
Telephone-Based Structured Communication Simulation Program for the Follow-Up of COVID-19 Cases and Contacts in Primary Care

 ,
,  , ,
, ,  ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Methods
2.1. Design
2.2. Setting and Sample
2.3. Training Program
2.3.1. Asynchronous General Theoretical Training
2.3.2. Synchronous Practical Training
Simulation Design Process
Prebriefing
- Detailed explanation of the development of the session.
- Clarification of the expectations and the answering of questions posed with respect to the development of the online simulation session.
- Explanation of the logistic details of the platform and the tools utilized.
- Explanation that a mistake is an opportunity to learn (the mistakes do not have risk or consequences).
- Establishment of a “fictional contract” with the participants.
- Agreement of confidentiality and commitment of respect to the other participants.
Teaching Problem Videos
Simulated Telephone Interviews
2.4. Data Collection Instrument
2.5. Statistical Analysis
2.6. Ethical Considerations
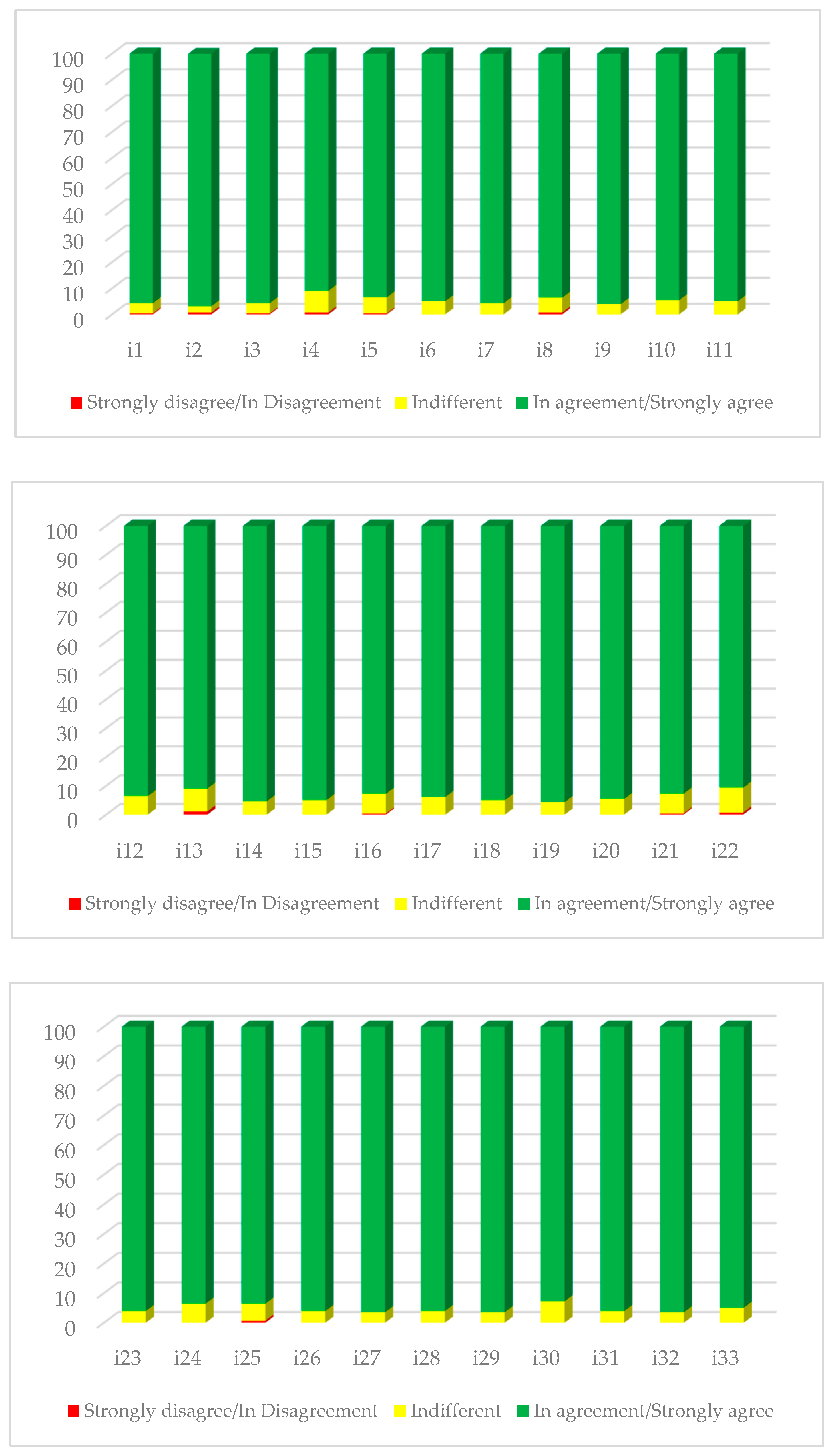
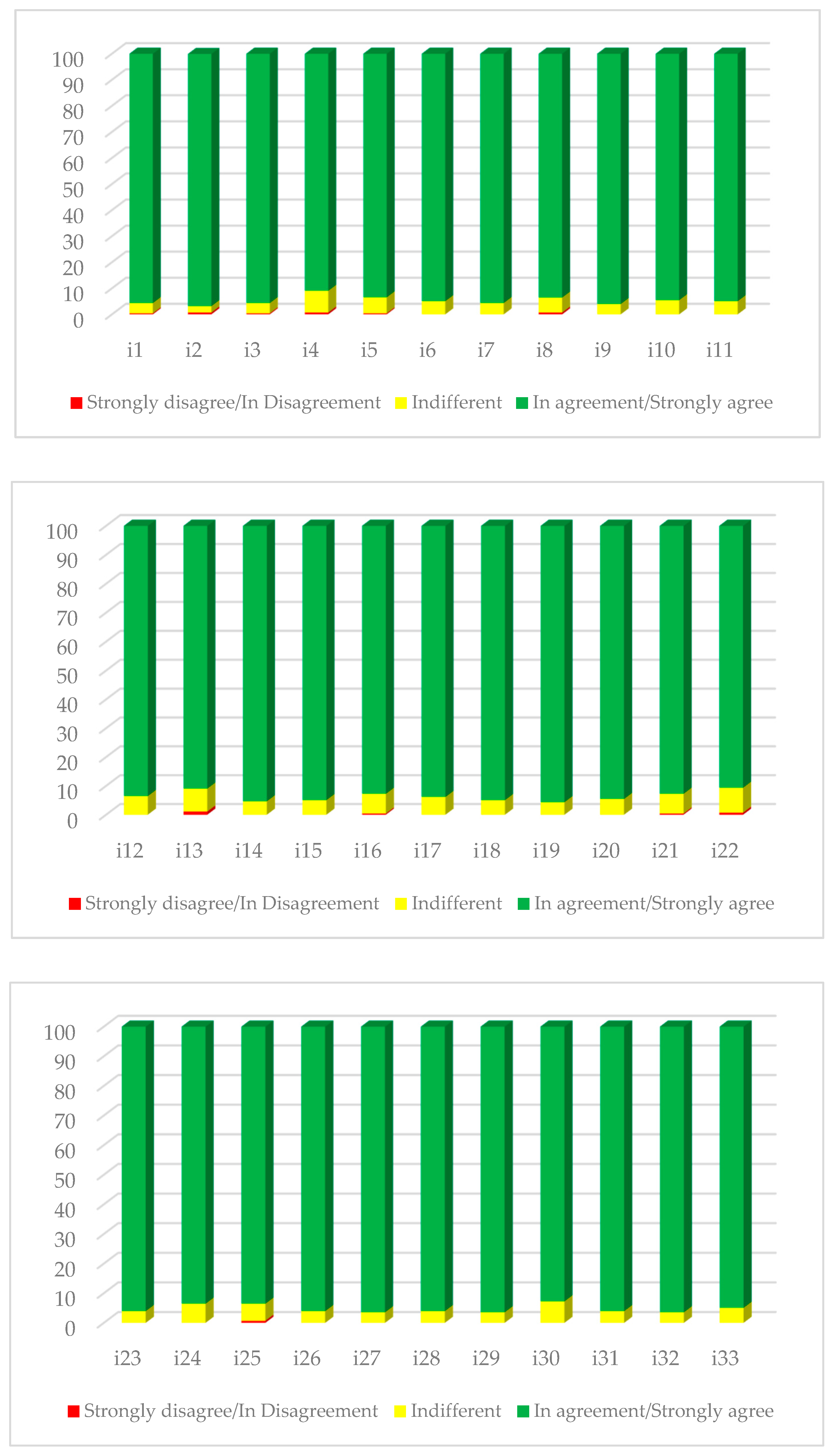
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization Declares Global Emergency: A Review of the 2019 Novel Coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Organización Mundial de la Salud (OMS). Nuevo Coronavirus 2019. Available online: https://www.who.int/es/emergencies/diseases/novel-coronavirus-2019 (accessed on 10 May 2020).
- Giwa, A.L.; Desai, A.; Duca, A. Novel 2019 Coronavirus SARS-CoV-2 (COVID-19): An Updated Overview for Emergency Clinicians. Emerg. Med. Pract. 2020, 22, 1–28. [Google Scholar] [PubMed]
- World Health Organization (WHO). Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 25 October 2021).
- Centro Nacional de Epidemiología. Situación de COVID-19 en España. Available online: https://cnecovid.isciii.es/covid19/ (accessed on 10 May 2020).
- Castilla, J.; Moreno-Iribas, C.; Ibero Esparza, C.; Martínez-Baz, I.; Trobajo-Sanmartín, C.; Ezpeleta, C.; Guevara, M.; Grupo para el Estudio de COVID-19 en Navarra. Primera onda pandémica de COVID-19 en Navarra, febrero–junio 2020. Anal. Sist. Sanit. Navarra, 2021; ahead of print. [Google Scholar] [CrossRef]
- De Nicolás Jiménez, J.M.; Blázquez Recio, L.M.; Fabregat Domínguez, M.T.; Palomo Cobos, L. COVID-19 y esfuerzo asistencial en atención primaria. Atenc. Prim. 2020, 52, 588–590. [Google Scholar] [CrossRef]
- Soriano, J.B.; Gerli, A.G.; Centanni, S.; Ancochea, J. Forecasting COVID-19 Infection Trends and New Hospital Admissions in Spain Due to SARS-CoV-2 Variant of Concern Omicron. Arch. Bronconeumol. 2022; in press. [Google Scholar] [CrossRef]
- Iacobucci, G. Covid-19: Runny Nose, Headache, and Fatigue Are Commonest Symptoms of Omicron, Early Data Show. BMJ 2021, 375, n3103. [Google Scholar] [CrossRef]
- Gobierno de España, Ministerio de Sanidad. Manejo en Atención Primaria y Domiciliaria del COVID-19; Gobierno de España, Ministerio de Sanidad: Madrid, Spain, 2020. [Google Scholar]
- Barrio Cortes, J.; Mir Sánchez, C.; Regato Pajares, P. Atención primaria en el domicilio en el marco de la pandemia COVID-19. Atenc. Prim. 2021, 53, 101963. [Google Scholar] [CrossRef]
- Mehrotra, A.; Ray, K.; Brockmeyer, D.M.; Barnett, M.L.; Bender, J.A. Rapidly Converting to “Virtual Practices”: Outpatient Care in the Era of COVID-19. NEJM Catal. Innov. Care Deliv. 2020. [Google Scholar] [CrossRef]
- Ludwig, C.; Stoevesandt, D.; Ludwig, C.; Fritsche, V. Telephone-Based Communication Training in the Era of COVID-19. GMS J. Med. Educ. 2021, 38, 1–6. [Google Scholar] [CrossRef]
- Sindhu, K.K. The Phone: Communication in the Age of COVID-19. Patient Educ. Couns. 2021, 104, 1889–1890. [Google Scholar] [CrossRef]
- Sales, M.B.; Mira, M.J.M. Consulta Telefónica. Rev. Med. Fam. Aten. Primaria 2020, 25, 1–4. [Google Scholar]
- Khan, M.N.B. Telephone Consultations in Primary Care, How to Improve Their Safety, Effectiveness and Quality. BMJ Qual. Improv. Rep. 2013, 2, u202013.w1227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flint, L.; Kotwal, A. The New Normal: Key Considerations for Effective Serious Illness Communication Over Video or Telephone During the Coronavirus Disease 2019 (COVID-19) Pandemic. Ann. Intern. Med. 2020, 173, 486–488. [Google Scholar] [CrossRef] [PubMed]
- Pinto, R.Z.; Ferreira, M.L.; Oliveira, V.C.; Franco, M.R.; Adams, R.; Maher, C.G.; Ferreira, P.H. Patient-Centred Communication Is Associated with Positive Therapeutic Alliance: A Systematic Review. J. Physiother. 2012, 58, 77–87. [Google Scholar] [CrossRef] [Green Version]
- Zolnierek, K.B.H.; Dimatteo, M.R. Physician Communication and Patient Adherence to Treatment: A Meta-Analysis. Med. Care 2009, 47, 826–834. [Google Scholar] [CrossRef] [Green Version]
- Organización Mundial de la Salud (OMS). “Nueve Soluciones para la Seguridad del Paciente” a Fin de Salvar Vidas y Evitar Daños; WHO: Geneva, Switzerland, 2007.
- Soar, J.; Böttiger, B.W.; Carli, P.; Couper, K.; Deakin, C.D.; Djärv, T.; Lott, C.; Olasveengen, T.; Paal, P.; Pellis, T.; et al. European Resuscitation Council Guidelines 2021: Adult Advanced Life Support. Resuscitation 2021, 161, 115–151. [Google Scholar] [CrossRef]
- Müller, M.; Jürgens, J.; Redaèlli, M.; Klingberg, K.; Hautz, W.E.; Stock, S. Impact of the Communication and Patient Hand-off Tool SBAR on Patient Safety: A Systematic Review. BMJ Open 2018, 8, e022202. [Google Scholar] [CrossRef] [Green Version]
- De Meester, K.; Verspuy, M.; Monsieurs, K.G.; Van Bogaert, P. SBAR Improves Nurse-Physician Communication and Reduces Unexpected Death: A Pre and Post Intervention Study. Resuscitation 2013, 84, 1192–1196. [Google Scholar] [CrossRef]
- Kostoff, M.; Burkhardt, C.; Winter, A.; Shrader, S. An Interprofessional Simulation Using the SBAR Communication Tool. Am. J. Pharm. Educ. 2016, 80, 157. [Google Scholar] [CrossRef]
- Real Academia Española de la Lengua (RAE). RAE Diccionario de la Lengua Española. Available online: https://dle.rae.es/ (accessed on 25 January 2022).
- Leal-Costa, C.; Orcajada-Muñoz, I.; Díaz Agea, J.L.; Adánez-Martínez, M.G. CERCAR to COVID-19: A structured communication model for the follow-up of cases and contacts in Primary Care. Anal. Sist. Sanit. Navarra, 2022; in press. [Google Scholar] [CrossRef]
- Motola, I.; Devine, L.A.; Chung, H.S.; Sullivan, J.E.; Issenberg, S.B. Simulation in Healthcare Education: A Best Evidence Practical Guide. AMEE Guide No. 82. Med. Teach. 2013, 35, e1511–e1530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batllori Gastón, M. Simulación Clínica y La Pandemia Por COVID-19. ¿De Dónde Venimos? ¿Hacia Dónde Queremos Ir? Anal. Sist. Sanit. Navarra 2020, 43, 125–129. [Google Scholar] [CrossRef]
- Díaz Agea, J.L.; Pujalte-Jesús, M.J.; Leal Costa, C.; Díaz Agea, J.L.; Pujalte-Jesús, M.J.; Leal Costa, C. Simular En Tiempos de Confinamiento. Cómo Transformar La Simulación Clínica a Un Formato Online En Un Contexto Universitario de Ciencias de La Salud. Anal. Sist. Sanit. Navarra 2020, 43, 273–276. [Google Scholar] [CrossRef]
- Thomas, C.M.; Bertram, E.; Johnson, D. The SBAR Communication Technique: Teaching Nursing Students Professional Communication Skills. Nurse Educ. 2009, 34, 176–180. [Google Scholar] [CrossRef]
- Noh, G.O.; Park, M.J. Effectiveness of Incorporating Situation-Background-Assessment-Recommendation (SBAR) Methods into Simulation-Based Education for Nursing Students: A Quasi-Experimental Study. Nurse Educ. Today 2022, 109, 105252. [Google Scholar] [CrossRef]
- Creswell, J.W.; Clark, V.L.P. Designing and Conducting Mixed Methods Research; SAGE: London, UK, 2011; ISBN 978-1-4129-7517-9. [Google Scholar]
- Watts, P.I.; McDermott, D.S.; Alinier, G.; Charnetski, M.; Ludlow, J.; Horsley, E.; Meakim, C.; Nawathe, P.A. Healthcare Simulation Standards of Best PracticeTM Simulation Design. Clin. Simul. Nurs. 2021, 58, 14–21. [Google Scholar] [CrossRef]
- Del Moral, I.; Maestre, J.M. A View on the Practical Application of Simulation in Professional Education. Trends Anaesth. Crit. Care 2013, 3, 146–151. [Google Scholar] [CrossRef]
- McDermott, D.S.; Ludlow, J.; Horsley, E.; Meakim, C. Healthcare Simulation Standards of Best PracticeTM Prebriefing: Preparation and Briefing. Clin. Simul. Nurs. 2021, 58, 9–13. [Google Scholar] [CrossRef]
- Rudolph, J.W.; Raemer, D.B.; Simon, R. Establishing a Safe Container for Learning in Simulation: The Role of the Presimulation Briefing. Simul. Healthcare 2014, 9, 339–349. [Google Scholar] [CrossRef]
- Turner, S.; Harder, N. Psychological Safe Environment: A Concept Analysis. Clin. Simul. Nurs. 2018, 18, 47–55. [Google Scholar] [CrossRef] [Green Version]
- Cheng, A.; Eppich, W.; Grant, V.; Sherbino, J.; Zendejas, B.; Cook, D.A. Debriefing for Technology-Enhanced Simulation: A Systematic Review and Meta-Analysis. Med. Educ. 2014, 48, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Decker, S.; Alinier, G.; Crawford, S.B.; Gordon, R.M.; Jenkins, D.; Wilson, C. Healthcare Simulation Standards of Best PracticeTM The Debriefing Process. Clin. Simul. Nurs. 2021, 58, 27–32. [Google Scholar] [CrossRef]
- Alconero-Camarero, A.R.; Gualdrón-Romero, A.; Sarabia-Cobo, C.M.; Martinez-Arce, A. Clinical Simulation as a Learning Tool in Undergraduate Nursing: Validation of a Questionnaire. Nurse Educ. Today 2016, 39, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.J.; Bogdan, R.; DeVault, M. Introduction to Qualitative Research Methods: A Guidebook and Resource; John Wiley & Sons: Hoboken, NJ, USA, 2015; ISBN 978-1-118-76729-0. [Google Scholar]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Díaz Agea, J.L.; Ramos-Morcillo, A.J.; Amo Setien, F.J.; Ruzafa-Martínez, M.; Hueso-Montoro, C.; Leal-Costa, C. Perceptions about the Self-Learning Methodology in Simulated Environments in Nursing Students: A Mixed Study. Int. J. Environ. Res. Public Health 2019, 16, 4646. [Google Scholar] [CrossRef] [Green Version]
- Warren, J.N.; Luctkar-Flude, M.; Godfrey, C.; Lukewich, J. A Systematic Review of the Effectiveness of Simulation-Based Education on Satisfaction and Learning Outcomes in Nurse Practitioner Programs. Nurse Educ. Today 2016, 46, 99–108. [Google Scholar] [CrossRef]
- Mirza, M.B.; Sulaiman, A.; Hashmi, S.; Zaki, S.; Rehman, R.; Akbar, R. Use of Simulation Based Technology in Pre-Clinical Years Improves Confidence and Satisfaction among Medical Students. JPMA J. Pak. Med. Assoc. 2021, 71, 1296–1302. [Google Scholar] [CrossRef]
- Jiménez-Rodríguez, D.; del Mar Torres Navarro, M.; del Pino, F.J.P.; Arrogante, O. Simulated Nursing Video Consultations: An Innovative Proposal During Covid-19 Confinement. Clin. Simul. Nurs. 2020, 48, 29–37. [Google Scholar] [CrossRef]
- Jiménez-Rodríguez, D.; Arrogante, O. Simulated Video Consultations as a Learning Tool in Undergraduate Nursing: Students’ Perceptions. Healthcare 2020, 8, 280. [Google Scholar] [CrossRef]
- Jiménez-Rodríguez, D.; Belmonte García, M.T.; Santillán García, A.; del Pino, F.J.P.; Ponce-Valencia, A.; Arrogante, O. Nurse Training in Gender-Based Violence Using Simulated Nursing Video Consultations during the COVID-19 Pandemic: A Qualitative Study. Int. J. Environ. Res. Public Health 2020, 17, 8654. [Google Scholar] [CrossRef]
- Waldner, M.H.; Olson, J.K. Taking the Patient to the Classroom: Applying Theoretical Frameworks to Simulation in Nursing Education. Int. J. Nurs. Educ. Scholarsh. 2007, 4, 18. [Google Scholar] [CrossRef] [PubMed]
- Lisko, S.A.; O’Dell, V. Integration of Theory and Practice: Experiential Learning Theory and Nursing Education. Nurs. Educ. Perspect. 2010, 31, 106–108. [Google Scholar] [PubMed]
- Shin, S.; Park, J.-H.; Kim, J.-H. Effectiveness of Patient Simulation in Nursing Education: Meta-Analysis. Nurse Educ. Today 2015, 35, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, A.; Kumar, A. Breaking the COVID-19 Barriers to Health Professional Team Training With Online Simulation. Simul. Healthcare J. Soc. Simul. Healthcare 2021, 16, 80–81. [Google Scholar] [CrossRef]
- Kim, J.; Park, J.-H.; Shin, S. Effectiveness of Simulation-Based Nursing Education Depending on Fidelity: A Meta-Analysis. BMC Med. Educ. 2016, 16, 152. [Google Scholar] [CrossRef] [Green Version]
- Rød, I.; Kynø, N.M.; Solevåg, A.L. From Simulation Room to Clinical Practice: Postgraduate Neonatal Nursing Students’ Transfer of Learning from in-Situ Resuscitation Simulation with Interprofessional Team to Clinical Practice. Nurse Educ. Pract. 2021, 52, 102994. [Google Scholar] [CrossRef]
- Hustad, J.; Johannesen, B.; Fossum, M.; Hovland, O.J. Nursing Students’ Transfer of Learning Outcomes from Simulation-Based Training to Clinical Practice: A Focus-Group Study. BMC Nurs. 2019, 18, 53. [Google Scholar] [CrossRef] [Green Version]
- Dufrene, C.; Young, A. Successful Debriefing—Best Methods to Achieve Positive Learning Outcomes: A Literature Review. Nurse Educ. Today 2014, 34, 372–376. [Google Scholar] [CrossRef]
- Levett-Jones, T.; Lapkin, S. A Systematic Review of the Effectiveness of Simulation Debriefing in Health Professional Education. Nurse Educ. Today 2014, 34, e58–e63. [Google Scholar] [CrossRef]
- Kaplan, B.; Litewka, S. Ethical Challenges of Telemedicine and Telehealth. Camb. Q. Healthcare Ethics 2008, 17, 401–416. [Google Scholar] [CrossRef]
- Khalil, K.; Das, P.; Kammowanee, R.; Saluja, D.; Mitra, P.; Das, S.; Gharai, D.; Bhatt, D.; Kumar, N.; Franzen, S. Ethical Considerations of Phone-Based Interviews from Three Studies of COVID-19 Impact in Bihar, India. BMJ Glob. Health 2021, 6, e005981. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Module 1 | Basic aspects of COVID-19 |
| Module 2 | Basic aspects of monitoring of COVID-19 patients and their contacts |
| Module 3 | Steps to take for identifying cases and investigate their contacts |
| Module 4 | Ethical/legal aspects in the management of COVID-19 patients |
| Module 5 | Skills needed to achieve effective communication |
| Video Title | Summary | Objectives |
|---|---|---|
| Clinical interview on COVID-19 | Clinical telephone-based interview of COVID-19 patient. |
|
| The telephone bring us closer | Clinical interview of a COVID-19 patient with social problems. |
|
| Go home | Clinical interview of a patient who is possibly not complying with confinement. |
|
| Scenario | Learning Objectives |
|---|---|
| You call Maria, her six-year old son Abel is waiting for PCR results due to a close contact at school, his PCR is positive |
|
| You call Mario, 43 years old. You inform him that his PCR test is positive. |
|
| You call Javier, 18 years old. Works in a private residential home, had a PCR test 24 h ago and is positive. |
|
| You call Yesica, 20 years old. PCR positive. The test was done 24 h ago. |
|
| You call Manuel, 36 years old, positive PCR. Test done 48 h ago. Negationist. |
|
| You call Habib. Positive PCR. Does not understand the language. You hear lots of coughing. Important communication barrier. A 10 year-old girl gets the phone. |
|
| You call Antonia, 82 years old. Follow-up call due to positive PCR test, it’s the third day you call. |
|
| You call Ruben for a follow-up. 20 years old. Positive PCR 10 days ago, asymptomatic on yesterday’s call. |
|
| You call Tomas, 50 years old, for a follow-up. Positive PCR 4 days ago. |
|
| You call Eugenia, 50 years old. Very symptomatic. Negative PCR. |
|
| You call Pedro, 18 years old, because he was a close contact. Positive PCR yesterday. |
|
| You call Felipe, 56 years old. Mild symptoms. He is homeless and lives on the street. |
|
| You call Julia, 22 years old. Does not answer the calls. |
|
| You call Ana, in quarantine due to close contact 10 days ago. She was just deemed positive. |
|
| You call Carmen to inform her she is PCR positive. She just came back from her father’s funeral, who died due to COVID-19. |
|
| You call Ruben, nursing student. He is positive. He already knows it because his girlfriend, a nurse, has just informed him. |
|
| You call Abel, 85 years old. His daughter answers the phone. She informs you that he has just passed away. |
|
| You call Mario, 43 years old, he was just discharged from the hospital. He was admited due to pneumonia due to COVID-19. |
|
| You call Javier, 23 years old. He has received two doses of the vaccine. He is positive due to close contact. |
|
| You call Monica, caregiver to the elderly in a residential home, she is a close contact. She resists vaccination. |
|
| Total n = 275 | Groups | p | ||
|---|---|---|---|---|
| Physician n = 156 | Nurse n = 119 | |||
| Age M (SD) | 31.2 (9.9) | 29.6 (8.2) | 33.3 (11.5) | 0.003 a |
| Gender n (%) | ||||
| Women | 205 (74.5) | 110 (70.5) | 95 (79.8) | 0.08 b |
| Men | 70 (25.5) | 46 (29.5) | 24 (20.2) | |
| Marital status n (%) | ||||
| Single | 202 (73.5) | 125 (80.1) | 77 (64.7) | 0.004 b |
| Married | 69 (25.1) | 28 (17.9) | 41 (34.5) | |
| Divorced | 3 (1.1) | 3 (2.0) | 0 (0) | |
| Widower | 1 (0.4) | 0 (0) | 1 (0.8) | |
| Resident in training n (%) | ||||
| Yes | 214 (77.8) | 141 (90.4) | 73 (61.3) | 0.000 b |
| No | 61 (22.2) | 15 (9.6) | 46 (38.7) | |
| Professional experience months M (SD) | 62.5 (241.1) | 26.1 (73.1) | 110.2 (352.1) | 0.012 a |
| Items M (SD) | Total n = 275 | Groups | p | |
|---|---|---|---|---|
| Physician n = 156 | Nurse n = 119 | |||
| 4.64 (0.58) | 4.62 (0.62) | 4.68 (0.52) | 0.35 |
| 4.73 (0.56) | 4.72 (0.56) | 4.75 (0.56) | 0.73 |
| 4.72 (0.55) | 4.71 (0.59) | 4.74 (0.49) | 0.68 |
| 4.53 (0.68) | 4.50 (0.70) | 4.56 (0.65) | 0.45 |
| 4.45 (0.63) | 4.46 (0.60) | 4.45 (0.66) | 0.90 |
| 4.77 (0.53) | 4.79 (0.51) | 4.74 (0.56) | 0.45 |
| 4.68 (0.55) | 4.66 (0.57) | 4.71 (0.53) | 0.50 |
| 4.53 (0.64) | 4.53 (0.64) | 4.53 (0.65) | 0.97 |
| 4.67 (0.55) | 4.65 (0.57) | 4.71 (0.53) | 0.38 |
| 4.67 (0.58) | 4.67 (0.57) | 4.66 (0.58) | 0.97 |
| 4.69 (0.56) | 4.69 (0.56) | 4.70 (0.56) | 0.94 |
| 4.63 (0.60) | 4.62 (0.61) | 4.65 (0.59) | 0.73 |
| 4.52 (0.69) | 4.53 (0.70) | 4.51 (0.67) | 0.82 |
| 4.71 (0.55) | 4.71 (0.56) | 4.70 (0.54) | 0.83 |
| 4.59 (0.59) | 4.57 (0.61) | 4.62 (0.55) | 0.47 |
| 4.58 (0.64) | 4.55 (0.65) | 4.62 (0.61) | 0.36 |
| 4.63 (0.60) | 4.60 (0.61) | 4.66 (0.58) | 0.40 |
| 4.56 (0.59) | 4.52 (0.59) | 4.61 (0.58) | 0.19 |
| 4.61 (0.57) | 4.57 (0.59) | 4.66 (0.54) | 0.22 |
| 4.64 (0.58) | 4.61 (0.61) | 4.67 (0.55) | 0.37 |
| 4.56 (0.64) | 4.57 (0.62) | 4.55 (0.66) | 0.84 |
| 4.52 (0.69) | 4.50 (0.70) | 4.55 (0.66) | 0.58 |
| 4.72 (0.53) | 4.71 (0.54) | 4.73 (0.52) | 0.76 |
| 4.63 (0.60) | 4.60 (0.64) | 4.68 (0.55) | 0.25 |
| 4.35 (0.62) | 4.38 (0.58) | 4.31 (0.67) | 0.38 |
| 4.61 (0.56) | 4.61 (0.56) | 4.61 (0.57) | 0.95 |
| 4.77 (0.50) | 4.76 (0.51) | 4.78 (0.49) | 0.68 |
| 4.75 (0.52) | 4.78 (0.50) | 4.71 (0.54) | 0.33 |
| 4.76 (0.51) | 4.77 (0.51) | 4.74 (0.51) | 0.63 |
| 4.45 (0.63) | 4.47 (0.63) | 4.43 (0.63) | 0.61 |
| 4.71 (0.53) | 4.70 (0.54) | 4.73 (0.53) | 0.62 |
| 4.73 (0.52) | 4.71 (0.53) | 4.76 (0.50) | 0.48 |
| 4.65 (0.57) | 4.63 (0.59) | 4.67 (0.55) | 0.59 |
| Items M (SD) | Total n = 145 | Groups | p | |
|---|---|---|---|---|
| Physician n = 92 | Nurse n = 55 | |||
| Consolidation of the learning | ||||
| 1. The training has improved your theoretical-practical knowledge in relation to COVID-19. | 4.44 (0.66) | 4.47 0.67 | 4.38 (0.65) | 0.45 |
| 2. It has implied an improvement in your technical competences. | 4.36 (0.66) | 4.40 (0.63) | 4.29 (0.71) | 0.33 |
| 3. The training has implied an improvement in your communication skills and the achievement of efficient communication. | 4.37 (0.65) | 4.41 (0.67) | 4.29 (0.63) | 0.27 |
| Applicability to the position at work | ||||
| 4. You have had the opportunity to apply the knowlede acquired related with COVID-19 at work. | 4.33 (0.72) | 4.41 (0.71) | 4.20 (0.73) | 0.08 |
| 5. The training has helped you in the making of decisions related to COVID-19 in your position at work | 4.32 (0.71) | 4.41 (0.67) | 4.16 (0.76) | 0.04 |
| 6. I’ve had the opportunity at work to participate in the telephone-based monitoring of COVID-19 cases | 4.38 (0.73) | 4.50 (0.62) | 4.17 (0.84) | 0.01 |
| 7. You have used the CERCAR© COVID-19 protocol in the monitoring of cases and close contacts. | 4.25 (0.65) | 4.33 (0.65) | 4.13 (0.64) | 0.07 |
| Benefit for the organization | ||||
| 8. Do you believe the training has been beneficial to the Organization? | 4.48 (0.61) | 4.51 (0.60) | 4.42 (0.63) | 0.38 |
| Category | Verbatim |
|---|---|
| Satisfaction with the experience based on clinical simulation | “I loved the course, it was very useful. The professors promoted interaction, dynamics, and trust!”(N40) “Thank you for this Learning” (N54) “It was a very complete, interesting, and stimulating course” (D74) “I consider the simulation sessions to be especially useful for our training” (D104) “Very useful and pertinent course at this moment in time” (D116) “The execution of the simulation sessions was very entertaining. Mi sincere congratulations to the professors” (D128) “Four very entertaining hours, I had never taken an online course that was this interactive. Congratulations to everyone” (D147) “Very good course and good simulation” (D183) “Very happy with this online initiative, I hope it is done more” (D199) |
| Transfer to clinical practice and the use of the structured communication protocol CER-CAR© COVID-19 | “The CERCAR protocol allowed me to not forget any key questions for my patients” (D40) “…it provides, in an easy manner, all the guidelines to follow to avoid our forgetting of important information, as well as confidence when making COVID-related calls” (D74) “It gives you the tools necessary for every day practice” (N57) “Thank you for organizing and teaching this course, it has greatly helped in the learning to deal with different situations that we may find daily in our consultations” (D217) “It has been a very interesting part, especially the simulation of diverse situations that we could experience in clinical practice” (D221) “Very useful and practical for my job as a physician” (D230) “...course, very necessary for physicians and nurses in primary care, who have cases of contacts or COVID+ cases, and we have to make telephone calls. I did not know the CERCAR protocol or the access to courses such as CORECAS, so I thought this course was very necessary” (N270) |
| Learning in a psychologically safe environment | “It is a novel methodology taught by excellent professionals, who have made learning easy“ (N131) “I am thankful for the opportunity given to us to be able to make mistakes in safe and tutored environments” (D160) “The fact that the course is interactive and participative is what makes it great” (D204) “I especially liked the practical part, as we were all able to participate, and it was therefore very dynamic”(D217) “Excellent teaching team. The dynamics they applied, as well as the videos chosen, the reflections, and the theoretical-practical part were excellent…” (D235) “The type of dynamics of the activity made it easier. It was never too long and boring, on the contrary, it was the putting into practice of what we had learned, and it allowed us to constantly participate, making these hours more entertaining. Having said that, it has exceeded my expectations” (D252) “…I want to thank the good attitude of the teaching staff, always in a good mood, without judging at any moment in time and helping us” (N270) |
| Fidelity of the simulation | “Excellent course; with simulations that were very similar to real life, which greatly help the putting into practice of what I had learned” (D235) |
| Benefits of reflection and debriefing | “…its practial nature and the debriefing helped analyze our mistakes and those of others to improve and learn…” (D155) “I liked the fact that it was participative. Debating and sharing discrepancies is always enriching. Many thanks to the professors; for making it entertaining and giving us freedom to talk” (D249) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adánez-Martínez, M.G.; Jiménez-Ruiz, I.; Carrillo-García, C.; Díaz-Agea, J.L.; Ramos-Morcillo, A.J.; Molina-Rodríguez, A.; Ruzafa-Martínez, M.; Leal-Costa, C. Telephone-Based Structured Communication Simulation Program for the Follow-Up of COVID-19 Cases and Contacts in Primary Care. Int. J. Environ. Res. Public Health 2022, 19, 3915. https://doi.org/10.3390/ijerph19073915
Adánez-Martínez MG, Jiménez-Ruiz I, Carrillo-García C, Díaz-Agea JL, Ramos-Morcillo AJ, Molina-Rodríguez A, Ruzafa-Martínez M, Leal-Costa C. Telephone-Based Structured Communication Simulation Program for the Follow-Up of COVID-19 Cases and Contacts in Primary Care. International Journal of Environmental Research and Public Health. 2022; 19(7):3915. https://doi.org/10.3390/ijerph19073915
Chicago/Turabian StyleAdánez-Martínez, María Gracia, Ismael Jiménez-Ruiz, César Carrillo-García, José Luis Díaz-Agea, Antonio Jesús Ramos-Morcillo, Alonso Molina-Rodríguez, María Ruzafa-Martínez, and César Leal-Costa. 2022. "Telephone-Based Structured Communication Simulation Program for the Follow-Up of COVID-19 Cases and Contacts in Primary Care" International Journal of Environmental Research and Public Health 19, no. 7: 3915. https://doi.org/10.3390/ijerph19073915
APA StyleAdánez-Martínez, M. G., Jiménez-Ruiz, I., Carrillo-García, C., Díaz-Agea, J. L., Ramos-Morcillo, A. J., Molina-Rodríguez, A., Ruzafa-Martínez, M., & Leal-Costa, C. (2022). Telephone-Based Structured Communication Simulation Program for the Follow-Up of COVID-19 Cases and Contacts in Primary Care. International Journal of Environmental Research and Public Health, 19(7), 3915. https://doi.org/10.3390/ijerph19073915