
The Fagerström and AUDIT Tests as Probable Screening Tools in Oral Cancer and Their Correlation with CYP1A1, GSTM1, GSTP1, and GSTT1 Gene Expression

 ,
,  , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
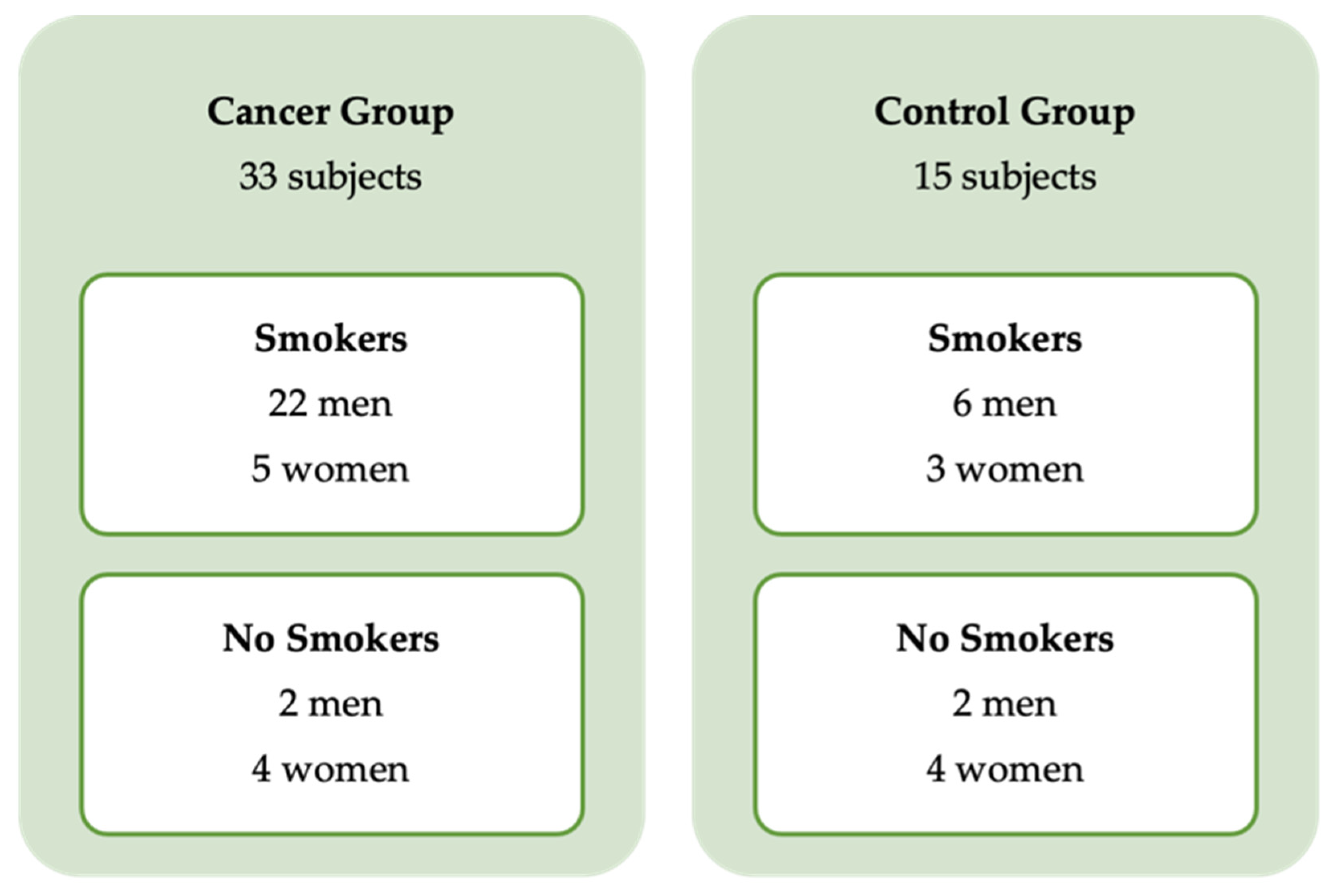
2.1. Sample Selection
2.2. Evaluation of Tobacco and Alcohol Dependence
2.3. RNA Extraction and Quantification
2.4. Selection of the Genes Studied
2.5. Gene Expression Analysis
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 27 December 2021).
- Wünsch Filho, V.; Mirra, A.P.; López, R.V.M.; Antunes, L.F. Tabagismo e câncer no Brasil: Evidências e perspectivas. Rev. Bras. Epidemiol. 2010, 13, 175–187. [Google Scholar] [CrossRef]
- Curado, M.P.; Hashibe, M. Recent changes in the epidemiology of head and neck cancer. Curr. Opin. Oncol. 2009, 21, 194–200. [Google Scholar] [CrossRef]
- Barnes, L.; Eveson, J.; Reichart, P.; Sidransky, D.; WHO. World Health Organization Classification of Tumours. Pathology and Genetics of Head and Neck Tumours; IARC Press: Lyon, France, 2005; 435p. [Google Scholar]
- Huang, S.H.; O’Sullivan, B. Overview of the 8th Edition TNM Classification for Head and Neck Cancer. Curr. Treat. Options Oncol. 2017, 18, 40. [Google Scholar] [CrossRef]
- Glynn, T.; Seffrin, J.R.; Brawley, O.W.; Grey, N.; Ross, H. The globalization of tobacco use: 21 challenges for the 21st century. CA Cancer J. Clin. 2010, 60, 50–61. [Google Scholar] [CrossRef][Green Version]
- World Health Organization—WHO. ICD-10 Version: 2016. 2016. Available online: https://icd.who.int/browse10/2016/en#/ (accessed on 27 December 2021).
- Warnakulasuriya, S.; Dietrich, T.; Bornstein, M.M.; Peidró, E.C.; Preshaw, P.M.; Walter, C.; Wennström, J.L.; Bergström, J. Oral health risks of tobacco use and effects of cessation. Int. Dent. J. 2010, 60, 7–30. [Google Scholar]
- Winn, D.M.; Lee, Y.A.; Hashibe, M.; Boffetta, P.; The INHANCE Consortium. The INHANCE consortium: Toward a better understanding of the causes and mechanisms of head and neck cancer. Oral Dis. 2015, 21, 685–693. [Google Scholar] [CrossRef]
- Hashibe, M.; Brennan, P.; Chuang, S.C.; Boccia, S.; Castellsague, X.; Chen, C.; Curado, M.P.; Dal Maso, L.; Daudt, A.W.; Fabianova, E.; et al. Interaction between tobacco and alcohol use and the risk of head and neck cancer: Pooled analysis in the INHANCE consortium. Cancer Epidemiol. Prev. Biomark. 2009, 18, 541–550. [Google Scholar] [CrossRef]
- Szymańska, K.; Hung, R.J.; Wünsch-Filho, V.; Eluf-Neto, J.; Curado, M.P.; Koifman, S.; Matos, E.; Menezes, A.; Fernandez, L.; Daudt, A.W.; et al. Alcohol and tobacco, and the risk of cancers of the upper aerodigestive tract in Latin America: A case-control study. Cancer Causes Control 2011, 22, 1037–1046. [Google Scholar] [CrossRef]
- Dobrossy, L. Epidemiology of head and neck cancer: Magnitude of the problem. Cancer Metastasis Rev. 2005, 24, 9–17. [Google Scholar] [CrossRef]
- Gandini, S.; Botteri, E.; Iodice, S.; Boniol, M.; Lowenfels, A.B.; Maisonneuve, P.; Boyle, P. Tobacco smoking and cancer: A meta-analysis. Int. J. Cancer 2008, 122, 155–164. [Google Scholar] [CrossRef]
- Petti, S. Lifestyle risk factors for oral cancer. Oral Oncol. 2009, 45, 340–350. [Google Scholar] [CrossRef]
- Marron, M.; Boffetta, P.; Zhang, Z.-F.; Zaridze, D.; Wünsch-Filho, V.; Winn, D.M.; Wei, Q.; Talamini, R.; Szeszenia-Dabrowska, N.; Sturgis, E.M.; et al. Cessation of alcohol drinking, tobacco smoking and the reversal of head and neck cancer risk. Int. J. Epidemiol. 2010, 39, 182–196. [Google Scholar] [CrossRef]
- Rendic, S.P.; Guengerich, F.P. Human Family 1–4 Cytochrome P450 Enzymes Involved in the Metabolic Activation of Xenobiotic and Physiological Chemicals: An Update. Arch. Toxicol. 2021, 95, 395–472. Available online: https://link.springer.com/article/10.1007/s00204-020-02971-4 (accessed on 27 December 2021). [CrossRef]
- Varela-Lema, L.; Taioli, E.; Ruano-Ravina, A.; Barros-Dios, J.M.; Anantharaman, D.; Benhamou, S.; Boccia, S.; Bhisey, R.A.; Cadoni, G.; Capoluongo, E.; et al. Meta-Analysis and Pooled Analysis of GSTM1 and CYP1A1 Polymorphisms and Oral and Pharyngeal Cancers: A HuGE-GSEC Review. Genet. Med. 2008, 10, 369–384. Available online: http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=18496222 (accessed on 27 December 2021). [CrossRef]
- Singh, R.R.; Reindl, K.M. Glutathione S-Transferases in Cancer. Antioxidants 2021, 10, 701. Available online: https://pubmed.ncbi.nlm.nih.gov/33946704/ (accessed on 19 February 2022). [CrossRef]
- Bongers, V.; Snow, G.B.; Braakhuis, B.J.M. The role of glutathione S-transferases in head and neck squamous cell carcinogenesis. Eur. J. Cancer Part B Oral Oncol. 1995, 31, 349–354. Available online: https://pubmed.ncbi.nlm.nih.gov/8746263/ (accessed on 21 February 2022). [CrossRef]
- Stewart, B.W.; Wild, C.; World Health Organization. World Cancer Report 2014; International Agency for Research on Cancer: Lyon, France, 2014; 630p. [Google Scholar]
- Gattás, G.J.F.; De Carvalho, M.B.; Siraque, M.S.; Curioni, O.A.; Kohler, P.; Eluf-Neto, J.; Wünsch-Filho, V. Genetic polymorphisms of CYP1A1, CYP2E1, GSTM1, and GSTT1 associated with head and neck cancer. Head Neck. 2006, 28, 819–826. [Google Scholar] [CrossRef]
- De Amorim, L.M.D.F.; Rossini, A.; Mendonça, G.A.S.; Lotsch, P.F.; de Almeida Simão, T.; de Moura Gallo, C.V.; Pinto, L.F.R. CYP1A1, GSTM1, and GSTT1 polymorphisms and breast cancer risk in Brazilian women. Cancer Lett. 2002, 181, 179–186. [Google Scholar] [CrossRef]
- Rossini, A.; Rapozo, D.; Lima, S.S.; Guimaraes, D.; Ferreira, M.; Teixeira, R.; Kruel, C.; Barros, S.; Andreollo, N.; Acatauassu, R.; et al. Polymorphisms of GSTP1 and GSTT1, but not of CYP2A6, CYP2E1 or GSTM1, modify the risk for esophageal cancer in a western population. Carcinogenesis 2007, 28, 2537–2542. [Google Scholar] [CrossRef]
- Rossini, A.; Rapozo, D.C.M.; Amorim, L.; Macedo, J.M.B.; Medina, R.; Neto, J.F.N.; Gallo, C.V.M.; Pinto, L.F.R. Frequencies of GSTM1, GSTT1, and GSTP1 polymorphisms in a Brazilian population. Genet. Mol. Res. 2002, 1, 233–240. [Google Scholar]
- Pinto, L.F.R.; Rossini, A.M.T.; Albano, R.M.; Felzenszwalb, I.; de Moura Gallo, C.V.; Nunes, R.A.; Andreollo, N.A. Mechanisms of esophageal cancer development in Brazilians. Mutat Res. 2003, 544, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerström, K.O. The Fagerström Test for Nicotine Dependence: A revision of the Fagerström Tolerance Questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Moretti-Pires, R.O.; Corradi-Webster, C.M. Adaptation and validation of the Alcohol Use Disorders Identification Test (AUDIT) for a river population in the Brazilian Amazon. Cad. Saude Publica 2011, 27, 497–509. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA. Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Fagerström, K. Determinants of tobacco use and renaming the FTND to the Fagerström Test for Cigarette Dependence. Nicotine Tob. Res. 2012, 14, 75–78. [Google Scholar] [CrossRef]
- Huang, C.L.; Lin, H.H.; Wang, H.H. Evaluating screening performances of the Fagerström tolerance questionnaire, the Fagerstrom test for nicotine dependence and the heavy smoking index among Taiwanese male smokers. J. Clin. Nurs. 2008, 17, 884–890. [Google Scholar] [CrossRef]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]
- Bandeira, C.M.; de Almeida, A.Á.; Carta, C.F.L.; Almeida, J.D.; Kaminagakura, E. How to improve the early diagnosis of oral cancer? Braz. Dent. Sci. 2017, 20, 25–31. [Google Scholar] [CrossRef]
- GENCAPO. Available online: http://www.gencapo.famerp.br/lmmb/ (accessed on 19 December 2021).
- Canova, C.; Hashibe, M.; Simonato, L.; Nelis, M.; Metspalu, A.; Lagiou, P.; Trichopoulos, D.; Ahrens, W.; Pigeot, I.; Merletti, F.; et al. Genetic Associations of 115 Polymorphisms with Cancers of the Upper Aerodigestive Tract across 10 European Countries: The ARCAGE Project. Cancer Res. 2009, 69, 2956–2965. Available online: https://pubmed.ncbi.nlm.nih.gov/19339270/ (accessed on 19 December 2021). [CrossRef]
- International Head and Neck Cancer Epidemiology Consortium|University of Utah. Available online: https://medicine.utah.edu/inhance/ (accessed on 19 December 2021).
- IARCRP: Home. Available online: https://interchange.iarc.fr/ (accessed on 19 December 2021).
- HEAD Space: Home. Available online: https://headspace.iarc.fr/ (accessed on 19 December 2021).
- Di Credico, G.; Polesel, J.; Dal Maso, L.; Pauli, F.; Torelli, N.; Luce, D.; Radoï, L.; Matsuo, K.; Serraino, D.; Brennan, P.; et al. Alcohol drinking and head and neck cancer risk: The joint effect of intensity and duration. Br. J. Cancer 2020, 123, 1456–1463. [Google Scholar] [CrossRef]
- Masood, N.; Malik, F.A.; Kayani, M.A. Expression of xenobiotic metabolizing genes in head and neck cancer tissues. Asian Pac. J. Cancer Prev. 2011, 12, 377–382. [Google Scholar]
- Aupérin, A. Epidemiology of head and neck cancers: An update. Curr. Opin. Oncol. 2020, 32, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Graner, K.M.; Rolim, G.S.; Moraes, A.B.A.; Padovani, C.R.; Lopes, M.A.; Santos-Silva, A.R.; A Ramos-Cerqueira, A.T. Feelings, perceptions, and expectations of patients during the process of oral cancer diagnosis. Support Care Cancer 2016, 24, 2323–2332. [Google Scholar] [CrossRef] [PubMed]
- Ministério da Saúde. Estimate/2020—Cancer Incidence in Brazil; Instituto Nacional do Câncer (INCA): Rio de Janeiro, Brazil, 2019. Available online: https://www.inca.gov.br/sites/ufu.sti.inca.local/files/media/document/estimativa-2020-incidencia-de-cancer-no-brasil.pdf (accessed on 22 December 2021).
- Lipsky, M.S.; Su, S.; Crespo, C.J.; Hung, M. Men and Oral Health: A Review of Sex and Gender Differences. Am. J. Men’s Health 2021, 15, 15579883211016361. [Google Scholar] [CrossRef]
- Smith, L.K.; Pope, C.; Botha, J.L. Patients’ help-seeking experiences and delay in cancer presentation: A qualitative synthesis. Lancet 2005, 366, 825–831. [Google Scholar] [CrossRef]
- Rendic, S. Summary of information on human CYP enzymes: Human P450 metabolism data. Drug Metab. Rev. 2002, 34, 83–448. [Google Scholar] [CrossRef]
- Masood, N.; Kayani, M.A. Expression patterns of carcinogen detoxifying genes (CYP1A1, GSTP1 & GSTT1) in HNC patients. Pathol. Oncol. Res. 2012, 19, 89–94. [Google Scholar]
- Zakiullah, Z.; Ahmadullah, A.; Khisroon, M.; Saeed, M.; Khan, A.; Khuda, F.; Ali, S.; Javed, N.; Ovais, M.; Masood, N.; et al. Genetic susceptibility to oral cancer due to combined effects of GSTT1, GSTM1 and CYP1A1 gene variants in tobacco addicted patients of pashtun ethnicity of Khyber Pakhtunkhwa Province of Pakistan. Asian Pac. J. Cancer Prev. 2015, 16, 1145–1150. [Google Scholar] [CrossRef]
- Losi-Guembarovski, R.; Cólus, I.M.; de Menezes, R.P.; Poliseli, F.; Chaves, V.N.; Kuasne, H.; Leichsenring, A.; Guembarovski, A.L.; Oliveira, B.W.; Ramos, G.; et al. Lack of association among polymorphic xenobiotic-metabolizing enzyme genotypes and the occurrence and progression of oral carcinoma in a Brazilian population. Anticancer. Res. 2008, 28, 1023–1028. [Google Scholar]
- Singh, R.; Haridas, N.; Shah, F.; Patel, J.; Shukla, S.; Patel, P. Gene Polymorphisms, Tobacco Exposure and Oral Cancer Susceptibility: A Study from GUJARAT, West India. Oral Dis. 2014, 20, 84–93. Available online: https://pubmed.ncbi.nlm.nih.gov/23444898/ (accessed on 22 February 2022). [CrossRef]
- Androutsopoulos, V.P.; Tsatsakis, A.M.; Spandidos, D.A. Cytochrome P450 CYP1A1: Wider Roles in Cancer Progression and Prevention. BMC Cancer 2009, 9, 187. Available online: https://pubmed.ncbi.nlm.nih.gov/19531241/ (accessed on 22 December 2021). [CrossRef] [PubMed]
- Chatterjee, S.; Chakrabarti, S.; Sengupta, B.; Poddar, S.; Biswas, D.; Sengupta, S.; Talukder, G. Prevalence of CYP1A1 and GST Polymorphisms in the Population of Northeastern India and Susceptibility of Oral Cancer. Oncol. Res. 2009, 17, 397–403. Available online: https://pubmed.ncbi.nlm.nih.gov/19718946/ (accessed on 22 December 2021). [CrossRef] [PubMed]
- He, X.; Feng, S. Role of Metabolic Enzymes P450 (CYP) on Activating Procarcinogen and Their Polymorphisms on the Risk of Cancers. Curr. Drug Metab. 2015, 16, 850–863. Available online: https://pubmed.ncbi.nlm.nih.gov/26652254/ (accessed on 22 December 2021). [CrossRef]
- Yokoyama, A.; Katada, C.; Yokoyama, T.; Takizawa, K.; Yano, T.; Oda, I.; Shimizu, Y.; Nakanishi, H.; Koike, T.; Hirao, M.; et al. The Alcohol Use Disorders Identification Test and the risk of metachronous cancer after endoscopic resection of esophageal cancer. Carcinogenesis 2020, 41, 1049–1056. [Google Scholar] [CrossRef]
- Almeida, A.A.; Bandeira, C.M.; Goncalves, A.J.; Araujo, A.J. Nicotine dependence and smoking habits in patients with head and neck cancer. J. Bras. Pneumol. 2014, 40, 286–293. [Google Scholar] [CrossRef]
- Schiller, U.; Inhestern, J.; Burger, U.; Singer, S.; Guntinas-Lichius, O. Predictors of post-treatment smoking and drinking behavior of head and neck cancer survivors: Results of a population-based survey. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 3337–3345. [Google Scholar] [CrossRef]


{kind=link}
| Sample | n = 48 | |||
|---|---|---|---|---|
| Age (Years, Mean ± SD) | 55 ± 14.5 | |||
| Cancer group | Control group | |||
| n = 33 (75) | n = 15 (25) | |||
| Gender | Male | Female | Male | Female |
| Subjects (n, %) | 24 (50) | 9 (18.75) | 8 (3.84) | 7 (3.36) |
| Cancer stage | ||||
| Stage I | 2 | - | - | - |
| Stage II | 3 | 6 | - | - |
| Stage III | 4 | 1 | - | - |
| Stage IV | 15 | 2 | - | - |
| AUDIT score (median ± IQR) | 12 ± 6.5 | 4 ± 5 | * | |
| ≥8 points | 19 | 2 | 2 | 1 |
| <8 points | 5 | 7 | 6 | 6 |
| FTCD Score of Dependence | Cancer Group (n/%) | Control Group (n/%) |
|---|---|---|
| 0–2 = very low dependence | 3 (8.33) | 2 (5.56) |
| 3–4 = low dependence | 6 (16.66) | 1 (2.78) |
| 5 = moderate dependence | 4 (11.11) | 3 (8.33) |
| 6–7 = high dependence | 11 (30.555) | 2 (5.56) |
| 8–10 = very high dependence | 3 (8.33) | 1 (2.78) |
| Total | 27 | 9 |
| AUDIT Score | ||
| 0–7 points = low risk use | 10 (26.32) | 4 (10.53) |
| 8–15 = risk use | 14 (3.84) | 2 (5.26) |
| 16–19 points = harmful use | 5 (13.16) | 1 (2.63) |
| ≥20 points = probable dependence | 2 (5.26) | - |
| Total | 31 * | 7 |
| Cigarettes Per Day | Duration of Tobacco Use | Tumor Size | Nodal Metastasis | AUDIT Score | CYP1A1 | ||
|---|---|---|---|---|---|---|---|
| Cigarettes per day | Rho | ||||||
| p-value | |||||||
| Duration of tobacco use | Rho | 0.606 | |||||
| p-value | 0.000 | ||||||
| Tumor size | Rho | 0.143 | 0.304 | ||||
| p-value | 0.333 | 0.036 | |||||
| Nodal metastasis | Rho | 0.249 | 0.073 | 0.536 | |||
| p-value | 0.088 | 0.624 | 0.000 | ||||
| AUDIT score | Rho | 0.308 | 0.433 | 0.483 | 0.371 | ||
| p-value | 0.033 | 0.002 | 0.001 | 0.009 | |||
| CYP1A1 | Rho | 0.057 | 0.285 | 0.361 | 0.353 | 0.445 | |
| p-value | 0.702 | 0.050 | 0.002 | 0.014 | 0.002 |
| Cigarettes Per Day | Duration of Tobacco Use | Fagerström Test | AUDIT Score | ||
|---|---|---|---|---|---|
| Cigarettes per day | Rho | ||||
| p-value | |||||
| Duration of tobacco use | Rho | 0.861 | |||
| p-value | 0.003 | ||||
| Fagerström test | Rho | 0.701 | 0.784 | ||
| p-value | 0.019 | 0.007 | |||
| AUDIT score | Rho | 0.761 | 0.800 | 0.876 | |
| p-value | 0.010 | 0.005 | 0.001 |
| Age | Smoking Status | Cigarettes per Day | Duration of Tobacco Use | Fagerström Test | GSTP1 | ||
|---|---|---|---|---|---|---|---|
| Age | Rho | ||||||
| p-value | |||||||
| Smoking status | Rho | 0.506 | |||||
| p-value | 0.066 | ||||||
| Cigarettes per day | Rho | 0.597 | 0.880 | ||||
| p-value | 0.021 | 0.000 | |||||
| Duration of tobacco use | Rho | 0.511 | 0.887 | 0.812 | |||
| p-value | 0.003 | 0.000 | 0.000 | ||||
| Fagerström test | Rho | 0.491 | 0.882 | 0.987 | 0.839 | ||
| p-value | 0.066 | 0.000 | 0.000 | 0.000 | |||
| GSTP1 | Rho | 0.730 | 0.601 | 0.566 | 0.542 | 0.533 | |
| p-value | 0.002 | 0.018 | 0.028 | 0.037 | 0.041 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bandeira, C.M.; Almeida, A.Á.; Alves, M.G.O.; Pascoal, M.B.N.; Chagas, J.F.S.; Neto, M.B.; de Barros, P.P.; Nunes, F.D.; Carta, C.F.L.; Almeida, J.D. The Fagerström and AUDIT Tests as Probable Screening Tools in Oral Cancer and Their Correlation with CYP1A1, GSTM1, GSTP1, and GSTT1 Gene Expression. Int. J. Environ. Res. Public Health 2022, 19, 3991. https://doi.org/10.3390/ijerph19073991
Bandeira CM, Almeida AÁ, Alves MGO, Pascoal MBN, Chagas JFS, Neto MB, de Barros PP, Nunes FD, Carta CFL, Almeida JD. The Fagerström and AUDIT Tests as Probable Screening Tools in Oral Cancer and Their Correlation with CYP1A1, GSTM1, GSTP1, and GSTT1 Gene Expression. International Journal of Environmental Research and Public Health. 2022; 19(7):3991. https://doi.org/10.3390/ijerph19073991
Chicago/Turabian StyleBandeira, Celso Muller, Adriana Ávila Almeida, Mônica Ghislaine Oliveira Alves, Maria Beatriz Nogueira Pascoal, José Francisco Sales Chagas, Morun Bernardino Neto, Patrícia Pimentel de Barros, Fábio Daumas Nunes, Celina Faig Lima Carta, and Janete Dias Almeida. 2022. "The Fagerström and AUDIT Tests as Probable Screening Tools in Oral Cancer and Their Correlation with CYP1A1, GSTM1, GSTP1, and GSTT1 Gene Expression" International Journal of Environmental Research and Public Health 19, no. 7: 3991. https://doi.org/10.3390/ijerph19073991
APA StyleBandeira, C. M., Almeida, A. Á., Alves, M. G. O., Pascoal, M. B. N., Chagas, J. F. S., Neto, M. B., de Barros, P. P., Nunes, F. D., Carta, C. F. L., & Almeida, J. D. (2022). The Fagerström and AUDIT Tests as Probable Screening Tools in Oral Cancer and Their Correlation with CYP1A1, GSTM1, GSTP1, and GSTT1 Gene Expression. International Journal of Environmental Research and Public Health, 19(7), 3991. https://doi.org/10.3390/ijerph19073991