
Breakdown of Diabetic Foot Ulcer Care during the First Year of the Pandemic in Poland: A Retrospective National Cohort Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
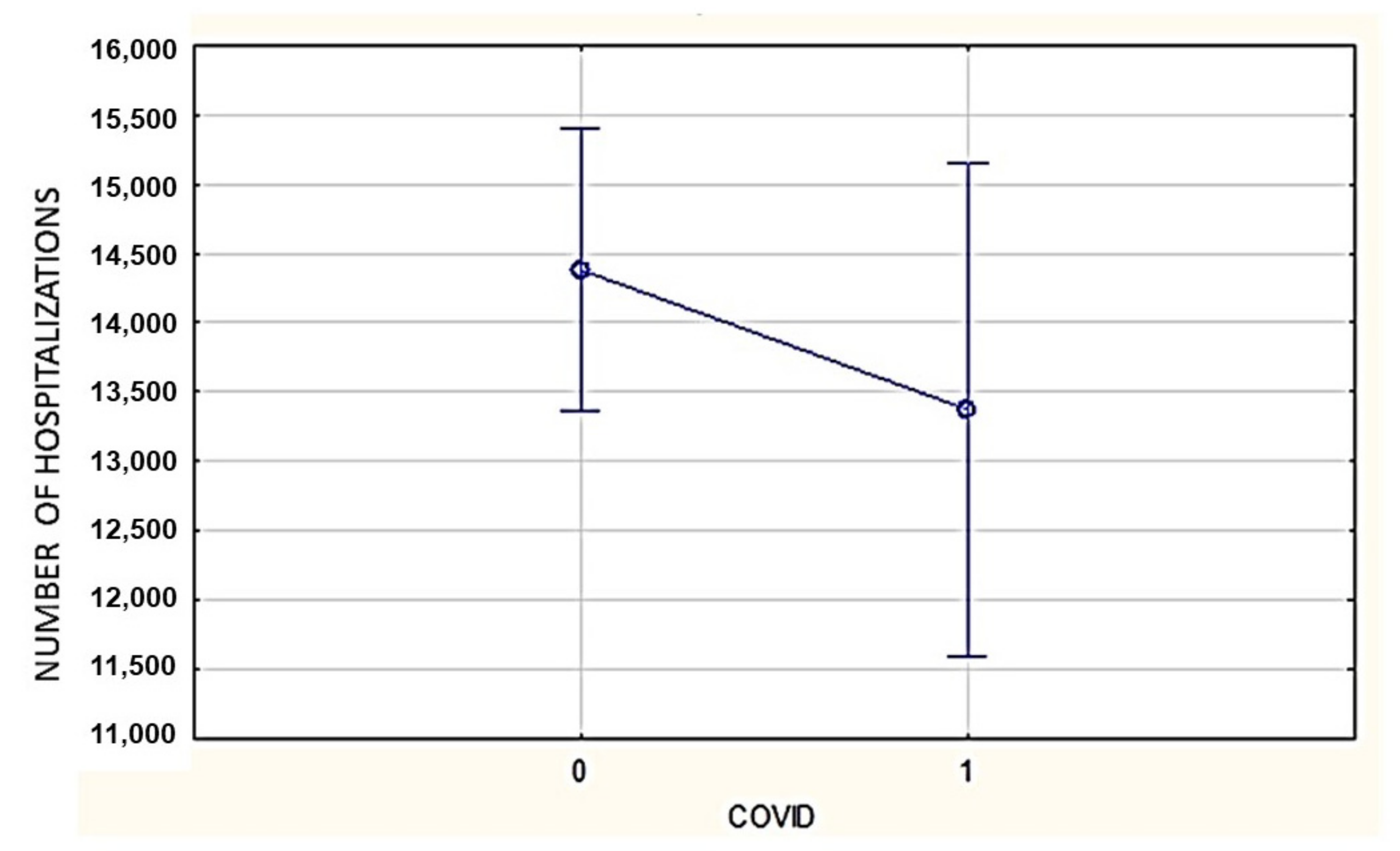
3.2. Number of Hospitalizations
3.3. Mode of Admission of Patients
3.4. DFU-Related Amputations
3.5. Limb-Salvage Procedures
3.6. Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tadic, M.; Cuspidi, C.; Sala, C. COVID-19 and diabetes: Is there enough evidence? J. Clin. Hypertens. 2020, 22, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Zhang, X.B.; Hu, L.; Ming, Q.; Wei, X.J.; Zhang, Z.Y.; Chen, L.D.; Wang, M.H.; Yao, W.Z.; Huang, Q.F.; Ye, Z.Q.; et al. Risk factors for mortality of coronavirus disease-2019 (COVID-19) patients in two centers of Hubei province, China: A retrospective analysis. PLoS ONE 2021, 16, e0246030. [Google Scholar] [CrossRef] [PubMed]
- Beran, D.; Aebischer Perone, S.; Castellsague Perolini, M.; Chappuis, F.; Chopard, P.; Haller, D.M.; Jacquerioz Bausch, F.; Maisonneuve, H.; Perone, N.; Gastaldi, G. Beyond the virus: Ensuring continuity of care for people with diabetes during COVID-19. Prim. Care Diabetes 2021, 15, 16–17. [Google Scholar] [CrossRef]
- Alshareef, R.; Al Zahrani, A.; Alzahrani, A.; Ghandoura, L. Impact of the COVID-19 lockdown on diabetes patients in Jeddah, Saudi Arabia. Diabetes Metab. Syndr. 2020, 14, 1583–1587. [Google Scholar] [CrossRef]
- Eberle, C.; Stichling, S. Impact of COVID-19 lockdown on glycemic control in patients with type 1 and type 2 diabetes mellitus: A systematic review. Diabetol. Metab. Syndr. 2021, 13, 95. [Google Scholar] [CrossRef]
- Patel, S.Y.; McCoy, R.G.; Barnett, M.L.; Shah, N.D.; Mehrotra, A. Diabetes Care and Glycemic Control During the COVID-19 Pandemic in the United States. JAMA Intern. Med. 2021, 181, 1412–1414. [Google Scholar] [CrossRef]
- Predieri, B.; Leo, F.; Candia, F.; Lucaccioni, L.; Madeo, S.F.; Pugliese, M.; Vivaccia, V.; Bruzzi, P.; Iughetti, L. Glycemic Control Improvement in Italian Children and Adolescents With Type 1 Diabetes Followed Through Telemedicine During Lockdown Due to the COVID-19 Pandemic. Front. Endocrinol. 2020, 11, 595735. [Google Scholar] [CrossRef]
- Selek, A.; Gezer, E.; Altun, E.; Sozen, M.; Topaloglu, O.; Koksalan, D.; Demirkan, H.; Karakaya, D.; Cetinarslan, B.; Canturk, Z.; et al. The impact of COVID-19 pandemic on glycemic control in patients with diabetes mellitus in Turkey: A multi-center study from Kocaeli. J. Diabetes Metab. Disord. 2021, 20, 1461–1467. [Google Scholar] [CrossRef]
- Nachimuthu, S.; Vijayalakshmi, R.; Sudha, M.; Viswanathan, V. Coping with diabetes during the COVID-19 lockdown in India: Results of an online pilot survey. Diabetes Metab. Syndr. 2020, 14, 579–582. [Google Scholar] [CrossRef]
- Levolger, S.; Bokkers, R.P.H.; Wille, J.; Kropman, R.H.J.; de Vries, J.P.M. Arterial thrombotic complications in COVID-19 patients. J. Vasc. Surg. Cases Innov. Tech. 2020, 6, 454–459. [Google Scholar] [CrossRef]
- Remuzzi, A.; Remuzzi, G. COVID-19 and Italy: What next? Lancet 2020, 395, 1225–1228. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Boulton, A.J.M.; Bus, S.A. Diabetic Foot Ulcers and Their Recurrence. N. Engl. J. Med. 2017, 376, 2367–2375. [Google Scholar] [CrossRef]
- Boulton, A.J.M. Diabetic Foot Disease during the COVID-19 Pandemic. Medicina 2021, 57, 97. [Google Scholar] [CrossRef]
- Caruso, P.; Longo, M.; Signoriello, S.; Gicchino, M.; Maiorino, M.I.; Bellastella, G.; Chiodini, P.; Giugliano, D.; Esposito, K. Diabetic Foot Problems during the COVID-19 Pandemic in a Tertiary Care Center: The Emergency among the Emergencies. Diabetes Care 2020, 43, e123–e124. [Google Scholar] [CrossRef]
- Shin, L.; Bowling, F.L.; Armstrong, D.G.; Boulton, A.J.M. Saving the Diabetic Foot During the COVID-19 Pandemic: A Tale of Two Cities. Diabetes Care 2020, 43, 1704–1709. [Google Scholar] [CrossRef]
- Peric, S.; Stulnig, T.M. Diabetes and COVID-19: Disease-Management-People. Wien. Klin. Wochenschr. 2020, 132, 356–361. [Google Scholar] [CrossRef]
- Kang, J.; Chen, Y.; Zhao, Y.; Zhang, C. Effect of remote management on comprehensive management of diabetes mellitus during the COVID-19 epidemic. Prim. Care Diabetes 2021, 15, 417–423. [Google Scholar] [CrossRef]
- Liu, C.; You, J.; Zhu, W.; Chen, Y.; Li, S.; Zhu, Y.; Ji, S.; Wang, Y.; Li, H.; Li, L.; et al. The COVID-19 Outbreak Negatively Affects the Delivery of Care for Patients With Diabetic Foot Ulcers. Diabetes Care 2020, 43, e125–e126. [Google Scholar] [CrossRef]
- Lipsky, B.A.; Senneville, E.; Abbas, Z.G.; Aragon-Sanchez, J.; Diggle, M.; Embil, J.M.; Kono, S.; Lavery, L.A.; Malone, M.; van Asten, S.A.; et al. Guidelines on the diagnosis and treatment of foot infection in persons with diabetes (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36 (Suppl. 1), e3280. [Google Scholar] [CrossRef] [Green Version]
- Gray, R.; Sanders, C. A reflection on the impact of COVID-19 on primary care in the United Kingdom. J. Interprof. Care 2020, 34, 672–678. [Google Scholar] [CrossRef]
- Chudasama, Y.V.; Gillies, C.L.; Zaccardi, F.; Coles, B.; Davies, M.J.; Seidu, S.; Khunti, K. Impact of COVID-19 on routine care for chronic diseases: A global survey of views from healthcare professionals. Diabetes Metab. Syndr. 2020, 14, 965–967. [Google Scholar] [CrossRef]
- Mariet, A.S.; Benzenine, E.; Bouillet, B.; Verges, B.; Quantin, C.; Petit, J.M. Impact of the COVID-19 Epidemic on hospitalization for diabetic foot ulcers during lockdown: A French nationwide population-based study. Diabet. Med. 2021, 38, e14577. [Google Scholar] [CrossRef]
- Urbancic-Rovan, V. Diabetic Foot Care Before and During the COVID-19 Epidemic: What Really Matters? Diabetes Care 2021, 44, e27–e28. [Google Scholar] [CrossRef]
- Ochal, M.; Romaszko, M.; Glinska-Lewczuk, K.; Gromadzinski, L.; Romaszko, J. Assessment of the Consultation Rate with General Practitioners in the Initial Phase of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 7710. [Google Scholar] [CrossRef]
- Schafer, I.; Hansen, H.; Menzel, A.; Eisele, M.; Tajdar, D.; Luhmann, D.; Scherer, M. The effect of COVID-19 pandemic and lockdown on consultation numbers, consultation reasons and performed services in primary care: Results of a longitudinal observational study. BMC Fam. Pract. 2021, 22, 125. [Google Scholar] [CrossRef]
- Kiss, P.; Carcel, C.; Hockham, C.; Peters, S.A.E. The impact of the COVID-19 pandemic on the care and management of patients with acute cardiovascular disease: A systematic review. Eur. Heart J. Qual. Care Clin. Outcomes 2021, 7, 18–27. [Google Scholar] [CrossRef]
- Anichini, R.; Brocco, E.; Caravaggi, C.M.; Da Ros, R.; Giurato, L.; Izzo, V.; Meloni, M.; Uccioli, L.; Calenda, P.; Federici, G.; et al. Physician experts in diabetes are natural team leaders for managing diabetic patients with foot complications. A position statement from the Italian diabetic foot study group. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 167–178. [Google Scholar] [CrossRef]
- Carinci, F.; Massi Benedetti, M.; Klazinga, N.S.; Uccioli, L. Lower extremity amputation rates in people with diabetes as an indicator of health systems performance. A critical appraisal of the data collection 2000-2011 by the Organization for Economic Cooperation and Development (OECD). Acta Diabetol. 2016, 53, 825–832. [Google Scholar] [CrossRef] [Green Version]
- Schlager, J.G.; Kendziora, B.; Patzak, L.; Kupf, S.; Rothenberger, C.; Fiocco, Z.; French, L.E.; Reinholz, M.; Hartmann, D. Impact of COVID-19 on wound care in Germany. Int. Wound J. 2021, 18, 536–542. [Google Scholar] [CrossRef]
- Murphy, C.; Atkin, L.; Hurlow, J.; Swanson, T.; de Ceniga, M.V. Wound hygiene survey: Awareness, implementation, barriers and outcomes. J. Wound Care 2021, 30, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Forde, R.; Arente, L.; Ausili, D.; De Backer, K.; Due-Christensen, M.; Epps, A.; Fitzpatrick, A.; Grixti, M.; Groen, S.; Halkoaho, A.; et al. The impact of the COVID-19 pandemic on people with diabetes and diabetes services: A pan-European survey of diabetes specialist nurses undertaken by the Foundation of European Nurses in Diabetes survey consortium. Diabet. Med. 2021, 38, e14498. [Google Scholar] [CrossRef] [PubMed]
- Tinelli, G.; Sica, S.; Guarnera, G.; Pitocco, D.; Tshomba, Y. Wound Care during COVID-19 Pandemic. Ann. Vasc. Surg. 2020, 68, 93–94. [Google Scholar] [CrossRef] [PubMed]
- Nachimuthu, S.; Ahmed Khan, B.; Viswanathan, V. Managing Diabetic Foot Complications During COVID-19 Lockdown in India: A Survey. Int. J. Low. Extrem. Wounds 2021, 15347346211063699. [Google Scholar] [CrossRef]
- Cole, W. A Look at the Impact of the COVID-19 Pandemic on Wound Care Practices a Year Later. Today’s Wound Clin. 2021. Available online: https://tinyurl.com/eyj54tbd (accessed on 15 December 2021).
- Naude, L. The impact of COVID-19 on Wound Care Provision in South Africa: A Personal Account. Wounds Int. 2021, 11, 17–19. Available online: https://tinyurl.com/w6jbur3m (accessed on 15 December 2021).
- Sagan, A.; Bryndova, L.; Kowalska-Bobko, I.; Smatana, M.; Spranger, A.; Szerencses, V.; Webb, E.; Gaal, P. A reversal of fortune: Comparison of health system responses to COVID-19 in the Visegrad group during the early phases of the pandemic. Health Policy 2021, in press. [CrossRef]
- Szlubowska, A. Ambulatoryjna Opieka Zdrowotna w 2020 Roku. Główny Urząd Statystyczny. Available online: https://tinyurl.com/2p8ny6vf (accessed on 15 December 2021).
- Mrozikiewicz-Rakowska, B.E.A.T.A.; Jawień, A.; Sopata, M.; Kucharzewski, M.; Szewczyk, M.T.; Kózka, M.; Korzon-Burakowska, A.N.N.A.; Rowiński, O.; Szopiński, P.; Oszkinis, G.; et al. Organizacja opieki nad chorymi z zespołem stopy cukrzycowej. Wytyczne Polskiego Towarzystwa Leczenia Ran. Leczenie Ran 2015, 12, 83–112. [Google Scholar] [CrossRef]
- Casciato, D.J.; Yancovitz, S.; Thompson, J.; Anderson, S.; Bischoff, A.; Ayres, S.; Barron, I. Diabetes-related major and minor amputation risk increased during the COVID-19 pandemic. J. Am. Podiatr. Med. Assoc. 2020. [Google Scholar] [CrossRef]
- Barshes, N.R.; Sigireddi, M.; Wrobel, J.S.; Mahankali, A.; Robbins, J.M.; Kougias, P.; Armstrong, D.G. The system of care for the diabetic foot: Objectives, outcomes, and opportunities. Diabet. Foot Ankle 2013, 4, 21847. [Google Scholar] [CrossRef]
- Tchero, H.; Noubou, L.; Becsangele, B.; Mukisi-Mukaza, M.; Retali, G.R.; Rusch, E. Telemedicine in Diabetic Foot Care: A Systematic Literature Review of Interventions and Meta-analysis of Controlled Trials. Int. J. Low. Extrem. Wounds 2017, 16, 274–283. [Google Scholar] [CrossRef]
- Yammine, K.; Estephan, M. Telemedicine and diabetic foot ulcer outcomes. A meta-analysis of controlled trials. Foot 2021, 50, 101872. [Google Scholar] [CrossRef]
- Łysoń, P. Wydatki na Ochronę Zdrowia w Latach 2018–2020. Główny Urząd Statystyczny. Available online: https://tinyurl.com/36wmwuxw (accessed on 15 December 2021).
- Schuivens, P.M.E.; Buijs, M.; Boonman-de Winter, L.; Veen, E.J.; de Groot, H.G.W.; Buimer, T.G.; Ho, G.H.; van der Laan, L. Impact of the COVID-19 Lockdown Strategy on Vascular Surgery Practice: More Major Amputations than Usual. Ann. Vasc. Surg. 2020, 69, 74–79. [Google Scholar] [CrossRef]
- Du, C.; Li, Y.; Xie, P.; Zhang, X.; Deng, B.; Wang, G.; Hu, Y.; Wang, M.; Deng, W.; Armstrong, D.G.; et al. The amputation and mortality of inpatients with diabetic foot ulceration in the COVID-19 pandemic and postpandemic era: A machine learning study. Int. Wound J. 2021. [Google Scholar] [CrossRef]
- Viswanathan, V.; Nachimuthu, S. Major Lower-Limb Amputation During the COVID Pandemic in South India. Int. J. Low. Extrem. Wounds 2021, 15347346211020985. [Google Scholar] [CrossRef]
- Valabhji, J.; Barron, E.; Vamos, E.P.; Dhatariya, K.; Game, F.; Kar, P.; Weaver, A.; Verma, S.; Young, B.; Khunti, K. Temporal Trends in Lower-Limb Major and Minor Amputation and Revascularization Procedures in People With Diabetes in England During the COVID-19 Pandemic. Diabetes Care 2021, 44, e133–e135. [Google Scholar] [CrossRef]
- Meloni, M.; Bouillet, B.; Ahluwalia, R.; Ludemann, C.; Sanchez-Rios, J.P.; Iacopi, E.; Lazaro-Martinez, J.L. Fast-track pathway for diabetic foot ulceration during COVID-19 crisis: A document from International Diabetic Foot Care Group and D-Foot International. Diabetes Metab. Res. Rev. 2021, 37, e3396. [Google Scholar] [CrossRef]
- Meloni, M.; Izzo, V.; Giurato, L.; Gandini, R.; Uccioli, L. Management of diabetic persons with foot ulceration during COVID-19 health care emergency: Effectiveness of a new triage pathway. Diabetes Res. Clin. Pract. 2020, 165, 108245. [Google Scholar] [CrossRef]
- Schmidt, B.M.; Munson, M.E.; Rothenberg, G.M.; Holmes, C.M.; Pop-Busui, R. Strategies to reduce severe diabetic foot infections and complications during epidemics (STRIDE). J Diabetes Complicat. 2020, 34, 107691. [Google Scholar] [CrossRef]
- Kelahmetoglu, O.; Camli, M.F.; Kirazoglu, A.; Erbayat, Y.; Asgarzade, S.; Durgun, U.; Mehdizade, T.; Yeniocak, A.; Yildiz, K.; Sonmez Ergun, S.; et al. Recommendations for management of diabetic foot ulcers during COVID-19 outbreak. Int. Wound J. 2020, 17, 1424–1427. [Google Scholar] [CrossRef]
- Rastogi, A.; Hiteshi, P.; Bhansali, A.A.; Jude, E.B. Virtual triage and outcomes of diabetic foot complications during Covid-19 pandemic: A retro-prospective, observational cohort study. PLoS ONE 2021, 16, e0251143. [Google Scholar] [CrossRef]
- Atri, A.; Kocherlakota, C.M.; Dasgupta, R. Managing diabetic foot in times of COVID-19: Time to put the best ‘foot’ forward. Int. J. Diabetes Dev. Ctries 2020, 40, 321–328. [Google Scholar] [CrossRef]
- Liu, C.; Shi, W.L.; You, J.X.; Li, H.Y.; Li, L. An internet-based algorithm for diabetic foot infection during the COVID-19 pandemic. J. Foot Ankle Res. 2020, 13, 37. [Google Scholar] [CrossRef]
- Adeleye, O.O.; Ugwu, E.T.; Gezawa, I.D.; Okpe, I.; Ezeani, I.; Enamino, M. Predictors of intra-hospital mortality in patients with diabetic foot ulcers in Nigeria: Data from the MEDFUN study. BMC Endocr. Disord. 2020, 20, 134. [Google Scholar] [CrossRef]

{kind=link}
| Variables | COVID = 0 | COVID = 1 | p | |
|---|---|---|---|---|
| n (%) | n (%) | |||
| All = 14,383.4 | All = 13,377 | |||
| Age | 0–17 | 203.7 (1.4) | 140 (1) | 0.21 |
| 18–40 | 806.3 (5.6) | 694 (5.2) | ||
| 41–60 | 3867 (26.9) | 3422 (25.6) | ||
| 61–80 | 7584.3 (52.7) | 7403 (55.3) | ||
| ≥81 | 1922 (13.4) | 1718 (12.8) | ||
| Gender | Male | 9394.7 (65.3) | 8981 (67.1) | 0.69 |
| Female | 4988.7 (34.7) | 4396 (32.9) | ||
| Mode of Admission | Years | Percentage | Standard Deviation | p |
|---|---|---|---|---|
| Elective | 2017–2019 | 29.6 | 0.36 | 0.001 |
| 2020 | 26.3 | 0.62 | ||
| Urgent | 2017–2019 | 67.0 | 0.36 | 0.01 |
| 2020 | 73.2 | 0.62 |
| Type of Procedures | Years | Number/Percentage | Standard Deviation | p | |
|---|---|---|---|---|---|
| Amputations | Minor | 2017–2019 | 3146 | 74 | 0.017 |
| 2020 | 4269 | 112.8 | |||
| Major | 2017–2019 | 2146 | 65 | 0.05 | |
| 2020 | 1600 | 112.6 | |||
| Limb-salvage procedures | 2017–2019 | 79.4% | 0.41 | 0.001 | |
| 2020 | 71.3% | 0.71 | |||
| Years | Percentage | Standard Deviation | p |
|---|---|---|---|
| 2017–2019 | 3.90 | 0.14 | 0.03 |
| 2020 | 4.84 | 0.25 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kleibert, M.; Mrozikiewicz-Rakowska, B.; Bąk, P.M.; Bałut, D.; Zieliński, J.; Czupryniak, L. Breakdown of Diabetic Foot Ulcer Care during the First Year of the Pandemic in Poland: A Retrospective National Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 3827. https://doi.org/10.3390/ijerph19073827
Kleibert M, Mrozikiewicz-Rakowska B, Bąk PM, Bałut D, Zieliński J, Czupryniak L. Breakdown of Diabetic Foot Ulcer Care during the First Year of the Pandemic in Poland: A Retrospective National Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(7):3827. https://doi.org/10.3390/ijerph19073827
Chicago/Turabian StyleKleibert, Marcin, Beata Mrozikiewicz-Rakowska, Patrycja Małgorzata Bąk, Daniel Bałut, Jakub Zieliński, and Leszek Czupryniak. 2022. "Breakdown of Diabetic Foot Ulcer Care during the First Year of the Pandemic in Poland: A Retrospective National Cohort Study" International Journal of Environmental Research and Public Health 19, no. 7: 3827. https://doi.org/10.3390/ijerph19073827
APA StyleKleibert, M., Mrozikiewicz-Rakowska, B., Bąk, P. M., Bałut, D., Zieliński, J., & Czupryniak, L. (2022). Breakdown of Diabetic Foot Ulcer Care during the First Year of the Pandemic in Poland: A Retrospective National Cohort Study. International Journal of Environmental Research and Public Health, 19(7), 3827. https://doi.org/10.3390/ijerph19073827