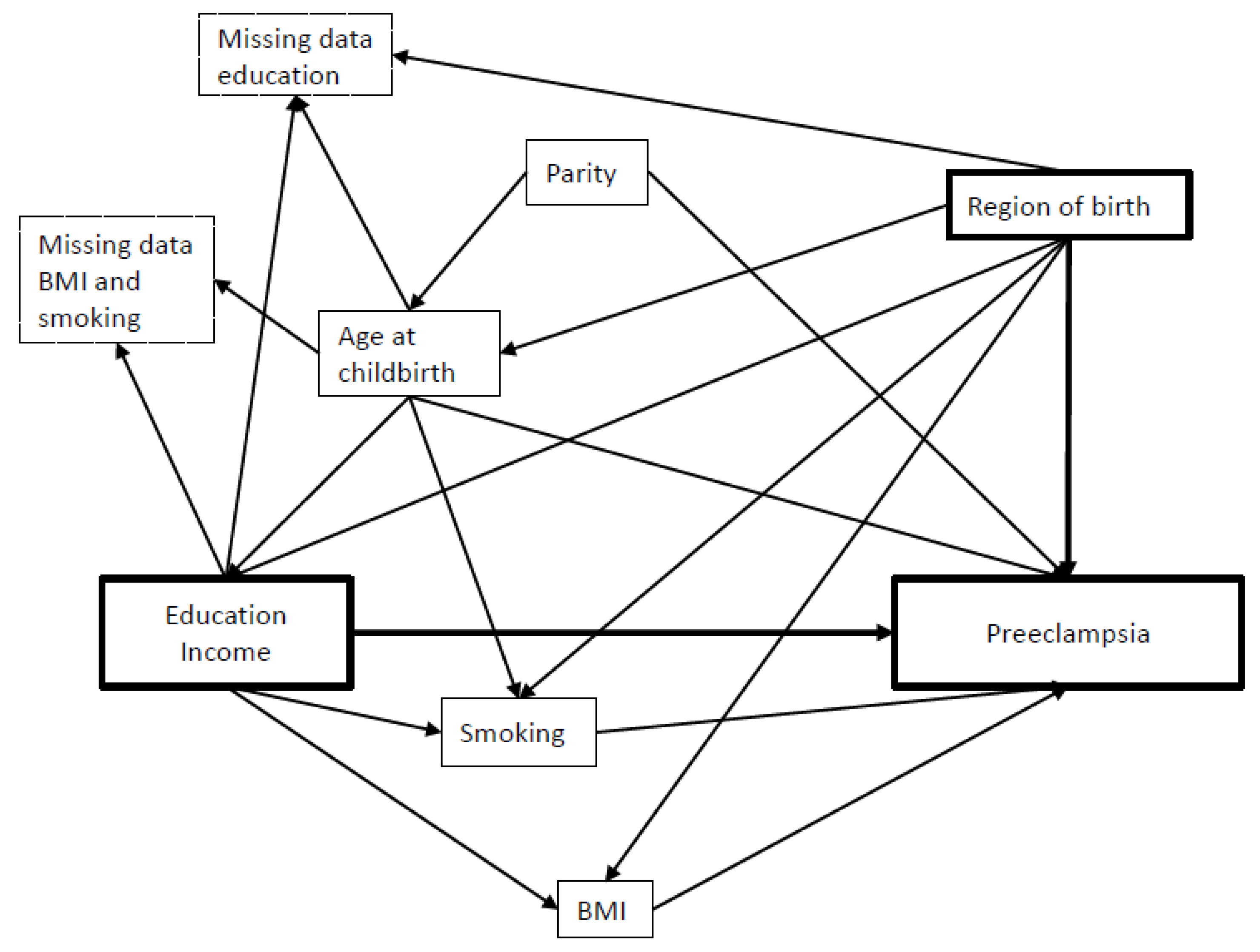
2.4. Covariates
Missing Data
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Duley, L. The Global Impact of Pre-eclampsia and Eclampsia. Semin. Perinatol. 2009, 33, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Esscher, A.; Haglund, B.; Högberg, U.; Essén, B. Excess mortality in women of reproductive age from low-income countries: A Swedish national register study. Eur. J. Public Health 2012, 23, 274–279. [Google Scholar] [CrossRef]
- Ekéus, C.; Cnattingius, S.; Essén, B.; Hjern, A. Stillbirth among foreign-born women in Sweden. Eur. J. Public Health 2011, 21, 788–792. [Google Scholar] [CrossRef] [Green Version]
- Wahlberg, Å.; Rööst, M.; Haglund, B.; Högberg, U.; Essén, B. Increased risk of severe maternal morbidity (near-miss) among immigrant women in Sweden: A population register-based study. BJOG Int. J. Obstet. Gynaecol. 2013, 120, 1605–1612. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Lee, S.M.; Bae, S.-H.; Kim, H.J.; Lim, N.G.; Yoon, S.-J.; Lee, J.Y.; Jo, M.-W. Socioeconomic status can affect pregnancy outcomes and complications, even with a universal healthcare system. Int. J. Equity Health 2018, 17, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haelterman, E.; Qvist, R.; Barlow, P.; Alexander, S. Social deprivation and poor access to care as risk factors for severe pre-eclampsia. Eur. J. Obstet. Gynecol. Reprod. Biol. 2003, 111, 25–32. [Google Scholar] [CrossRef]
- Choe, S.A.; Min, H.S.; Cho, S.I. The income-based disparities in preeclampsia and postpartum hemorrhage: A study of the Ko-rean National Health Insurance cohort data from 2002 to 2013. Springerplus 2016, 5, 895. [Google Scholar] [CrossRef] [Green Version]
- Silva, L.M.; Coolman, M.; Steegers, E.A.P.; Jaddoe, V.W.V.; Moll, H.A.; Hofman, A.; Mackenbach, J.P.; Raat, H. Low socioeconomic status is a risk factor for preeclampsia: The Generation R Study. J. Hypertens. 2008, 26, 1200–1208. [Google Scholar] [CrossRef]
- Heshmati, A.; Mishra, G.; Koupil, I. Childhood and adulthood socio-economic position and hypertensive disorders in preg-nancy: The Uppsala Birth Cohort Multigenerational Study. J. Epidemiol. Community Health 2013, 67, 939–946. [Google Scholar] [CrossRef]
- Lawlor, D.A.; Morton, S.M.; Nitsch, D.; Leon, D.A. Association between childhood and adulthood socioeconomic position and pregnancy induced hypertension: Results from the Aberdeen children of the 1950s cohort study. J. Epidemiol. Community Health 2005, 59, 49–55. [Google Scholar] [CrossRef] [Green Version]
- Lisonkova, S.; Joseph, K.S. Incidence of preeclampsia: Risk factors and outcomes associated with early- versus late-onset dis-ease. Am. J. Obstet. Gynecol. 2013, 209, 544.e1–544.e12. [Google Scholar] [CrossRef] [PubMed]
- Haelterman, E.; Marcoux, S.; Croteau, A.; Dramaix, M. Population-based study on occupational risk factors for preeclampsia and gestational hypertension. Scand. J. Work. Environ. Health 2007, 33, 304–317. [Google Scholar] [CrossRef] [Green Version]
- Lisonkova, S.; Sabr, Y.; Mayer, C.; Young, C.; Skoll, A.; Joseph, K. Maternal Morbidity Associated With Early-Onset and Late-Onset Preeclampsia. Obstet. Gynecol. 2014, 124, 771–781. [Google Scholar] [CrossRef] [PubMed]
- Jaatinen, N.; Jääskeläinen, T.; Laivuori, H.; Ekholm, E. The non-traditional and familial risk factors for preeclampsia in the FINNPEC cohort. Pregnancy Hypertens. 2021, 23, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Jwa, S.C.; Fujiwara, T.; Hata, A.; Arata, N.; Sago, H.; Ohya, Y. BMI mediates the association between low educational level and higher blood pressure during pregnancy in Japan. BMC Public Health 2013, 13, 389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, L.M.; Coolman, M.; Steegers, E.A.P.; Jaddoe, V.W.V.; Moll, H.A.; Hofman, A.; Mackenbach, J.P.; Raat, H. Maternal educa-tional level and risk of gestational hypertension: The Generation R Study. J. Hum. Hypertens. 2008, 22, 483–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gudmundsson, S.; Björgvinsdóttir, L.; Molin, J.; Gunnarsson, G.; Marsal, K. Socioeconomic status and perinatal outcome ac-cording to residence area in the city of Malmö. Acta Obstet. Gynecol. Scand. 1997, 76, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, G.; Grewal, J.; Männistö, T.; Mendola, P.; Chen, Z.; Xie, Y.; Laughon, S.K. Racial/ethnic differences in pregnancy-related hypertensive disease in nulliparous women. Ethn. Dis. 2014, 24, 283–289. [Google Scholar]
- Racapé, J.; Schoenborn, C.; Sow, M.; Alexander, S.; De Spiegelaere, M. Are all immigrant mothers really at risk of low birth weight and perinatal mortality? The crucial role of socio-economic status. BMC Pregnancy Childbirth 2016, 16, 75. [Google Scholar] [CrossRef] [Green Version]
- Villalonga-Olives, E.; Kawachi, I.; Von Steinbüchel, N. Pregnancy and Birth Outcomes Among Immigrant Women in the US and Europe: A Systematic Review. J. Immigr. Minor. Health 2017, 19, 1469–1487. [Google Scholar] [CrossRef]
- Carr, A.; Kershaw, T.; Brown, H.; Allen, T.; Small, M. Hypertensive disease in pregnancy: An examination of ethnic differences and the Hispanic paradox. J. Neonatal-Perinat. Med. 2013, 6, 11–15. [Google Scholar] [CrossRef] [PubMed]
- National Board of Health and Welfare. Normer för Ekonomiskt Bistånd (Socialbidrag) 1985–2005; National Board of Health and Welfare: Stockholm, Sweden, 2009. [Google Scholar]
- A Hughes, R.; Heron, J.; Sterne, J.; Tilling, K. Accounting for missing data in statistical analyses: Multiple imputation is not always the answer. Int. J. Epidemiol. 2019, 48, 1294–1304. [Google Scholar] [CrossRef] [PubMed]
- Darj, E.; Lindmark, G. Mödrahälsovården utnyttjas inte av alla gravida kvinnor. Läkartidningen 2002, 99, 41–44. [Google Scholar] [PubMed]
- Galobardes, B.; Shaw, M.; Lawlor, D.A.; Lynch, J.W.; Davey Smith, G. Indicators of socioeconomic position (part 1). J. Epidemiol. Community Health 2006, 60, 7–12. [Google Scholar] [CrossRef] [Green Version]
- Mogos, M.F.; Salinas-Miranda, A.A.; Salemi, J.L.; Medina, I.M.; Salihu, H.M. Pregnancy-Related Hypertensive Disorders and Immigrant Status: A Systematic Review and Meta-analysis of Epidemiological Studies. J. Immigr. Minor. Health 2016, 19, 1488–1497. [Google Scholar] [CrossRef]
- Liu, C.; Ahlberg, M.; Hjern, A.; Stephansson, O. Perinatal health of refugee and asylum-seeking women in Sweden 2014–17: A register-based cohort study. Eur. J. Public Health 2019, 29, 1048–1055. [Google Scholar] [CrossRef] [Green Version]
- Juárez, S.; Mussino, E.; Hjern, A. Being a refugee or having a refugee status? Birthweight and gestational age outcomes among offspring of immigrant mothers in Sweden. Scand. J. Public Health 2018, 47, 730–734. [Google Scholar] [CrossRef]
- Andersson, G.; Obucina, O.; Scott, K. Marriage and divorce of immigrants and descendants of immigrants in Sweden. Demogr. Res. 2015, 33, 31–64. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Reference Women | Preeclampsia | |
|---|---|---|
| Women total n = 46,618 | n = 44,298 | n = 1345 |
| Maternal age at childbirth (years) | ||
| <25 | 6256 (14.1%) | 198 (14.7%) |
| 25–29 | 13,850 (31.3%) | 446 (33.2%) |
| 30–34 | 15,771 (35.6%) | 424 (31.5%) |
| 35–39 | 7145 (16.1%) | 221 (16.4%) |
| ≥40 | 1276 (2.9%) | 56 (4.2%) |
| Parity | ||
| 0 (primipara) | 20,543 (46.4%) | 937 (69.7%) |
| 1 | 15,476 (34.9%) | 261 (19.4%) |
| ≥2 | 8279 (18.7%) | 147 (10.9%) |
| Pre-pregnancy BMI (kg/m2) | ||
| Missing | 5342 (12.1%) | 193 (14.3%) |
| <18.5 (underweight) | 1056 (2.4%) | 17 (1.3%) |
| 18.5–<25 (normal weight) | 24,755 (55.9%) | 537 (39.9%) |
| 25–<30 (overweight) | 9416 (21.3%) | 339 (25.2%) |
| ≥30 (obesity) | 3729 (8.4%) | 259 (19.3%) |
| Smoking during pregnancy | ||
| Missing | 3137 (7.1%) | 122 (9.1%) |
| Non-smoker | 36,962 (83.4%) | 1140 (84.8%) |
| Smoker | 4199 (9.5%) | 83 (6.2%) |
| Household disposable income | ||
| Not registered or <80,000 SEK/year | 1811 (4.1%) | 63 (4.7%) |
| Lowest quintile | 7955 (18.0%) | 232 (17.2%) |
| Second quintile | 8282 (18.7%) | 280 (20.8%) |
| Third quintile | 8653 (19.5%) | 284 (21.1%) |
| Fourth quintile | 8769 (19.8%) | 266 (19.8%) |
| Highest quintile | 8828 (19.9%) | 220 (16.4%) |
| Maternal educational level | ||
| Primary (9 yrs) | 5910 (13.3%) | 149 (11.1%) |
| Secondary (12 yrs) | 19,097 (43.1%) | 647 (48.1%) |
| Post-secondary (>12 yrs) | 19,291 (43.5%) | 549 (40.8%) |
| Maternal region of birth | ||
| Sweden | 31,754 (71.7%) | 1037 (77.1%) |
| Nordic countries | 928 (2.1%) | 19 (1.4%) |
| EU-27 | 1858 (4.2%) | 55 (4.1%) |
| Rest of Europe incl Russia | 2850 (6.4%) | 77 (5.7%) |
| The Americas | 678 (1.5%) | 24 (1.8%) |
| Asia and Oceania | 5302 (12.0%) | 101 (7.5%) |
| Africa | 928 (2.1%) | 32 (2.4%) |
| Preeclampsia (n = 1345) | |||||
|---|---|---|---|---|---|
| Maternal Education | No Preeclampsia | Preeclampsia | Model 1 a | Model 2 b | Model 3 c |
| Primary (9 yrs) | 6098 | 149 | 0.87 (0.72, 1.06) | 1.09 (0.85, 1.39) | 1.16 (0.89, 1.50) |
| Secondary (12 yrs) | 19,522 | 647 | 1.19 (1.05, 1.34) | 1.24 (1.09, 1.41) | 1.23 (1.08, 1.41) |
| Post-secondary (>12 yrs) | 19,653 | 549 | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Maternal income quintile | |||||
| Not registered or <80,000 SEK/year | 1846 | 63 | 1.39 (1.05, 1.85) | 1.17 (0.83, 1.65) | 1.31 (0.91, 1.87) |
| Lowest | 8178 | 232 | 1.16 (0.96, 1.40) | 1.07 (0.86, 1.34) | 1.25 (0.99, 1.59) |
| Second | 8496 | 280 | 1.35 (1.13, 1.61) | 1.32 (1.07, 1.62) | 1.36 (1.10, 1.68) |
| Third | 8822 | 284 | 1.32 (1.10, 1.57) | 1.19 (0.99, 1.45) | 1.22 (1.00, 1.48) |
| Fourth | 8935 | 266 | 1.22 (1.02, 1.46) | 1.13 (0.89, 1.33) | 1.14 (0.90, 1.33) |
| Highest | 8996 | 220 | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Women Total, n = 46,618 | Reference Women | Preeclampsia | Model 1 a | Model 2 b | Model 3 c |
|---|---|---|---|---|---|
| Sweden | 32,252 | 1037 | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| Nordic countries | 944 | 19 | 0.63 (0.40, 0.99) | 0.61 (0.39, 0.96) | 0.68 (0.43, 1.06) |
| EU-27 | 1897 | 55 | 0.90 (0.68, 1.20) | 0.88 (0.66, 1.17) | 0.97 (0.73, 1.29) |
| Rest of Europe incl Russia | 2919 | 77 | 0.82 (0.65, 1.04) | 0.76 (0.59, 0.97) | 0.89 (0.69, 1.14) |
| The Americas | 696 | 24 | 1.07 (0.70, 1.65) | 1.01 (0.66, 1.55) | 1.00 (0.65, 1.53) |
| Asia and Oceania | 5580 | 101 | 0.56 (0.45, 0.70) | 0.54 (0.43, 0.67) | 0.60 (0.47, 0.75) |
| Africa | 985 | 32 | 1.01 (0.69, 1.49) | 0.96 (0.65, 1.43) | 1.05 (0.69, 1.58) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mattsson, K.; Juárez, S.; Malmqvist, E. Influence of Socio-Economic Factors and Region of Birth on the Risk of Preeclampsia in Sweden. Int. J. Environ. Res. Public Health 2022, 19, 4080. https://doi.org/10.3390/ijerph19074080
Mattsson K, Juárez S, Malmqvist E. Influence of Socio-Economic Factors and Region of Birth on the Risk of Preeclampsia in Sweden. International Journal of Environmental Research and Public Health. 2022; 19(7):4080. https://doi.org/10.3390/ijerph19074080
Chicago/Turabian StyleMattsson, Kristina, Sol Juárez, and Ebba Malmqvist. 2022. "Influence of Socio-Economic Factors and Region of Birth on the Risk of Preeclampsia in Sweden" International Journal of Environmental Research and Public Health 19, no. 7: 4080. https://doi.org/10.3390/ijerph19074080
APA StyleMattsson, K., Juárez, S., & Malmqvist, E. (2022). Influence of Socio-Economic Factors and Region of Birth on the Risk of Preeclampsia in Sweden. International Journal of Environmental Research and Public Health, 19(7), 4080. https://doi.org/10.3390/ijerph19074080